Embed Size (px)
Citation preview
Mt. Vernon Department of Recreation
2015SUMMER
CAMP
JULY & AUGUST
CAMPS !! CLINICS!!
MOUNT VERNON RECREATION OFFICE HOURS 8:30AM-4:30PM. FOR MORE INFORMATION CALL (914) 665-2420 OR WWW.CMVNY.COM
*No refunds will be given after JUNE 1, 2015. In the event that a child withdraws from the program, a $25 processing fee will be assessed towards refund*
Honorable Ernest D. DavisMayorDarren M. Morton, Ed. D.CommissionerDiane Atkins, MPADeputy-Commissioner
Welcome Parents/Guardians
The Mount Vernon Department of Recreation is excited to announce the return of our Summer camps featuring an array of fun filled activities. The Recreation Department proudly offers a summer filled with healthy, safe and affordable activities organized under the leadership of Commissioner Darren Morton. Returning this year are: • Senior Camp will be held at Holmes Elementary School, boys and girls ages 9 to 12 years old. • Junior Camp will be held at Pennington Elementary School for boys and girls ages 5 to 8 years old. • The Rose Simon Camp is a specialized camp designed for children with disabilities. For more information please call (914) 665 – 2437.
The Recreation Department is dedicated to making this summer a memorable one for the youth of Mount Vernon. There are many activities that will be included in the camp experience such as but not limited to: swimming, arts and crafts, field trips, outdoor activities, dance, drama and organized games. Camp starts July 6, 2015 - August 14, 2015. Monday - Friday, 9:00a.m. - 3:00p.m.
Fee $550.00 (Senior & Junior Camps). $450.00 EARLY BIRD SPECIAL FOR SENIOR & JUNIOR CAMP.
PAYMENT IN FULL BY May 1, 2015.
The Department also offers clinics which has a shorter day schedule
Basketball Clinic - $425.00 for six weeks or $90.00 per week. Mon.-Fri. 1:00pm-5:00pm Tennis Clinic - $100.00 for twelve week session. Fridays ONLYSoccer Clinic - $200.00 per session or $50.00 per week, Mon. - Thurs. 4:00p.m. - 6:00p.m. Band Clinic - $200.00 for six weeks Mon. - Thurs. 9:00a.m. - 2:30p.m.
*Enrollment is based on a first come first served basis. Early registration is recommended as well. Registration will not be accepted without completing
the Medical and Swim waiver.
Families registering may do so at Mount Vernon City Hall, 1 Roosevelt Square (room #11)
Ernest D. DavisMayor
Darren M. MortonCommissioner
Ric WrightDirector of Athletics, Programs and Services
Diane AtkinsDeputy Commissioner
City of Mount Vernon, New York Mount Vernon
Department of Recreation

Join Us! Monday - Friday from 9:00 a.m. - 3:00 p.m for recreational activities! Activities include, basketball, kick ball, baseball, arts & crafts and more! Campers will enjoy trips along with weekly swimming.
EARLY BIRD SPECIAL
$450.00
Monday, July 6, 2015 - Friday, August 14, 2015Register NOW
(Checks, cash or money orders only!)Program Fee: $550.00 for 6 weeks
SUMMER CAMPS
Department of Recreation Summer 2015 City of Mount Vernon
RECREATION “The City That Believes”
Honorable Ernest D. Davis Mayor Darren Morton, Commissioner Diane Atkins, Deputy Commissioner
For more information call (914) 665-2420 Monday through Friday from 8:30 a.m. - 4:30 p.m.
Recreation Summer Fun!!
pay in full before May 1, 2015
JUNIOR CAMP SENIOR CAMP AGES 5-8 AGES 9-12
BASKETBALL CLINIC TENNIS CLINIC BAND CLINIC SOCCER CLINIC
THE DATESALL CLINICS WILL START MONDAY, JULY 6, 2015 THROUGH AUGUST 14, 2015
BASKETBALL CLINIC - LOCATION - MT. VERNON HIGH SCHOOLSESSION 1 - JULY 6TH - JULY 10TH - 1pm-5pmSESSION 2 - JULY 13TH - JULY 17TH - 1pm-5pmSESSION 3 - JULY 20ST - JULY 24TH - 1pm-5pmSESSION 4 - JULY 27TH - JULY 31TH - 1pm-5pmSESSION 5 - AUGUST 3TH - AUGUST 7TH - 1pm-5pmSESSION 6 - AUGUST 10TH - AUGUST 14TH - 1pm-5pm
TENNIS CLINIC - LOCATION - TBAJUNE 26TH - SEPTEMBER 18TH (12 WEEK SESSIONS)5PM-8PM
SOCCER CLINIC - LOCATION - HUTCHINSON FIELDSESSION 1 - JULY 6TH - JULY 10TH - 4pm-6pmSESSION 2 - JULY 13TH - JULY 17TH - 4pm-6pmSESSION 3 - JULY 20ST - JULY 24TH - 4pm-6pmSESSION 4 - JULY 27TH - JULY 31TH - 4pm-6pmSESSION 5 - AUGUST 3TH - AUGUST 7TH - 4pm-6pmSESSION 6 - AUGUST 10TH - AUGUST 14TH - 4pm-6pm
BAND CLINIC - LOCATION - MANDELA HIGH SCHOOLSESSION 1 - JULY 6TH - JULY 10TH - 9am-2:30pmSESSION 2 - JULY 13TH - JULY 17TH - 9am-2:30pmSESSION 3 - JULY 20ST - JULY 24TH - 9am-2:30pmSESSION 4 - JULY 27TH - JULY 31TH - 9am-2:30pmSESSION 5 - AUGUST 3TH - AUGUST 7TH - 9am-2:30pmSESSION 6 - AUGUST 10TH - AUGUST 14TH - 9am-2:30pm
THE FEESBASKETBALL CLINIC
$425.00 FOR SIX WEEK SESSIONOR
$90.00 PER WEEK
FRIDAY TENNIS CLINIC $100.00 PER SESSION
SOCCER CLINIC$200 FOR SIX WEEK SESSION
OR $50.00 PER WEEK
BAND CLINIC$200 FOR SIX WEEK SESSION

Biddy-Midget Basketball
League/CLINIC Hartley Park
Boys and Girls ages 6 - 14
July 6, 2015 - August 15, 2015
Monday, Tuesday: 4:30pm - 8:30pm
Saturday: 9:00am - 11:00am
FEE: $35.00
Register NOW City Hall, RM 11Monday through Friday 8:30am - 4:30pm
Department of Recreation Parks Activation Program
Monday through Thursday 10:00 a.m. to 3:00 p.m.
FREE
Come join the Department of Recreation as we bring our parks to life this summer. Children of all ages can join us for FREE activities. Children under the age of ten (10) must be accompanied by parent/guardian.
Howard Street Playground 10:00am-12:00pm - Howard street & High Street
Fleetwood Playground 10:00am-12:00pm - Corner of Fleetwood Avenue & Broad Street
Old 7th Avenue Playground 1:00pm - 3:00pm - 7th Avenue
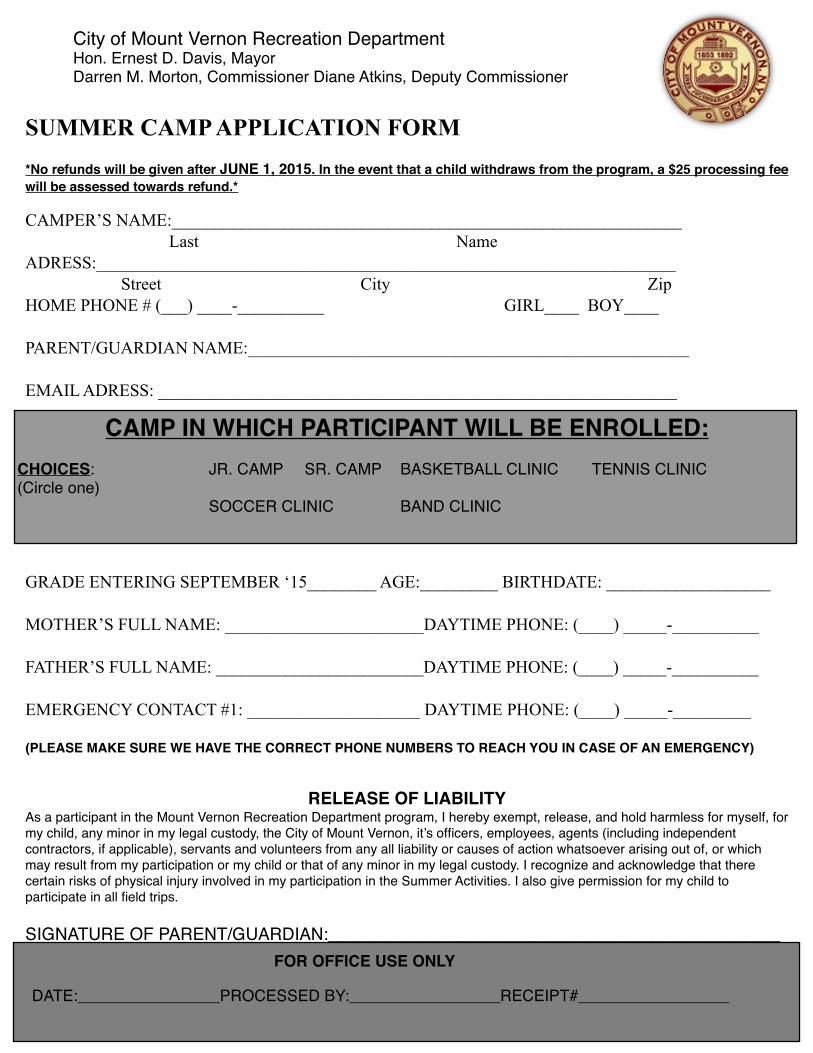
! City of Mount Vernon Recreation Department ! Hon. Ernest D. Davis, Mayor! Darren M. Morton, Commissioner Diane Atkins, Deputy Commissioner
SUMMER CAMP APPLICATION FORM*No refunds will be given after JUNE 1, 2015. In the event that a child withdraws from the program, a $25 processing fee will be assessed towards refund.*
CAMPER’S NAME:___________________________________________________________ Last NameADRESS:___________________________________________________________________ Street City ZipHOME PHONE # (___) ____-__________ GIRL____ BOY____
PARENT/GUARDIAN NAME:___________________________________________________
EMAIL ADRESS: ____________________________________________________________
GRADE ENTERING SEPTEMBER ‘15________ AGE:_________ BIRTHDATE: ___________________
MOTHER’S FULL NAME: _______________________DAYTIME PHONE: (____) _____-__________
FATHER’S FULL NAME: ________________________DAYTIME PHONE: (____) _____-__________
EMERGENCY CONTACT #1: ____________________ DAYTIME PHONE: (____) _____-_________
(PLEASE MAKE SURE WE HAVE THE CORRECT PHONE NUMBERS TO REACH YOU IN CASE OF AN EMERGENCY)
RELEASE OF LIABILITYAs a participant in the Mount Vernon Recreation Department program, I hereby exempt, release, and hold harmless for myself, for my child, any minor in my legal custody, the City of Mount Vernon, it’s officers, employees, agents (including independent contractors, if applicable), servants and volunteers from any all liability or causes of action whatsoever arising out of, or which may result from my participation or my child or that of any minor in my legal custody. I recognize and acknowledge that there certain risks of physical injury involved in my participation in the Summer Activities. I also give permission for my child to participate in all field trips.
SIGNATURE OF PARENT/GUARDIAN:_______________________________________________
CAMP IN WHICH PARTICIPANT WILL BE ENROLLED:CHOICES: ! ! ! JR. CAMP ! SR. CAMP! BASKETBALL CLINIC ! TENNIS CLINIC(Circle one)! ! !! ! ! ! SOCCER CLINIC! ! BAND CLINIC
DATE:________________PROCESSED BY:_________________RECEIPT#_________________
FOR OFFICE USE ONLY
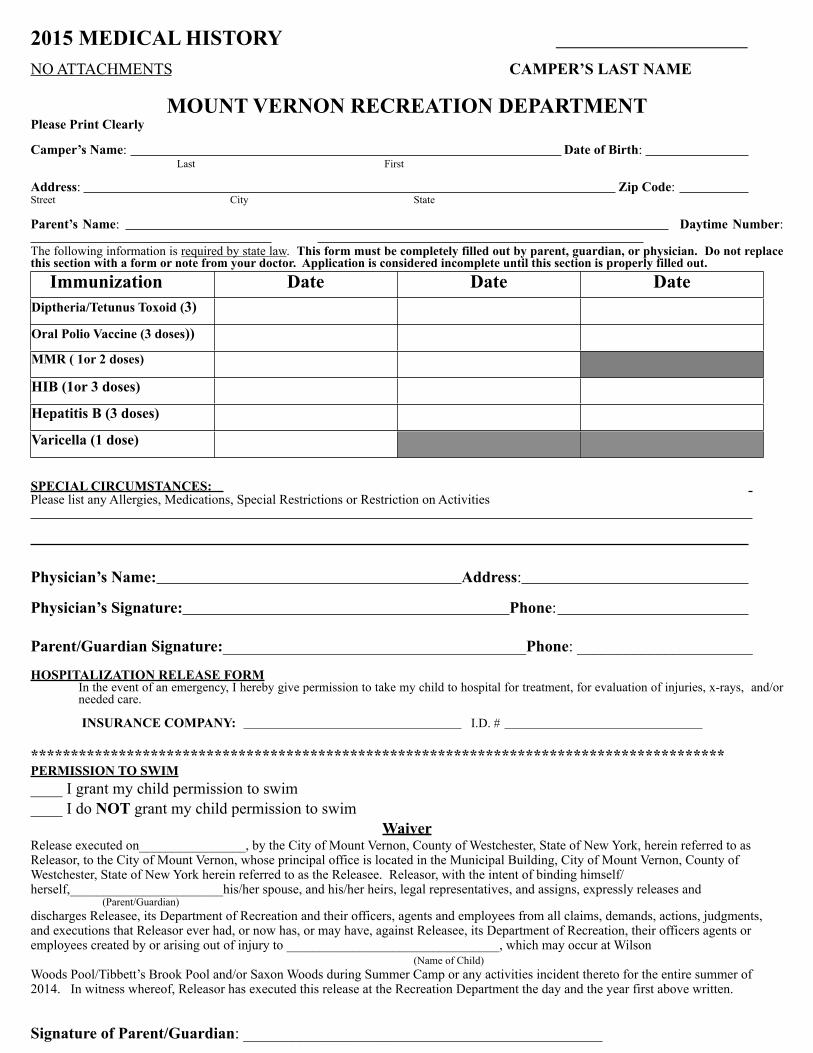
2015 MEDICAL HISTORY ________________________
NO ATTACHMENTS CAMPER’S LAST NAME
MOUNT VERNON RECREATION DEPARTMENTPlease Print Clearly
Camper’s Name: Date of Birth: Last First
Address: Zip Code: Street City State
Parent’s Name: Daytime Number: The following information is required by state law. This form must be completely filled out by parent, guardian, or physician. Do not replace this section with a form or note from your doctor. Application is considered incomplete until this section is properly filled out. Immunization Date Date DateDiptheria/Tetunus Toxoid (3)
Oral Polio Vaccine (3 doses))
MMR ( 1or 2 doses)
HIB (1or 3 doses)
Hepatitis B (3 doses)
Varicella (1 dose)
SPECIAL CIRCUMSTANCES: Please list any Allergies, Medications, Special Restrictions or Restriction on Activities
Physician’s Name: Address:
Physician’s Signature: Phone:
Parent/Guardian Signature:______________________________________Phone: ______________________
HOSPITALIZATION RELEASE FORMIn the event of an emergency, I hereby give permission to take my child to hospital for treatment, for evaluation of injuries, x-rays, and/or needed care.
INSURANCE COMPANY: I.D. #
***************************************************************************************PERMISSION TO SWIM____ I grant my child permission to swim____ I do NOT grant my child permission to swim
WaiverRelease executed on________________, by the City of Mount Vernon, County of Westchester, State of New York, herein referred to as Releasor, to the City of Mount Vernon, whose principal office is located in the Municipal Building, City of Mount Vernon, County of Westchester, State of New York herein referred to as the Releasee. Releasor, with the intent of binding himself/herself,_______________________his/her spouse, and his/her heirs, legal representatives, and assigns, expressly releases and (Parent/Guardian)discharges Releasee, its Department of Recreation and their officers, agents and employees from all claims, demands, actions, judgments, and executions that Releasor ever had, or now has, or may have, against Releasee, its Department of Recreation, their officers agents or employees created by or arising out of injury to ________________________________, which may occur at Wilson (Name of Child)Woods Pool/Tibbett’s Brook Pool and/or Saxon Woods during Summer Camp or any activities incident thereto for the entire summer of 2014. In witness whereof, Releasor has executed this release at the Recreation Department the day and the year first above written.
Signature of Parent/Guardian: _____________________________________________