Embed Size (px)
Citation preview

Now the public seems to be sidingwith the critters. In a survey conductedfor the Fund for Animals last year, al-most three fourths of the Washingtonresidents polled opposed the Park Ser-viceÕs plan. Those Þgures agree roughlywith the balance of comments receivedby the Park Service following publica-tion of its draft environmental-impact
statement last year. Park sources saypublic opposition could sway the ser-viceÕs Þnal decision, which is due inApril. And they expect a legal challengeno matter what is decided.
But even if the scheme is implement-ed this summer, it probably will not becurtains for the Olympic mountaingoats, according to Morris. For better
or worse, their complete eradication onthe Olympic Peninsula is highly unlike-ly, because goats also occupy the na-tional forest that surrounds much ofthe park. ÒWeÕve already caught the vil-lage idiots,Ó the park superintendentsays; only the most elusive animals arestill at large. Morris adds, ruefully, ÒWeÕllnever get the last goat.ÓÑKaren Wright
26 SCIENTIFIC AMERICAN March 1996
In 1994 half a million Americans suffered a stroke; ofthese, 154,000 died, more than the number who died
from any other cause except coronary heart disease. Withmore than three million stroke survivors currently incapac-itated, it is the leading cause of disability in the U.S. World-wide, probably more than six million people died fromstroke in 1994. The disease, which occurs because of block-ing or hemorrhaging of blood vessels in the brain, may re-sult in paralysis of limbs, loss of speech, and other infirmi-ties. The stroke mortality rate of women in most countriesis 60 to 90 percent that of men, but because the rates risesteeply with age, and because women live longer thanmen do, more women actually die of the disease.
Differences in stroke mortality among countries are wide;for example, the former Soviet Union has a rate more thanfive times that of the U.S. Part of the difference, at leastwhen comparing western countries with eastern Europeancountries, is the result of inferior medical treatment ineastern Europe; however, risk factors, including hyperten-sion, the dominant precursor of stroke, are higher in theEast, and cigarette smoking and excessive drinking, whichalso contribute to the disease, are more widespread thereas well. Other, more hypothetical risk factors may add to
the eastern European rates, such as a scarcity of citrus fruit,a prime source of vitamin C. Vitamin C and other antioxi-dants block formation of free oxygen radicals, thought toplay a role in the development of atherosclerosis, the un-derlying condition leading to blockage of arteries.
In the U.S., as in virtually every other country for whichdata are available, stroke mortality rates have declineddramatically in recent decades. One reason is better detec-tion of milder, more treatable strokes through computedtomography scanning. Since the 1970s, public health pro-grams designed to reduce hypertension through drugs,diet and exercise have been in place, and some countries,such as the U.S., have benefited from declining consump-tion of cigarettes and alcohol.
Black Americans die from stroke at more than twice therate of white Americans, primarily because of higherblood pressure levels, apparently resulting, at least in part,from greater sensitivity to dietary salt. Blacks may also beat risk because of poor fetal and infant nutrition, whichmay contribute to hypertension in later life. In the north-ern U.S., blacks have a lower stroke mortality rate, perhapsbecause they are more affluent and hence less apt to suf-fer nutritional deprivation as children. —Rodger Doyle
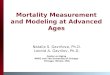
Stroke Mortality in Men Ages 35 to 74
PANAMACOSTA RICA
HONG KONG
SINGAPORE
KUWAIT
ISRAEL
MAURITIUS
TRINIDAD
U.S. BLACK
U.S.WHITE
FEWER THAN 80 DEATHS PER 100,000 PEOPLE
80 TO 129.9 PER 100,000
130 OR MORE PER 100,000
NO DATA OR DATA UNRELIABLESOURCE: World Health Organization. Data are for most recentyear available (usually 1988, 1989 or 1990) and are age-adjusted.
RO
DG
ER
DO
YLE
Copyright 1996 Scientific American, Inc.