Embed Size (px)
DESCRIPTION
NAMLIT 1096
Citation preview
Straumann®Bone Level Tapered Implant
Clinical Review

Designed for primary stability
Fast osseointegration
Immediate function
Broad treatment options

Roxolid® An alloy of titanium and zirconium with excellent mechanical properties
SLActive® surface allows fast and predictable osseointegration
Apically tapered implant body design allows underpreparation and is designed to support primary stability in soft bone
STRAUMANN® CROSSFIT® CONNECTIONRestorative flexibility with the prosthetic components
of the Straumann® Bone Level Implant line

HIGH PRIMARY STABILITY
Primary stability of dental implants, defined as the stability at the time of implant placement, is an important prerequisite for achieving successful osseointegration (Branemark et al.,1977; Meredith, 1998). High primary stability prevents micromovements of the implant and therefore war- rants its rigidity. This is important since the implant should not be sub-jected to micromotion of more than 50‒150 µm during the heal- ing phase in order to avoid fibrous tissue encapsulation (Cameron et al., 1973; Szmukler-Moncler et al., 1998). A study demonstrated that for ta-pered implants the initial stability is secured over the bone remodeling stages (Rokn et al., 2011).
FAST OSSEOINTEGRATION
Surface modifications play an important role in the speed of osseointe-gration and thereby influence implant stability as well as success of im-mediate and early loading protocols (Buser et al., 1991; Coelho et al., 2011; Elias et al., 2008; Shalabi et al., 2006). Straumann® SLActive® is a chemically modified hydrophilic surface which is clinically proven to accelerate the osseous healing* (Buser et al., 2004; Lang et al., 2011; Oates et al., 2007; Schwarz et al., 2007). The hydrophilic and chemi-cally active properties of SLActive® provide a larger accessible surface area for increased blood protein adsorption (Kopf et al., 2015), greater osteoblast differentiation and increased production of bone-building osteocalcin (Zhao et al., 2005) as well as stimulated blood vessel growth
One reason for this is that the tapered implant body design allows for preparing the site with tools one size smaller than the diameter of the implant, thus increasing the resis-tance to implant insertion. The lat-eral compression of the bone around the underprepared osteotomy walls leads to a continuous increase of insertion torque, an important observation especially for soft bone types as increasing peak torque values have been correlated to increased implant stability during the healing phase (Molly, 2006).
Straumann® Bone Level Tapered Implants have an apically tapered implant body and are designed for primary stability in soft bone and fresh extraction sockets.
*Compared to SLA

(Schwarz et al., 2008). Beyond that, studies with Roxolid® Implants with the SLActive® surface have osseointegration properties similar or even better than those of titanium SLActive® implants (Gottlow et al., 2012; Lang et al., 2011; Wen et al., 2013). Roxolid® is a metal alloy composed of ~15 % zirconium and ~85 % titanium, the only two metals commonly used in implantology that do not inhibit the growth of osteoblasts (Steinemann, 1998). Interestingly, titanium-zirconium alloys like Roxolid® have better biocompatibility than titanium (Ikarashi Y et al., 2005) and an up to 40 % higher fatigue strength than comparable titanium implants (Straumann data on file). Straumann® Bone Level Tapered Implants with the combination of Roxolid® and SLActive® surface speed up the process of new bone formation on the implant and thereby shorten the critical transition phase between primaryand secondary stability.
DID YOU KNOW?The current global tapered design implants market is continuously growing (Fig. 1). More and more dental experts use tapered implants. The trend is driven by the growing patient demand for the immediate restoration of esthetics and function, but with simpler, more cost-effective and less time-consuming treatment procedures.
Fig. 1: Current global tapered design implants market trends (iData Research Inc., 2013; Millenium Research Group, 2015).
20142013 2015 2016 2017 2018 2019
0
500
1000
1500
2000
2500
■ Tapered Design (USA) ■ Tapered Design (Canada)
in k
uni
tes
3000
IMMEDIATE FUNCTION
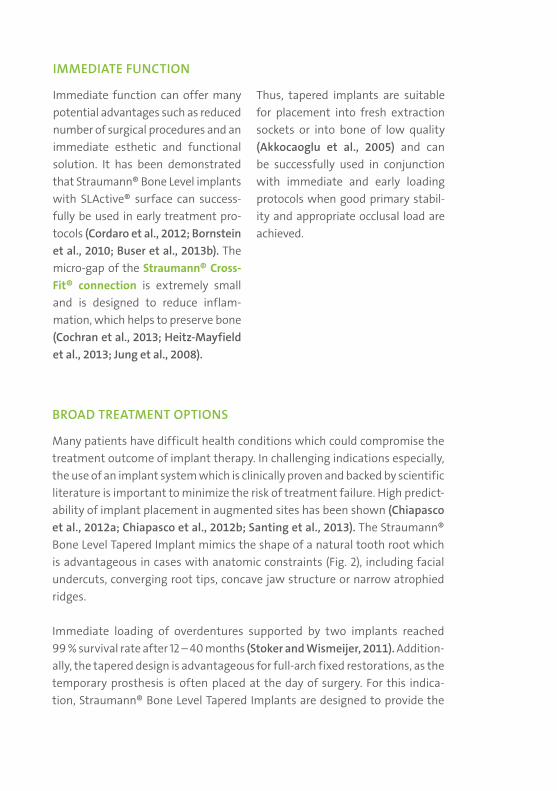
Immediate function can offer many potential advantages such as reduced number of surgical procedures and an immediate esthetic and functional solution. It has been demonstrated that Straumann® Bone Level implants with SLActive® surface can success-fully be used in early treatment pro-tocols (Cordaro et al., 2012; Bornstein et al., 2010; Buser et al., 2013b). The micro-gap of the Straumann® Cross-Fit® connection is extremely small and is designed to reduce inflam- mation, which helps to preserve bone (Cochran et al., 2013; Heitz-Mayfield et al., 2013; Jung et al., 2008).
Thus, tapered implants are suitable for placement into fresh extraction sockets or into bone of low quality (Akkocaoglu et al., 2005) and can be successfully used in conjunction with immediate and early loading protocols when good primary stabil-ity and appropriate occlusal load are achieved.
BROAD TREATMENT OPTIONS
Many patients have difficult health conditions which could compromise the treatment outcome of implant therapy. In challenging indications especially, the use of an implant system which is clinically proven and backed by scientific literature is important to minimize the risk of treatment failure. High predict-ability of implant placement in augmented sites has been shown (Chiapasco et al., 2012a; Chiapasco et al., 2012b; Santing et al., 2013). The Straumann® Bone Level Tapered Implant mimics the shape of a natural tooth root which is advantageous in cases with anatomic constraints (Fig. 2), including facial undercuts, converging root tips, concave jaw structure or narrow atrophied ridges.
Immediate loading of overdentures supported by two implants reached 99 % survival rate after 12 – 40 months (Stoker and Wismeijer, 2011). Addition-ally, the tapered design is advantageous for full-arch fixed restorations, as the temporary prosthesis is often placed at the day of surgery. For this indica-tion, Straumann® Bone Level Tapered Implants are designed to provide the
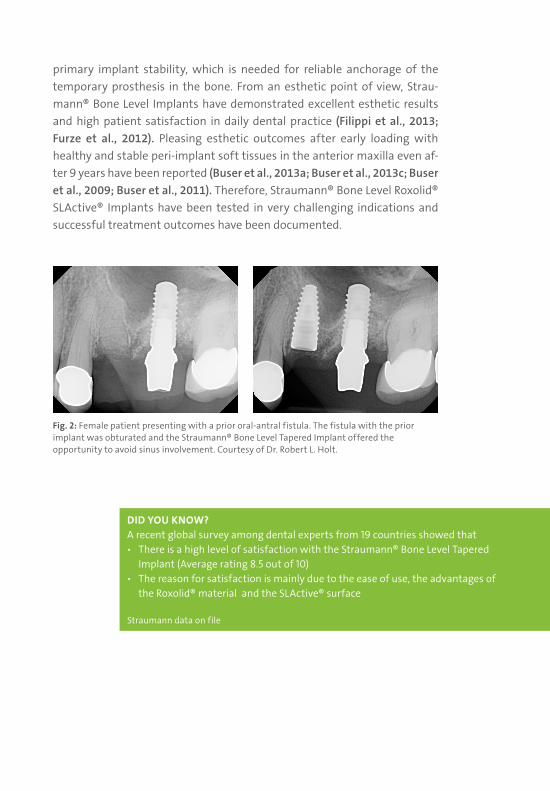
Fig. 2: Female patient presenting with a prior oral-antral fistula. The fistula with the prior implant was obturated and the Straumann® Bone Level Tapered Implant offered the opportunity to avoid sinus involvement. Courtesy of Dr. Robert L. Holt.
DID YOU KNOW?A recent global survey among dental experts from 19 countries showed that ѹ There is a high level of satisfaction with the Straumann® Bone Level Tapered
Implant (Average rating 8.5 out of 10) ѹ The reason for satisfaction is mainly due to the ease of use, the advantages of
the Roxolid® material and the SLActive® surface
Straumann data on file
primary implant stability, which is needed for reliable anchorage of the temporary prosthesis in the bone. From an esthetic point of view, Strau-mann® Bone Level Implants have demonstrated excellent esthetic results and high patient satisfaction in daily dental practice (Filippi et al., 2013; Furze et al., 2012). Pleasing esthetic outcomes after early loading with healthy and stable peri-implant soft tissues in the anterior maxilla even af-ter 9 years have been reported (Buser et al., 2013a; Buser et al., 2013c; Buser et al., 2009; Buser et al., 2011). Therefore, Straumann® Bone Level Roxolid® SLActive® Implants have been tested in very challenging indications and successful treatment outcomes have been documented.

NAM
LIT
1096
10/1
5
Akkocaoglu M et al. Implant design and intraosseous stability of immediately placed implants: a human cadaver study. Clin Oral Implants Res. 2005 Apr;16(2):202-9. - Bornstein MM et al. Early loading at 21 days of non-submerged titanium implants with a chemically modified sandblasted and acid-etched surface: 3-year results of a prospective study in the posterior mandible.J Periodontol. 2010 Jun;81(6):809-18. - Branemark PI et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Re-constr Surg Suppl. 1977;16:1-132. — Buser D et al. Enhanced bone apposition to a chemically modified SLA titanium surface. J Dent Res. 2004 Jul;83(7):529-33. — Buser D et al. Long-term stability of contour augmentation with early implant placement following single tooth extraction in the esthetic zone: a prospective, cross-sectional study in 41 patients with a 5- to 9-year follow-up. J Periodontol. 2013 Nov;84(11):1517-27. Epub 2013 Jan 24. — Buser D et al. Long-term stability of early implant placement with contour augmentation. J Dent Res. 2013 Dec;92(12 Suppl):176S-82S. Epub 2013 Oct 24. — Buser D et al. Long-term stability of early implant placement with contour augmentation. J Dent Res. 2013 Dec;92(12 Suppl):176S-82S. Epub 2013 Oct 24. — Buser D et al. Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: 12-month results of a prospective study with 20 consecutive patients. J Periodontol. 2009 Jan;80(1):152-62. — Buser D et al. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J Biomed Mater Res. 1991 Jul;25(7):889-902. — Buser D et al. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. J Periodontol. 2011 Mar;82(3):342-9. Epub 2010 Sep 10. — Cameron HU et al. The effect of movement on the bonding of porous metal to bone. J Biomed Mater Res. 1973 Jul;7(4):301-11. — Chiapasco M et al. Evaluation of peri-implant bone resorption around Straumann Bone Level implants placed in areas reconstructed with autogenous vertical onlay bone grafts.Clin Oral Implants Res. 2012 Sep;23(9):1012-21. Epub 2011 Aug 9. — Chiapasco M et al. Titanium-zirconium alloy narrow-diameter implants (Straumann Roxolid(®)) for the rehabilitation of horizontally deficient edentulous ridges: prospective study on 18 consecutive patients. Clin Oral Implants Res. 2012 Oct;23(10):1136-41. Epub 2011 Aug 18. — Cochran DL et al. Soft and hard tissue histologic dimensions around dental implants in the canine restored with smaller-diameter abut-ments: a paradigm shift in peri-implant biology. Int J Oral Maxillofac Implants. 2013 Mar-Apr;28(2):494-502. — Coelho PG et al. The effect of different implant macrogeometries and surface treatment in early biomechanical fixation: an experimental study in dogs. J Mech Behav Biomed Mater. 2011 Nov;4(8):1974-81. Epub 2011 Jul 3. — Cordaro L et al. Implant-supported single tooth restoration in the aesthetic zone: transmucosal and submerged healing provide similar outcome when simultaneous bone augmentation is needed. Clin Oral Implants Res. 2013 Oct;24(10):1130-6. Epub 2012 Jun 15. — Elias CN. Relationship between surface properties (roughness, wettability and morphology) of titanium and dental implant removal torque. J Mech Behav Biomed Mater. 2008 Jul;1(3):234-42. Epub 2007 Dec 31. — Filippi A et al. A prospec-tive noninterventional study to document implant success and survival of the Straumann Bone Level SLActive dental implant in daily dental practice. Quintessence Int. 2013 Jul;44(7):499-512. — Furze D et al. Clinical and esthetic outcomes of single-tooth implants in the anterior maxilla. Quintessence Int. 2012 Feb;43(2):127-34. — Gottlow J et al. Evaluation of a new titanium-zirconium dental implant: a biomechanical and histological comparative study in the mini pig. Clin Implant Dent Relat Res. 2012 Aug;14(4):538-45. Epub 2010 Jun 25. — Heitz-Mayfield LJ et al. Preservation of crestal bone by implant design. A comparative study in minipigs. Clin Oral Implants Res. 2013 Mar;24(3):243-9. Epub 2012 Jun 19. — Ikarashi Y et al. Improved biocampatibility of Titanium-Zirkonium (Ti-Zr) alloy: Tissue reaction and sensitization to Ti-Zr alloy compared with pure Ti and Zr in rat implantation study. Materials Transaction, 2005 46, 10, 2260-2267. — Jung RE et al. The influence of non-matching implant and abutment diameters on radiographic crestal bone levels in dogs. J Periodontol. 2008 Feb;79(2):260-70. — Kopf BS et al. The role of nanostructures and hydrophilicity in osseointegration: In-vitro protein-adsorption and blood-interaction studies. J Biomed Mater Res A. 2015 Aug;103(8):2661-72. Epub 2015 Feb 11. — Lang NP et al. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin Oral Implants Res. 2011 Apr;22(4):349-56. — Meredith N. Assessment of implant stability as a prognostic determinant. Int J Prosthodont. 1998 Sep-Oct;11(5):491-501. — Millenium Research Group (2015). Dental Implants & Final Abutments 2014 and 2015. Millennium Report, Pg 69. — Molly L. Bone density and primary stability in implant therapy. Clin Oral Implants Res. 2006 Oct;17 Suppl 2:124-35. — Oates TW et al. Enhanced implant stability with a chemically modified SLA surface: a randomized pilot study. Int J Oral Maxillofac Implants. 2007 Sep-Oct;22(5):755-60. — Rokn A et al. Evaluation of stability changes in tapered and parallel wall implants: a human clinical trial. J Dent (Tehran). 2011 Fall;8(4):186-200. Epub 2011 Dec 20. — Santing HJ et al. Performance of the Straumann Bone Level Implant system for anterior single-tooth replacements in augmented and nonaugmented sites: a prospective cohort study with 60 consecutive patients. Clin Oral Implants Res. 2013 Aug;24(8):941-8. Epub 2012 Apr 30. — Schwarz F et al. Effects of surface hydrophilicity and microtopography on early stages of soft and hard tissue integration at non-submerged titanium implants: an immunohistochemical study in dogs. J Periodontol. 2007 Nov;78(11):2171-84. — Schwarz F et al. Bone regeneration in dehiscence-type defects at non-submerged and submerged chemically modified (SLActive) and conventional SLA titanium implants: an immunohistochemical study in dogs. J Clin Periodontol. 2008 Jan;35(1):64-75. Epub 2007 Nov 21. — Shalabi MM et al. The effects of implant surface roughness and surgical technique on implant fixation in an in vitro model. Clin Oral Implants Res. 2006 Apr;17(2):172-8. — Steinemann SG. Titanium--the material of choice? Periodontol 2000. 1998 Jun;17:7-21. — Stoker GT et al. Immediate loading of two implants with a mandibular implant-retained overdenture: a new treatment protocol. Clin Implant Dent Relat Res. 2011 Dec;13(4):255-61. Epub 2009 Aug 3. — Szmukler-Moncler S. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. J Biomed Mater Res. 1998 Summer;43(2):192-203. — Wen B et al. The osseointegration behavior of titanium-zirconium implants in ovariectomized rabbits. Clin Oral Implants Res. 2014 Jul;25(7):819-25. Epub 2013 Feb 21. — Zhao G et al. High surface energy enhances cell response to titanium substrate microstructure. J Biomed Mater Res A. 2005 Jul 1;74(1):49-58.
International Headquarters Institut Straumann AG Peter Merian-Weg 12 CH-4002 Basel, Switzerland Phone +41 (0)61 965 11 11 Fax +41 (0)61 965 11 01
Straumann North American Headquarters Straumann USA, LLC 60 Minuteman Road Andover, MA 01810 Phone 800/448 8168 (US) 800/363 4024 (CA) Fax 978/747 2490 www.straumann.us www.straumann.ca
© Straumann USA, LLC 2015. All rights reserved. Straumann® and/or other trademarks and logos from Straumann® that are mentioned herein are the trademarks or registered trademarks of Straumann Holding AG and/or its affiliates. All rights reserved.