Embed Size (px)
Citation preview
Strategies & Principles ofCommunity Based PreventionCommunity Based Prevention
Kevin P. Haggerty, Ph.D.Director
Social Development Research Group,
School of Social Work
Objectives
• What are the key principles guiding prevention efforts?– Risk Factors
– Protective Factors– Protective Factors
– Evidence Based Programs
• How can communities use the research base for prevention?– Communities that Care
3
4
Community Prevention Guidedby Prevention Science
• Community owned and operated• Data Driven: Ongoing monitoring of risk and
protective factors –use your surveys
• Evidence Based: adoption of effective programs– Evaluations of unproven programs are required and – Evaluations of unproven programs are required and
supported.
• Outcome Focused: reductions in community levels of adolescent risk taking behavior
• Sustainable• Sound Investment
35 Years of Research Advances
1. We know what predicts many negative developmental outcomes as well as behavioral health.
2. We know what works to change those 2. We know what works to change those predictors and prevent behavioral problems in our youth.– Experimental trials have identified over 50 effective
interventions for promoting behavioral health and preventing negative developmental outcomes.

King County Best Startskingcounty.gov.beststarts
6
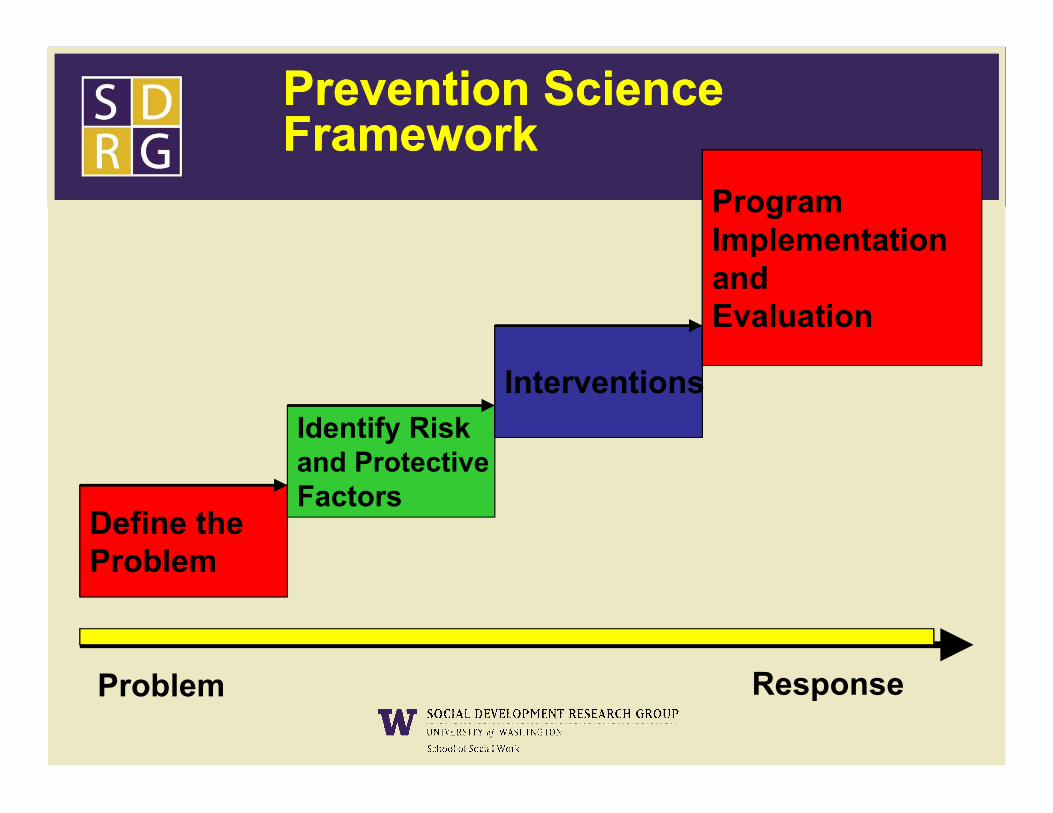
InterventionsInterventions
Program Implementation and Evaluation
Prevention SciencePrevention ScienceFrameworkFramework
Define the Problem
Identify Riskand ProtectiveFactors
Problem Response
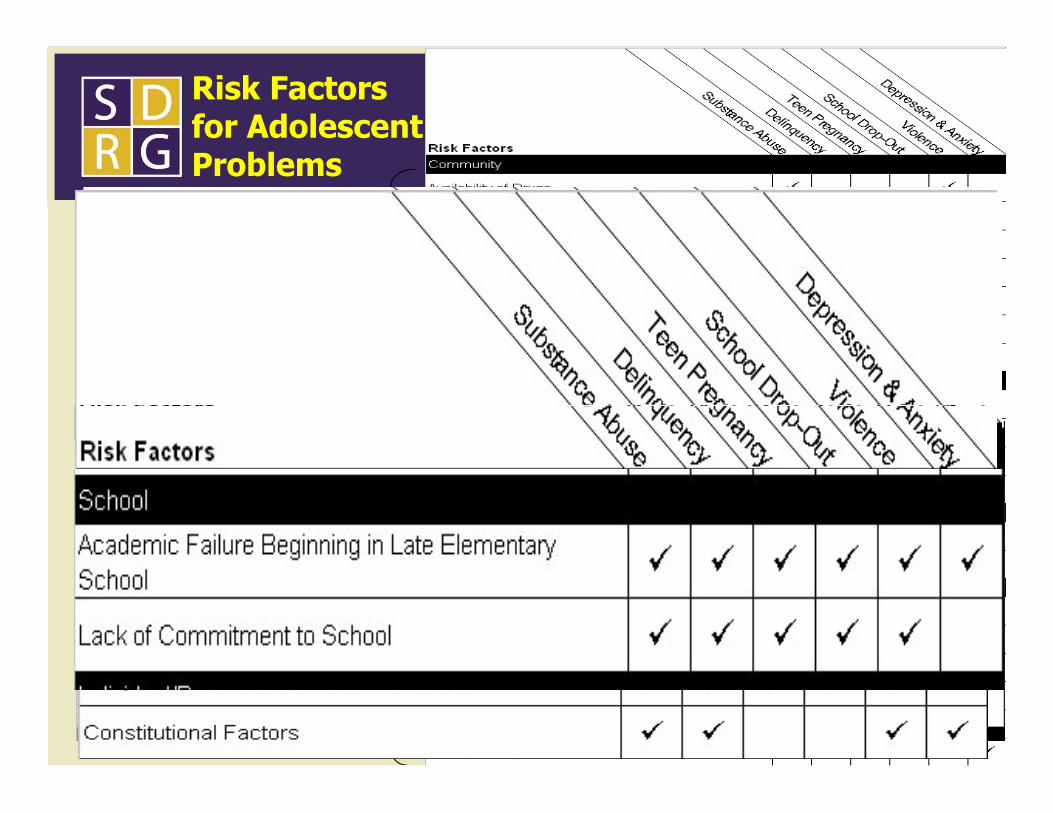
Community
Risk Factors for Adolescent Problems
8
Family
School
Individual/Peer
Protective Factors
Individual Characteristics– High Intelligence– Resilient Temperament– Competencies and Skills – Competencies and Skills
In each social domain (family, school, peer group and neighborhood)– Prosocial Opportunities– Reinforcement for Prosocial Involvement– Bonding– Healthy Beliefs and Clear Standards

The Social Development Model—Five elements of Protection
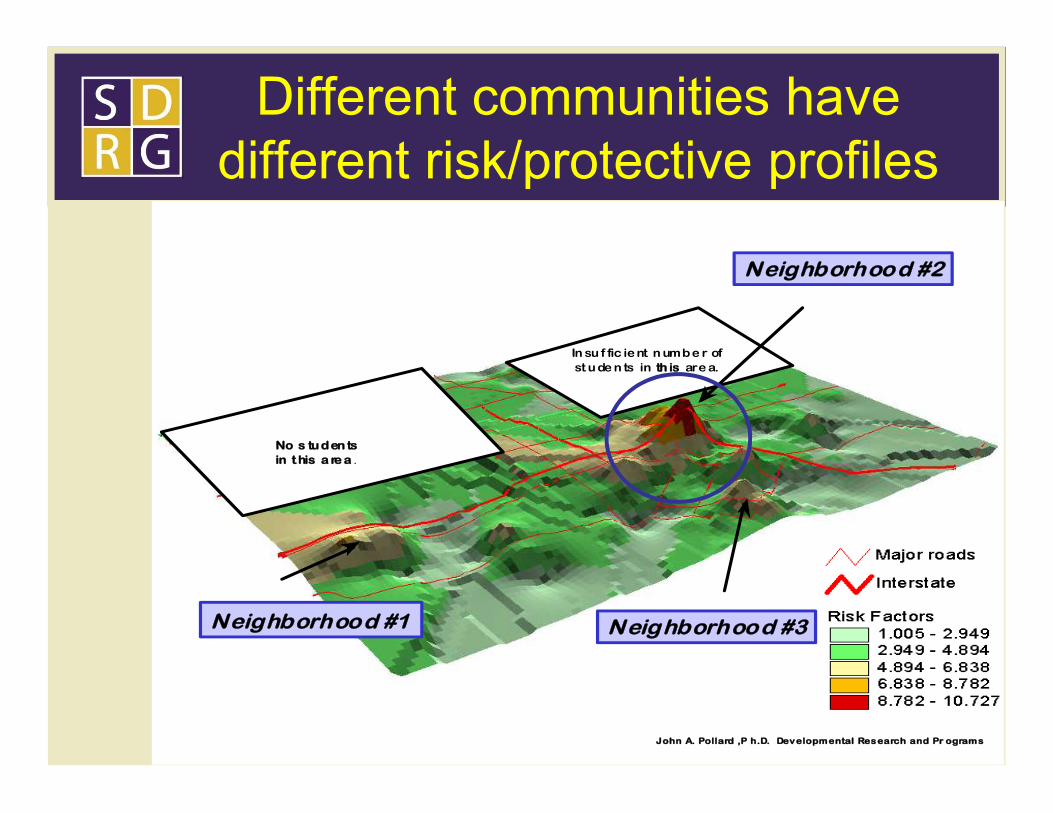
Different communities havedifferent risk/protective profiles
In su f fic ie nt n umbe r ofst u de n ts in th is are a.
Neighborhood #2
12John A. Pollard , P h.D. Dev elopmental Res earch and Pr ogram s
No s tu den tsin t his a re a .
Neighborhood #1 Neighborhood #3
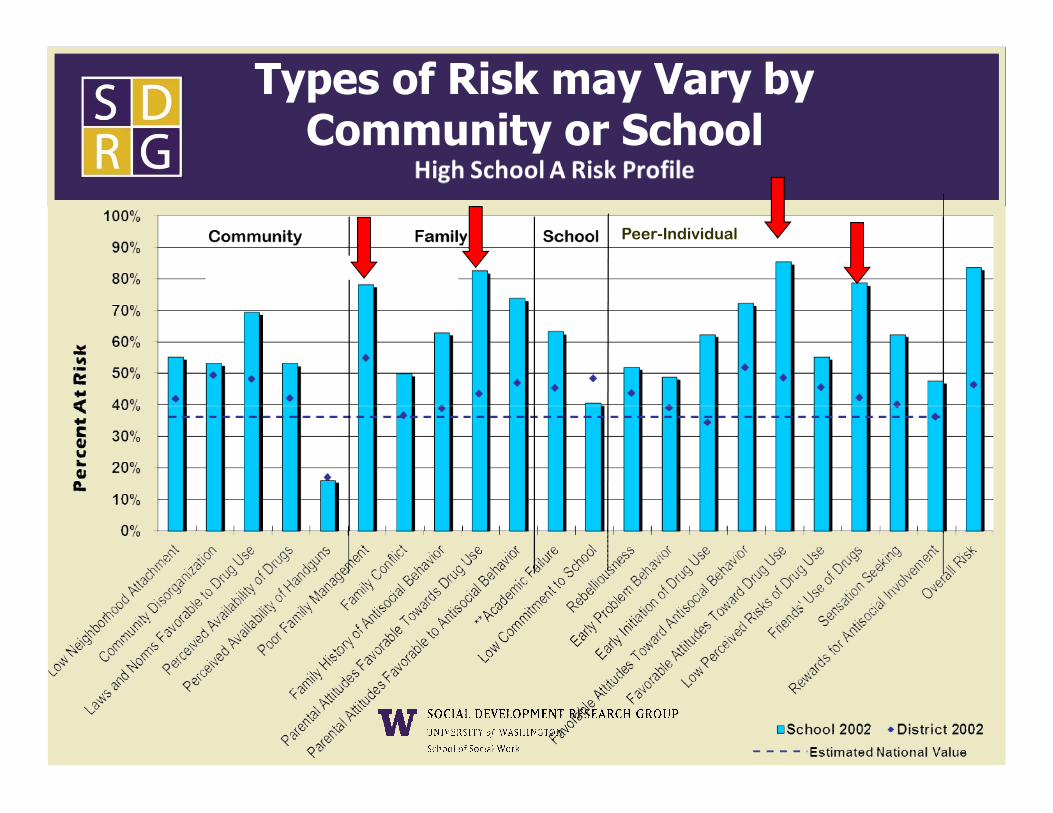
Peer-Individual
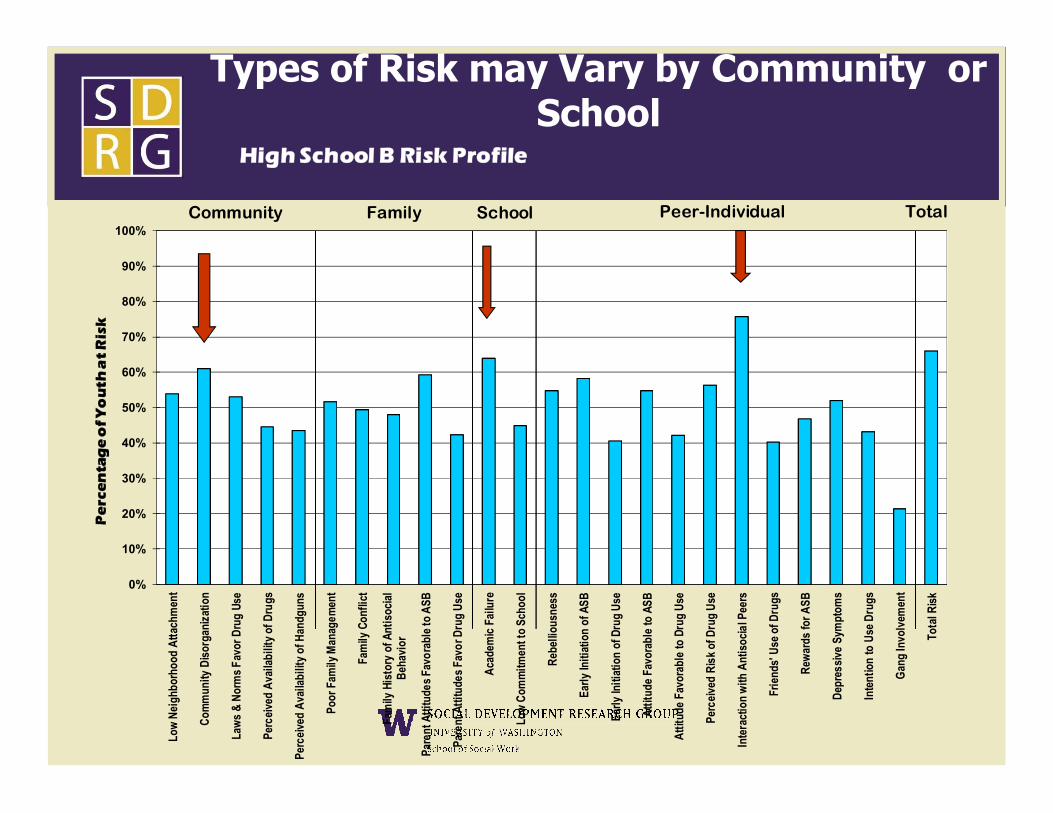
Types of Risk may Vary by Community or School
50%
60%
70%
80%
90%
100%
High School B Risk Profile
Community Family School Peer-Individual Total
Pe
rce
nta
ge
of
Yo
uth
at
Ris
k
Types of Risk may Vary by Community or School
0%
10%
20%
30%
40%
50%
Low
Nei
ghbo
rhoo
d A
ttach
men
t
Com
mun
ity D
isor
gani
zatio
n
Law
s &
Nor
ms
Favo
r Dru
g Us
e
Perc
eive
d A
vaila
bilit
y of
Dru
gs
Perc
eive
d A
vaila
bilit
y of
Han
dgun
s
Poor
Fam
ily M
anag
emen
t
Fam
ily C
onfli
ct
Fam
ily H
isto
ry o
f Ant
isoc
ial
Beh
avio
r
Pare
nt A
ttitu
des
Favo
rabl
e to
ASB
Pare
nt A
ttitu
des
Favo
r Dru
g U
se
Aca
dem
ic F
ailu
re
Low
Com
mitm
ent t
o Sc
hool
Reb
ellio
usne
ss
Early
Initi
atio
n of
ASB
Early
Initi
atio
n of
Dru
g U
se
Atti
tude
Fav
orab
le to
ASB
Atti
tude
Fav
orab
le to
Dru
g U
se
Perc
eive
d R
isk
of D
rug
Use
Inte
ract
ion
with
Ant
isoc
ial P
eers
Frie
nds'
Use
of D
rugs
Rew
ards
for A
SB
Dep
ress
ive
Sym
ptom
s
Inte
ntio
n to
Use
Dru
gs
Gan
g In
volv
emen
t
Tota
l Ris
k
Pe
rce
nta
ge
of
Yo
uth
at
Ris
k
1. In every sphere
2. Same factors predict many well-being outcomes
3. Addressing one can impact many outcomes
Five key points about risk andprotective factors?
FamilySchool
15
impact many outcomes
4. Operate in the same way across gender, race and ethnic, socio economic and regions
5. More protection = Fewer problemsMore risk = More problems
Individual/Peer
Community
Evidence Based Programs: Whatbenefits do proven programs offer?
1. Improve child well-being at a population level
2. Stronger and more consistent positive outcomes for children and positive outcomes for children and youth in the community
3. Strong ethical argument – avoid potential harmful effects
4. Potential cost savings to taxpayers and society 16

Evidence Based Program Examples: Risk focused programs address variety
of outcomes
Strong African American Families
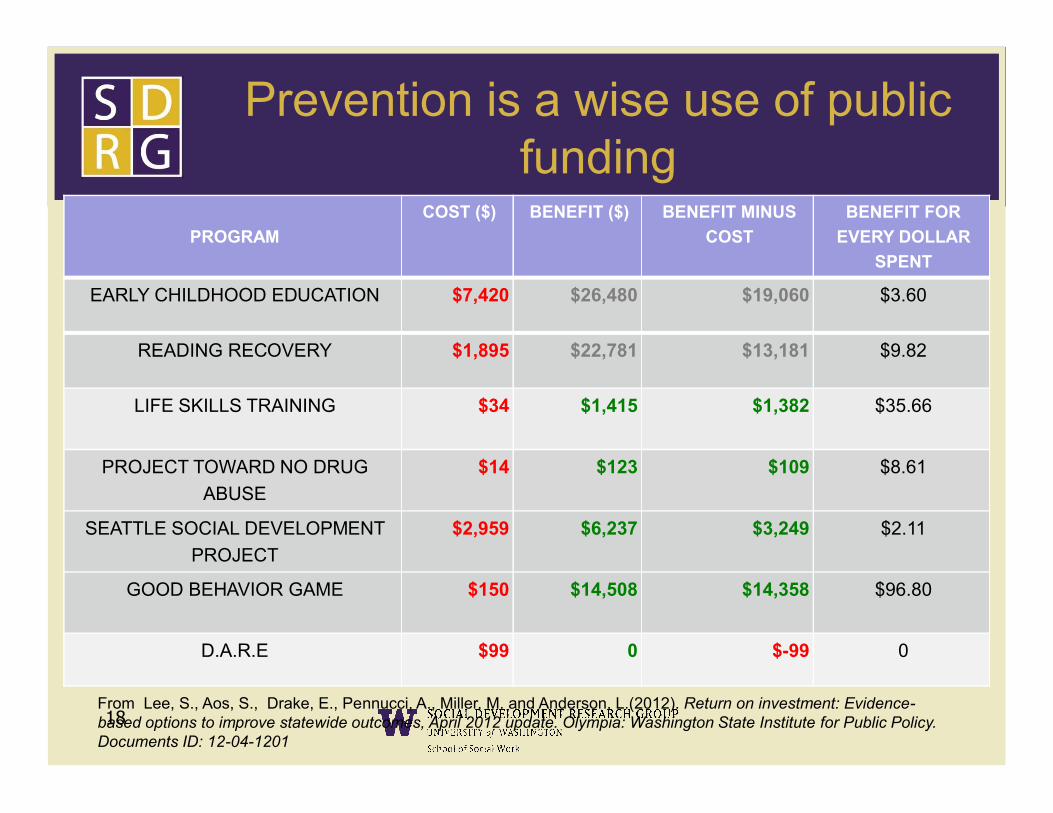
Prevention is a wise use of publicfunding
PROGRAM
COST ($) BENEFIT ($) BENEFIT MINUS
COST
BENEFIT FOR
EVERY DOLLAR
SPENT
EARLY CHILDHOOD EDUCATION $7,420 $26,480 $19,060 $3.60
READING RECOVERY $1,895 $22,781 $13,181 $9.82
LIFE SKILLS TRAINING $34 $1,415 $1,382 $35.66
From Lee, S., Aos, S., Drake, E., Pennucci, A., Miller, M. and Anderson, L.(2012). Return on investment: Evidence-based options to improve statewide outcomes, April 2012 update. Olympia: Washington State Institute for Public Policy. Documents ID: 12-04-1201
18
LIFE SKILLS TRAINING $34 $1,415 $1,382 $35.66
PROJECT TOWARD NO DRUG
ABUSE
$14 $123 $109 $8.61
SEATTLE SOCIAL DEVELOPMENT
PROJECT
$2,959 $6,237 $3,249 $2.11
GOOD BEHAVIOR GAME $150 $14,508 $14,358 $96.80
D.A.R.E $99 0 $-99 0

How does a program earn thedistinction of being proven?
Attain strong evidence of
positive program outcomes
Produce indicators
of positive
• Conduct evaluation with random assignment
• Conduct evaluation with random assignment Ensure
Obtain evidence of
positive program
outcomes
19
Develop a strong
program design
• Carry out evaluation with a comparison group
• Conduct regression analysis (quasi-experimental design )
• Perform multiple pre- and post -evaluations
• Meta-analysis
• Carry out evaluation with a comparison group
• Conduct regression analysis (quasi-experimental design )
• Perform multiple pre- and post -evaluations
• Meta-analysis
positive outcomes
assignment (experimental design)
• Carry out multiple evaluations with strong comparison group (quasi-experimental design)
assignment (experimental design)
• Carry out multiple evaluations with strong comparison group (quasi-experimental design)
• Conduct pre- and post-intervention evaluation
• Conduct pre- and post-intervention evaluation
• Evaluate program quality and process
• Establish continuous improvement system
• Evaluate program quality and process
• Establish continuous improvement system
Ensure fidelity of
Implement-ation
• Create logic model and replication materials
• Create logic model and replication materials
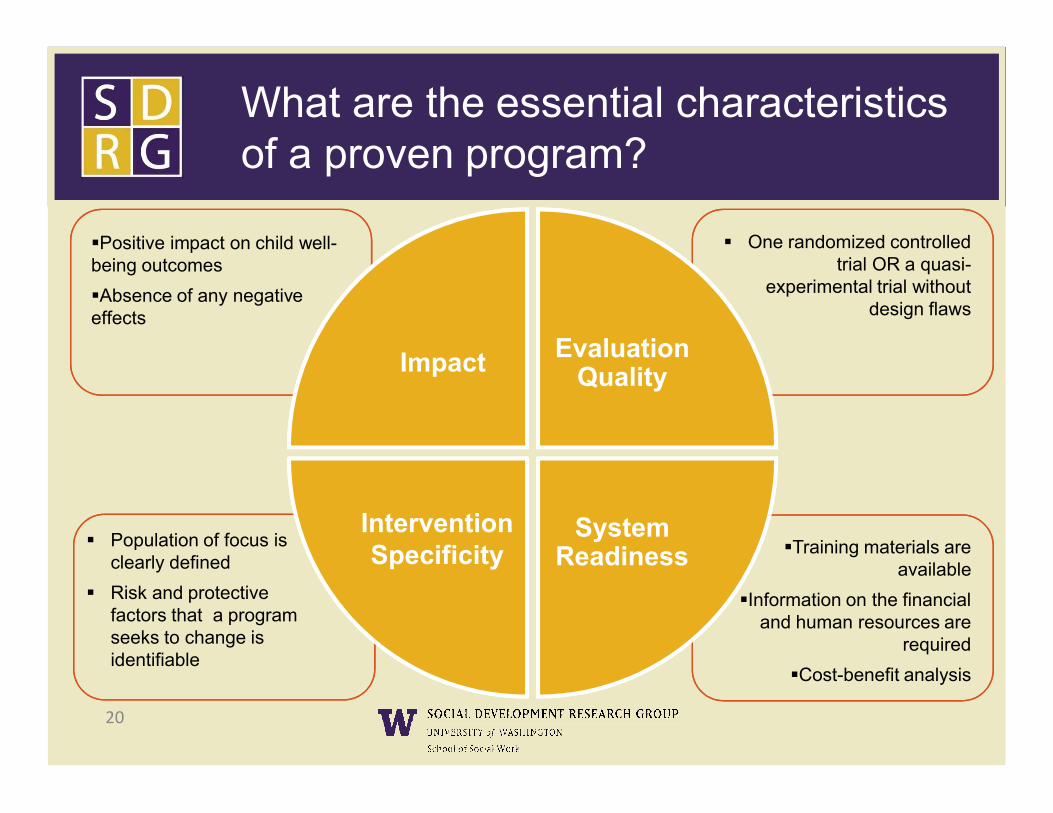
What are the essential characteristics of a proven program?
Impact Evaluation Quality
Positive impact on child well-being outcomes
Absence of any negative effects
One randomized controlled trial OR a quasi-
experimental trial without design flaws
20
System Readiness
Intervention Specificity
Population of focus is clearly defined
Risk and protective factors that a program seeks to change is identifiable
Training materials are available
Information on the financial and human resources are
required
Cost-benefit analysis
Evidence Based Programs….Where to Turnhttp://www.colorado.edu/cspv/blueprints/
Why Universal Programming?
22
The Challenge
How can we take tested and effective
23
effective prevention programs to scale?
What Has NOT Worked in Community Based Preventive Trials ?
Providing resources to support community
coalitions without a structure or process to ensure
• clearly defined, focused, and manageable goals based in data, with corresponding high-quality data sources to data, with corresponding high-quality data sources to monitor progress;
• use of tested and effective programs, with careful attention to monitoring of implementation quality and fidelity;
• evaluation of program impacts on outcomes meaningful to the community(Hallfors et al. (2002); Klerman et al. (2005); Merzel & D'Afflitti, (2003).
24
What Has Worked in Community-Based Prevention Trials?
• Preventive interventions focused on malleable community level risk / protective factors. factors.
• Strategies that build local partnerships or coalitions to promote use of tested and effective programs to address community
prevention needs.
25
Examples
• Communities Mobilizing for Change on Alcohol- Wagenaar
• Community Trials Intervention to Reduce High Risk Drinking- Holder
26
High Risk Drinking- Holder
• Project Northland- Perry
• Midwestern Prevention Project –Pentz
• PROSPER-Spoth/Greenberg
• Communities that Care— Hawkins, et al.
Common Elements ofCollective Impact
• Common Agenda
• Shared Measurement System• Shared Measurement System
• Mutually Reinforcing Activities
• Continuous Communications
• Backbone Support Organizations
27
Kania & Kramer, 2011
Communities Communities That Care That Care Develops Capacity toDevelops Capacity to
Build a coalition of diverse stakeholders to achieve collective impact.
Assess and prioritize for action- risk, protection, and behavioral health outcomes.
28
outcomes.
Strengthen protection and address priority risks with effective preventive interventions.
Sustain high fidelity implementation of preventive interventions to reach all those targeted.
CTC Overview Video
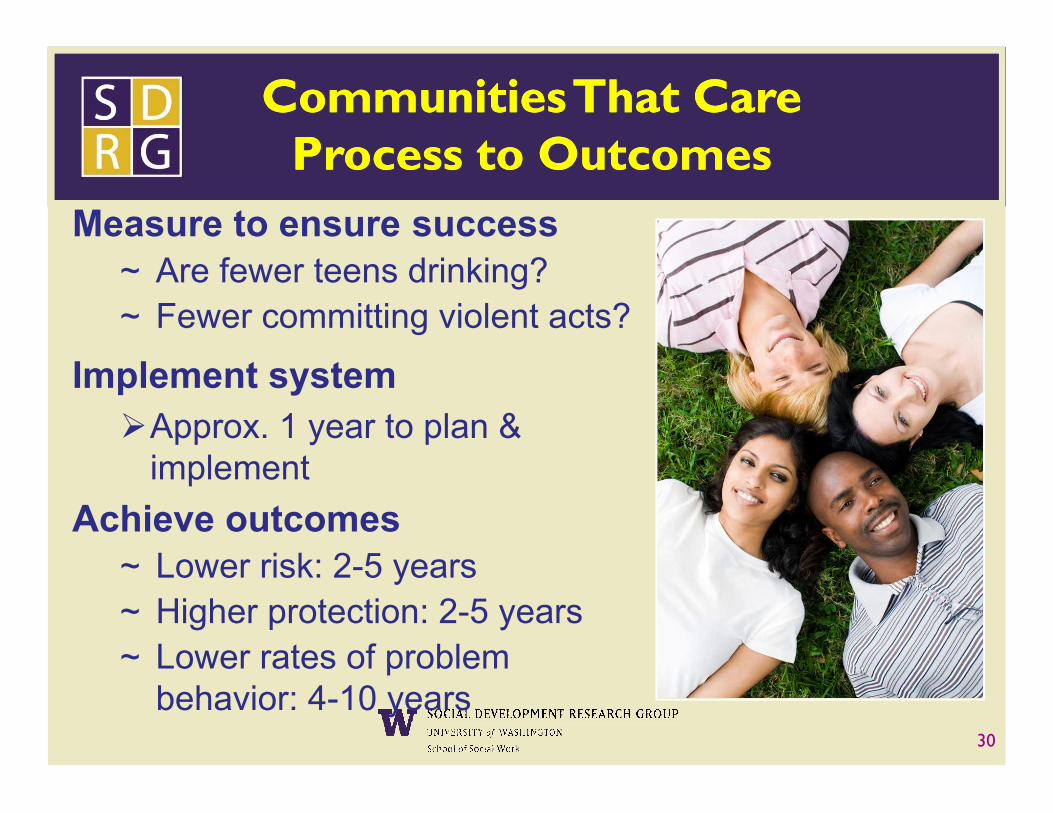
Measure to ensure success~ Are fewer teens drinking? ~ Fewer committing violent acts?
Implement system
Communities Communities That Care That Care Process to OutcomesProcess to Outcomes
30
Approx. 1 year to plan & implement
Achieve outcomes~ Lower risk: 2-5 years~ Higher protection: 2-5 years~ Lower rates of problem
behavior: 4-10 years
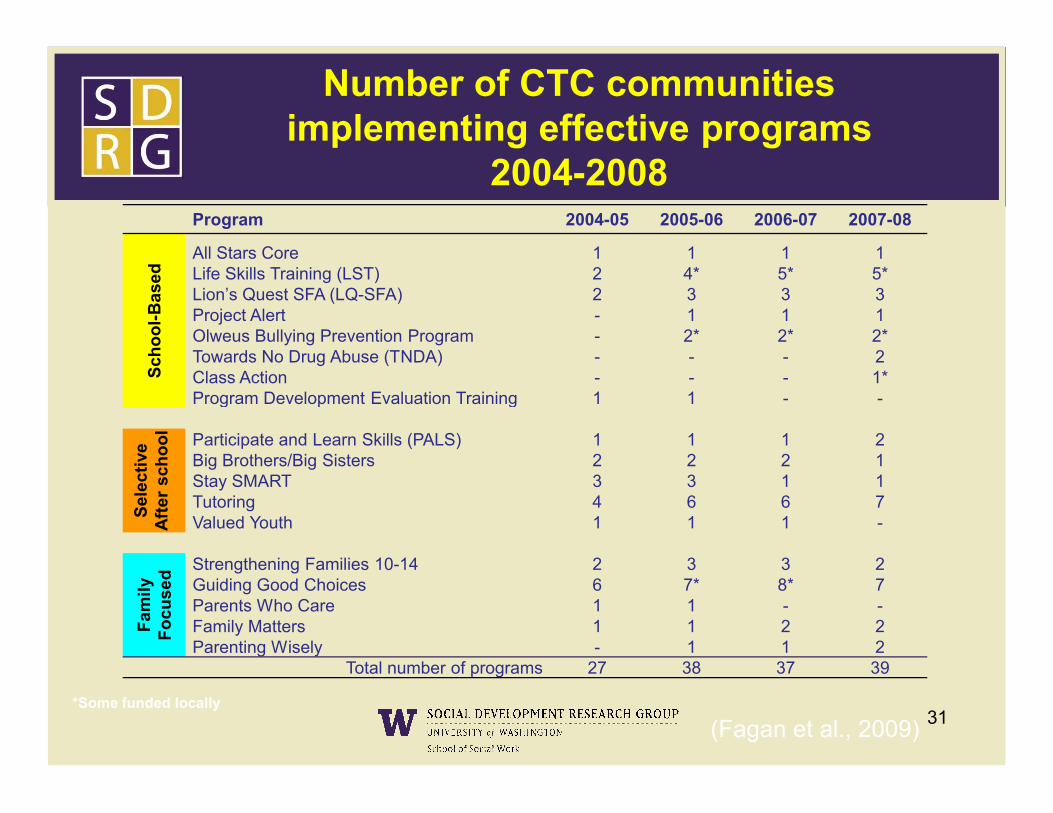
Number of CTC communities implementing effective programs
2004-2008Program 2004-05 2005-06 2006-07 2007-08
Sch
oo
l-B
ased
All Stars Core 1 1 1 1Life Skills Training (LST) 2 4* 5* 5*Lion’s Quest SFA (LQ-SFA) 2 3 3 3Project Alert - 1 1 1Olweus Bullying Prevention Program - 2* 2* 2*Towards No Drug Abuse (TNDA) - - - 2Class Action - - - 1*Program Development Evaluation Training 1 1 - -Program Development Evaluation Training 1 1 - -
Sel
ecti
veA
fter
sch
oo
l
Participate and Learn Skills (PALS) 1 1 1 2Big Brothers/Big Sisters 2 2 2 1Stay SMART 3 3 1 1Tutoring 4 6 6 7Valued Youth 1 1 1 -
Fam
ily
Fo
cuse
d
Strengthening Families 10-14 2 3 3 2Guiding Good Choices 6 7* 8* 7Parents Who Care 1 1 - -Family Matters 1 1 2 2Parenting Wisely - 1 1 2
Total number of programs 27 38 37 39
31*Some funded locally
(Fagan et al., 2009)
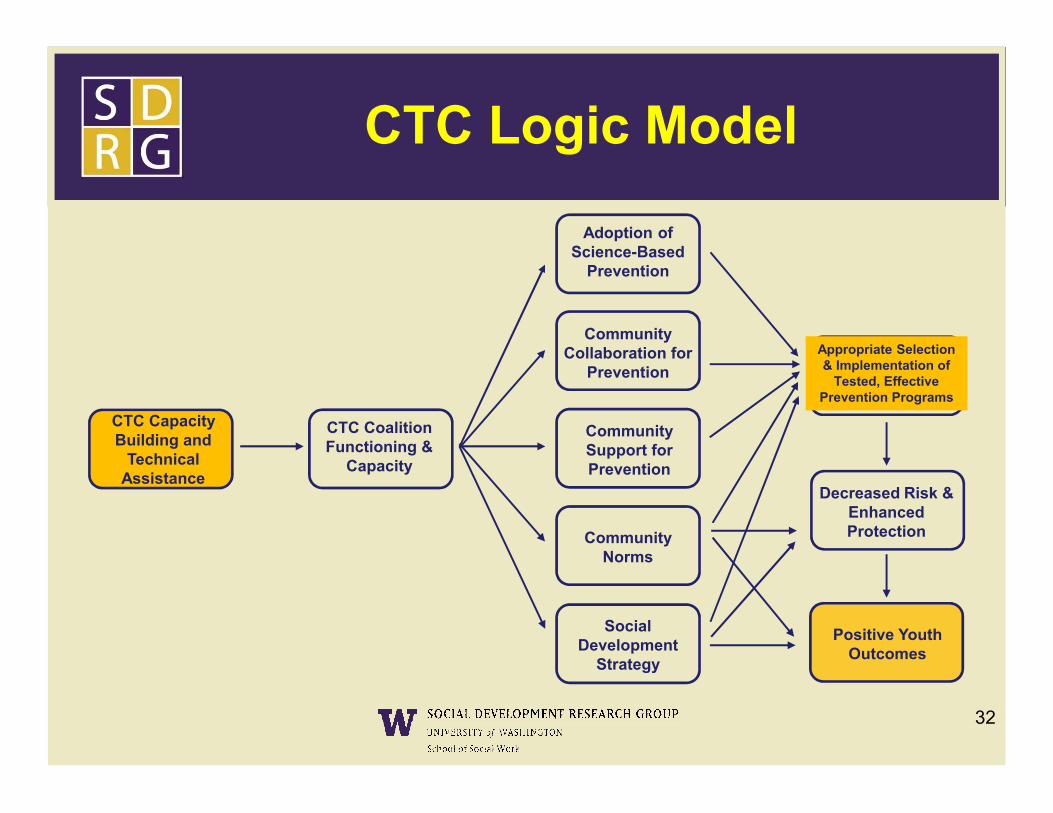
Adoption of Science-Based
Prevention
Community Collaboration for
Prevention
Appropriate Selection & Implementation of
Tested, Effective Prevention Programs
CTC Logic Model
32
CTC Coalition Functioning &
Capacity
Community Norms
Social Development
Strategy
Community Support for Prevention
Positive Youth Outcomes
Decreased Risk & Enhanced Protection
CTC Capacity Building and
Technical Assistance
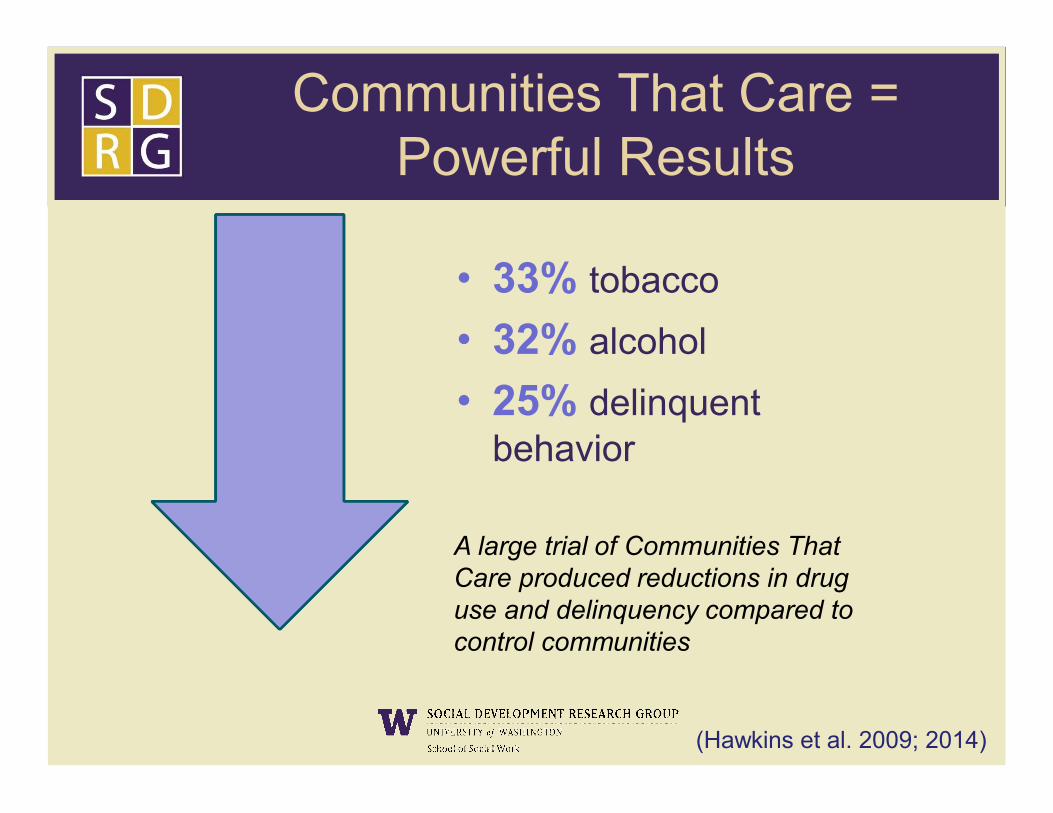
Communities That Care =Powerful Results
• 33% tobacco
• 32% alcohol
• 25% delinquent
A large trial of Communities That Care produced reductions in drug use and delinquency compared to control communities
• 25% delinquent behavior
(Hawkins et al. 2009; 2014)
Sustained Effects One Year after Intervention Funding Ended
• In the panel, compared to controls, 10th graders from CTC communities had:– Lower levels of targeted risk factors.
– Less initiation of delinquent behavior, alcohol use, and cigarette use.alcohol use, and cigarette use.
– Lower prevalence of past-month cigarette use.
– Lower prevalence of past-year delinquency
– Lower prevalence of past-year violence.
Hawkins et al., 2012, Archives of Pediatrics and Adolescent Medicine
Is the benefit worth the cost of CTC?
35

Yes!
Communities That Care is Cost-Beneficial –even when effect sizes are reduced by 50%
For every $1 spent $4.23 return on investment
36
For every $1 spent $4.23 return on investment~ Low risk of negative investment return
Largest share of benefits was from delinquency prevention
Findings sustained from 8th through 12th grade

The Social Development Model—Five elements of Protection
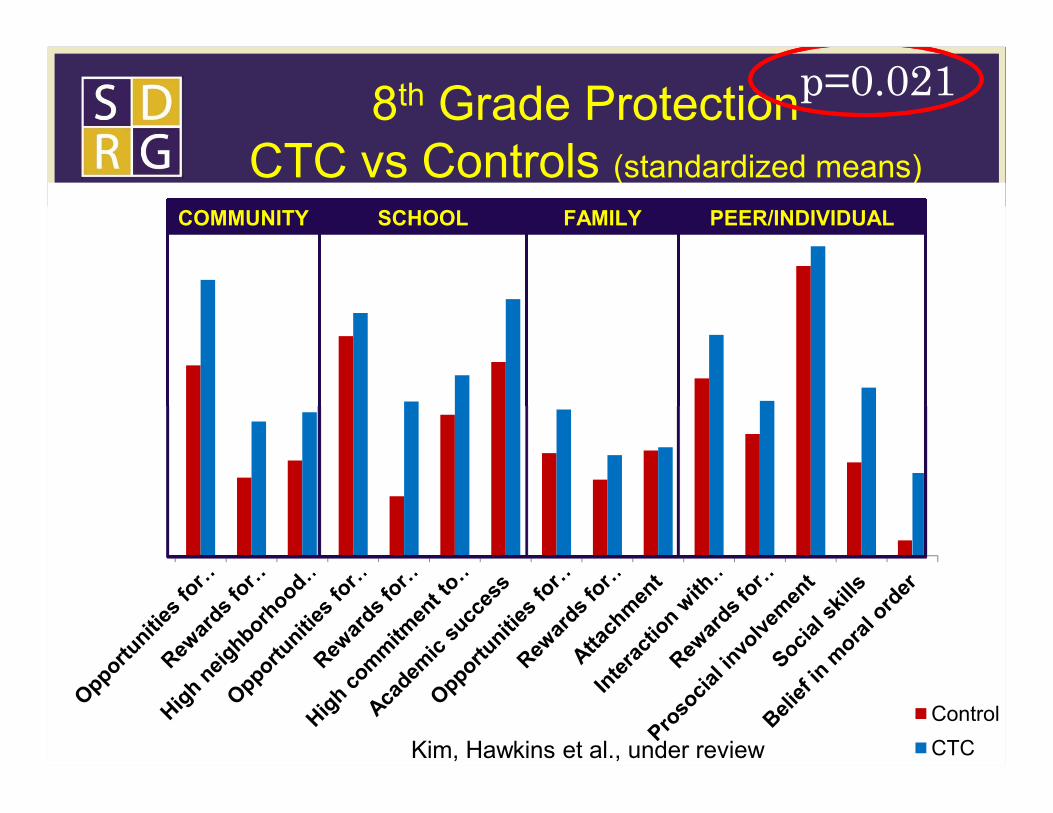
8th Grade ProtectionCTC vs Controls (standardized means)
COMMUNITY SCHOOL FAMILY PEER/INDIVIDUAL
p=0.021
38Control
CTCKim, Hawkins et al., under review
39
A Future Guided by PreventionScience Principles
• Community owned and operated• Data Driven: Ongoing monitoring of risk and
protective factors –use your surveys
• Evidence Based: adoption of effective programs– Evaluations of unproven programs are required and – Evaluations of unproven programs are required and
supported.
• Outcome Focused: reductions in community levels of adolescent risk taking behavior
• Sustainable• Sound Investment

The eCTC ImplementationSupport System
• CTC workshops are locally facilitated and streamed as communities are ready for them in an accessible format.
• Web streamed workshops allow flexibility in scheduling the CTC workshops, refresher workshops, and training for new community leaders and coalition members.
40
ConclusionsPrevention Science Advances
• Behavior problems are significant causes of adolescent morbidity and mortality
• Risk and protective factors that predict behavior problems are potential targets for intervention
• There is sufficient evidence from controlled trials that policies • There is sufficient evidence from controlled trials that policies and programs can prevent adolescent behavior problems
• Community based prevention should include a combination of locally prioritized and chosen efficacious preventive policies and programs
• CTC achieved intervention fidelity and impact at scale

www.communitiesthatcare.net
42
Kevin P. Haggerty, Ph.D.Director of Research
School of Social [email protected]





























