Embed Size (px)
Citation preview
The Continuing Education You Want. Quality Content, Live Near You, or Online 24/7/365
Upgrade from this workshop to an “All Access” Subscription Plan, the only plan with unlimited Live/In-Person and Online CE Courses, for ONLY $100!
HURRY! This limited time offer expires 30 days after today’s workshop!
Call (800) 433-9570 to upgrade today!
“All Access” Subscription Upgrade - ONLY $100!
Fall Prevention StrategiesEvidence-Based Tools to Reduce Re-Hospitalization and Maximize Functional Outcomes
Presented by Brandi Singleton, PT, DPT, CCI
WelcomeWelcome to today’s Summit Professional Education workshop! We are committed to providing you with high-quality instructors and content, and look forward to showing you this commitment today. Additionally, our Customer Service team is only a phone call or email away to provide you with the highest level of service available.
After today’s workshop, you’ll receive an email link to an online survey. Please be candid as each survey is reviewed by our workshop development team. We also appreciate any topic ideas you recommend for future workshops – your suggestions matter! We thank you for being a customer of Summit Professional Education and hope to see you again soon.
Enjoy the workshop!
Disclosures• Guidelines exist whereby all speakers must disclose any relevant relationships. All relevant relationships are published in the
workshop brochure.
• Summit Professional Education does not accept commercial support of any kind.
• Approvals of this activity refer only to continuing education activities and do not imply that there is real or implied endorsement of any product, service, or company referred to in this activity nor of any company subsidizing costs related to the activity.
• You will be notified if a presentation relates to any product used for a purpose other than that for which it was approved by the U.S. Food and Drug Administration.
IMPORTANT:Customer Service is available weekdays between 6AM-6PM Central time at 800-433-9570. For weekend calls, contact Customer Service on the following Monday.
Workshop FAQsWhat are Summit’s Workshop Completion Requirements?
To receive a Certificate of Completion, participants must:1. Pay workshop fee2. Sign in3. Attend the entire workshop (partial credit is not available)4. Complete a program evaluation (required), Attendee Information Form (if upgrading or not pre-registered), CE Supplements
(if applicable), and ASHA Participation Form (if applicable).5. Sign out
When Will I Receive a Certificate of Completion?Certificates will be made available at the end of today’s workshop for those who registered at least five business days prior to the workshop. If your certificate is not present, please fill out an Attendee Information Form. You will receive your certificate within 28 days via email or address you have provided.
What If There’s an Emergency and I Need to Leave Early?You may certainly leave the workshop at any point. Please call Summit Customer Service at your earliest convenience at 800-433-9570 (available 6AM-6PM Central) to discuss options. Please leave a message on weekends or after-hours.
What If I Need a Receipt for Reimbursement?If you need a receipt, other than the initial confirmation email you were sent when you registered, please contact Summit Customer Service at 800-433-9570 (available 6AM-6PM Central) with your receipt request. Please leave a message on weekends or after-hours.
How Can I Become a Summit “All Access” Subscriber?Upgrading is easy! As a special offer, only good for 30 days after this live course, you can upgrade to Summit’s “All Access” Subscription - normally priced at $299.99 - for just $100! You’ll unlock unlimited Live/In-Person Course attendance and unlimited Online Video and Text Courses for the next 12 months.
The Continuing Education You Want!
Tight Budgets? Group Savings!• 5 or More Professionals that Need CE? Extra Discounts on:
Not an “All Access” Subscriber?
Unlimited attendance to all 2,200+ yearly Live/In-Person CE Courses
Unlimited access to all 200+ Online Video and Text CE Courses
Yearly price of ONLY $29999 - Over 60% savings on annual CE cost
Upgrade within 30 days of today’s workshop for ONLY $10000!
“ALL ACCESS” UPGRADE
Upgrade from this workshop to an “All Access” plan.Call (800) 433-9570 or see the Attendee Information Form to upgrade today!
ONLY $100
SPECIAL GROUP SAVINGS OFFERS
Save time and money with Group Savings at Summit. With multiple options, we can tailor what works best for you. Call (615) 376-8890 for more details!
SAVE EXTRA
10-30%
• “All Access” and “Online Access” Subscriptions• Single course purchase for any Live/In-Person or Online CE Course
• Private CE Course: Pick the instructor and topic to be held privately• Public Hosting: You provide the location for a CE course open to the public
• Want CE Offered at Your Organization’s Location?
Instructor Please rate the following items on a SCALE of 1 (poor) to 5 (excellent)
Knowledge Base EffectivenessTeaching Ability Organization of Material
Objectives Please rate the following items on a SCALE of 1 (poor) to 5 (excellent)
After attending the program, how well do you feel you are able to:
PO Box 908 | Franklin, TN 37065Phone: 800-433-9570 | www.summit-education.com | Fax: (615) 376-8233
NAME: PROFESSIONAL TITLE: SETTING/POPULATION:
WORKSHOP CITY/STATE: DATE: INSTRUCTOR:
PROGRAM EVALUATION FORM
Workshop Facility/Registration Please rate the following items on a SCALE of 1 (poor) to 5 (excellent)
Content Please rate the following items on a SCALE of 1 (poor) to 5 (excellent)
Advertised Level of Material Appropriate
Lack of Bias or Commercialism
Questions/Concerns were Addressed Effectively
Relevance/Value of Information for Work
Content Matches Stated Objectives
Utility of Handouts/Visuals
Course Material Current Questions/Concerns were Addressed in a Timely Manner
Please comment on what was the most beneficial part of the program?
Meeting Location/Facility Conducive to Learning
Disability Accommodations Made Clear
Registration was User-Friendly
If you have any general comments on this workshop or instructor, please explain. You may use the back of this form to elaborate.
Fall Prevention StrategiesEvidence-Based Tools to Reduce Re-Hospitalization and Maximize Functional Outcomes
Brandi Singleton
ѩ 1. Identify three physiological contributors to falls in the elderly population.
ѩ 2. Utilize appropriate assessment tools for determining fall risk in the aging senior population.
ѩ 3. Implement treatment of balance deficits to prevent hospital re-admissions with or without cutting-edge equipment.
ѩ 4. Develop individualized exercise programs to improve strength and stability in older adults with balance deficits.
ѩ 5. Conduct environmental modifications on a shoestring budget to prevent falls in the home.
ѩ 6. Justify medical necessity and ensure reimbursement with accurate documentation of balance and strength training services.

CHECK ALL THAT APPLY:
I would like to upgrade to an “All Access” Subscription (additional steps below) I have not pre-registered and am a walk-in attendee I have pre-registered, but my name is not on the Sign-In/Sign-Out sheet I have pre-registered, but my certificate is missing My certificate is misspelled (please print corrected name/title on certificate and return to Instructor) I am a substitute for a registered attendee
CHECK: (Please attach; make payable to Summit Professional Education)
CREDIT CARD INFORMATION:
NAME ON CARD:
CREDIT CARD NUMBER:
EXPIRATION DATE: SECURITY CODE:
Payment Information (NO CASH)IMPORTANT: Certificate will not be processed until payment is verified.
COMPANY:
EMAIL:
HOME ADDRESS:
BILLING ADDRESS:
Attendee Information (PLEASE PRINT, ALL FIELDS REQUIRED)
AMOUNT: $ Walk-In Rate: $259.99 “All Access” Subscription: $299.99 Pre-Registered “All Access” Upgrade: $100.00
Summit “All Access” Subscription Plan - Opportunity to PurchaseYES! I want unlimited CE for a year!
$100.00 “All Access” Subscription Upgrade (pre-registered attendees only)
$299.99 “All Access” Subscription (not pre-registered attendee; this price includes today’s workshop)
I agree to the Summit Subscription Terms & Conditions (must be checked to process). By checking this box, you have agreed to the complete Summit Subscription Terms & Conditions. For your convenience, all subscriptions automatically renew until cancelled. Your renewal will be billed at the then current rate using your payment method on file. You can cancel your subscription pursuant to the terms of our cancellation policy by calling our Customer Service team at 800-433-9570. Your subscription is governed by our terms and conditions: https://summit-education.com/subscription/terms/.
IMPORTANT:Customer Service is available weekdays between 6AM-6PM Central time at 800-433-9570. For weekend calls, contact Customer Service on the following Monday.
Name of registered attendee: Order #
WORKSHOP CITY/STATE: DATE: INSTRUCTOR:
NAME: PROFESSIONAL TITLE:
CELL PHONE: DAY PHONE:
ATTENDEE INFORMATION FORM(FOR SUBSCRIPTION PURCHASE OR SPECIAL CIRCUMSTANCES)
Brandi Singleton

Workshop Notes

Workshop Notes

Workshop Notes
Fall�Prevention�Strategies
Evidence�Based�Tools�to�Reduce�Re�Hospitalizationand�Maximize�Functional�Outcomes
Presented�by:Brandi�Singleton,�PT,�DPT,CCI
1
Course�Objectives1. Understand�the�Impact�that�Falls�Have�on�the�
Healthcare�Industry2. Identify�Various�Contributors�to�Falls�in�the�
Geriatric�Population3. Administer�The�Best�Standardized�Assessment�
Tools�to�Track�Patient�Functional�Status4. Provide�Customized�Treatments�for�Patients�of�
Varying�Functional�Levels5. Teach�Essential�Skills�Needed�to�Reintegrate�Into�
Home�and�Community�Environments6. Master�Effective�and�Efficient�Documentation�
Based�on�the�Latest�Medicare�Guidelines.�2
What�impact�do�falls�have�on�the�healthcare�industry�as�a�whole?
3
Impact�of�Falls
• Each�year�~30%�of�adults�over�the�age�of�65�experience�a�fall
•20%�of�falls�result�in�serious�injury�requiring�visits�to�the�emergency�room
•40%�of�hospital�admissions�of�older�adults�are�a�result�of�falls
4
Impact�of�falls
• Falls�are�the�leading�cause�of�death�from�injury�in�older�adults
• Even�without�injury,�falls�often�lead�to�a�downward�spiral,�resulting�in�inactivity,�decreased�strength,�balance�problems,�and�decreased�independence
• $30�million�is�spent�annually�in�direct�and�indirect�medical�costs�related�to�falls
5
Role�of�Therapists�in�Falls�Prevention
• Evidence�suggests�that�falls�can�be�prevented�by:
• Screening�to�determine�risk�factors�
• Prescription�of�individualized�interventions�to�address�risk�factors
6
11
Identifying�and�understanding�risk�factors�for�falls�in�the�aging�senior�
population• Intrinsic�risk�factors
• Extrinsic�risk�factors
•Psychological�risk�factors
•Vestibular�Influences�on�balance�deficits7
Intrinsic�Risk�factors
• Visual�deficits
• Impaired�sensation
•Medication�side�effects
• Incontinence
• Proprioceptive�deficits
•Muscle�weakness
• Gait�impairments
• Neurological�deficits
8
Visual�Deficits
•Age�related�visual�changes• The�ability�of�the�eyes�to�adjust�to�change�in�lighting�diminishes�with�age�– more�time�required�to�adjust,�especially�with�transition�to�dark.
• Reduced�contrast�sensitivity�limits�perception�of�objects�in�environment
• Deficits�in�depth�perception� 9
Visual�Deficits
•Conditions�commonly�seen�in�the�aging�population:• Cataracts
• Glaucoma�
•Macular�degeneration
• Neurologic�Vision�Impairments10
Cataracts
• Eye�lens�progressively�becomes�more�opaque
•Presents�as�“cloudy”�or�”blurred�vision
•Can�be�effectively�treated�with�surgical�procedure
11
Glaucoma
• Caused�by�damage�to�the�optic�nerve
• Peripheral�vision�is�lost�first
•With�progression�medial�vision�also�lost�–presents�like�“tunnel�vision”
• There�is�no�cure�for�glaucoma�and�visual�losses�are�permanent 12
12
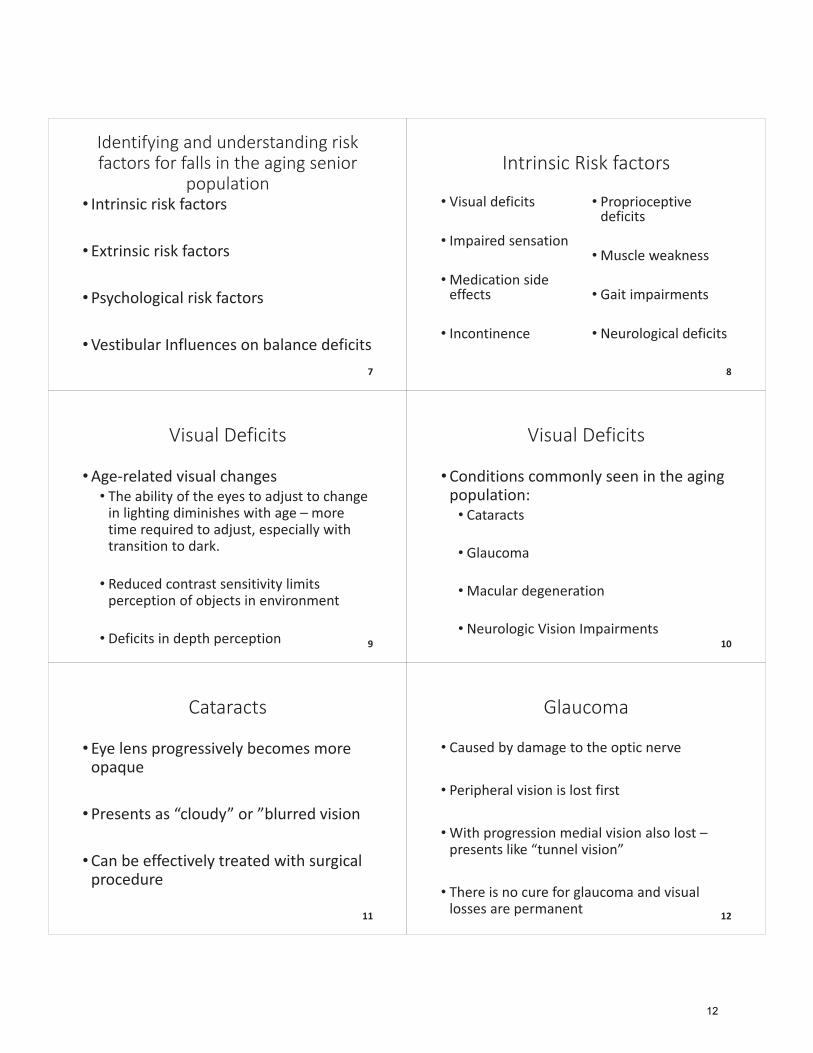
Macular�Degeneration• Damage�to�central�part�of�the�retina�(the�macula)• Early,�intermediate,�and�late�stages• Symptoms�typically�not�reported�until�late�stages
• Leads�to�”low�vision”• Difficulty�reading• Difficulty�recognizing�objects�and�facial�features
• Central�vision�is�completely�lost�in�advanced�stages�– legally�blind• Peripheral�vision�is�often�retained
13
Neurologic�Vision�Impairments
•Visual�field�cuts
•Visual�field�neglect
14
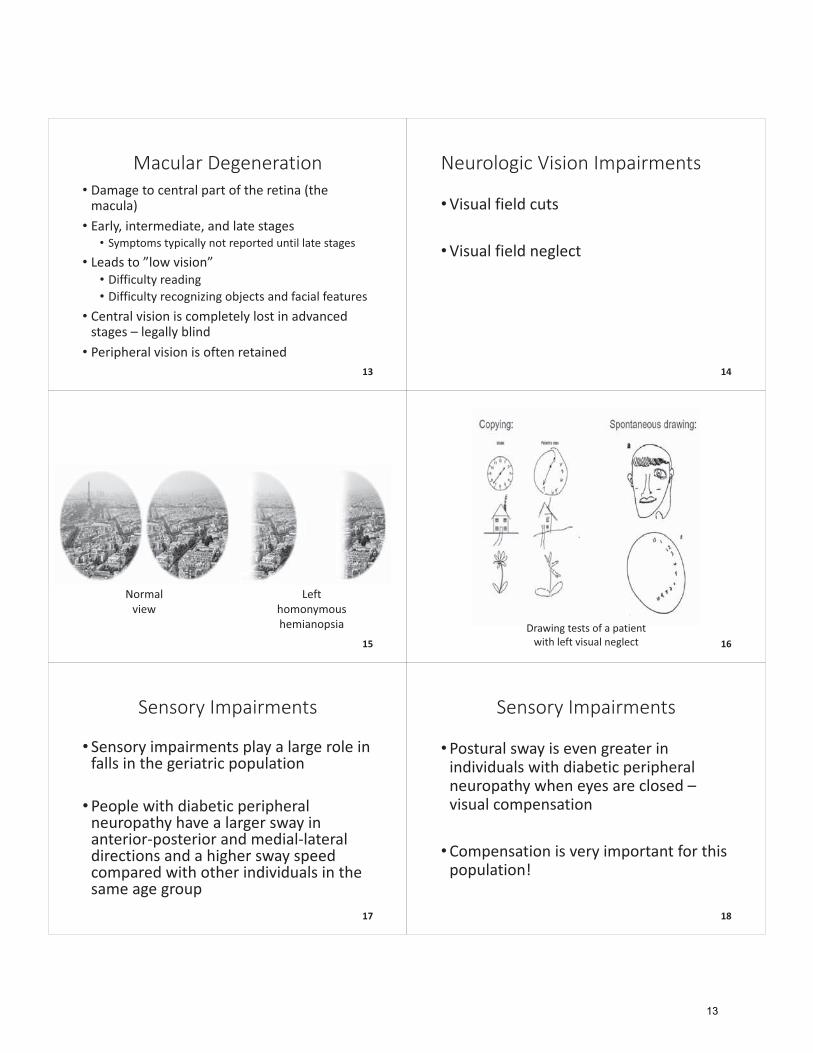
Left�homonymous�hemianopsia
Normal�view
15Drawing�tests�of�a�patient�with�left�visual�neglect 16
Sensory�Impairments
• Sensory�impairments�play�a�large�role�in�falls�in�the�geriatric�population
•People�with�diabetic�peripheral�neuropathy�have�a�larger�sway�in�anterior�posterior�and�medial�lateral�directions�and�a�higher�sway�speed�compared�with�other�individuals�in�the�same�age�group
17
Sensory�Impairments
•Postural�sway�is�even�greater�in�individuals�with�diabetic�peripheral�neuropathy�when�eyes�are�closed�–visual�compensation
•Compensation�is�very�important�for�this�population!
18
13
Double�Trouble!• Patients�who’s�sensory�deficits�are�related�to�diabetic�peripheral�neuropathy�(DPN)�often�also�have�visual�deficits�from�the�condition,�known�as�diabetic�retinopathy
• Now�the�individual�is�further�compromised�and�at�a�higher�risk�for�falls
• Proper�assistive�device�selection�is�very�important�when�this�set�of�symptoms�is�present*
19
Medication�Side�Effects
• Incidence�in�falls�increases�in�individuals�who�utilize:• Psychotropic�drugs
• Cardiac�drugs
• Polypharmacy• Use�of�two�or�more�drugs�concurrently�
20
Common�Psychotropic�Drugs
• Benzodiazepines• Diazepam�(Valium),�Lorazepam�(Ativan),�Clonazepam�(Clonipin)
• Anti�depressants• Sertraline�(Zoloft),�Fluoxetine��(Prozac),�Escitalopram�(Lexapro),�Citalopram�(Celexa)
• Antipsychotics�• Risperdone (Risperidol),�Haloperidol�(Haldol),�Olanzapine�(Zyprexa)
21
Common�Cardiac�Drugs
• Beta�Blockers• Atenolol�(Tenormin),�Metoprolol�(Lopressor)
• Calcium�Channel�Blockers• Amlodipine�(Norvasc),�Diltiazem�(Cardizem)
• Diuretics• Furosemide�(Lasix),�Bumetadine (Bumex),�Chlorothiazide (Diuril)
22
Quick�Resource�for�Drug�Information�and�Side�Effects
23
Proprioceptive�Deficits
•When�surfaces�are�varied�and�vision�is�controlled�for,�low�stance�duration�is�related�to�postural�control�beginning�at�the�ankle
• Somatosensory�input�from�the�ankles�provides�a�critical�source�of�information�for�controlling�the�degree�in�body�sway�in�elders�who�fall
24
14
Proprioceptive�Deficits
•We�can�improve�proprioception�by�challenging�our�patients’�balance�in�the�clinic
• Strengthen�righting�and�reaction�strategies�by�eliciting�them
25
Incontinence
• Incidence�of�falls�increased�in�patients�with�urge�incontinence�and�stress�incontinence
• Urge�incontinence�• The�sudden�urge�to�urinate�with�little�to�no�warning
• Stress�incontinence• Involuntary�loss�of�urine�when�abdominal�pressure�increases• Can�be�triggered�by�coughing,�sneezing,�laughing,�jumping,�etc.�
26
Incontinence�
•May�lead�to�reduction�in�mobility�due�to�patient’s�preoccupation�with�remaining�close�to�a�restroom
• Patients�with�these�types�of�incontinence�may�not�be�aware�of�environmental�hazards�due�to�anxiety�related�to�incontinent�episodes
27
How�can�we�help�reduce�the�incidence�of�falls�related�to�
incontinence?•Reducing�extrinsic�factors�such�as�clutter
•Recommending�DME�to�improve�safety
•Pelvic�floor�therapy
•Bowel�and�bladder�program�training�and�implementation 28
Extrinsic�Risk�Factors
29
Extrinsic�Risk�Factors
30
15
Extrinsic�Risk�Factors
31
Extrinsic�Risk�Factors�Special�Consideration:�Diabetic�Footwear
32
Extrinsic�Risk�Factors�Special�Consideration:�Diabetic�Footwear
• Footwear�is�particularly�important�to�the�diabetic�patient
•We�must�stress�this�importance�if�we�notice�a�patient�with�diabetes�not�wearing�appropriate�footwear
• Educate�patient�regarding�foot�hygiene�and�daily�skin�checks
33
Extrinsic�Risk�Factors�Special�Consideration:�Diabetic�Footwear• Inform�patient�that�with�a�diagnosis�of�diabetes,�Medicare�will�cover�one�pair�of�diabetic�shoes,�including�custom�shoes�per�calendar�year
•Medicare�will�also�cover�two�pairs�of�custom�inserts�per�calendar�year
•We�must�stress�the�importance�of�proper�footwear�for�the�diabetic�patient�both�to�aid�in�fall�prevention�and�in�overall�patient�well�being
34
Psychological�Risk�Factors
•Cognitive�deficits
• Fear�of�falling
35
What�role�do�cognitive�deficits�play�in�fall�risk?• Impaired�executive�function• Planning• Execution• Initiation• Judgement• Safety�awareness• Diminished�ability�to�perform�complex�tasks
36
16
Dementia
• A�set�of�symptoms�that�can�include�memory�loss,�difficulty�thinking,�impaired�problem�solving,�or�language�deficits
•We�will�see�various�causes�of�Dementia,�including:• Alzheimer’s�Disease
• Vascular�Dementia
• Lewy�Body�Dementia�
37
Alzheimer’s�Disease
•Most�common�type�of�dementia
• Initial�symptoms�include�short�term�memory�loss
• Disorientation�
• Impaired�Judgement
• Downward�gaze�and�shuffling�gait38
Vascular�Dementia
•Multi�infarct�or�post�stroke�dementia
• Initial�symptoms�include�impaired�judgement�and�difficulty�with�sequencing�tasks
• Symptoms�related�to�region�of�the�brain�that�is�affected�by�vessel�blockages
39
Lewy�Body�Dementia
• Caused�by�clumps�of�proteins�in�the�brain�(Lewy�Bodies)
•More�likely�to�have�earlier�onset�of�hallucinations,�gait�disturbances,�reduced�gait�speed�and�other�Parkinsonian�movement�deficits
40
Mixed�Dementia
• The�presence�of�two�or�more�types�of�dementia
41
Stages�of�Dementia�and�how�they�affect�fall�risk�and�our�ability�to�improve�patient�
outcomes• Stage�1: Normal�– Independent• Stage�2:�Mild�memory�loss�� Independent• Normal�on�tests
• Stage�3:�Mild�cognitive�impairment�– Independent/Part�time�assistance• Deficits�may�be�noticeable�to�those�who�know�individual�well• Possible�objective�deficits�on�testing
• Stage�4: Early�Dementia�– Independent/Assist�from�caregivers�or�family• Difficulty�with�complex�tasks• Denial�or�withdrawal�may�be�present• Deficits�on�testing
42
17
Stages�of�Dementia�and�how�they�affect�fall�risk�and�our�ability�to�
improve�patient�outcomes�continued• Stage�5:Moderate�Dementia�– Full�time�supervision�assistance• Forgetful�– may�forget�family�members• Disorientation• Difficulty�choosing�appropriate�clothing• Can�perform�ADLs�without�assistance
• Stage�6:Moderately�Severe�Dementia�– Complex�care�facility• May�forget�name�of�close�family�members• Unaware�of�life�events• Assistance�with�ADLs• Psych�symptoms�common�(i.e.�agitation,�delusions)
43
Stages�of�Dementia�and�how�they�affect�fall�risk�and�our�ability�to�
improve�patient�outcomes�continued• Stage�7: Severe�Dementia• Verbal�abilities�lost• Unable�to�ambulate• Unable�to�feed�self
44
Brain�Injury
• Visual�perceptual�impairments
• Difficulty�sustaining�movements
• Impulsive�behavioral�style
• Decreased�awareness�of�impairments
• Poor�judgement
• Difficulty�with�self�correction
• Difficulty�processing�visual�cues
• Memory�impairments
Right�brain�injury�often�leads�to:
45
Brain�Injury
• Difficulty�with�planning�and�sequencing�movements
• Apraxia
• Disorganized�problem�solving
• Processing�delays
• Difficulty�processing�verbal�cues�or�commands
Left�brain�injury�often�leads�to:
46
What�is�fear�of�falling?
• Defined�as�an�ongoing�concern�about�falling�that�limits�the�performance�of�daily�activities
• Present�in�12%�65%�of�community�dwelling�adults�over�65�who�have�not fallen
• Present�in�29%�92%�of�adults�over�65�who�have�experienced�a�fall
47
Why�are�we�concerned�with�fear�of�falling?
• Often�presents�as�patient�not�wanting�to�participate�in�an�activity�that�they�once�enjoyed�or�cared�about
• Correlated�with�decreased�quality�of�life
• Indicator�of�increased�morbidity�and�mortality
• Results�in�further�decline�in�functional�status48
18
Identifying�Vestibular�Influences�on�Balance�
Deficits
49
Three�Systems�Assist�With�Maintenance�of�Balance
•Vision
•Proprioception
•Vestibular�Inputs
50
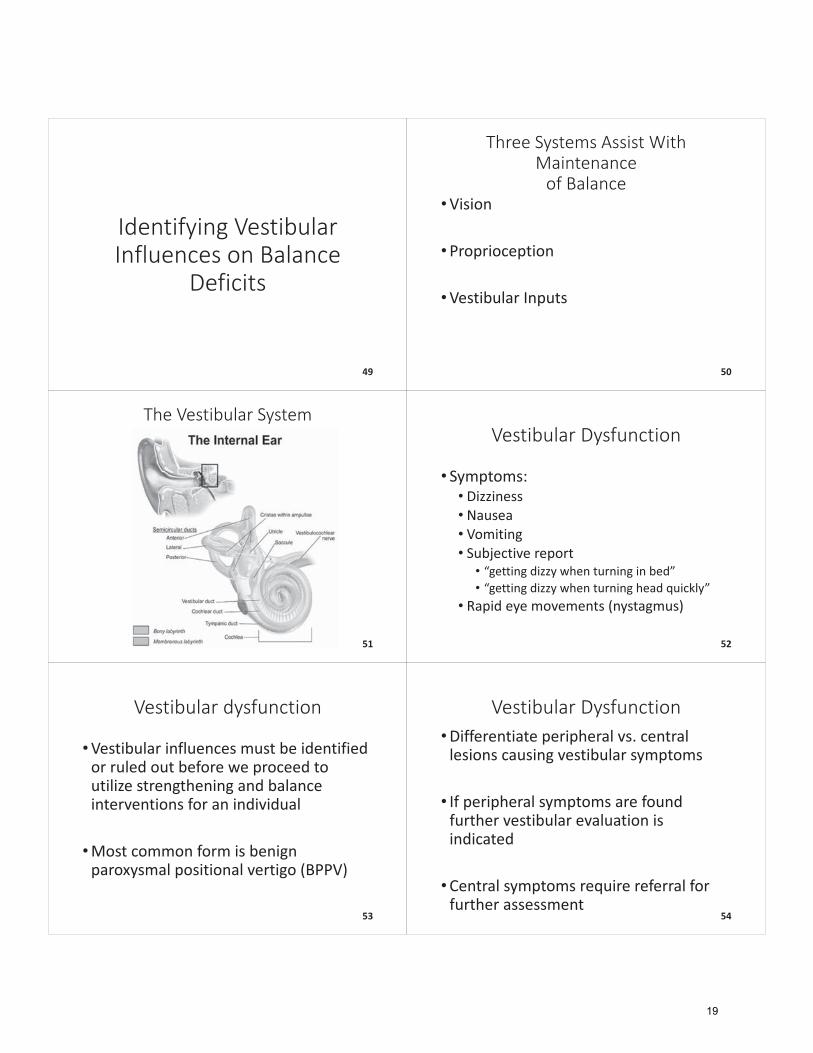
The�Vestibular�System
51
Vestibular�Dysfunction
• Symptoms:• Dizziness• Nausea• Vomiting• Subjective�report• “getting�dizzy�when�turning�in�bed”�• “getting�dizzy�when�turning�head�quickly”
• Rapid�eye�movements�(nystagmus)
52
Vestibular�dysfunction
•Vestibular�influences�must�be�identified�or�ruled�out�before�we�proceed�to�utilize�strengthening�and�balance�interventions�for�an�individual
•Most�common�form�is�benign�paroxysmal�positional�vertigo�(BPPV)
53
Vestibular�Dysfunction•Differentiate�peripheral�vs.�central�lesions�causing�vestibular�symptoms
• If�peripheral�symptoms�are�found�further�vestibular�evaluation�is�indicated
•Central�symptoms�require�referral�for�further�assessment
54
19
Central�Vestibular�Red�Flags��• Severe�ataxia
• Abnormal�smooth�pursuit
• Brainstem�symptoms• i.e.�diplopia,�dysarthria,�altered�consciousness
• Pendular nystagmus�(eyes�oscillate�at�equal�speeds�– no�slow�or�fast�phase)
• Persistent�vertical�nystagmus�that�persists�without�positional�testing
55
Assessment�tools�for�Balance�Dysfunction
56
Utilizing�appropriate�assessment�tools�for�determining�fall�risk�in�the�
aging�senior�population•Physical�based�assessments
•Psychological�based�assessments
57
Physical�based�Assessments
• BERG�Balance�assessment
• Tinetti Performance�Oriented�Mobility�Assessment�(POMA)
• Four�Step�Square�Test
• Timed�Up�and�Go�(TUG)�Test
• Dynamic�Gait�Index�(DGI)
• Functional�Reach�Test
• Five�Times�Sit�to�Stand�(FTSS)�Test
• Walking�Speed�Assessment�
58
BERG�Balance�Assessment�
•Objective�assessment�to�assess�static�balance�and�fall�risk
• Instructions:�Lead�patient�through�14�item�assessment• Includes:�sit�<�>�stand,�transfers,�static�standing,�EC,�forward�reach,�head�turns,�360�degree�turns,�alternating�step�tapping,�narrow�BOS�standing,�tandem�standing,�SLS,�object�retrieval�from�floor
59
BERG�Balance�Assessment
• Total�points:�56
•Categories:• 0�20:�high�fall�risk/wheelchair�bound• 21�40:�medium�fall�risk/walks�with�assistance�or�assistive�device• 41�56:�low�fall�risk• 46�and�above�indicate�lowest�fall�risk*
60
20
Tinetti Performance�Oriented�Mobility�Assessment�(POMA)
•Objective�measure�of�balance�and�gait�abilities
• Instructions:�lead�patient�through�16�item�assessment• Includes:�sitting�balance,�sit�<�>�stand,�standing�balance,�perturbation,�romberg,�360�degree�turns,�gait�initiation,�gait�quality,�trunk�sway�during�gait,�walking�stance
61
Tinetti Performance�Oriented�Mobility�Assessment�(POMA)
• Total�points:�28• 16�Balance• 12�Gait
•Categories:• High�fall�risk:�<19•Medium�fall�risk:�19�24• Low�Fall�risk:��25�28
62
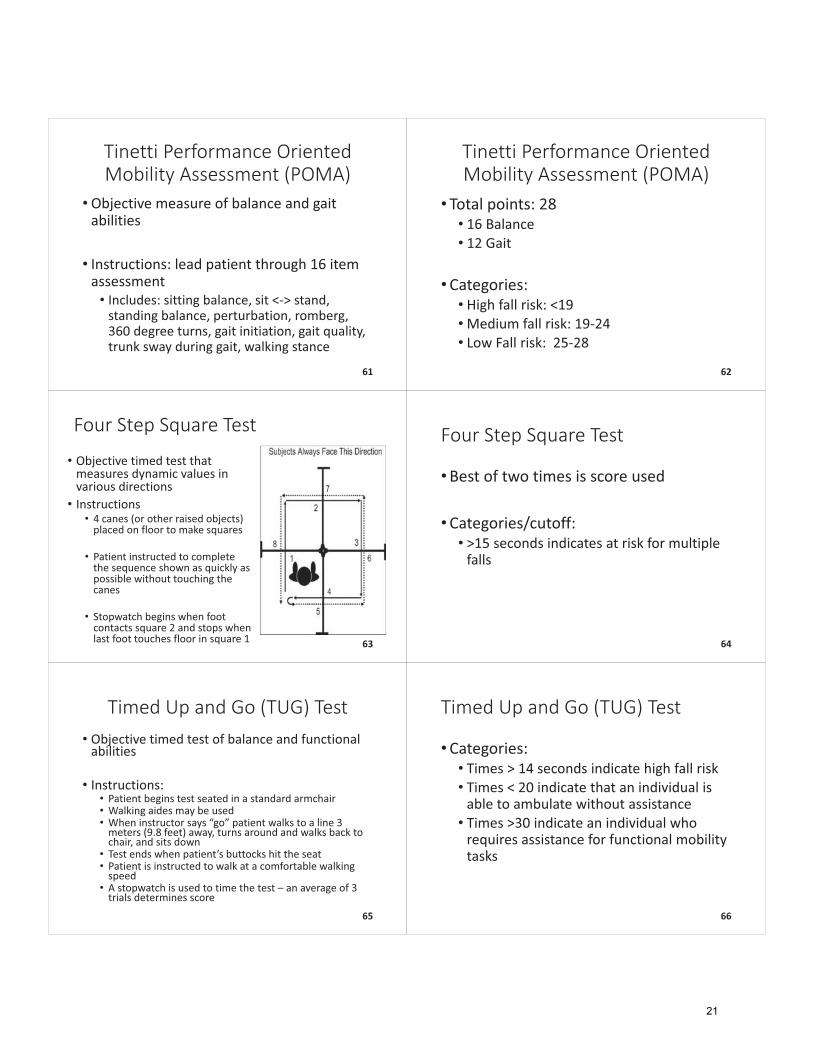
Four�Step�Square�Test
• Objective�timed�test�that�measures�dynamic�values�in�various�directions• Instructions
• 4�canes�(or�other�raised�objects)�placed�on�floor�to�make�squares
• Patient�instructed�to�complete�the�sequence�shown�as�quickly�as�possible�without�touching�the�canes
• Stopwatch�begins�when�foot�contacts�square�2�and�stops�when�last�foot�touches�floor�in�square�1 63
Four�Step�Square�Test
•Best�of�two�times�is�score�used
•Categories/cutoff:�• >15�seconds�indicates�at�risk�for�multiple�falls
64
Timed�Up�and�Go�(TUG)�Test• Objective�timed�test�of�balance�and�functional�abilities
• Instructions:• Patient�begins�test�seated�in�a�standard�armchair• Walking�aides�may�be�used• When�instructor�says�“go”�patient�walks�to�a�line�3�meters�(9.8�feet)�away,�turns�around�and�walks�back�to�chair,�and�sits�down
• Test�ends�when�patient’s�buttocks�hit�the�seat• Patient�is�instructed�to�walk�at�a�comfortable�walking�speed
• A�stopwatch�is�used�to�time�the�test – an�average�of�3�trials�determines�score
65
Timed�Up�and�Go�(TUG)�Test
•Categories:• Times�>�14�seconds�indicate�high�fall�risk• Times�<�20�indicate�that�an�individual�is�able�to�ambulate�without�assistance• Times�>30�indicate�an�individual�who�requires�assistance�for�functional�mobility�tasks
66
21
Dynamic�Gait�Index
• 8�item�objective�test�utilized�to�assess�a�patient’s�ability�to�modify�balance�while�ambulating�in�the�presence�of�external�demands
• Includes:�Gait�on�level�surfaces,�change�in�gait�speed,�gait�with�horizontal�head�turns,�gait�with�vertical�head�turns,�gait�with�pivot�turns,�stepping�over�obstacles,�walking�around�obstacles,�steps�(stairs)
67
Dynamic�Gait�Index
• Total�points:�24
•Categories:�• <19/24:�predictive�of�falls�in�the�elderly• >22/24:�safe�ambulators
68
Functional�Reach
• Objective�measure�of�patient’s�ability�to�reach�forward�• Instructions• Yardstick�mounted�to�wall�at�level�of�patient’s�acromion�in�standing
• Patient�stands�close�to�wall�with�arm�in�90�degrees�of�shoulder�flexion�with�closed�fist
• Starting�position�recorded�at�3rd metacarpal�head�on�yardstick
• Patient�instructed�to�reach�as�far�as�they�can�without�taking�a�step
• Difference�between�start�and�end�position�measured�(usually�in�inches)
• 5�trials�allowed:�2�practice�and�then�average�of�3�test�trials
69
Modified�Functional�Reach• Instructions:• Yardstick�mounted�to�wall�at�level�of�patient’s�acromion�in�sitting• Hips,�knees,�ankles�positioned�at�90�degrees�flexion�with�feet�on�floor• Starting�position�measured�as�position�of�third�metacarpal�head�with�patient�sitting�against�back�of�chair�with�UE�flexed�to�90�degrees• Measurements�taken�in�3�positions:• Sitting�with�UE�near�wall�leaning�forward• Sitting�with�back�to�the�wall�leaning�right• Sitting�with�back�to�the�wall�leaning�left
70
Modified�Functional�Reach
• Instructions�(cont.):�• Patient�instructed�to�lean�as�far�in�each�direction�as�possible�without�rotation�and�without�touching�wall• Once�patient�leans,�mark�position�of�3rd metacarpal�head�along�yard�stick• If�patient�unable�to�make�a�fist�use�ulnar�styloid�process�as�landmark• Record�distance�(usually�in�centimeters)�covered�in�each�direction• If�patient�unable�to�raise�affected�arm�use�distance�covered�by�acromion�in�leaning• First�trial�is�practice�and�not�recorded�in�final�measurement
71
Functional�Reach�&�Modified�Functional�Reach�Test
•Categories• Community�dwelling�seniors• <�7�inches�(17.78�cm)�indicates:�unable�to�leave�neighborhood�without�help,�limited�mobility�skills,�and�most�restricted�in�ADL
• Frail�seniors• <�7.3�inches�(18.5�cm)�indicates�fall�risk
72
22
Five�Times�Sit�to�Stand�(FTSS)�Test
• Objective�assessment�of�functional�lower�extremity�strength,�transitional�movements,�balance,�and�fall�risk
• Instructions:• Patient�seated�upright��with�arms�folded�and�back�against�chair�in�standard�height�chair�with�straight�back• Patient�instructions:�“please�stand�up�straight�as�quickly�as�you�can�five�times,�without�stopping�in�between.��Keep�your�arms�folded�across�you�chest,�ready�begin”
73
Five�Times�Sit�to�Stand�(FTSS)Test�
• Timer�started�when�therapist�says�“begin”�and�stopped�when�patient�reaches�standing�position�on�fifth�repetition�
•Categories:• >�13.6�seconds�associated�with�increased�disability�and�morbidity• >�15�seconds�predictive�of�recurrent�falls
74
Walking�Speed
•Objective�measurement�of�gait�speed�measure�by�patient�walking�a�known�distance�with�the�distance�and�time�converted�into�m/s
• Implications•Walking�speed�<1.0�m/s�is�indicative�of�increased�falls,�increased�morbidity,�and�increased�mortality�in�the�aging�senior�population
75
Walking�Speed�Assessments
• 10�meter�walking�test�(20�meter�course)• Found�to�have�similar�implications�to�2�minute�walk�test�and�takes�less�time�in�the�clinic• Speed�is�measured�in�the�central�10�meters�of�a�20�meter�course
• 4�meter�walking�test�(6�meter�course)• Useful�in�small�environments�such�as�home/small�clinics• Speed�is�measured�in�central�4�meters�of�6�meter�course
76
Psychological�based�Assessments
• Tinetti Falls�Efficacy�Scale�(FES)
•Activities�specific�Balance�Confidence�Scale�(ABC)
77
Tinetti Falls�Efficacy�Scale�(FES)
• 10�item�subjective�test�to�assess�balance�and�stability�during�activities�of�daily�living�and�fear�of�falling�in�the�elderly�population
• Instructions�read:�”how�confident�are�you�that�you�do�the�following�activities�without�falling…”• taking�bath/shower,�reaching�into�cabinets/closets,�walking�around�house,�preparing�meals,�answering�door/phone,�getting�in/out�of�chair,�enter/exit�car,�dressing/undressing,�personal�grooming,�getting�on/off�toilet
78
23

Tinetti Falls�Efficacy�Scale�(FES)
•Answers�range�from�1(very�confident)�to�10�(not�confident�at�all)
• Total�points:�100
•Categories:• Scores�>�70�indicative�of�fear�of�falling�in�the�elderly
79
Activities�specific�Balance�Confidence�(ABC)�Scale
• 16�item�subjective�measure�of�confidence�in�performing�various�ambulatory�activities�without�falling�or�experiencing�a�sense�of�unsteadiness
• Instructions�read:�“how�confident�are�you�that�you�will�not�lose�your�balance�or�become�unsteady�when�you…”• Walk�around�house,�walk�up/down�stairs,�bend�to�pick�up�slipper,�reach�for�eye�level�shelf,�stand�on�tip�toes�and�reach�overhead,�stand�on�chair�and�reach,�sweep�floor,�walk�to�car�in�driveway,�get�in/out�of�car,�walk�across�mall�parking�lot,�walk�up/down�ramp,�walk�in�crowded�mall,�step�on/off�escalator�holding�railing/not�holding�railing,�walk�on�icy�sidewalks 80
Activities�specific�Balance�Confidence�(ABC)�Scale
• Patient�gives�percentage�ratings�0%�(no�confidence)�to�100%�(completely�confident)�to�each�question�then�total�is�divided�by�16�to�get�percentage
• Categories:• >80%:�high�level�of�physical�functioning• 50�80%:�moderate�level�of�physical�functioning�• <50%:�low�level�of�physical�functioning• <67%:�older�adults�at�risk�for�falling;�predictive�of�future�fall
81
Quick�Reference�for�Standardized�Test�and�Measures
www.rehabmeasures.org
82
Evaluation�Considerations�when�assessing�the�high�fall�risk�
population
83
Chart�Review
• PMH/PSH
• Co�morbidities�
•Medications
• Precautions
• Contraindications84
24
Subjective
• Prior�level�of�function
•Who�lives�in�home�with�patient?
•Was�an�assistive�device�used?
• Are�there�steps�into�or�inside�of�home?
85
Subjective
•What�is�the�set�up�of�the�restroom?
•Was�patient�managing�medicines?• What�strategies�were�used?
•Was�patient�driving?
•Who�did�grocery�shopping?
86
Subjective•Was�patient�cooking?• If�so,�light�meal�prep�or�heavy�meals?
•Was�patient�doing�own�laundry?• At�home�or�laundromat?
•Was�patient�managing�finances?
•What�type�of�family�and�social�support�does�patient�have?
87
Subjective
•What�are�the�patient’s�goals
• Caregiver/family�goals?
• Hobbies?
• Occupation?• Current�or�past
88
Subjective• Falls�history
• Psychological�based�standardized�assessments
• Level�of�alertness
• Orientation
• Safety�awareness89
Subjective
• Discharge�plan�–*discharge�planning�begins�on�evaluation�day*
• Is�plan�to�return�to�prior�living�setting?• If�not,�what�is�the�plan?
•What�DME�does�patient�already�own?• This�is�often�different�from�what�they�are�using
90
25
Objective
• Bathing�
• Dressing
• Toileting
• Grooming
91
Objective�
• Activity�tolerance
• Decision�making
• Ability�to�follow�commands�and�type�of�commands�required
• Current�assistive�device�needs
92
Objective�
• Standardized�Assessments
• Bed�mobility
• Transfers
• Balance�grade
• Range�of�motion93
Objective�
•Manual�Muscle�Testing• Key�muscles�for�the�high�fall�risk�patient:• Hip�flexors• Hip�abductors• Hip�extensors• Ankle�dorsiflexors• Shoulder�flexors• Elbow�extensors
94
Customized�Treatment�for�
Patients�of�Varying�Functional�Levels
95
What�Postural�abnormalities�does�your�client�have�that�may�affect�stability?
Sway�Back Lumbar�Lordosis
Thoracic�Kyphosis
Forward�Head
Good�Posture 96
26
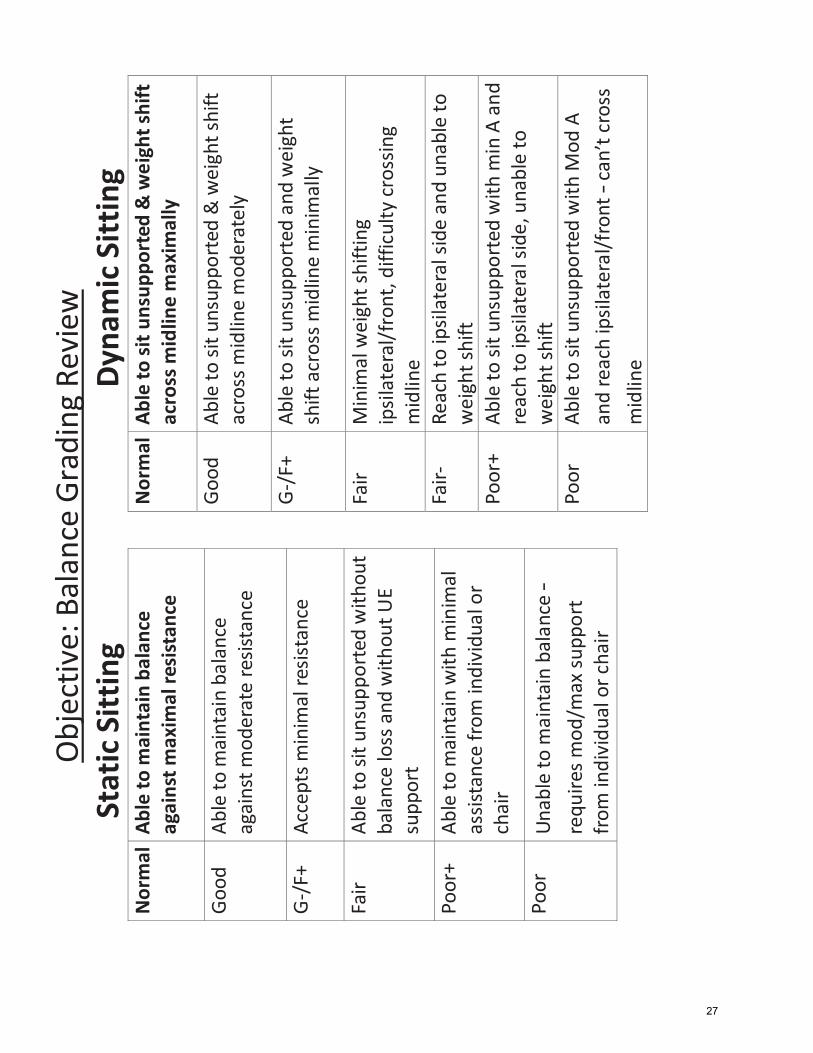
Obj
ectiv
e: B
alan
ce G
radi
ng R
evie
w
Stat
ic S
ittin
g N
orm
al A
ble
to m
aint
ain
bala
nce
agai
nst m
axim
al re
sist
ance
Goo
d Ab
le to
mai
ntai
n ba
lanc
e ag
ains
t mod
erat
e re
sista
nce
G-/
F+
Acce
pts m
inim
al re
sista
nce
Fair
Able
to si
t uns
uppo
rted
with
out
bala
nce
loss
and
with
out U
E su
ppor
t
Poor
+ Ab
le to
mai
ntai
n w
ith m
inim
al
assis
tanc
e fro
m in
divi
dual
or
chai
r
Poor
Un
able
to m
aint
ain
bala
nce –
requ
ires m
od/m
ax su
ppor
t fro
m in
divi
dual
or c
hair
Dyna
mic
Sitt
ing
Nor
mal
Abl
e to
sit u
nsup
port
ed &
wei
ght s
hift
ac
ross
mid
line
max
imal
ly
Goo
d Ab
le to
sit u
nsup
port
ed &
wei
ght s
hift
ac
ross
mid
line
mod
erat
ely
G-/
F+
Able
to si
t uns
uppo
rted
and
wei
ght
shift
acr
oss m
idlin
e m
inim
ally
Fair
Min
imal
wei
ght s
hift
ing
ipsi
late
ral/f
ront
, diff
icul
ty c
ross
ing
mid
line
Fair-
Re
ach
to ip
sila
tera
l sid
e an
d un
able
to
wei
ght s
hift
Poor
+ Ab
le to
sit u
nsup
port
ed w
ith m
in A
and
re
ach
to ip
sila
tera
l sid
e, u
nabl
e to
w
eigh
t shi
ft Po
or
Able
to si
t uns
uppo
rted
with
Mod
A
and
reac
h ip
sila
tera
l/fro
nt – c
an’t
cros
s m
idlin
e
27
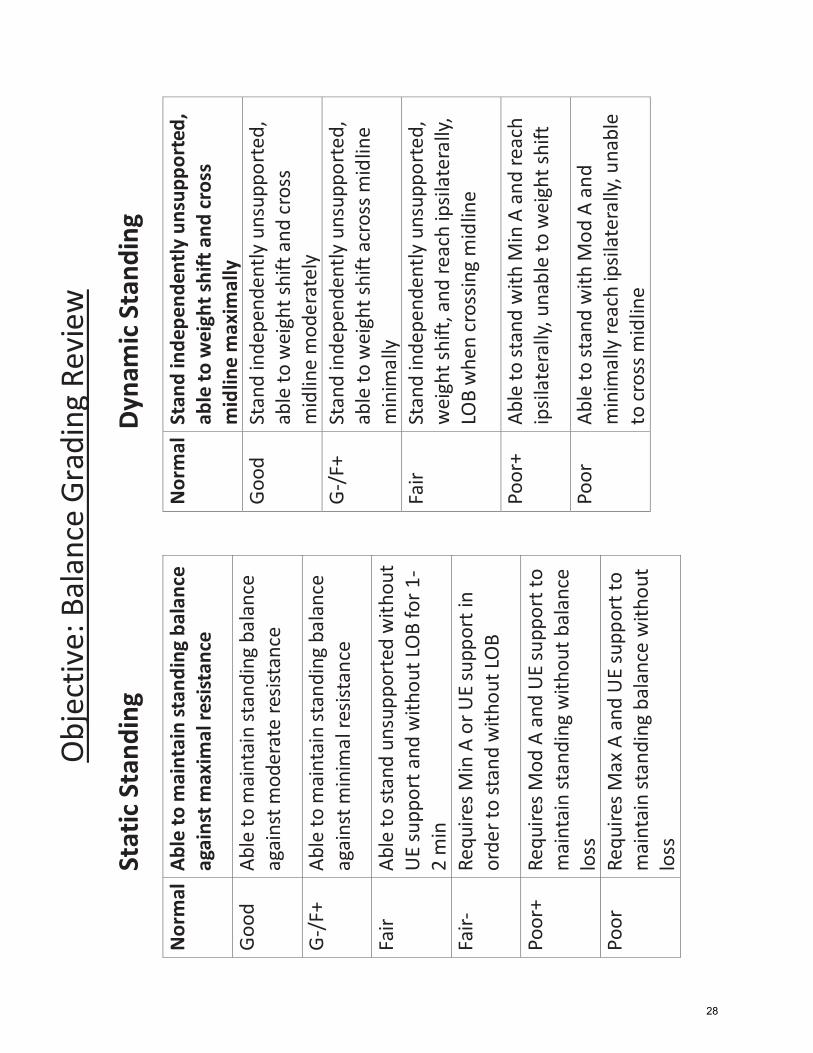
Obj
ectiv
e: B
alan
ce G
radi
ng R
evie
w
Stat
ic S
tand
ing
Nor
mal
Abl
e to
mai
ntai
n st
andi
ng b
alan
ce
agai
nst m
axim
al re
sist
ance
Goo
d
Able
to m
aint
ain
stan
ding
bal
ance
ag
ains
t mod
erat
e re
sista
nce
G-/
F+
Able
to m
aint
ain
stan
ding
bal
ance
ag
ains
t min
imal
resis
tanc
e
Fair
Able
to st
and
unsu
ppor
ted
with
out
UE
supp
ort a
nd w
ithou
t LO
B fo
r 1-
2 m
in
Fair-
Re
quire
s Min
A o
r UE
supp
ort i
n or
der t
o st
and
with
out L
OB
Poor
+ Re
quire
s Mod
A a
nd U
E su
ppor
t to
mai
ntai
n st
andi
ng w
ithou
t bal
ance
lo
ss
Poor
Re
quire
s Max
A a
nd U
E su
ppor
t to
mai
ntai
n st
andi
ng b
alan
ce w
ithou
t lo
ss
Dyna
mic
Sta
ndin
g
Nor
mal
Sta
nd in
depe
nden
tly u
nsup
port
ed,
able
to w
eigh
t shi
ft a
nd cr
oss
mid
line
max
imal
ly
Goo
d St
and
inde
pend
ently
uns
uppo
rted
, ab
le to
wei
ght s
hift
and
cro
ss
mid
line
mod
erat
ely
G-/
F+
Stan
d in
depe
nden
tly u
nsup
port
ed,
able
to w
eigh
t shi
ft a
cros
s mid
line
min
imal
ly
Fair
Stan
d in
depe
nden
tly u
nsup
port
ed,
wei
ght s
hift
, and
reac
h ip
sila
tera
lly,
LOB
whe
n cr
ossin
g m
idlin
e
Poor
+ Ab
le to
stan
d w
ith M
in A
and
reac
h ip
sila
tera
lly, u
nabl
e to
wei
ght s
hift
Poor
Ab
le to
stan
d w
ith M
od A
and
m
inim
ally
reac
h ip
sila
tera
lly, u
nabl
e to
cro
ss m
idlin
e
28
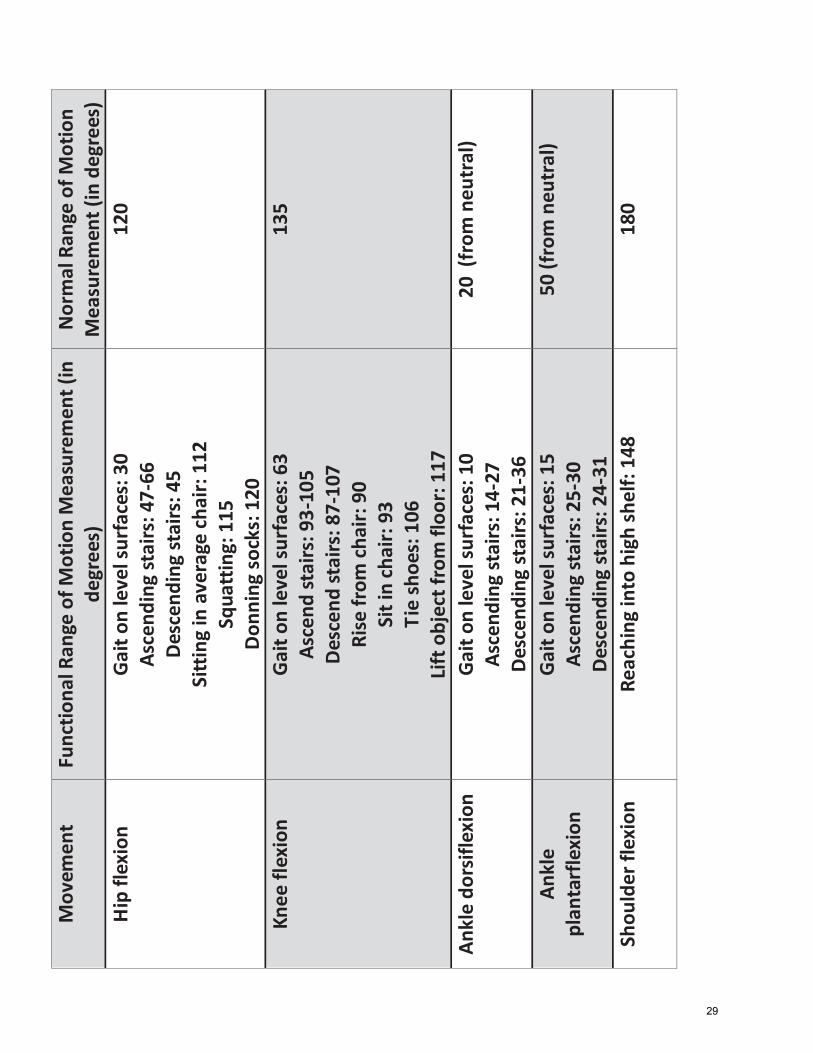
Mov
emen
t Fu
nctio
nal R
ange
of M
otio
n M
easu
rem
ent (
in
degr
ees)
N
orm
al R
ange
of M
otio
n M
easu
rem
ent (
in d
egre
es)
Hip
flex
ion
Gait
on le
vel s
urfa
ces:
30
Asce
ndin
g st
airs
: 47-
66
Desc
endi
ng st
airs
: 45
Sitt
ing
in a
vera
ge ch
air:
112
Squa
ttin
g: 1
15
Don
ning
sock
s: 1
20
120
Knee
flex
ion
Gait
on le
vel s
urfa
ces:
63
Asce
nd st
airs
: 93-
105
Desc
end
stai
rs: 8
7-10
7 Ri
se fr
om ch
air:
90
Sit i
n ch
air:
93
Tie
shoe
s: 1
06
Lift
obj
ect f
rom
floo
r: 11
7
135
Ankl
e do
rsifl
exio
n Ga
it on
leve
l sur
face
s: 1
0 As
cend
ing
stai
rs: 1
4-27
De
scen
ding
stai
rs: 2
1-36
20 (
from
neu
tral
)
Ankl
e pl
anta
rfle
xion
Ga
it on
leve
l sur
face
s: 1
5 As
cend
ing
stai
rs: 2
5-30
De
scen
ding
stai
rs: 2
4-31
50 (f
rom
neu
tral
)
Shou
lder
flex
ion
Reac
hing
into
hig
h sh
elf:
148
180
29
Swayback�posture
• Swayback�
• Posteriorly�positioned�shoulders
• Backward�lean�of�trunk
• Slight�flexion�of�knees
• Posteriorly�tilted�pelvis�97
Swayback�posture• Treatment�strategies:•Wall�standing• Promotes�postural�re�training• Patient�has�no�option�but�to�stand�in�improved�mildine position
• Promote�neutral�pelvic�position• Moving�patient�out�of�posterior�pelvic�tilt• Core�strengthening�• Quadriceps�strengthening�• Hamstring�stretching
98
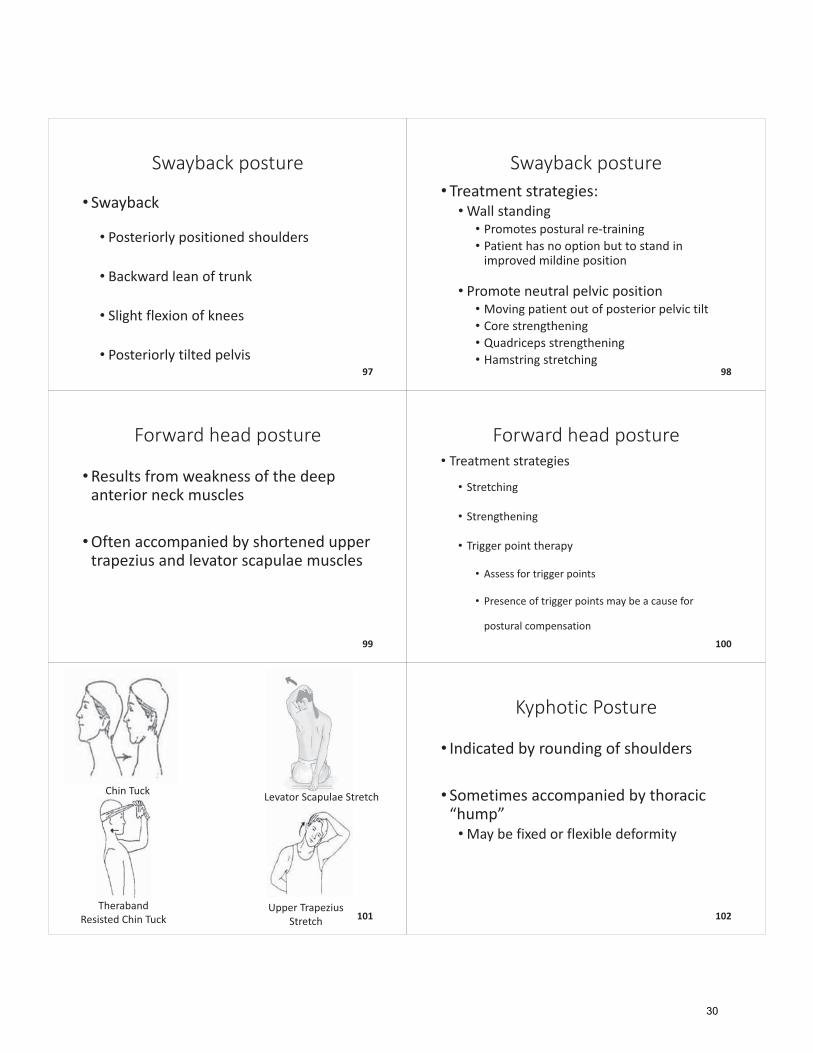
Forward�head�posture
•Results�from�weakness�of�the�deep�anterior�neck�muscles
•Often�accompanied�by�shortened�upper�trapezius�and�levator scapulae�muscles�
99
Forward�head�posture• Treatment�strategies
• Stretching
• Strengthening
• Trigger�point�therapy
• Assess�for�trigger�points
• Presence�of�trigger�points�may�be�a�cause�for�
postural�compensation100
Chin�Tuck
TherabandResisted�Chin�Tuck
Upper�Trapezius�Stretch
Levator Scapulae�Stretch
101
Kyphotic�Posture
• Indicated�by�rounding�of�shoulders
• Sometimes�accompanied�by�thoracic�“hump”•May�be�fixed�or�flexible�deformity�
102
30
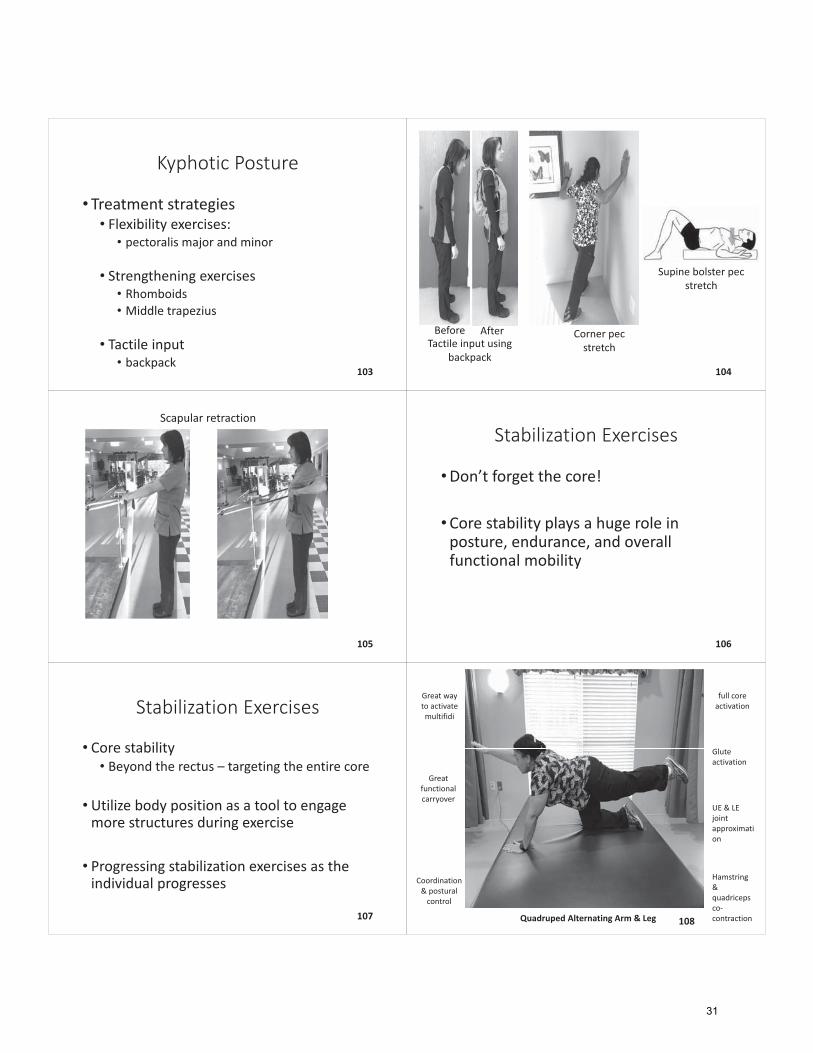
Kyphotic�Posture
• Treatment�strategies• Flexibility�exercises:• pectoralis�major�and�minor
• Strengthening�exercises• Rhomboids• Middle�trapezius
• Tactile�input• backpack
103
Corner�pec�stretch
Supine�bolster�pec�stretch
Tactile�input�using�backpack
Before After
104
Scapular�retraction
105
Stabilization�Exercises
•Don’t�forget�the�core!
•Core�stability�plays�a�huge�role�in�posture,�endurance,�and�overall�functional�mobility
106
Stabilization�Exercises
• Core�stability• Beyond�the�rectus�– targeting�the�entire�core
• Utilize�body�position�as�a�tool�to�engage�more�structures�during�exercise
• Progressing�stabilization�exercises�as�the�individual�progresses
107 Quadruped�Alternating�Arm�&�Leg
Great�way�to�activate�multifidi
full�core�activation
Great�functional�carryover
UE�&�LE�joint�approximation
Coordination�&�postural�control
Hamstring�&�quadriceps�co�contraction
Glute�activation
108
31
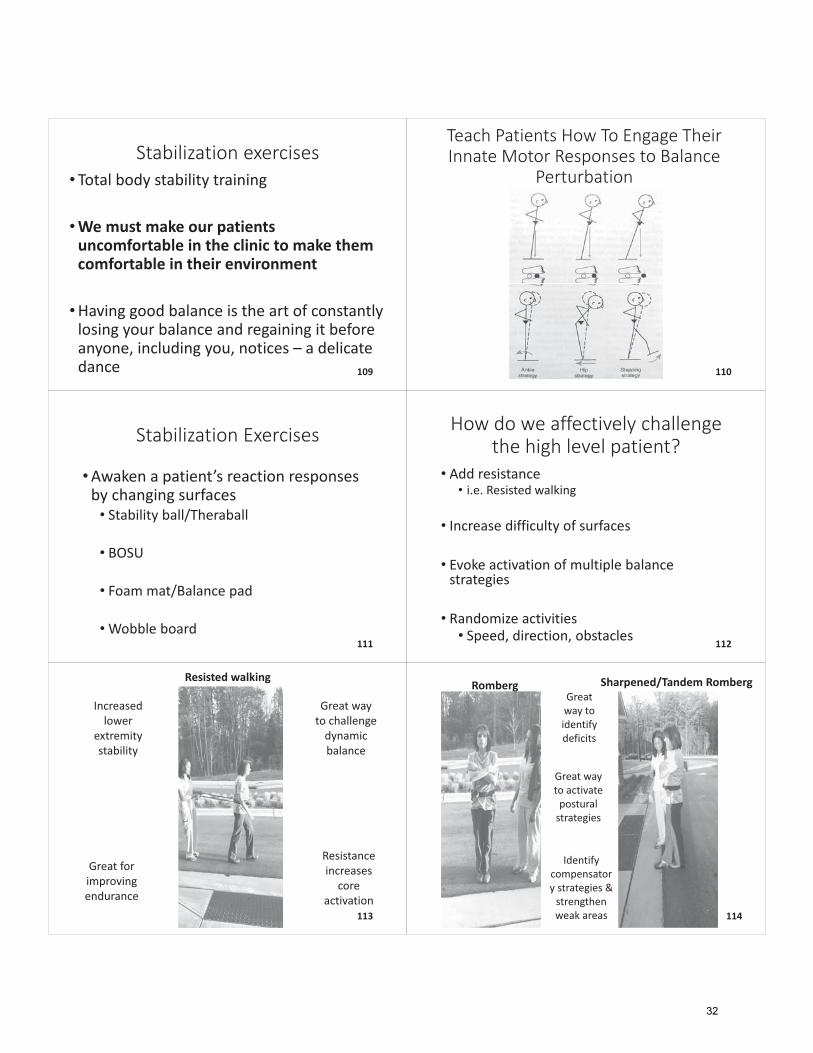
Stabilization�exercises• Total�body�stability�training�
•We�must�make�our�patients�uncomfortable�in�the�clinic�to�make�them�comfortable�in�their�environment
•Having�good�balance�is�the�art�of�constantly�losing�your�balance�and�regaining�it�before�anyone,�including�you,�notices�– a�delicate�dance 109
Teach�Patients�How�To�Engage�Their�Innate�Motor�Responses�to�Balance�
Perturbation
110
Stabilization�Exercises
•Awaken�a�patient’s�reaction�responses�by�changing�surfaces• Stability�ball/Theraball
• BOSU
• Foam�mat/Balance�pad
•Wobble�board111
How�do�we�affectively�challenge�the�high�level�patient?
• Add�resistance• i.e.�Resisted�walking
• Increase�difficulty�of�surfaces
• Evoke�activation�of�multiple�balance�strategies
• Randomize�activities• Speed,�direction,�obstacles
112
Resisted�walking
Great�way�to�challenge�dynamic�balance
Great�for�improving�endurance�
Resistance�increases�core�
activation
Increased�lower�
extremity�stability
113
Romberg Sharpened/Tandem�RombergGreat�way�to�identify�deficits
Great�way�to�activate�postural�strategies
Identify�compensatory�strategies�&�strengthen�weak�areas 114
32

BOSU�Lunges:�Modified�forward�lunge BOSU�Lunges:�Full�forward�lunge
Great�way�to�
strengthen�ankle�&�stepping�strategies
Activation�of�
multiple�muscle�groups
Dynamic�stability�training
115
BOSU�forward�step�through
Stepping�strategies
Reaction�strategies
Ankle�stability
Hip�stability Postural�
awareness
116
BOSU�unilateral�step�reaching BOSU�standing�with�reaching
Total�body�stability�with�
functional�task
Challenge�limits�of�stability
117BOSU�barefoot�standing BOSU�side�step
Lateral�stability
Improve�activation�of�foot�intrinsics
118
Resisted�side�stepping�with�squat
Strength�and�stability�combination
Co�contraction�of�key�muscles
Incorporate�postural�awareness
Improve�precision�of�movement
119 Object�step�overs
Promotes�postural�stability�and�awareness
Promote�correct�midline�orientation�during�dynamic�gait�tasks
120
33
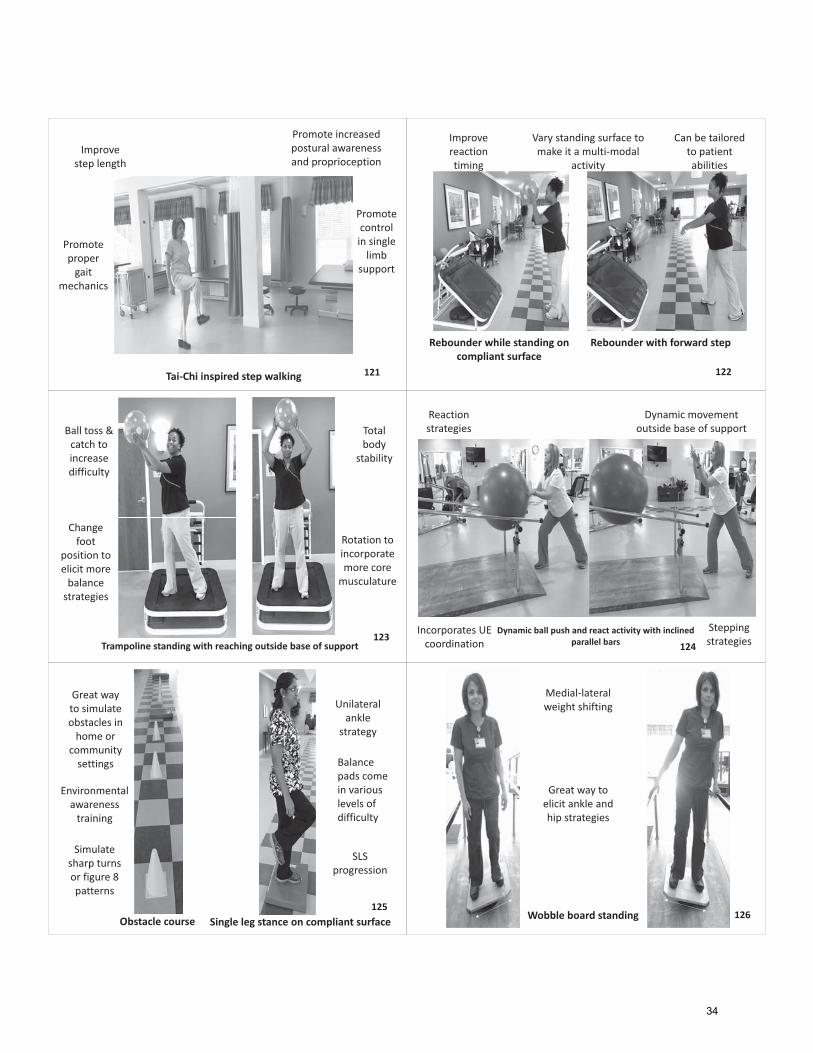
Tai�Chi�inspired�step�walking
Promote�control�in�single�limb�
support
Improve�step�length
Promote�increased�postural�awareness�and�proprioception
Promote�proper�gait�
mechanics
121
Rebounder�while�standing�on�compliant�surface
Rebounder�with�forward�step
Improve�reaction�timing
Can�be�tailored�to�patient�abilities
Vary�standing�surface�to�make�it�a�multi�modal�
activity
122
Trampoline�standing�with�reaching�outside�base�of�support
Rotation�to�incorporate�more�core�musculature
Ball�toss�&�catch�to�increase�difficulty
Total�body�
stability
Change�foot�
position�to�elicit�more�balance�strategies
123
Reaction�strategies
Dynamic�movement�outside�base�of�support
Stepping�strategies
Incorporates�UE�coordination
Dynamic�ball�push�and�react�activity�with�inclined�parallel�bars 124
Obstacle�course Single�leg�stance�on�compliant�surface
Great�way�to�simulate�obstacles�in�home�or�
community�settings
Environmental�awareness�training
Simulate�sharp�turns�or�figure�8�patterns
Unilateral�ankle�
strategy
SLS�progression
Balance�pads�come�in�various�levels�of�difficulty
125Wobble�board�standing
Medial�lateral�weight�shifting
Great�way�to�elicit�ankle�and�hip�strategies
126
34
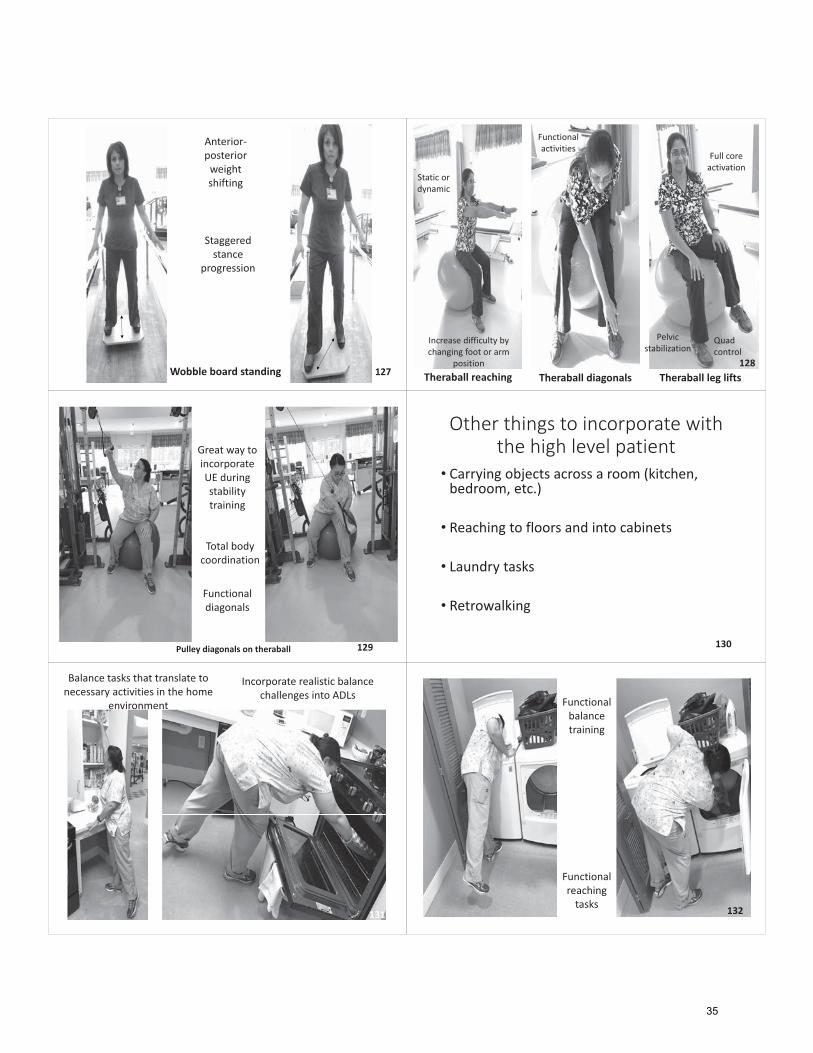
Wobble�board�standing
Anterior�posterior�weight�shifting
Staggered�stance��
progression
127 Theraball leg�liftsTheraball diagonalsTheraball reaching
Pelvic�stabilization
Quad�control
Full�core�activation
Functional�activities
Static�or�dynamic
Increase�difficulty�by�changing�foot�or�arm�
position 128
Pulley�diagonals�on�theraball
Great�way�to�incorporate�UE�during�stability�training
Total�body�coordination
Functional�diagonals
129
Other�things�to�incorporate�with�the�high�level�patient
• Carrying�objects�across�a�room�(kitchen,�bedroom,�etc.)
• Reaching�to�floors�and�into�cabinets
• Laundry�tasks
• Retrowalking
130
Incorporate�realistic�balance�challenges�into�ADLs
Balance�tasks�that�translate�to�necessary�activities�in�the�home�
environment
131
Functional�balance�training
Functional�reaching�tasks 132
35
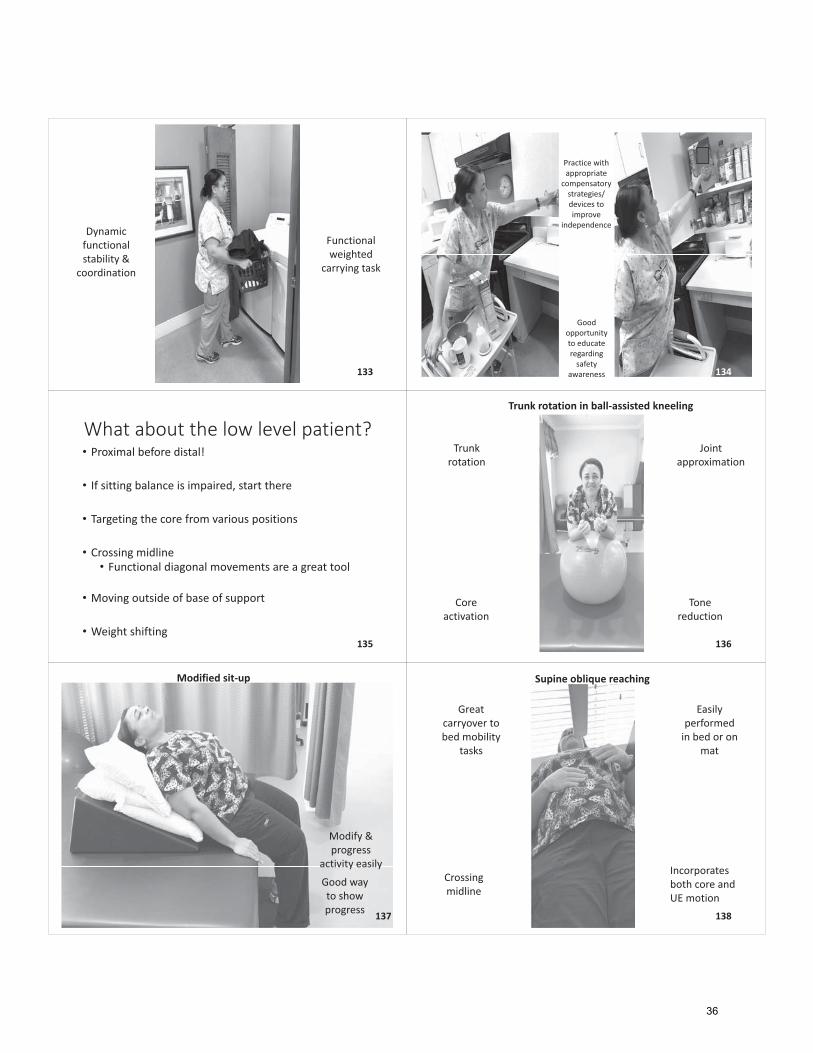
Functional�weighted�
carrying�task
Dynamic�functional�stability�&�
coordination
133
Practice�with�appropriate�
compensatory�strategies/devices�to�improve�
independence�
Good�opportunity�to�educate�regarding�safety�
awareness 134
What�about�the�low�level�patient?• Proximal�before�distal!�
• If�sitting�balance�is�impaired,�start�there
• Targeting�the�core�from�various�positions
• Crossing�midline• Functional�diagonal�movements�are�a�great�tool
• Moving�outside�of�base�of�support
• Weight�shifting135
Trunk�rotation�in�ball�assisted�kneeling
Trunk�rotation
Joint�approximation
Tone�reduction
Core�activation
136
Modified�sit�up
Modify�&�progress�
activity�easily
Good�way�to�show�progress 137
Supine�oblique�reaching
Easily�performed�in�bed�or�on�
mat
Great�carryover�to�bed�mobility�
tasks
Incorporates�both�core�and�UE�motion
Crossing�midline
138
36
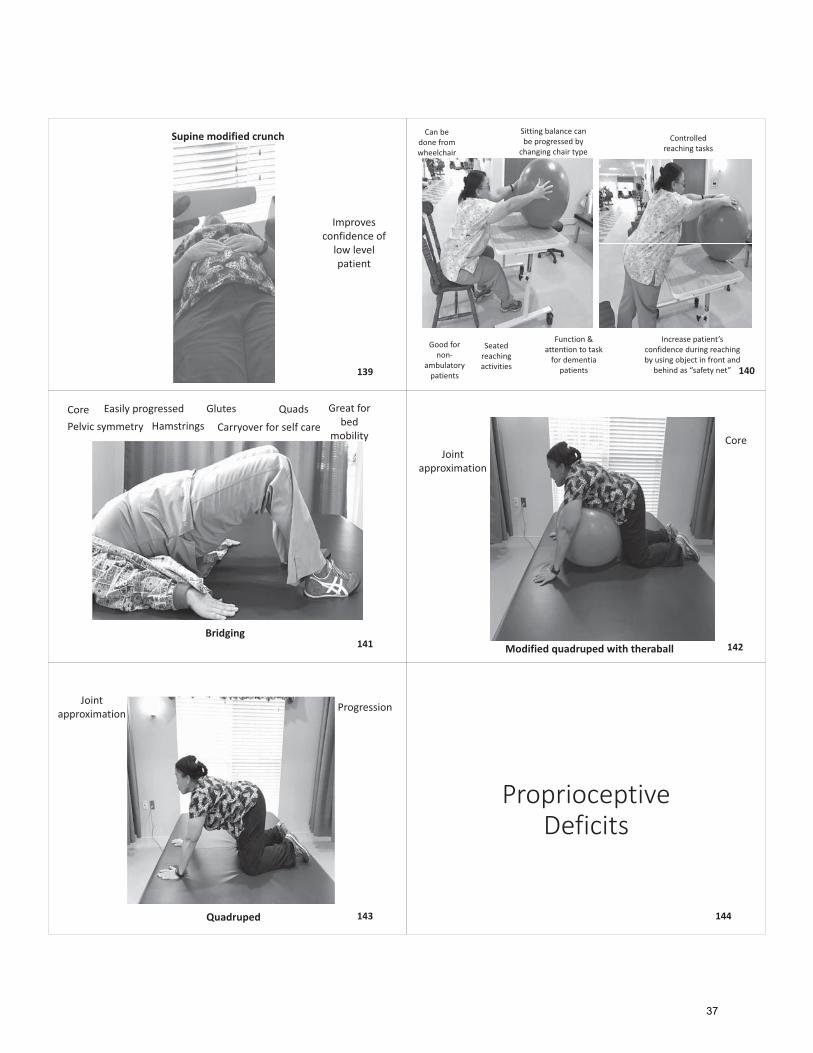
Supine�modified�crunch
Improves�confidence�of�low�level�patient
139
Seated�reaching�activities
Sitting�balance�can�be�progressed�by�changing�chair�type
Can�be�done�from�wheelchair
Good�for�non�
ambulatory�patients
Function�&�attention�to�task�for�dementia�patients
Increase�patient’s�confidence�during�reaching�by�using�object�in�front�and�
behind�as�“safety�net”
Controlled�reaching�tasks
140
Bridging
GlutesCoreHamstringsPelvic�symmetry
Easily�progressed
Carryover�for�self�careQuads Great�for�
bed�mobility
141 Modified�quadruped�with�theraball
CoreJoint�
approximation
142
Quadruped
ProgressionJoint�approximation
143
Proprioceptive�Deficits
144
37
What�about�the�patient�with�proprioceptive�deficits?�
•Proprioception�refers�to�the�ability�to�utilize�sensory�information�to�understand�where�one’s�body�parts�are�in�space– peripheral�kinesthetic�sense
• Impaired�proprioception�can�have�a�significant�effect�on�balance�and�safety�awareness
145
Propriceptive Deficits• Retropulsion• The�patient�who�is�constantly�leaning�backward�and�often�reports�falling�backward
• Incorrect�perception�of�midline�– patient�feels�like�leaning�backward�is�midline�so�anything�anterior�to�that�feels�like�falling
• Often�seen�in�patients�with�fear�of�falling�
146
Proprioceptive�Deficits• How�do�we�address�retropulsion?• Start�with�the�basics
• Promote�a�proper�sit�to�stand�transition
• Patient�must�be�re�acclimated�to�midline
• Place�patient�against�a�wall�– this�will�remove�the�option�of�leaning�backward• Progress�to�reaching,�forward�flexion,�moving�away�from�wall
• Unsupported�standing�progression147 Wall�Standing
Great�way�to�promote�proper�standing�posture
Midline�orientation
Easily�progressed�
with�reaching�tasks
Can�be�done�in�any�setting�and�with�little�space
148
Proprioceptive�Deficits• Impaired�lower�extremity�sensation• Compensatory�strategies�• Teach�patient�to�“feel”�proper�center�of�mass�over�base�of�support�position�• Visual�cues�• Focus�on�righting�strategies• Ankle�strength�and�stability�very�important�• Teaching�multi�tasking�very�important
• i.e.�scanning�environment�during�ambulation,�head�turns
• Assistive�devices�are�very�helpful�in�this�population
149
Gait�Abnormalities�that�Play�a�Role�in�Falls
150
38
Gait�Terminology�Review• Traditional/Ranchos�Los�Amigos• Stance�Phase
• Heel�strike/Initial�Contact
• Foot�flat/Loading�response
• Midstance/Midstance• Heel�off/Terminal�stance
• Toe�off/Preswing
• Traditional/Ranchos�Los�Amigos• Swing�Phase
• Acceleration/Initial�swing
• Midswing/Midswing• Deceleration/Terminal�Swing
151
Correction�of�Gait�Abnormalities�
• Foot�Drop
• Scissoring�
• Trendelenburg�
• Slow�walking�speed
• Parkinsonian�Gait�Deficits
152
Foot�Drop
• Often�a�result�of�neurological�impairments
•Weakness�or�misfiring�of�tibialis�anterior�muscle
• Patient�unable�to�utilize�proper�heel�to�toe�gait�pattern
• Places�patient�at�high�risk�for�falls�due�to�“toe�drag”�
153
Foot�Drop:�Ankle�Foot�Orthoses�(AFO)
154
AFO:�Posterior�Leaf�Spring
155
AFO:�Posterior�Leaf�Spring
• Custom�or�off�shelf
•Mild�to�moderate�foot�drop
• During�early�stance�the�upright�bends�backward�slightly�when�patient�applies�force�to�foot
•When�patient�progresses�into�swing�phase�the�plastic�recoils�forward�to�lift�foot
156
39
AFO:�Solid�Ankle
157
AFO:�Solid�Ankle
• Custom�only
•More�options�for�control�of�medial�lateral�instability
• Can�be�set�in�varying�degrees�of�ankle�dorsiflexion�or�plantarflexion
• Can�accommodate�for�edema�or�contractures
• Bulkier�than�posterior�leaf�spring158
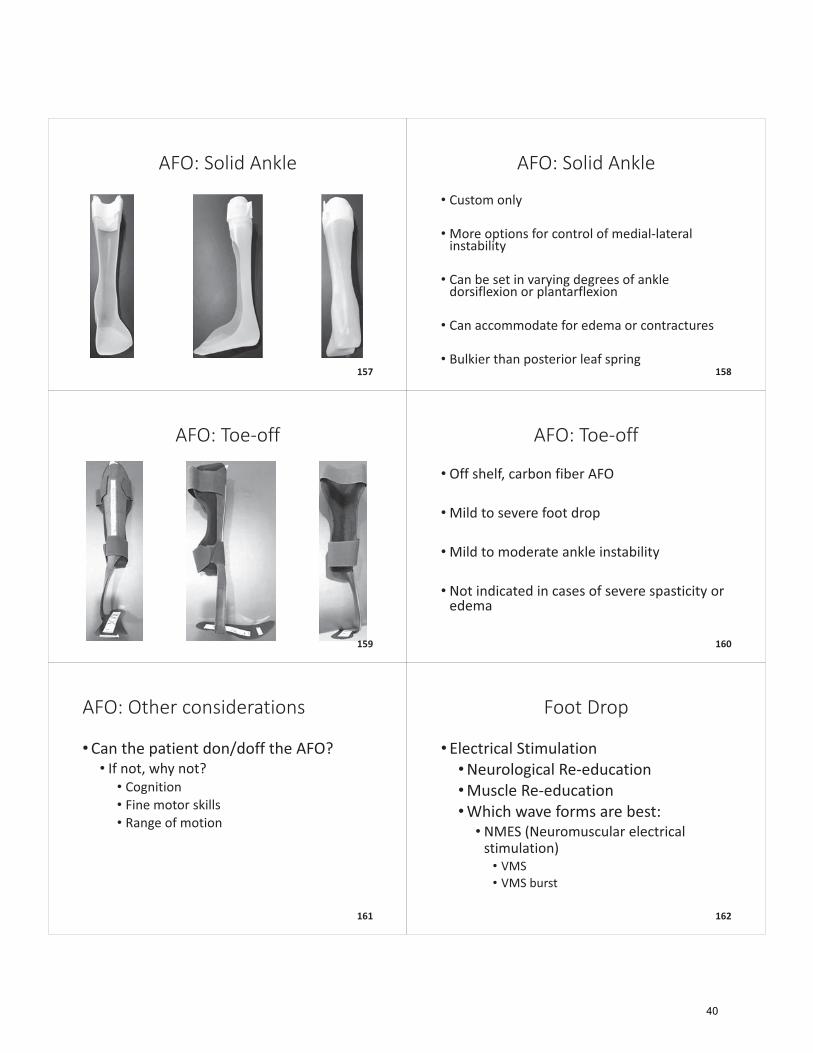
AFO:�Toe�off
159
AFO:�Toe�off
• Off�shelf,�carbon�fiber�AFO
•Mild�to�severe�foot�drop
•Mild�to�moderate�ankle�instability
• Not�indicated�in�cases�of�severe�spasticity�or�edema
160
AFO:�Other�considerations
•Can�the�patient�don/doff�the�AFO?• If�not,�why�not?• Cognition• Fine�motor�skills• Range�of�motion
161
Foot�Drop
• Electrical�Stimulation•Neurological�Re�education•Muscle�Re�education�•Which�wave�forms�are�best:• NMES�(Neuromuscular�electrical�stimulation)• VMS• VMS�burst�
162
40
Foot�Drop:�Electrical�Stimulation�Placement
163
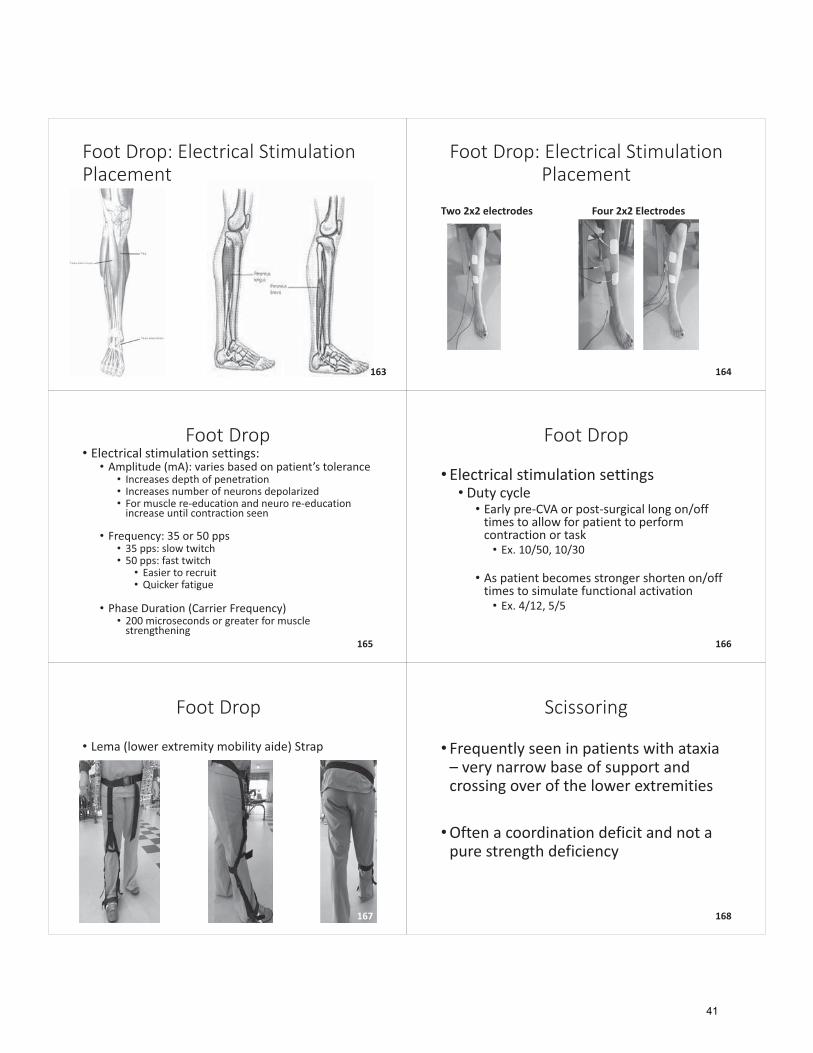
Foot�Drop:�Electrical�Stimulation�Placement
Two�2x2�electrodes Four�2x2�Electrodes
164
Foot�Drop• Electrical�stimulation�settings:• Amplitude�(mA):�varies�based�on�patient’s�tolerance
• Increases�depth�of�penetration• Increases�number�of�neurons�depolarized• For�muscle�re�education�and�neuro�re�education�increase�until�contraction�seen
• Frequency:�35�or�50�pps• 35�pps:�slow�twitch• 50�pps:�fast�twitch
• Easier�to�recruit• Quicker�fatigue
• Phase�Duration�(Carrier�Frequency)• 200�microseconds�or�greater�for�muscle�strengthening
165
Foot�Drop
• Electrical�stimulation�settings• Duty�cycle• Early�pre�CVA�or�post�surgical�long�on/off�times�to�allow�for�patient�to�perform�contraction�or�task• Ex.�10/50,�10/30
• As�patient�becomes�stronger�shorten�on/off�times�to�simulate�functional�activation• Ex.�4/12,�5/5
166
Foot�Drop
• Lema (lower�extremity�mobility�aide)�Strap
167
Scissoring
• Frequently�seen�in�patients�with�ataxia�– very�narrow�base�of�support�and�crossing�over�of�the�lower�extremities
•Often�a�coordination�deficit�and�not�a�pure�strength�deficiency�
168
41
Scissoring
• Increasing�base�of�support�to�increase�stability• Start�basic• Pre�gait�stepping�strategies• Tai�Chi�stepping�tasks• Standing�coordination�tasks�that�promote�increased�base�of�support
• Visual�feedback• Create�a�”pathway”�with�appropriately�spaced�tape�to�acclimate�patient�to�maintaining�a�wider�base�of�support�during�ambulation
169
Exaggerated�pathway
Visual�feedback�to�improve�base�of�support
Great�way�to�re�train�proper�mechanics�in�
patient�with�coordination�deficits
170
Alternating�cone�tapping
Great�for�ataxia�or�other�
coordination�deficits
Promotes�concentric�
and�eccentric�muscle�controlCarryover�with�
increased�step�length�during�reciprocal�movement� 171
Trendelenburg�
• Presents�as�a�“dropping”�of�the�pelvis�during�swing�phase
• Leads�to�increased�energy�expenditure�during�ambulation�– reduces�gait�efficiency�and�endurance
• Indicates�weakness�of�the�_____________
172
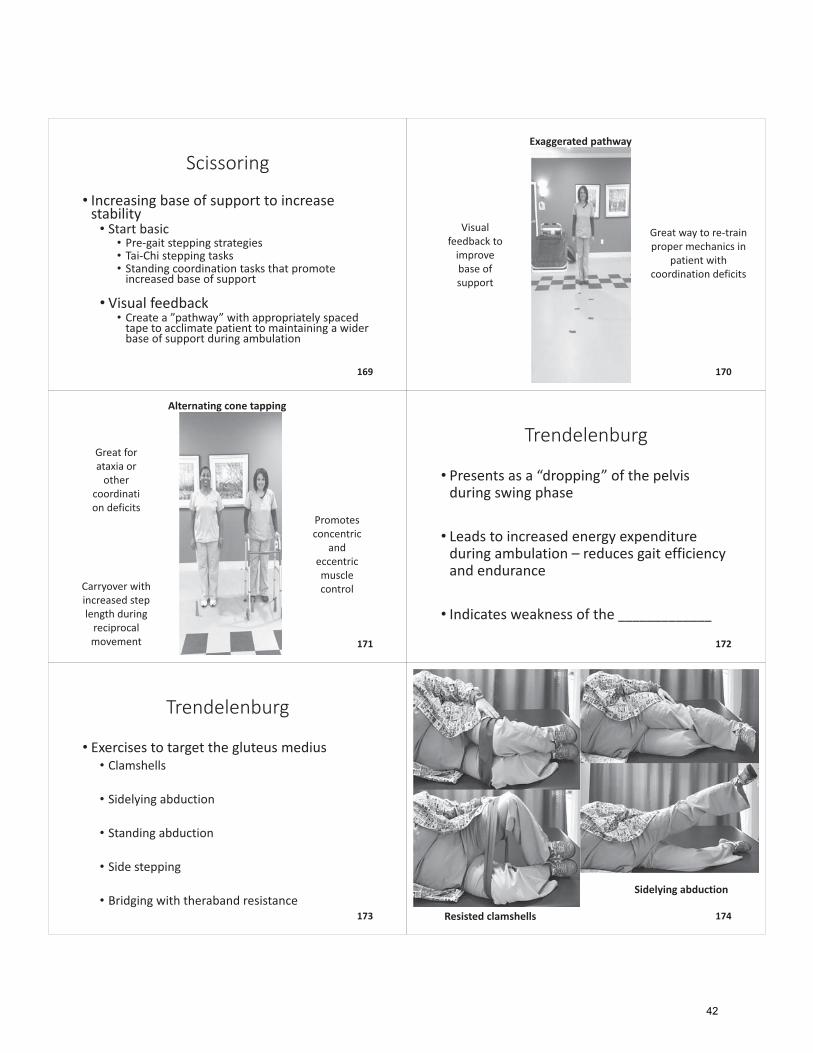
Trendelenburg
• Exercises�to�target�the�gluteus�medius• Clamshells
• Sidelying abduction
• Standing�abduction
• Side�stepping
• Bridging�with�theraband resistance173 Resisted�clamshells
Sidelying abduction
174
42
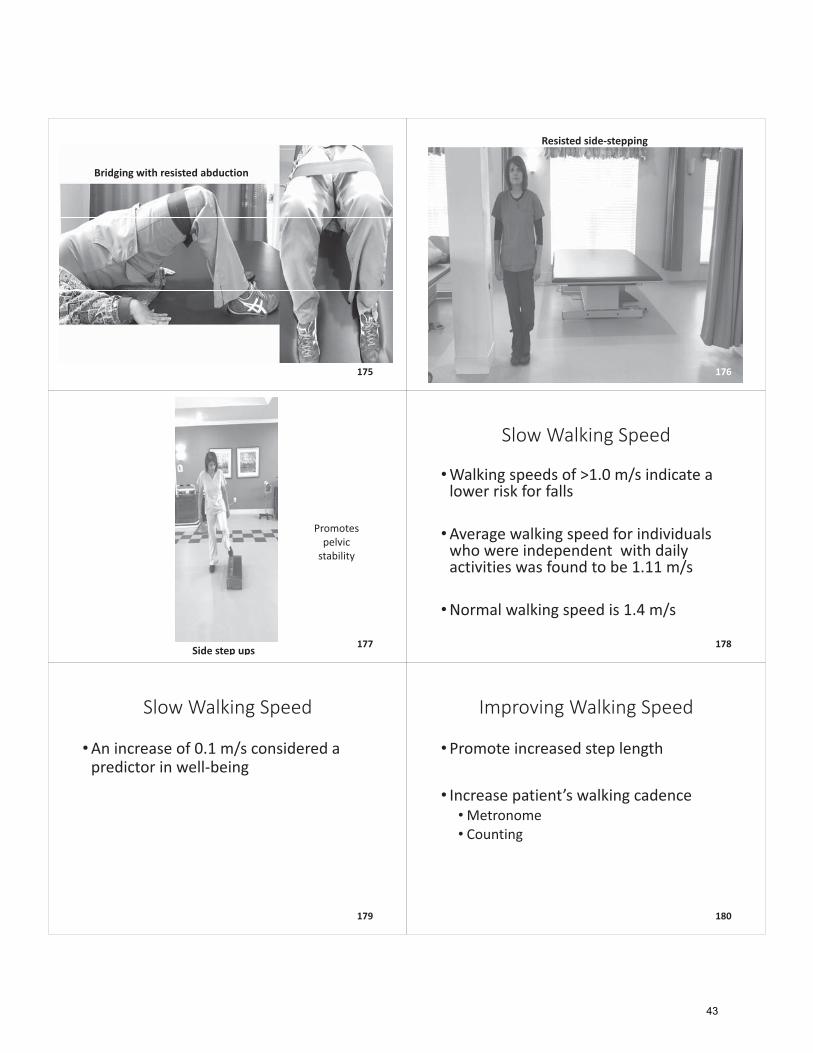
Bridging�with�resisted�abduction
175
Resisted�side�stepping
176
Side�step�ups
Promotes�pelvic�stability
177
Slow�Walking�Speed
•Walking�speeds�of�>1.0�m/s�indicate�a�lower�risk�for�falls
•Average�walking�speed�for�individuals�who�were�independent� with�daily�activities�was�found�to�be�1.11�m/s
•Normal�walking�speed�is�1.4�m/s
178
Slow�Walking�Speed
•An�increase�of�0.1�m/s�considered�a�predictor�in�well�being
179
Improving�Walking�Speed
•Promote�increased�step�length
• Increase�patient’s�walking�cadence•Metronome• Counting�
180
43
Parkinsonian�Gait�Deficits• Difficulty�with�initiation• Shuffling• Freezing• Rigidity• Bradykinesia�(slow�movements)• Akinesia�(hesitancy)• Hypokinesia (reduced�amplitude)
181
Parkinson’s�Treatment
• In�recent�years,�treatment�of�Parkinson’s�Disease�has�shifted�from�reactive�to�preventative�
•What�is�LSVT?�–Lee�Silverman�Voice�Treatment�began�with�LOUD,�focusing�on�the�speech�motor�system�
• Extended�to�LSVT�BIG,�focusing�on�limb�motor�systems�in�individuals�with�Parkinson’s�Disease
182
Parkinson’s�Treatment:�LSVT�BIG• Promote�exaggerated�movements�with�increased�amplitude
• Leads�to�increased�speed�and�precision�of�movement�
• Continuous�feedback�on�motor�performance�provided�to�counteract�reduced�gains�due�to�impaired�sensorimotor�processing
• Repetition�of�tasks�is�utilized�to�promote�carryover–minimum�of�15�repetitions�
• Visual�feedback,�i.e.�video�of�patient�walking�to�show�that�their�“big”�movements�are�actually�normal�movements�
183
Resources:�LSVT�BIG�Certification
•www.lsvtglobal.com
• 2�day�course
184
Upper�Extremity�Contributors�to�Poor�
Gait�Mechanics
185
Upper�Extremity�Contributors
• Flaccid�upper�extremity
•Upper�extremity�weight�bearing�restrictions
186
44
Flaccid�Upper�Extremity
• Limits�types�of�assistive�devices�that�may�be�utilized
•Causes�asymmetrical�weight�distribution�in�standing
187
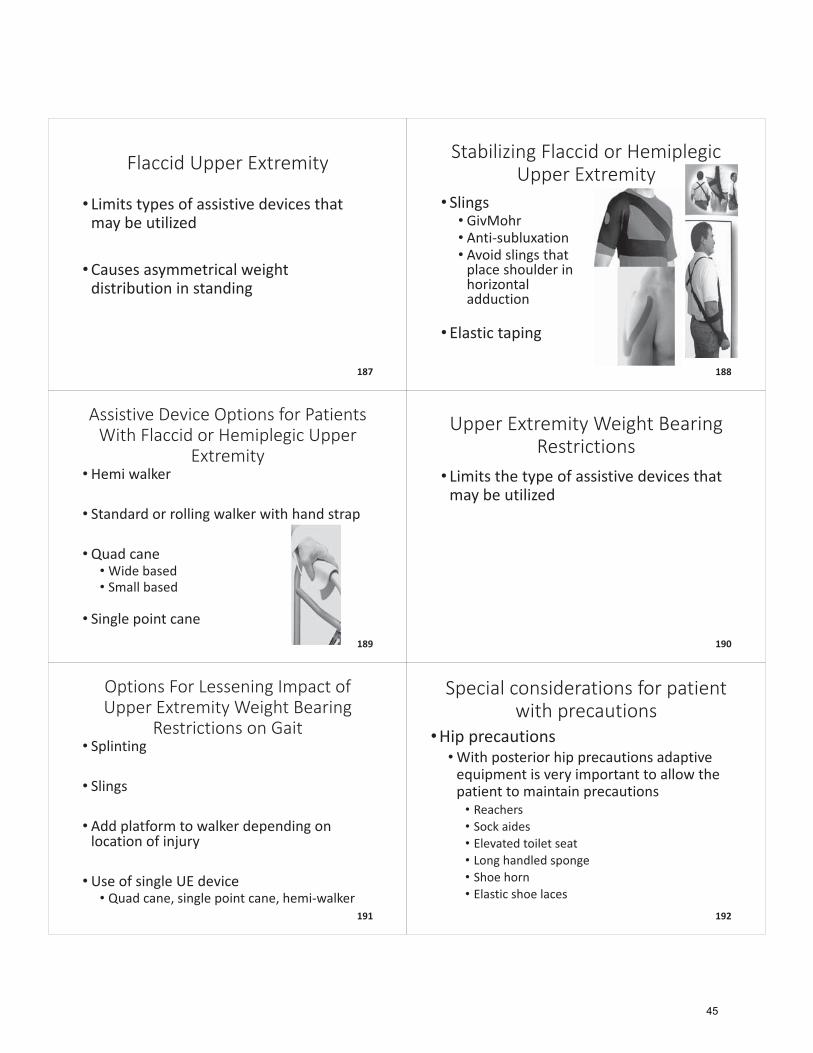
Stabilizing�Flaccid�or�Hemiplegic�Upper�Extremity
• Slings• GivMohr• Anti�subluxation• Avoid�slings�that�place�shoulder�in�horizontal�adduction
• Elastic�taping
188
Assistive�Device�Options�for�Patients�With�Flaccid�or�Hemiplegic�Upper�
Extremity• Hemi�walker
• Standard�or�rolling�walker�with�hand�strap
•Quad�cane•Wide�based• Small�based
• Single�point�cane189
Upper�Extremity�Weight�Bearing�Restrictions
• Limits�the�type�of�assistive�devices�that�may�be�utilized�
190
Options�For�Lessening�Impact�of�Upper�Extremity�Weight�Bearing�
Restrictions�on�Gait• Splinting
• Slings
• Add�platform�to�walker�depending�on�location�of�injury
• Use�of�single�UE�device• Quad�cane,�single�point�cane,�hemi�walker
191
Special�considerations�for�patient�with�precautions
•Hip�precautions•With�posterior�hip�precautions�adaptive�equipment�is�very�important�to�allow�the�patient�to�maintain�precautions• Reachers• Sock�aides�• Elevated�toilet�seat• Long�handled�sponge• Shoe�horn• Elastic�shoe�laces
192
45
Special�considerations�for�patients�with�precautions
•Back�precautions• Patient�restricted�from�bending,�twisting,�lifting
• TLSO�or�LSO�may�be�ordered�by�surgeon• Can�patient�don�and�doff?
• Adaptive�equipment�will�be�necessary�to�maintain�precautions�with�some�activities
193
Special�considerations�for�patients�with�precautions
• Sternal�precautions• No�pushing,�pulling,�lifting,�reaching�overhead,�limited�or�no�UE�weighted�exercise• Lower�extremity�strength�very�important�for�this�patient�–especially�quadriceps• Must�be�trained�to�sit�to�stand�without�use�of�upper�extremities• Education�regarding�sternal�incision�important• Frequent�short�walks�are�indicated• Pacing�very�important�with�this�patient
194
Improving�balance�in�the�patient�with�lower�
extremity�weight�bearing�restrictions
195
Review:�weight�bearing�precaution�definitions
*adapted�from�the�Orthopedic�Specialists�of�North�Carolina�guidelines*
• Non�weight�bearing�(NWB)• No�weight�placed�on�injured�leg• Injured�leg�must�be�held�off�of�floor�when�standing�or�walking
• Toe�touch�weight�bearing�(TTWB)�or�touch�down�weight�bearing�(TDWB)• Injured�leg�can�only�touch�floor�for�balance• No�body�weight�should�be�placed�on�leg• Imagine�there�is�an�egg�under�foot�that�you�are�not�to�crush
196
Review:�weight�bearing�precaution�definitions
*adapted�from�the�Orthopedic�Specialists�of�North�Carolina�guidelines*
• Partial�weight�bearing�(PWB)• When�standing�or�walking�some�of�weight�may�be�placed�on�injured�leg• Doctor�decides�on�exact�percentage�of�weight�allowed
• Weight�bearing�as�tolerated�(WBAT)• When�standing�or�walking�patient�may�place�as�much�weight�on�leg�as�feels�comfortable• Amount�of�weight�bearing�is�guided�by�pain
• Full�weight�bearing�(FWB)• No�restriction�– full�weight�on�leg
197
Addressing�balance�in�patient�with�weight�bearing�restrictions
• Strengthening• Limb�not�being�used�normally�for�weight�bearing�tasks�• Important�to�address�strength�to�reduce�muscle�wasting/atrophy�• Upper�extremity�strength�is�very�important�for�proper�adherence�to�weight�bearing�restrictions�during�standing�and�walking�tasks
• Keep�the�core�strong• Seated�activities�on�a�ball• Place�BOSU�or�foam�mat�in�a�chair�and�have�patient�do�activities�while�on�compliant�surfaces
• Progress�to�single�leg�stance�activities�in�unilateral�NWB�and�TTWB�patient
198
46
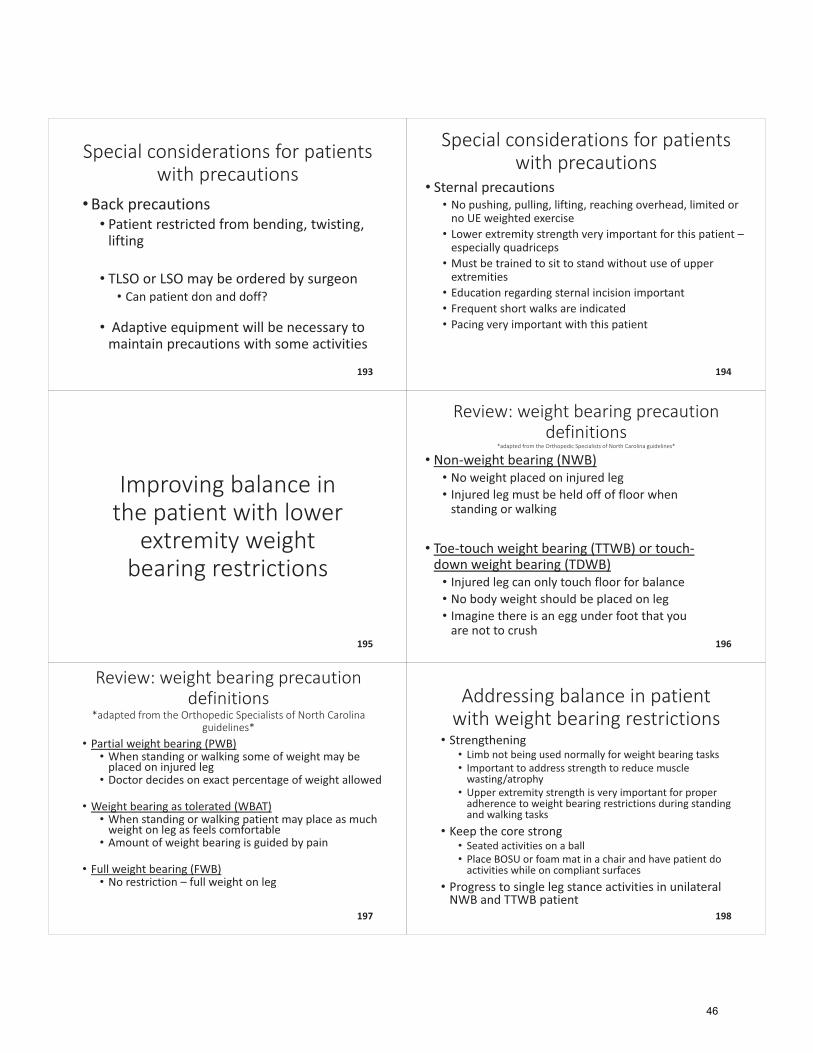
Compliant�surface�sitting�balance�tasks� 199 BOSU�sitting�activities
Increase�difficulty�of�core�stability�tasks�when�LE�
WB�restrictions�present
200
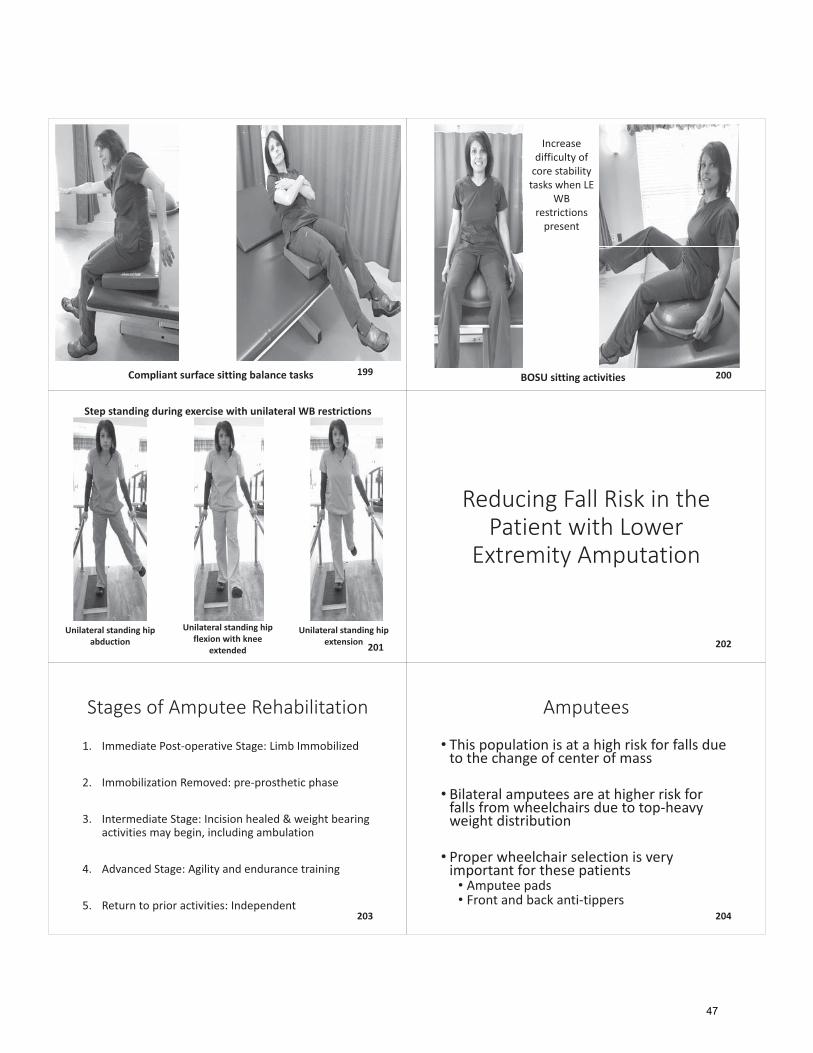
Step�standing�during�exercise�with�unilateral�WB�restrictions
Unilateral�standing�hip�abduction
Unilateral�standing�hip�flexion�with�knee�
extended
Unilateral�standing�hip�extension 201
Reducing�Fall�Risk�in�the�Patient�with�Lower�
Extremity�Amputation
202
Stages�of�Amputee�Rehabilitation
1. Immediate�Post�operative�Stage:�Limb�Immobilized
2. Immobilization�Removed:�pre�prosthetic�phase
3. Intermediate�Stage:�Incision�healed�&�weight�bearing�activities�may�begin,�including�ambulation
4. Advanced�Stage:�Agility�and�endurance�training
5. Return�to�prior�activities:�Independent203
Amputees
• This�population�is�at�a�high�risk�for�falls�due�to�the�change�of�center�of�mass
• Bilateral�amputees�are�at�higher�risk�for�falls�from�wheelchairs�due�to�top�heavy�weight�distribution
• Proper�wheelchair�selection�is�very�important�for�these�patients• Amputee�pads• Front�and�back�anti�tippers
204
47
Balance�Training�for�the�Amputee
• Sitting�balance• Because�of�the�change�of�weight�distribution,�patient�must�re�learn�proper�displacement�of�center�of�mass�(COM)�over�base�of�support�(BOS)
• Long�sitting�activities�are�a�great�starting�point
•Manual�resistance• Perturbations• PNF�techniques�(i.e.�alternating�isometrics,�rhythmic�stabilization)
205
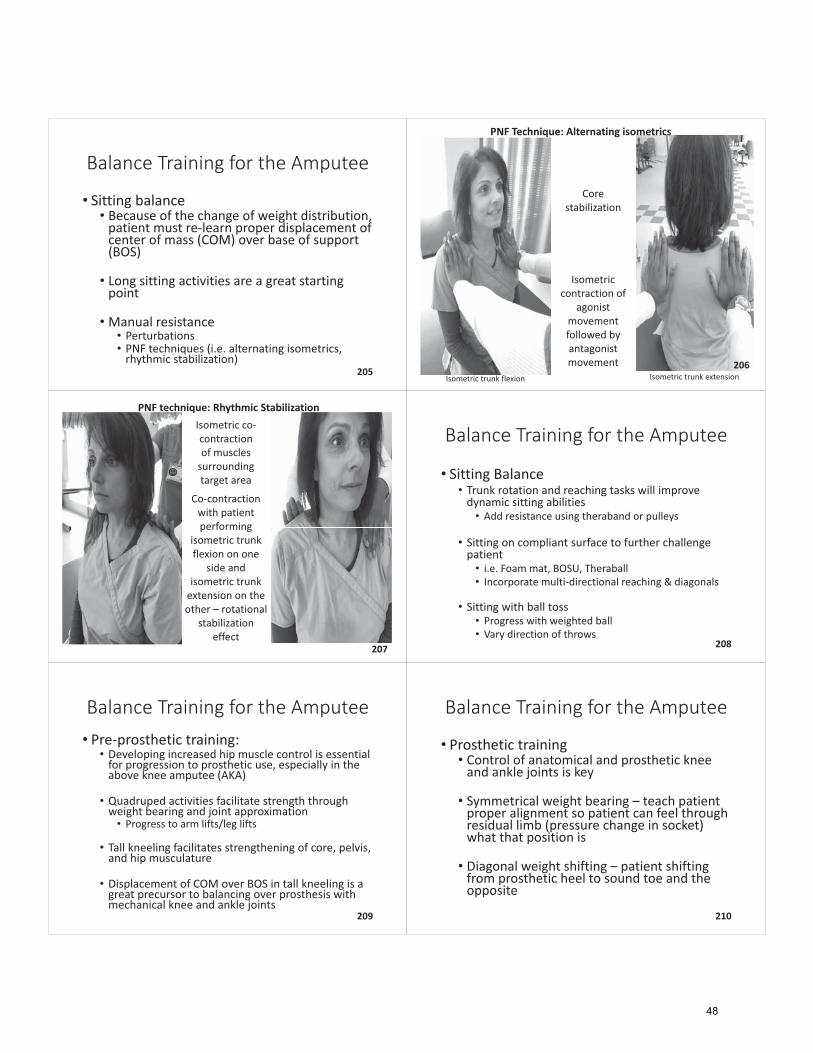
PNF�Technique:�Alternating�isometrics
Core�stabilization�
Isometric�contraction�of�
agonist�movement�followed�by�antagonist�movement
Isometric�trunk�flexion Isometric�trunk�extension206
PNF�technique:�Rhythmic�StabilizationIsometric�co�contraction�of�muscles�surrounding�target�area
Co�contraction�with�patient�performing�
isometric�trunk�flexion�on�one�
side�and�isometric�trunk�extension�on�the�other�– rotational�
stabilization�effect
207
Balance�Training�for�the�Amputee
• Sitting�Balance• Trunk�rotation�and�reaching�tasks�will�improve�dynamic�sitting�abilities• Add�resistance�using�theraband or�pulleys
• Sitting�on�compliant�surface�to�further�challenge�patient• i.e.�Foam�mat,�BOSU,�Theraball• Incorporate�multi�directional�reaching�&�diagonals�
• Sitting�with�ball�toss• Progress�with�weighted�ball• Vary�direction�of�throws
208
Balance�Training�for�the�Amputee• Pre�prosthetic�training:• Developing�increased�hip�muscle�control�is�essential�for�progression�to�prosthetic�use,�especially�in�the�above�knee�amputee�(AKA)
• Quadruped�activities�facilitate�strength�through�weight�bearing�and�joint�approximation• Progress�to�arm�lifts/leg�lifts
• Tall�kneeling�facilitates�strengthening�of�core,�pelvis,�and�hip�musculature
• Displacement�of�COM�over�BOS�in�tall�kneeling�is�a�great�precursor�to�balancing�over�prosthesis�with�mechanical�knee�and�ankle�joints
209
Balance�Training�for�the�Amputee
• Prosthetic�training�• Control�of�anatomical�and�prosthetic�knee�and�ankle�joints�is�key
• Symmetrical�weight�bearing�– teach�patient�proper�alignment�so�patient�can�feel�through�residual�limb�(pressure�change�in�socket)�what�that�position�is�
• Diagonal�weight�shifting�– patient�shifting�from�prosthetic�heel�to�sound�toe�and�the�opposite
210
48
Balance�Training�for�the�Amputee
• Prosthetic�training• Single�leg�stance�is�important�for�progression�to�proper�gait�mechanics• Without�proper�ability�to�maintain�single�leg�stance�gait�deviations�will�be�present
• Stepping�up�with�sound�limb�to�promote�stance�through�prosthesis
•Manual�perturbations�in�standing�with�prosthesis
211
Balance�Training�for�the�Amputee
•Progress�to�unsupported�balance�tasks
•When�stability�improves�patient�can�be�progressed�to�high�level�balance�challenges�that�we�would�use�with�our�non�amputee�patients
212
Preparing�Clients�for�Re�integration�to�home�and�
community
213
Home�Exercise�Program
• Continued�activity�following�discharge�is�important�in�the�maintenance�of�functional�gains
• Provide�patients�with�3�5�exercises�that�can�be�completed�safely�in�the�home
• Provide�photographs�and�descriptions�to�ensure�proper�completion�of�exercises
214
Quick�Resource�for�Home�Exercise�Programs
•www.hep2go.com
215
OTAGO
• Exercise�program�to�prevent�falls�in�older�adults�
•Created�by�Accident�Compensation�Corporation�(ACC)�in�New�Zealand
216
49
OTAGO• A�set�of�lower�extremity�strengthening�and�balance�retraining�exercises�with�progressive�difficulty�designed�to�prevent�falls
• Participants�are�expected�to�complete�strength�and�balance�exercises�3�times�per�week�and�walking��program�twice�a�week
• Participants�record�their�progress�and�instructor�(therapist)�follows�up�via�phone�or�home�visit�once�per�month
• Follow�up�face�to�face�visits�are�recommended�every�6�months
217
OTAGO�
•Program�found�to�reduce�falls�and�fall�related�injuries�by�35%
•Recommended�for�individuals�80�and�over�with�have�fallen�in�the�past�year
•OTAGO�training�for�physical�therapists�is�available�online�and�through�some�employers
218
Preparing�Patients�for�the�Unexpected
I�Fell…Now�what?
219
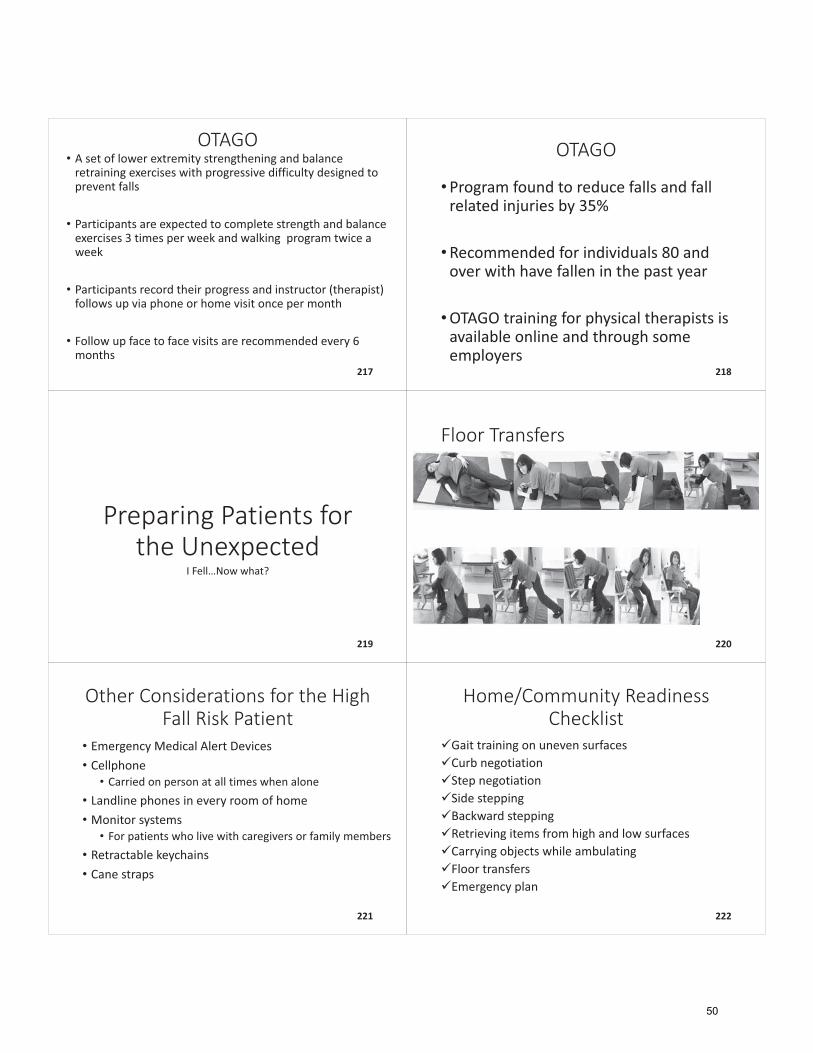
Floor�Transfers
220
Other�Considerations�for�the�High�Fall�Risk�Patient
• Emergency�Medical�Alert�Devices• Cellphone• Carried�on�person�at�all�times�when�alone
• Landline�phones�in�every�room�of�home• Monitor�systems• For�patients�who�live�with�caregivers�or�family�members
• Retractable�keychains• Cane�straps
221
Home/Community�Readiness�Checklist
�Gait�training�on�uneven�surfaces�Curb�negotiation�Step�negotiation�Side�stepping�Backward�stepping�Retrieving�items�from�high�and�low�surfaces�Carrying�objects�while�ambulating�Floor�transfers�Emergency�plan
222
50
Appropriate�DME�Recommendations
223
Medicare�Guidelines�for�DME�
•Documentation�should�include:• Physical�limitations�that�prevent�patient�from�completing�mobility�related�ADLs�in�the�home• Mental�capabilities�must�be�sufficient�for�safe�and�adequate�performance�of�mobility�related�ADLs�with�use�of�equipment• Physical�capabilities�are�sufficient�for�safe�and�adequate�performance�of�mobility�related�ADLs�with�the�use�of�equipment• Characteristics�of�home�are�suitable�for�use�of�appropriate�equipment• Patient�demonstrates�willingness�to�utilize�equipment�regularly
224
DME�Recommendations
•Based�on�individual�patient�presentation
•May�be�affected�by�other�co�morbidities
•Consider�ability�to�utilize�device�in�environment
225
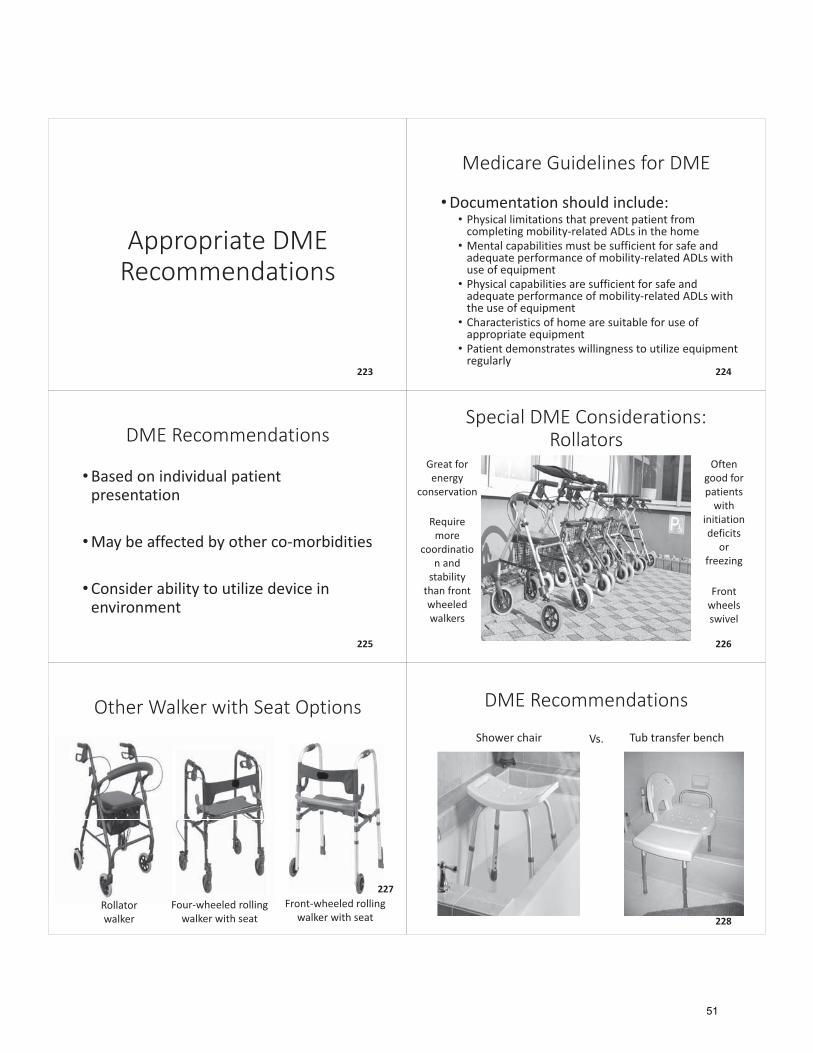
Special�DME�Considerations:�Rollators
Great�for�energy�
conservation
Often�good�for�patients�with�
initiation�deficits�
or�freezing
Require�more�
coordination�and�stability�than�front�wheeled�walkers
Front�wheels�swivel
226
Rollator�walker
Four�wheeled�rolling�walker�with�seat
Front�wheeled�rolling�walker�with�seat
Other�Walker�with�Seat�Options
227
DME�Recommendations�
Shower�chair Vs. Tub�transfer�bench
228
51
Other�Recommendations
Hanging�shoe�rack Pant�clipPush�lights
229
Environmental�Modifications
If�Home�Assessment�is�Possible
230
What�is�the�safest�method�to�enter�home?
• If�there�are�multiple�options�for�entry,�which�is�the�safest?•Which�is�the�most�used�by�patient?
231
Hallways
•Are�they�wide�enough�for�patient’s�assistive�device�if�used?• If�not,�what�alternative�methods�are�appropriate?
•Are�hallways�free�of�clutter�and�tripping�hazards?
232
Bathroom
• Can�assistive�device�fit�through�bathroom�door?• If�not,�what�other�methods�can�be�utilized?
• Can�patient�safely�enter�and�exit�tub?��• If�not,�what�modifications�or�training�may�assist�with�this?
• Can�patient�transfer�onto�and�off�of�commode�safety?• If�not,�what�modifications�may�assist�with�this?
• Can�patient�access�items�in�cabinets�if�necessary?
233
Living�Area
•Can�patient�safety�transfer�onto�and�off�of�choice�seating?• If�not,�what�modifications�may�improve�this?
•Are�there�throw�rugs?• If�yes,�are�the�edges�secure?• Are�they�necessary?
•Does�the�area�have�sufficient�lighting?
234
52
Bedroom
• Can�patient�utilize�assistive�device�in�area?• Can�patient�access�closets�and�dresser�drawers�safely?• Can�patient�safety�transfer�onto�and�off�of�bed?• If�not,�what�are�some�suggestions?
• Is�there�a�restroom�available�in�room?• If�not,�is�a�bedside�commode�necessary�for�safety�during�the�night�hours?
• Is�patient�able�to�reach�light�source�from�bed?235
Pets
• Do�they�live�inside�the�home?
• Do�they�pose�a�tripping�hazard?
• Are�there�water/food�bowls�on�the�floor�in�walking�
areas?
• Does�the�patient�have�assistance�caring�for�them?
236
Home�Assessment�Findings
• Incorporate�home�assessment�findings�into�treatment�sessions�following�the�assessment�– this�may�require�adjustment�to�discharge�plan
• If�you�work�in�home�health�the�sky�is�the�limit�� every�treatment�session�is�an�opportunity�to�teach�a�patient�to�perform�better�in�their�own�environment
237
Environmental�Modifications
If�Home�Assessment�is�Not Possible
238
Replicating�patient’s�home�environment�in�clinic
• Ask�family�member�to�provide�photographs• Get�measurements�of:• Hallways• Doorways• Step�height• Seat�to�floor�height�for�seating�used�by�client• Height�of�bed• Toilet�height�
239
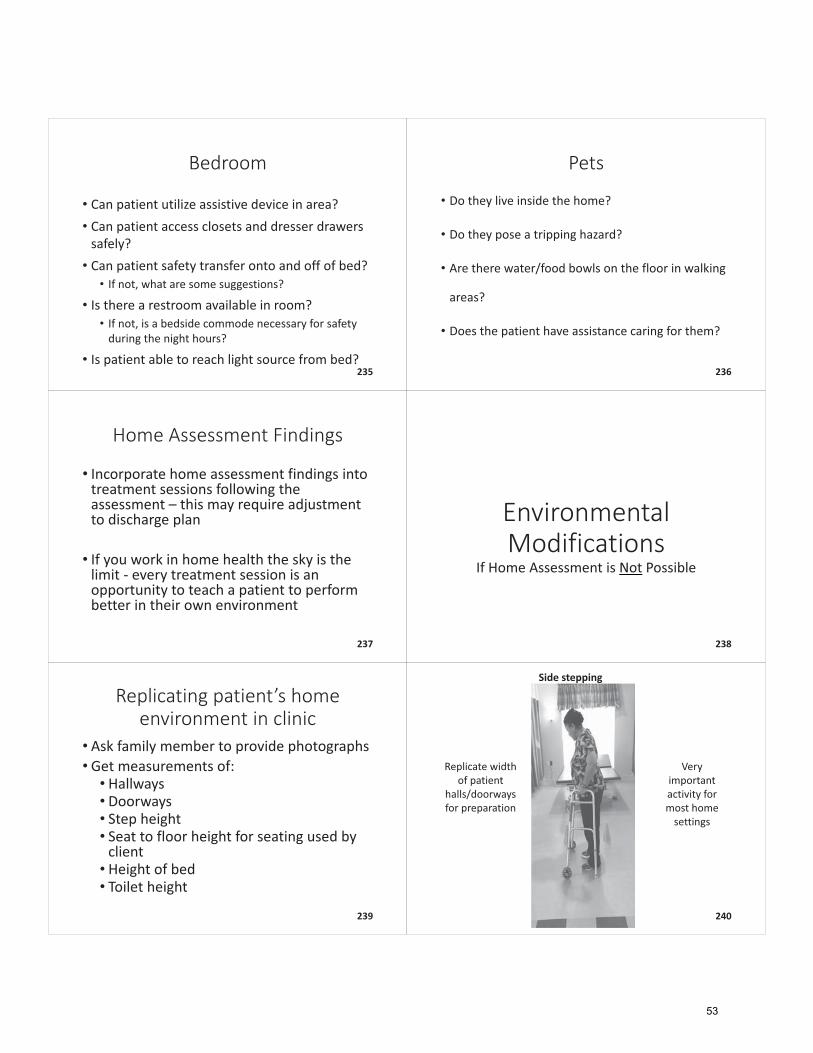
Side�stepping
Very�important�activity�for�most�home�settings
Replicate�width�of�patient�
halls/doorways�for�preparation
240
53
Moving�object�negotiation/pet�preparation
241
Documentation�of�Balance�Goals�and�Daily�
Treatment
242
Medicare�Documentation�Guidelines:�Plan�of�Care
• The�plan�of�care�should�contain,�at�minimum:• Diagnoses• Long�term�treatment�goals• Type,�amount,�duration�and�frequency�of�therapy�services• Amount�of�treatment�refers�to�the�number�of�times�in�a�day�the�type�of�treatment�will�be�provided
• Frequency�refers�to�the�number�of�times�in�a�week�the�type�of�treatment�is�provided
• Duration�is�the�number�of�weeks,�or�the�number�of�treatment�sessions
243
Medicare�Documentation�Guidelines:�Plan�of�Care
•When�devising�a�plan�of�care,�a�therapist�is�expected�to:• Establish�a�rehabilitation�diagnosis• Individualized�plan�for�each�patient�based�on�the�evaluation/examination• Establish�a�treatment�program• Specific�interventions�must�be�used�to�treat�the�patient’s�needs• (i.e.��Therapeutic�exercise,�functional�training,�manual�therapy�techniques,�adaptive�devices/equipment�needs,�modalities)
244
Medicare�Documentation�Guidelines:�Plan�of�Care�Continued
• Establish�anticipated�goals,�expected�outcomes,�any�predicted�level�of�improvement• Short�term�goals�(optional)• Long�term�goals• Determine�the�intensity,�frequency,�and�duration�of�care
• The�plan�of�care�includes�anticipated�discharge�plans
245
Medicare�Documentation�Guidelines:�Treatment�Encounter�Notes
• Record�of�all�treatment• Documentation�is�required�for�every�treatment�day,�and�every�therapy�service,�it�must�record�the:• Date�of�treatment• Treatment,�intervention,�or�activity• Total�timed�code�treatment�minutes�and�total�treatment�time�minutes�(includes�timed�and�untimed�codes)• Signature�and�professional�identity�of�qualified�professional�furnishing�treatment• Additional�information�may�be�included�(response�to�treatment,�changes) 246
54
Medicare�Documentation�Guidelines:�Treatment�Encounter�Notes
• Document�to�meet�requirements• Services�should�be�appropriate�type,�frequency,�intensity,�and�duration�for�the�individual�needs�of�patient• The�fact�that�services�are�billed�is�not�necessarily�evidence�that�they�were�appropriate• Documentation�of�objective�measures• Needs�of�patient
• Contributing�factors�i.e.�motivation,�cognition,�onset,�psychological�stability,�social�stability
247
Medicare�Documentation�Guidelines:�Reasonable�and�Necessary�Services• Services�meet�accepted�standards�of�medical�practice
• Specific�and�effective�treatment�for�the�condition
• A�level�of�complexity/sophistication�or�the�condition�of�the�patient�shall�be�such�that�the�services�required�can�be�safely�and�effectively�performed�only�by�a�qualified�therapist�(or�supervised�PTA/OTA),�and
• Patient’s�clinical�condition�requires�the�skills�of�a�therapist
248
Medicare�Documentation�Guidelines:�Services�Require�Skills�of�a�Therapist• Services�must�not�only�be�provided�by�the�qualified�professional,�but�they�must�require�the�expertise,�knowledge,�clinical�judgement,�decision�making�and�abilities�of�a�therapist�that�assistants,�qualified�personnel,�caretakers�or�the�patient�cannot�provide�independently
• A�clinician�may�not�merely�supervise,�but�must�apply�the�skills�of�a�therapist�by�actively�participating�in�the�treatment�of�the�patient�during�each�progress�reporting�period
249
Medicare�Guidelines:�Services�Require�Skills�of�a�Therapist
• A�therapist’s�skills�may�be�documented,�by�the�clinician’s�descriptions�of�their�skilled�treatment,�the�changes�made�to�the�treatment�due�to�a�clinician's�assessment�of�the�patient’s�needs�on�a�particular�treatment�day�or�changes�due�to�progress�the�clinician�judged�sufficient�to�modify�the�treatment�toward�the�next�more�complex�or�difficult�task
250
Documentation�of�Services�Related�to�Falls�and�Balance�Deficits
Now�that�we�have�the�Medicare�guidelines�down!
251 252
55
Goals�Recipe•Who?• Who�is�being�addressed�in�the�goal
•Action�words• Strong,�skilled�language�indicating�how�you�are�teaching�or�training
•Measure• Quantitative�or�qualitative�measurement�of�what�you�are�assessing
• Device:• Type�of�device�utilized�during�activity
• Time�Frame:• Based�on�therapist’s�judgement�after�reviewing�subjective�and�objective�findings�and�PLOF�information
•Why?• Explain�what�this�goal�will�accomplish 253
Who?
•Patient
•Caregiver
• Facility�staff
• Family�member254
Action�words�goal�examples�
• “will�demonstrate”
• “will�list”
• “will�report”
255
Measure• Standardized�assessment�score�(i.e.�46/56�on�BERG�balance�assessment)
• Muscle�grade�(i.e.�3/5�hip�flexor�strength)
• Balance�grade�(i.e.�Fair�dynamic�balance)
• Gait�speed�measurement�(i.e.�gait�speed�of�1.1�m/s)
• Gait�distance�(i.e.�150�feet)
• Level�of�assistance�(i.e.�Standby�assistance)256
Device• “Without�assistive�device”
• “With�rolling�walker”
• “With�single�point�cane”
• “At�wheelchair�level”
•With�hemi�walker” 257
Time�Frame
• “in�two�weeks”
• “In�four�weeks”
• Based�on�evaluation�time�frames�selected�by�therapist
258
56
Why?• “To�promote�return�to�prior�level�of�function
• “To�reduce�risk�for�falls�and�improve�functional�independence”
• “to�promote�return�to�prior�living�setting”
• “to�reduce�caregiver�burden”�
259
Goals:�Case�Example�– Mr.�Jones
• 72�year�old�male�who�lived�independently�in�single�level�home�with�3�steps�to�enter�with�hand�rail�on�right�side�going�up.��
• Was�independent�with�all�mobility,�ADL,�and�IADL�and�managed�all�medication�and�finances
• He�did�not�use�any�assistive�devices�prior�to�hospitalization
• He�has�a�walk�in�shower�without�shower�chair�and�handheld�shower�head
• He�was�driving�and�volunteered�at�the�senior�center�3�days�a�week
260
Goals:�Case�Example�� Mr.�Jones
• Mr.�Jones�was�hospitalized�for�5�days�with�community�acquired�pneumonia�and�has�now�completed�antibiotic�course�and�has�been�admitted�to�rehab�in�skilled�nursing�facility
• On�evaluation�Mr.�Jones�required�contact�guard�assistance�for�sit�to�stand�and�was�able�to�ambulate�150�feet�using�rolling�walker�with�contact�guard�assistance�before�needing�to�sit�due�to�fatigue
• BERG�balance�assessment�score�was�38/56�and�TUG�test�was�performed�in�36�seconds�using�a�rolling�walker
261
Goals:�Case�Example�– Mr.�Jones
• He�completed�shower�with�contact�guard�assistance�to�transfer�to�shower�bench�and�bathed�upper�body�with�set�up�and�required�Min�A�for�lower�body�bathing�secondary�to�difficulty�maintaining�sitting�balance�while�lifting�foot�off�of�floor
• He�was�able�to�don�shirt�with�Mod�I�and�required�Min�A�for�lower�body�dressing�and�clothing�management�due�to�instability�in�standing
262
Goals:�Case�Example�– Mr.�Jones
• Using�our�goals�cookbook�as�a�reference,�write�a�recipe�for�Mr.�Jones’�short�term�and�long�term�goals
• Be�sure�to�focus�on�areas�that�will�increase�his�safety�and�promote�return�to�independence�
263 264
57
265 266
Daily�Documentation�Recipe
• Who?• Who�is�being�addressed�in�the�activity?
• Action�words• Strong,�skilled�statements
• What?• Name�specific�activity�or�exercises
• How?• What�are�specific�details�of�activity?
• Cuing?• What�cuing�strategies�were�utilized?
• Why• What�is�the�benefit�of�this�activity?
• Patient�Response• What�are�objective�or�subjective�patient�responses�noted�during�treatment?�
267
Who?
•Patient
•Caregiver
• Facility�staff
• Family�member268
Action�words:�DDo’s
• Instruct• Direct• Educate• Create• Train• Demonstrate• Problem�Solve• Stabilize
• Plan• Assess• Formulate• Solve• Grade• Develop• Adapt• Challenged
269
Action�Words:�DDont’s
• Helped• Motivate• Assisted• Encouraged• Patient�Seen
• Monitor• Slow�progress• Repeated• Review• Practice
270
58
Action�words�daily�notes�examples
• “was�instructed�in”
• “was�educated�regarding”
• “was�assessed”
271
What?
• “dynamic�standing�on�foam�while�reaching�outside�base�of�support”
• “obstacle�negotiation�on�even�surfaces”
• “step�negotiation�using�unilateral�hand�rail”
272
How?
• “without�assistive�device”
• “with�single�upper�extremity�support”
• “with�contact�guard�assistance”
273
Cuing
• “with�verbal�cues�for�environmental�awareness”
• “with�tactile�cues�for�posture”
• “with�visual�cues�to�promote�increased�base�of�support”�
274
Why?
• “to�elicit�ankle�and�hip�strategies�to�improve�patient’s�righting�responses�and�reduce�risk�for�falls”
• “to�improve�postural�awareness�during�activities�of�daily�living�to�promote�increased�stability�and�functional�independence”
275
Patient�Response
• “patient�had�two�episodes�of�loss�of�balance�during�turning”
• “patient�demonstrates�increased�trunk�control�with�repetition�of�activity”
• “patient�required�seated�rest�break�following�bout�secondary�to�fatigue”
276
59
Daily�Notes:�Case�Example�– Mr.�Jones
• During�his�treatment�session�today�Mr.�Jones�completed�balance�activities�lead�by�his�physical�therapist• Mr.�Jones�stepped�onto�foam�mat�and�therapist�asked�Mr.�Jones�to�move�his�feet�apart�to�steady�himself• Mr.�Jones�performed�activity�where�he�reached�in�various�directions�while�remaining�on�foam�mat• Mr.�Jones�lost�his�balance�twice�during�this�task�but�he�was�able�stabilize�at�the�ankles�to�correct�balance�without�assistance�from�therapist• The�therapist�remained�in�contact�with�the�patient�to�steady�him�if�needed�but�did�not�provide�physical�assistance�during�task
277
Daily�Notes:�Case�Example�– Mr.�Jones
•Use�your�daily�notes�recipe�to�create�a�daily�documentation�note�for�Mr.�Jones
278
279 280
Documentation�and�Productivity
•Productivity�varies�in�each�setting
•One�common�theme�across�settings�is�the�rise�of�productivity�standards
•What�effect�do�productivity�standards�have�on�you�as�a�therapist?
281
Documentation�and�Productivity• What�are�some�ways�to�improve�productivity?• Point�of�service�documentation
• When�we�provide�this�type�of�documentation,�it�is�important�that�we�incorporate�the�patient• Document�during�therapeutic�rest�breaks• Standing�desks�for�therapists• During�evaluation�and�progress�reports�discuss�the�information�you�are�inputting�and�how�it�affects�the�patient• This�is�a�great�time�to�ask�the�patient�how�they�feel�they�are�progressing• Get�patient�input�on�goals�and�progress
282
Additional Supplements are available at the below link:https://blog.summit-education.com/singleton/
60
References
Alzheimer’s Association. “What is Alzheimer’s?” “Dementia with Lewy Bodies.” “Vascular Dementia.” www.alz.org. Web. 12 Feb. 2017. American Macular Degeneration Foundation. “What is Macular Degeneration?” www.macular.org. Web. 05 Mar. 2017. Anacker, S. and Difabio, R. (2016). Influence of Sensory Inputs on Standing Balance in Community-Dwelling Elders with a Recent History of Falling. Physical Therapy, 72 (8). 575-581. Avin, K., et. al. (2015). Management of Falls in Community Dwelling Older Adults: Clinical Guidance Statement from the Academy of Geriatric Physical Therapy of the American Physical Therapy Association. Physical Therapy, 95 (6). 815-834. Campbell, S. (2005). Deteriorating Vision, Falls, and Older People: The Links. Published by Visibility. ISBN 0 951 52874 2. 1-43. Centers for Medicare & Medicaid Services. www.cms.gov. Web. 8 Mar 2017. Fischer, B., et. al. (2014). Declining Cognition and Falls: Role of Risky Performance of Everyday Mobility Activities. Physical Therapy, 94 (3). 355 362. Fox, C., et. al. (2012). LSVT LOUD and LSVT BIG: Behavioral Treatment Programs for Speech and Body Movement in Parkinson Disease. Hindawi Publishing Corporation. Parkinson’s Disease, 2012, Article ID 391946. 1-12. Gailey, R. and Gailey, A. (1994). Balance, Agility, Coordination, and Endurance For Lower Extremity Amputees. Miami, Florida. Advanced Rehabilitation Therapy Incorporated. Kirkness, C., et. al. (2015) Race Differences: Use of Walking Speed to Identify Community Dwelling Women at Risk for Poor Health Outcomes-Osteoarthritis Initiative Study. Physical Therapy, 95 (7). 955-965. Landers, M., et. al. (2016). Balance Confidence and Fear of Falling Avoidance Behavior are Most Predictive of Falling in Older Adults: A Prospective Analysis. Physical Therapy, 96 (4). 433-442. Letgers, K. (2002). Fear of Falling. Physical Therapy, 82 (3). 264-272. Norkin, C. and White, D. (2003). Measurement of Joint Motion: A Guide to Goniometry 3rd edition. Philadelphia, Pennsylvania. F.A. Davis Company. O’Sullivan,S. and Schmitz,T. (2007). Physical Rehabilitation Fifth Edition. Philadelphia, Pennsylvania. F.A. Davis Company. Protas, E., et. al.(2005)Gaitand Step Training to Reduce Falls in Parkinson’s Disease. NeuroRehabilitation, 20. 183-190. Shumway-Cook, A., et. al. (2009). Falls in the Medicare Population: Incidence,Associated Factors,and Impact on Healthcare. Physical Therapy, 89 (4). 324-332. Stubbs, B., et. al. (2015). What Works to Prevent Falls in Community-Dwelling Older Adults? Umbrella Review of Meta-Analyses of Randomized Controlled Trials. Physical Therapy, 95 (8). 1095-1110.
61
The Continuing Education You Want. Quality Content, Live Near You, or Online 24/7/365
Any opinions, findings, recommendations or conclusions expressed by the author(s) or speaker(s) do not necessarily reflect the views of Summit Professional Education. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold with the understanding that the publisher is not engaged in rendering legal, accounting or other professional service. If legal advice or other expert assistance is required, the services of a competent professional person should be sought.
© Copyright 2018 Brandi Singleton & Summit Professional Education. No part of this workbook may be reproduced in any manner without the expressed written consent of Instructor/Credentials and Summit Professional Education.
From a Declaration of Principles jointly adopted by a committee of the American Bar Association and a committee of Publishers.
Workshop Manual ID: 4308