Embed Size (px)
Citation preview
P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
Journal of Mammary Gland Biology and Neoplasia, Vol. 9, No. 1, January 2004 ( C© 2004)
Steroid Receptors and Cell Cycle in NormalMammary Epithelium
Elizabeth Anderson1,2 and Robert B. Clarke1
The ovarian steroids estrogen and progesterone (E2 and P) are essential for normal mam-mary gland growth and development; however, the mechanisms by which they influence theproliferative activity of the mammary epithelium remain unclear. Mammary epithelial cellscells expressing the receptors for E2 and P (ER and PR respectively) are separate from, al-though often adjacent to, those capable of proliferating, implying that the ovarian steroids actindirectly via paracrine or juxtacrine growth factors to stimulate entry into the cell cycle. Alarge number of candidate factors have been identified in a variety of different experimen-tal systems, and it appears that transforming growth factor β may play a role in preventingproliferation of steroid receptor-containing cells. Dysregulation of the strict inverse relation-ship between ERα expression and proliferation is detectable in premalignant human breastlesions, indicating that it might be essential to the tumorigenic process. Challenges for thefuture include determining which of the candidates identified as being mediators of the effectsof E2 are physiologically and clinically relevant as well as finding out how ERα-containing cellsbecome proliferative during tumorigenesis. Answering these questions could greatly increaseour understanding of the factors controlling mammary gland development and the processesleading to cancer formation.
KEY WORDS: mammary epithelium; estrogen; progesterone; estrogen receptor; progesterone receptor;cell cycle.
INTRODUCTION
The mammary epithelium undergoes multiplecycles of proliferation, differentiation, apoptosis, andremodelling during the mammalian reproductivelifespan. Most malignant tumors arise within theepithelial component, and the risk of breast cancer isrelated, in part, to duration of proliferation withoutensuing differentiation. The ovarian hormones estra-diol (E2) and progesterone (P) are key regulatorsof mammary gland proliferation, and E2 has anobligate role in the development of breast cancer.However, much of our knowledge of the mechanisms
1 Christie Hospital NHS Trust, Manchester, UK.2 To whom correspondence should be addressed at Clinical Re-
search Department, Christie Hospital NHS Trust, WilmslowRoad, Manchester M20 4BX, UK; e-mail: [email protected].
by which E2 and P alter passage of breast epithelialcells through the cell cycle is derived from studies onbreast cancer cell lines in long-term culture (1), andrelatively little information is available on the effectsof steroids on the cell cycle in the normal gland. Thereare a number of reasons why this is the case, includingthe poor availability of in vitro models of normal
Abbreviations used: E2, estrogen; P, progesterone; ERα, estrogenreceptor alpha; ERβ, estrogen receptor beta; PR, progesteronereceptor; TDLU, terminal ductal lobulo-alveolar unit; TEB, ter-minal end bud; CALLA, common acute lymphoblastic leukemiaantigen; SMA, smooth muscle actin, OCP, oral contraceptive pill;HRT, hormone replacement therapy; CDK, cyclin-dependent ki-nase; CDKI, cyclin-dependent kinase inhibitor; ERKO, estro-gen receptor α knock out; PRKO, progesterone receptor knockout; RANKL, receptor activator of nuclear kappa B ligand; LIF,leukemia inhibitory factor; EGF, epidermal growth factor; IGF-I/II, insulin-like growth factor I/II; FGF, fibroblast growth factor;TGFβ, transforming growth factor beta; wt, wild type.
31083-3021/04/0100-0003/0 C© 2004 Plenum Publishing Corporation

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
4 Anderson and Clarke
mammary epithelium that retain steroid responsive-ness. Nevertheless, it is becoming clear that we cannotextrapolate all the results from studies on breastcancer cells to the normal situation. Thus, the aim ofthis article is to describe what is known about the roleof E2 and P in promoting normal mammary epithelialcell proliferation and progression through the cellcycle and to make some suggestions as to futuredirections.
Structure and Development ofthe Mammary Gland
The human breast, in common with the mam-mary glands of other species, contains both epithe-lial and mesenchymal components. The adult humanmammary gland comprises a number of “tree-like”glandular structures formed by dichotomous branch-ing of each of several ducts arising from the nipple.The major functional units of the mammary gland arethe lobular structures comprising several small blind-ended ductules situated at the end of the terminalducts and known as terminal ductal lobular units (TD-LUs). The entire ductal system is lined by a contin-uous layer of luminal epithelial cells surrounded bya layer of myoepithelial cells which, in turn, is sur-rounded by and in direct contact with a basementmembrane. The TDLUs are then surrounded by de-limiting fibroblasts and embedded in a specialized in-tralobular stroma (2). Each of these cell types canbe differentiated in terms of unique patterns of anti-gen expression. For example, only luminal epithelialcells express the sialomucin MUC1, whereas myoep-ithelial cells express the common acute lymphoblasticleukemia antigen (CALLA) and smooth muscle actin(SMA) (3–5). Each of the cell types has a characteris-tic pattern of cytokeratin expression, and all expresspanepithelial antigens such as that recognized by theBer-EP4 antibody (6,7). It is important to understandthat the majority of proliferating cells are found withinthe luminal epithelial population, whereas cell divi-sion or expression of antigens associated with prolif-eration is exceedingly rare in the myoepithelial celltype (8). Likewise, receptors for E2 and P are foundexclusively in the luminal compartment of the humanbreast (9). It is even more important to realize that,despite the current histological classification into duc-tal or lobular subtypes, most human breast tumoursarise from the TDLUs. Careful histological examina-tion reveals that most tumors have the morphologicalfeatures of luminal epithelial cells; they express the
cytokeratin profile of luminal epithelial cells togetherwith the receptors for E2 and P (4,5,10). Clearly, theluminal epithelial cell population must be regarded asthe primary target for the oncogenic events leading totumor formation.
The mammary glands of most mammalianspecies, including humans, are not fully developedand functional at birth. Instead, there is a small prim-itive ductal structure extending a small distance fromthe nipple. Between birth and puberty, the growth ofthis structure is isometric in relation to the rest ofthe body, but at puberty, under the influence of ovar-ian and pituitary hormones, the gland undergoes thefirst phase of allometric growth. In mice, this processstarts at about 21 days of age and is characterized byenlargement of the duct termini to form terminal endbuds (TEBs), which are the major sites of prolifera-tion through which ductal elongation and ramificationinto the mammary fat pad are achieved (11). In thehuman mammary parenchyma, the site of active ep-ithelial cell proliferation is also a TEB-like structure.Although the mouse and human TEB structures differin the finer details of structure and histology, a simi-lar process of dichotomous and sympodial branchingleads to the formation of increasingly smaller ductsand ductules (12). Alveolar budding at the ends ofterminal ductules eventually gives rise to the TDLUs.In humans, once menstruation is established, there isa cyclical increase in proliferation associated with theluteal phase, and the TDLUs become more elaboratein terms of the number of alveoli they contain witheach successive ovulatory cycle (12). This progressivedevelopment of the epithelium continues to the ageof approximately 35 years.
The second phase of allometric growth in themammary gland occurs during pregnancy. In micethere is an enormous increase in ductal proliferativeactivity and in the formation of alveolar buds; bylate pregnancy the alveoli fill the mammary fatpad and the luminal epithelial cells achieve theirfully differentiated function of secreting milk (13).The changes that occur in the human breast duringpregnancy and lactation are not well-describedbecause there are few specimens of tissue fromthese stages of development. However, the limitedavailable data suggest that the changes are similar tothose seen in rodent mammary glands, i.e. there is ahuge increase in the epithelial component to producemore TDLUs containing large numbers of acini (2).In rodents, once weaning has occurred, the mammarygland involutes; the secretory luminal epithelial cellsapoptose, the alveoli collapse and by 3 weeks both

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
Steroids and Normal Mammary Epithelium 5
epithelial and stromal components are remodelled toresemble the prepregnant state (13). Again there isvery little information on the involution process inthe human breast, but it is thought to be similar tothat occurring in the rodent gland.
In summary, there are two developmental stagesat which the mammary epithelium undergoes amassive increase in proliferation—puberty and earlypregnancy. In between these two stages, however,the epithelium undergoes small cyclical changes inproliferative and apoptotic activity in response to thefluctuations in ovarian hormone levels of the men-strual cycle. While it is recognized that the mammaryepithelium is particularly vulnerable to carcinogenicchallenge during puberty (14), cyclical variation inproliferation between puberty and pregnancy alsohas a highly significant effect on breast cancer risk(15,16). Therefore, there is considerable interestin understanding how the ovarian steroids controlproliferation in the mammary epithelium
The Role of Ovarian Steroids in MammaryGland Development
In terms of biological activity, E2 is the most im-portant circulating estrogen in women, whereas P isthe most important progestogen. From the advent ofmenarche until menopause both E2 and P are synthe-sized and secreted in a cyclical manner by the ovariesunder the control of the pituitary gonadotrophins.The clinical and epidemiological evidence for anobligate role of E2 in mammary gland developmentand tumor formation is considerable. The clinicalmanagement of girls with E2 deficiency from, forexample, gonadal dysgenesis or gonadotrophininsufficiency demonstrates that the steroid is strictlynecessary, although not sufficient, to induce pubertalbreast development (17). The incidence of breastcancer in men is 1% of that seen in women. Reducingexposure of the mammary epithelium to the fluctu-ating E2 and P levels of the menstrual cycle throughan early natural or artificially induced menopausesubstantially lowers the risk of developing breastcancer. Conversely, increased exposure through earlymenarche, late menopause, or late age at first full termpregnancy raises the risk of cancer, as does use ofexogenous ovarian hormones in the form of the oralcontraceptive pill (OCP) or hormone replacementtherapy (HRT) (15,16). However, treatment withantiestrogens such as tamoxifen reduces breast cancerincidence in high risk women (18). The dominant role
of E2 in mammary gland development and tumori-genesis has been confirmed in several rat and mousemodels, but perhaps the most resounding confirma-tion has come from studies on mice in which the ERαgene has been knocked out. The mammary glandsin these ER knock out (ERKO) mice comprise rudi-mentary ducts without TEBs or alveolar buds (19).These structures are confined to the nipple area andcannot be induced to develop further by E2 treatment.Moreover, the vestigial mammary glands are resis-tant, although not completely, to malignant tumorformation following introduction of oncogenes suchas wnt-1 through genetic manipulation (19). Finally,a large number of studies on rat models of mammarycarcinogenesis show that administration of exoge-nous E2 greatly enhances tumor formation whereasreduction of endogenous E2 levels through ovariec-tomy or adminstration of inhibitors of E2 synthesisreduces or even eliminates tumor incidence (20,21).
The role of P in mammary gland developmentin humans is less clear. Studies on mice in which thereceptor for progesterone (PR) has been deleted sug-gest that P promotes lobulo-alveolar development,whereas E2 stimulates ductal elongation (22). It isassumed, but is by no means clear, that P has a similarrole in the human breast and stimulates TDLUformation and expansion during puberty and preg-nancy. As far as is known, this aspect has never beendemonstrated, probably because it is almost impos-sible to study human mammary epithelium at thesedevelopmental stages. As for a role for P in breasttumorigenesis, there is now strong evidence thatexogenous progestins taken in the form of combinedHRT increase the risk of postmenopausal breastcancer to a greater extent than E2 alone (23–25).
Estrogen and Progesterone Receptorsand Their Mechanisms of Action
Steroid hormones such as E2 and P are smalllipophilic molecules that enter target cells and nucleiprimarily by diffusing through the plasma and nuclearmembranes. Once in the nucleus they encounterreceptors which bind their cognate ligands with highaffinity and specificity. There are two receptors forE2, ERα, and ERβ, both of which are members ofthe steroid/thyroid nuclear receptor superfamily ofligand-dependent transcription factors. Both the ERproteins have the modular structure that character-izes the nuclear receptor superfamily, comprising sixfunctional domains designated A-F, which include

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
6 Anderson and Clarke
regions involved in steroid binding and interactionwith DNA (26,27). Although the two ERs are highlyhomologous in their ligand- and DNA-bindingdomains, it is clear that they are derived from twoseparate genes. The ERβ is the shorter of the two, ithas a different chromosomal location and its proteinproduct is smaller. These features, together with theiroverlapping but distinctly different patterns of tissuedistribution, have led some workers to suggest thatthe ERβ mediates some of the nonclassical effectsof the estrogens and antiestrogens. Alternatively, thefact that the ERβ is expressed in some of the sametissues as the ERα has led to speculation that ERβmight interact with and modulate the actions of theERα (28).
Progesterone also has two receptors, PRA andPRB. Unlike the ERs, however, the two PRs are tran-scribed from the same gene via alternative promoterusage. PRB is longer than PRA; it contains an addi-tional 164 amino acids at its N-terminal, but other-wise the two proteins are identical (29). PRA andPRB also are members of the steroid/thyroid hor-mone nuclear receptor superfamily and function asligand-dependent transcription factors. It has beensuggested that PRB is the major activator of genetranscription, whereas PRA represses PRB activity(30). However, recent studies on breast cancer cellsengineered to express either PRA or PRB alone orin mice in which the isoforms have been selectivelydeleted suggest that PRA as well as PRB can activategene transcription (31). Moreoever, the two isoformscan be differentiated in terms of the profile of genesthat they activate and by the fact that PRB but notPRA mediates the effects of progesterone on mousemammary gland development (32).
The simplest definition of the function of steroidreceptors such as the ER and PR is that they areligand-dependent nuclear transcription factors (33).Thus, ligand binding induces formation of receptordimers which then interact with the regulatory regionsof their target genes. The receptor dimers bind eitherdirectly to specific short DNA sequences (responseelements) or to other transcription factors. They thenpromote assembly of coregulatory molecules andcomponents of the general transcription machinery,which has the net effect of overcoming the repressiveeffects of chromatin structure on gene transcription(34). In cases where gene transcription is repressedby steroid receptor action, the net effect is to pro-mote chromatin condensation. In addition to inter-acting with regulatory regions of target genes, it isbecoming clear that steroid receptors act as points
of integration with other signaling pathways. Thus,downstream effects of cell surface receptors can phos-phorylate the ER and enhance its interactions withcoregulatory molecules and/or allow binding to its re-sponse element in the absence of ligand. On the otherhand, steroid receptors appear to exert nongenomiceffects by modulating the activity of signaling proteinssuch as c-src (33).
In normal tissues, the frequency with which cellsenter the cell cycle is very tightly regulated by checkor restriction points, which cannot be passed unless astringent set of conditions is met, including the pres-ence of mitogenic signals such as estrogen. The keyfactors that regulate progression through the cell cycleare a family of proteins called the cyclin-dependentkinases (CDKs), all of which are serine/threoninekinases activated at specific points of the cell cycle tophosphorylate specific protein targets (35). As theirname suggests, activation of the CDKs requires inter-action with another set of proteins called the cyclins.Whereas CDK protein expression remains relativelyconstant through the cell cycle, cyclin protein levelsrise and fall to periodically activate the CDKs at theappropriate timepoints (36,37). The exceptions arethe D-type cyclins (cyclins D1–D3), which bind to andactivate CDK4 and CDK6 and which are essential forentry into G1 from G0 (38). In the case of these cy-clins, expression is induced by mitogenic factors andremains elevated only for as long as the factors arepresent. The other cyclin/CDK complex importantfor transition through the G1/S boundary is cyclinE/CDK2 (39). There are several mechanisms bywhich transcription of the components and activationof the cyclin/CDK complexes is regulated. For exam-ple, there are two families of cyclin dependent kinaseinhibitors (CDKIs) and the role of one of these,p27KIP1, in mammary gland development is discussedin this issue (see article by Musgrove). Other CDKIsthat are involved include p21CIP1 and membersof the INK family (40). Activation of cyclin/CDKcomplexes may itself require phosphorylation, andcyclin degradation via ubiquitin-mediated proteolysisis another important point of regulation (1).
Studies using breast cancer cell lines in culturehave identified cyclin D1 as a primary E2 target (41).The steroid appears to have a direct effect on cy-clin D1 gene transcription, and inhibition of cyclinD1 expression abrogates the effects of E2 on G1/Stransition. Estradiol also enhances the activity of thecyclin E/CDK2 complex, apparently by preventingCDKI p21CIP1 from interacting with it. Thus, cyclinD1, p21CIP1 and the cyclin E/CDK2 complex can all

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
Steroids and Normal Mammary Epithelium 7
be regarded as mediators of the effects of E2 on pro-gression of breast cancer cells through the cell cycle(1,41). The evidence presented below suggests thatthis may not be the case in the normal mammaryepithelium.
Steroid Receptor Expression in the NormalMammary Gland
Most data on ER and PR expression in the nor-mal human breast have been obtained in the courseof studies on tissue taken from adult women who areneither pregnant nor lactating. These results showthat ERα is expressed in a minority (approx. 15–30%)of luminal epithelial cells and not at all in any of theother cell types (9,42). Moreover, the ERα positivecells are scattered relatively evenly throughout themammary epithelium. Estimates of the proportion ofERα-expressing cells in luminal epithelial cells of themouse mammary gland vary from less than 10–60%according to developmental stage (43). As in thehuman gland, the ERα positive cells are scatteredevenly throughout the luminal epithelium of the adultmouse mammary gland and are never seen in themyoepithelium. Unlike the human breast, however,ERα can be detected in the stromal compartment ofthe mouse mammary gland. In fact, the receptor isdetectable only in the stroma at embryonic days 18–19, whereas luminal epithelial expression becomesevident 1 day after birth (43). In adult mice, theluminal epithelium is the major site of ERα expres-sion, although the dense stroma associated with thenipple and primary ducts still contains the receptor.Another point of divergence between humans andmice is that adipocytes in the mouse mammary fatpad express ERα, albeit heterogeneously.
Studies on ERβ expression indicate that in thenormal human breast, the ERβ is present in mostluminal epithelial and myoepithelial cells as wellas being detectable in fibroblasts and other stromalcells (44). This widespread distribution is not veryinformative as to the likely function of the ERβ innormal human breast growth and development. Fur-thermore, the results of studies on mice in which theERβ gene has been deleted indicate that mammarygland development is grossly normal, and that thefemales have no difficulty in nursing their young (45).Taken together, these data suggest that, despite itsmore restricted pattern of expression, the ERα is thekey mediator of the effects of E2 on the mammarygland.
Most of the studies in which distribution ofPR expression in the mammary gland has beenexamined were carried out before reagents capableof distinguishing between the two isoforms in tissuesections became available. In the human breast,the proportion of cells expressing the PR is verysimilar to that containing ERα, i.e. it is expressed ina minority of cells which are scattered throughoutthe luminal epithelium (42). As in the case of ERα,the PR is not expressed in the myoepithelial orstromal compartments of the human breast. Previousstudies have shown that PR expression in the luminalepithelium is regulated by E2; accordingly, dual labelimmunofluorescence techniques have been used toshow that all the cells that express PR also contain theERα (42). Recent studies which have used antibodiescapable of distinguishing PRA and PRB suggestthat the two isoforms are present in approximatelyequal amounts in the normal human mammaryepithelium and that the ratio is deranged in tumors,often favoring the A form (46). Again, estimatesof the number of PR-positive cells in the luminalepithelium of the mouse mammary gland vary ac-cording to developmental stage from about 8% in therudiment present at embryonic days 18–19 to 55%in the adult gland (43). As is the case for ERα, PRis never expressed in the myoepithelium but, unlikeERα, neither is it present in the stromal or adipocytecompartments.
E2 and P Control Normal Mammary GlandDevelopment Indirectly Via Paracrine Factors
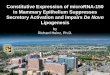
Having established major roles of E2 and P inregulating mammary gland growth and development,it was somewhat surprising to learn that, in thenormal human breast, proliferating cells containneither the ERα nor the PR (42). Instead, the steroidreceptor-expressing cells are separate from, althoughoften adjacent to, those labeled with markers ofproliferation, such as the antigen recognized bythe Ki67 antibody, or markers of S-phase, such astritiated thymidine (Fig. 1). This dissociation betweensteroid receptor expression and proliferation hasbeen confirmed by other groups in both humanbreast and in the mammary glands of mice andrats (47). The implication of this finding is that E2
and/or P control the proliferative activity of luminalepithelial cells indirectly by a mechanism in whichthe receptor-containing cells act as “sensors” thatsecrete positive or negative paracrine growth factors

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
8 Anderson and Clarke
Fig. 1. Micrograph of a section of formalin-fixed, paraffin-embedded human mammary ep-ithelium stained immunohistochemically to show expression of the progesterone receptor(indicated by the arrowheads) followed by autoradiography to demonstrate nuclei labelledwith tritiated thymidine, a marker of proliferative activity (indicate by the arrows). Bothsteroid receptor positive and proliferating cells are distributed in a punctate fashion through-out the mammary epithelium. However, cells that express steroid receptors are separate from,although often adjacent to, those that are proliferating.
according to the prevailing steroid concentration toinfluence the activity of nearby division-competentcells.
Studies on mammary tissue from ERα or PR KOmice transplanted into the cleared mammary fat padsor under the renal capsules of syngeneic or immunod-eficient mice has confirmed that the effects of E2 andP on mammary gland development are indirect andthat they are mediated by paracrine factors secretedby the epithelium itself or the surrounding stroma. Inaddition, use of the ERKO mice has revealed someinteresting differences in the roles of epithelial andstromal ERα at various developmental stages. Thus,tissue recombination studies in which mammary ep-ithelium derived from neonatal wild type (wt) mice ismixed with stroma from neonatal ERKO mice or viceversa, then implanted under the renal capsule, showthat stromal ERα is sufficient to induce mammaryductal growth (48). However, similar experiments inwhich epithelium from adult wt or ERKO mice is im-planted into the cleared mammary fat pads of otheradult wt or ERKO mice indicate that both stromaland epithelial ERα are required for ductal develop-ment at this stage (49). These findings are in agree-ment with those showing that in neonatal mice ERα isexpressed only in the stroma, whereas at later stages
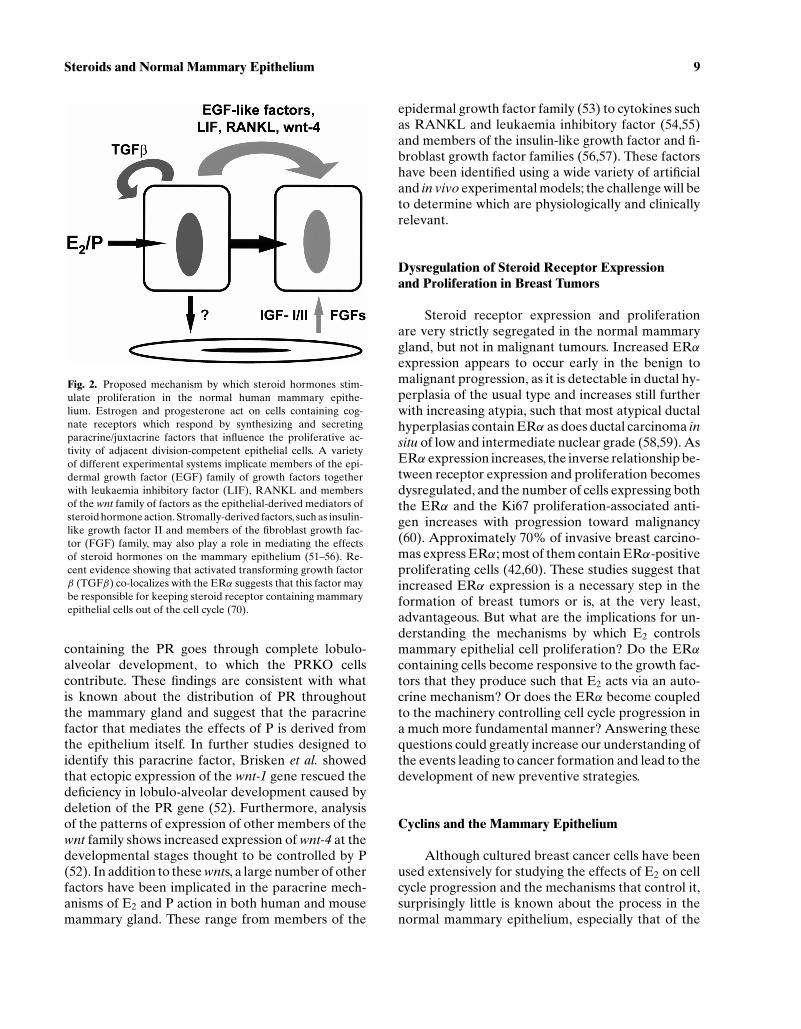
of development the receptor is to be found in boththe epithelial and stromal components (43). It is notclear whether the stroma plays a role in controlling theductal development of the human breast; however, itseems unlikely as ERα has not yet been detected inthe stromal compartment at any of the developmen-tal stages examined (50). It would appear thereforethat the paracrine factors that mediate the effects ofE2 on the human breast epithelium are derived fromthe epithelium itself (Fig. 2).
The involvement of a paracrine factor that medi-ates the effects of P on lobulo-alveolar developmenthas been demonstrated by Brisken et al. in a set ofelegant experiments in which mammary epitheliumisolated from PRKO mice was implanted into fatpads of either wt or PRKO mice and vice versa (51).In some cases, PRKO epithelium was combined withthat from ROSA26 transgenic animals which stablyexpress β-galactosidase in most of their tissues andwhich allows the PRKO epithelium to be discernedfrom the wt after mixing. These studies show that wtmammary epithelium transplanted into stroma lack-ing PR develops normally, whereas PRKO epitheliumfails to form lobulo-alveolar structures even whenimplanted into wt fat pads. The chimeric epitheliumin which PRKO cells are in close proximity to those
P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
Steroids and Normal Mammary Epithelium 9
Fig. 2. Proposed mechanism by which steroid hormones stim-ulate proliferation in the normal human mammary epithe-lium. Estrogen and progesterone act on cells containing cog-nate receptors which respond by synthesizing and secretingparacrine/juxtacrine factors that influence the proliferative ac-tivity of adjacent division-competent epithelial cells. A varietyof different experimental systems implicate members of the epi-dermal growth factor (EGF) family of growth factors togetherwith leukaemia inhibitory factor (LIF), RANKL and membersof the wnt family of factors as the epithelial-derived mediators ofsteroid hormone action. Stromally-derived factors, such as insulin-like growth factor II and members of the fibroblast growth fac-tor (FGF) family, may also play a role in mediating the effectsof steroid hormones on the mammary epithelium (51–56). Re-cent evidence showing that activated transforming growth factorβ (TGFβ) co-localizes with the ERα suggests that this factor maybe responsible for keeping steroid receptor containing mammaryepithelial cells out of the cell cycle (70).
containing the PR goes through complete lobulo-alveolar development, to which the PRKO cellscontribute. These findings are consistent with whatis known about the distribution of PR throughoutthe mammary gland and suggest that the paracrinefactor that mediates the effects of P is derived fromthe epithelium itself. In further studies designed toidentify this paracrine factor, Brisken et al. showedthat ectopic expression of the wnt-1 gene rescued thedeficiency in lobulo-alveolar development caused bydeletion of the PR gene (52). Furthermore, analysisof the patterns of expression of other members of thewnt family shows increased expression of wnt-4 at thedevelopmental stages thought to be controlled by P(52). In addition to these wnts, a large number of otherfactors have been implicated in the paracrine mech-anisms of E2 and P action in both human and mousemammary gland. These range from members of the
epidermal growth factor family (53) to cytokines suchas RANKL and leukaemia inhibitory factor (54,55)and members of the insulin-like growth factor and fi-broblast growth factor families (56,57). These factorshave been identified using a wide variety of artificialand in vivo experimental models; the challenge will beto determine which are physiologically and clinicallyrelevant.
Dysregulation of Steroid Receptor Expressionand Proliferation in Breast Tumors
Steroid receptor expression and proliferationare very strictly segregated in the normal mammarygland, but not in malignant tumours. Increased ERαexpression appears to occur early in the benign tomalignant progression, as it is detectable in ductal hy-perplasia of the usual type and increases still furtherwith increasing atypia, such that most atypical ductalhyperplasias contain ERα as does ductal carcinoma insitu of low and intermediate nuclear grade (58,59). AsERα expression increases, the inverse relationship be-tween receptor expression and proliferation becomesdysregulated, and the number of cells expressing boththe ERα and the Ki67 proliferation-associated anti-gen increases with progression toward malignancy(60). Approximately 70% of invasive breast carcino-mas express ERα; most of them contain ERα-positiveproliferating cells (42,60). These studies suggest thatincreased ERα expression is a necessary step in theformation of breast tumors or is, at the very least,advantageous. But what are the implications for un-derstanding the mechanisms by which E2 controlsmammary epithelial cell proliferation? Do the ERαcontaining cells become responsive to the growth fac-tors that they produce such that E2 acts via an auto-crine mechanism? Or does the ERα become coupledto the machinery controlling cell cycle progression ina much more fundamental manner? Answering thesequestions could greatly increase our understanding ofthe events leading to cancer formation and lead to thedevelopment of new preventive strategies.
Cyclins and the Mammary Epithelium
Although cultured breast cancer cells have beenused extensively for studying the effects of E2 on cellcycle progression and the mechanisms that control it,surprisingly little is known about the process in thenormal mammary epithelium, especially that of the

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
10 Anderson and Clarke
human. One of the reasons for this lack of knowledgeis the paucity of suitable experimental models thatcan be manipulated in the same way as cancer cells inlong-term culture. Expression of ERα and PR and,thus, steroid responsiveness is lost once mammaryepithelial cells are isolated and placed into mono-layer culture. Several immortalized human mammaryepithelial cell lines have been generated but, to date,none of them has retained estrogen responsiveness(61). Thus, most of what is known about the roles ofcyclins, CDKS and CDKIs in the mammary gland hascome from animal models in which the relevant geneshave been deleted or overexpressed. These showthat deletion of the cyclin D1 gene seriously impairslobulo-alveolar development of the mammary glandin early pregnancy, which prevents lactation and con-fers resistance to mammary tumor induction by some(c-neu and v-Ha-ras) but not all oncogenes (62,63).Conversely, overexpression of cyclin D1 increasesproliferation, promotes precocious lobulo-alveolardevelopment and induces formation of mammaryadenocarcinomas (64). Taken together, the dataderived from animal models indicate that cyclin D1has an important role in rodent mammary gland de-velopment and tumorigenesis. What about the humanbreast epithelium? A number of studies show overex-pression of cyclin D1 protein in approximately 50%of human breast tumors (65). Moreover, increasedexpression is detectable in premalignant proliferativelesions in which the proportion of cyclin D1-positivecells is correlated with the degree of atypia, implyingthat the cyclin might be important in the developmentof some human tumors (66). However, in normalhuman mammary epithelium taken from adultnonpregnant, nonlactating women, only 0.3% of cellsstain positively for cyclin D1 (67). Contrary to expec-tation, none of the cyclin D1 positive cells coexpressthe Ki67 proliferation-associated antigen, but theyare more likely to express the ERα. Even in tumorswhere the protein is overexpressed, colocalization ofcyclin D1 and the Ki67 antigen is a very rare event,although the strong association between cyclin D1and ER expression is maintained (67).
Given the low level of cyclin D1 expression andits lack of association with proliferative indices, itwould seem that this cyclin might not have an im-portant role in regulating proliferation in the normalhuman breast. However, studies on expression of theother D-type cyclins and their relationship to steroidreceptor expression and proliferation have yet to beperformed; those cyclins may play a greater role inregulating cell cycle progression in the normal human
mammary epithelium. Alternatively, it is possible thatcyclin D1 expression has not been studied at the ap-propriate developmental stage. The studies on ani-mal models suggest that cyclin D1 action is requiredfor lobulo-alveolar development in early pregnancy(62,64). Most of the samples used to examine cyclinD1 expression in the normal mammary epitheliumwere taken from adult nonpregnant women; perhapsan association between the protein and proliferationhas been missed.
The earlier question of whether direct couplingof the ERα to the machinery controlling cell cycle pro-gression occurs during tumorigenesis is still unsettled.While the studies on breast cancer cell lines do not ruleout completely the possibility that these cells have be-come capable of responding to the growth factors thatthey produce, a direct link between ERα and the cellcycle machinery is suggested. The key question is howis this achieved? It would appear that simple overex-pression of the ERα in receptor negative breast can-cer cell lines is not sufficient either to induce cyclin D1expression or to confer estrogen responsiveness andproliferation (68,69). Perhaps clues may be gained bydetermining what prevents proliferation of the ER-positive cells in the normal mammary epithelium. Onepromising candidate is transforming growth factorbeta (TGFβ), the active form of which has been shownby Barcellos-Hoff and her colleagues to co-localizewith ERα in mouse mammary epithelial cells (70).Moreover, the proportion of ERα-positive prolifer-ating mammary epithelial cells is increased in mice inwhich the tgfβ gene has been deleted heterozygously,which reduces TGFβ protein levels by 90%. Clearlywe need to find out whether TGFβ really does pre-vent proliferation of the ER-positive breast epithelialcells together with the mechanisms by which it acts.
CONCLUSIONS
The ovarian steroids E2 and P are major mito-gens for the normal mammary epithelium, but it isbecoming clear that they act indirectly via secretionof paracrine factors to stimulate cell cycle progressionand, hence, proliferation. This mechanism may be oneway of attenuating the sensitivity of the mammary ep-ithelium to the effects of the ovarian steroids and ofensuring that significant proliferative activity occursonly when needed, i.e. during puberty and pregnancy.
Increased ERα expression and loss of the in-verse relationship between steroid receptor expres-sion and proliferation occurs at the earliest stages of

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
Steroids and Normal Mammary Epithelium 11
human breast tumor development, implying that dys-regulation of ERα expression is an important step.Clearly, enhanced steroid receptor expression wouldsensitize the malignant epithelium to the effects ofE2 and P, but it remains to be determined whetherthese steroids continue to drive proliferation by theindirect mechanisms utilized by the normal epithe-lium or whether the receptors have become linked tothe machinery controlling cell cycle progression in amuch more fundamental way. The results of experi-ments on E2-responsive breast cancer cell lines canbe interpreted as providing evidence for both sug-gestions. Thus, it seems imperative to discover whatprevents ERα-positive cells in the normal epitheliumfrom proliferating. In turn, this discovery may lead toa greater understanding of the processes leading totumor formation and provide new targets for breastcancer prevention.
REFERENCES
1. R. L. Sutherland and E. A. Musgrove (2004). Cyclins and breastcancer. J. Mammary Gland Biol. Neoplasia.
2. B. A. Howard and B. A. Gusterson (2000). Human breast de-velopment. J. Mammary Gland Biol. Neoplasia 5:119–137.
3. B. A. Gusterson, P. Monaghan, R. Mahendran, J. Ellis, and M.J. O’Hare (1986). Identification of myoepithelial cells in humanand rat breasts by anti-common acute lymphoblastic leukemiaantigen antibody A12. J. Natl. Cancer Inst. 77:343–349.
4. J. Taylor-Papadimitriou, R. Millis, J. Burchell, R. Nash, L. Pang,and J. Gilbert (1986). Patterns of reaction of monoclonal anti-bodies HMFG-1 and -2 with benign breast tissues and breastcarcinomas. J. Exp. Pathol. 2:247–60.
5. J. Taylor-Papadimitriou, M. Stampfer, J. Bartek, A. Lewis, M.Boshell, E. B. Lane, et al. (1989). Keratin expression in humanmammary epithelial cells cultured from normal and malignanttissue: Relation to in vivo phenotypes and influence of medium.J. Cell Sci. 94(Pt. 3):403–413.
6. J. T. Emerman, J. Stingl, A. Petersen, E. J. Shpall, and C. J.Eaves (1996). Selective growth of freshly isolated human breastepithelial cells cultured at low concentrations in the presence orabsence of bone marrow cells. Breast Cancer Res. Treat. 41:147–159.
7. U. Latza, G. Niedobitek, R. Schwarting, H. Nekarda, and H.Stein (1990). Ber-EP4: New monoclonal antibody which distin-guishes epithelia from mesothelial. J. Clin. Pathol. 43:213–219.
8. K. Joshi, J. A. Smith, N. Perusinghe, and P. Monoghan (1986).Cell proliferation in the human mammary epithelium. Differ-ential contribution by epithelial and myoepithelial cells. Am. J.Pathol. 124:199–206.
9. O. W. Petersen, P. E. Hoyer, and B. van Deurs (1987). Frequencyand distribution of estrogen receptor-positive cells in normal,nonlactating human breast tissue. Cancer Res. 47:5748–5751.
10. S. R. Wellings, H. M. Jensen, and R. G. Marcum (1975). Anatlas of subgross pathology of the human breast with specialreference to possible precancerous lesions. J. Natl. Cancer Inst.55:231–273.
11. C. W. Daniel and G. B. Silberstein (1987). Postnatal develop-ment of the rodent mammary gland. In M. C. Neville and C. W.Daniel (eds.), The Mammary Gland. Development, Regulationand Function, Plenum, New York, pp. 3–36.
12. J. Russo and I. H. Russo, (1987). Development of the humanmammary gland. In M. C. Neville and C. W. Daniel (eds.),The Mammary Gland. Development, Regulation and Function,Plenum, New York, pp. 67–93.
13. M. M. Richert, K. L. Schwertfeger, J. W. Ryder, and S. M. An-derson (2000). An atlas of mouse mammary gland develop-ment. J. Mammary Gland Biol. Neoplasia 5:227–241.
14. H. McGregor, C. E. Land, K. Choi, S. Tokuoka, P. I. Liu, T.Wakabayashi, et al. (1977). Breast cancer incidence amongatomic bomb survivors, Hiroshima and Nagasaki, 1950–69. J.Natl. Cancer Inst. 59:799–811.
15. M. Clemons and P. Goss (2001). Estrogen and the risk ofbreast cancer. N. Engl. J. Med. 344:276–285.
16. R. C. Travis and T. J. Key (2003). Oestrogen exposure andbreast cancer risk. Breast Cancer Res. 5:239–247.
17. Z. Laron, R. Pauli, and A. Pertzelan (1989). Clinical evidenceon the role of estrogens in the development of the breasts.Proc. R. Soc. Edinb. B1 95:13–22.
18. B. Fisher, J. P. Costantino, D. L. Wickerham, C. K. Redmond,M. Kavanah, W. M. Cronin, et al. (1998). Tamoxifen forprevention of breast cancer: Report of the National SurgicalAdjuvant Breast and Bowel Project P-1 Study. J. Natl. CancerInst. 90:1371–1388.
19. W. P. Bocchinfuso and K. S. Korach (1997). Mammary glanddevelopment and tumorigenesis in estrogen receptor knockoutmice. J. Mammary Gland Biol. Neoplasia 2:323–334.
20. R. A. Lubet, V. E. Steele, R. DeCoster, C. Bowden, M. You,M. M. Juliana, et al. (1998). Chemopreventive effects of thearomatase inhibitor vorozole (R 83842) in the methylnitro-sourea-induced mammary cancer model. Carcinogenesis19:1345–1351.
21. S. Nandi, R. C. Guzman, and J. Yang (1995). Hormones andmammary carcinogenesis in mice, rats, and humans: A unifyinghypothesis. Proc. Natl. Acad. Sci. U.S.A. 92:3650–3657.
22. R. C. Humphreys, J. P. Lydon, B. W. O’Malley, and J. M. Rosen(1997). Use of PRKO mice to study the role of progesteronein mammary gland development. J. Mammary Gland Biol.Neoplasia 2:343–354.
23. V. Beral (2003). Breast cancer and hormone-replacementtherapy in the Million Women Study. Lancet 362:419–427.
24. R. K. Ross, A. Paganini-Hill, P. C. Wan, and M. C. Pike (2000).Effect of hormone replacement therapy on breast cancer risk:Estrogen versus estrogen plus progestin. J. Natl. Cancer Inst.92:328–332.
25. C. Schairer, J. Lubin, R. Troisi, S. Sturgeon, L. Brinton,and R. Hoover (2000). Menopausal estrogen and estrogen-progestin replacement therapy and breast cancer risk. JAMA283:485–491.
26. E. Enmark, M. Pelto-Huikko, K. Grandien, S. Lagercrantz, J.Lagercrantz, G. Fried, et al. (1997). Human estrogen receptorbeta-gene structure, chromosomal localization, and expressionpattern. J. Clin. Endocrinol. Metab. 82:4258–4265.
27. V. Kumar, S. Green, G. Stack, M. Berry, J. R. Jin, and P.Chambon (1987). Functional domains of the human estrogenreceptor. Cell 51:941–951.
28. J. M. Hall and D. P. McDonnell (1999). The estrogen receptorbeta-isoform (ERbeta) of the human estrogen receptor mod-ulates ERalpha transcriptional activity and is a key regulator

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
12 Anderson and Clarke
of the cellular response to estrogens and antiestrogens.Endocrinology 140:5566–5578.
29. C. L. Clarke and R. L. Sutherland (1990). Progestin reg-ulation of cellular proliferation. Endocr. Rev. 11:266–301.
30. E. Vegeto, M. M. Shahbaz, D. X. Wen, M. E. Goldman, B. W.O’Malley, and D. P. McDonnell (1993). Human progesteronereceptor A form is a cell- and promoter-specific repressor ofhuman progesterone receptor B function. Mol. Endocrinol.7:1244–1255.
31. J. K. Richer, B. M. Jacobsen, N. G. Manning, M. G. Abel, D. M.Wolf, and K. B. Horwitz (2002). Differential gene regulationby the two progesterone receptor isoforms in human breastcancer cells. J. Biol. Chem. 277:5209–5218.
32. B. Mulac-Jericevic, J. P. Lydon, F. J. DeMayo, and O. M.Conneely (2003). Defective mammary gland morphogenesisin mice lacking the progesterone receptor B isoform. Proc.Natl. Acad. Sci. U.S.A. 100:9744–9749.
33. S. Ali and R. C. Coombes (2002). Endocrine-responsive breastcancer and strategies for combating resistance. Nat. Rev.Cancer 2:101–112.
34. D. P. McDonnell and J. D. Norris (2002). Connections and regu-lation of the human estrogen receptor. Science 296:1642–1644.
35. K. Vermeulen, D. R. Van Bockstaele, and Z. N. Berneman(2003). The cell cycle: A review of regulation, deregulationand therapeutic targets in cancer. Cell Prolif. 36:131–149.
36. T. Evans, E. T. Rosenthal, J. Youngblom, D. Distel, and T. C.Hunt (1983). Cyclin: A protein specified by maternal mRNAin sea urchin eggs that is destroyed at each cleavage division.Cell 33:389–396.
37. J. C. Pines (1991). Cyclins: Wheels within wheels. Cell GrowthDiffer. 2:305–310.
38. C. J. Sherr (1994). G1 phase progression: Cycling on cue. Cell79:551–555.
39. M. Ohtsubo, A. M. Theodoras, J. Schumacher, J. M. Roberts,and M. Pagano (1995). Human cyclin E, a nuclear protein es-sential for the G1-to-S phase transition. Mol. Cell Biol. 15:2612–2624.
40. C. J. Sherr and J. M. Roberts (1999). CDK inhibitors: Positiveand negative regulators of G1-phase progression. Genes Dev.13:1501–1512.
41. S. F. Doisneau-Sixou, C. M. Sergio, J. S. Carroll, R. Hui, E.A. Musgrove, and R. L. Sutherland (2003). Estrogen andantiestrogen regulation of cell cycle progression in breastcancer cells. Endocr Relat Cancer 10:179–186.
42. R. B. Clarke, A. Howell, C. S. Potten, and E. Anderson(1997). Dissociation between steroid receptor expression andcell proliferation in the human breast. Cancer Res. 57:4987–4991.
43. G. Shyamala, Y. C. Chou, S. G. Louie, R. C. Guzman, G. H.Smith, and S. Nandi (2002). Cellular expression of estrogenand progesterone receptors in mammary glands: Regulationby hormones, development and aging. J. Steroid Biochem.Mol. Biol. 80:137–148.
44. V. Speirs, G. P. Skliris, S. E. Burdall, and P. J. Carder (2002).Distinct expression patterns of ER alpha and ER beta innormal human mammary gland. J. Clin. Pathol. 55:371–374.
45. J. F. Couse and K. S. Korach (1999). Estrogen receptor nullmice: What have we learned and where will they lead us?Endocr. Rev. 20:358–417.
46. P. A. Mote, S. Bartow, N. Tran, and C. L. Clarke (2002). Lossof co-ordinate expression of progesterone receptors A and B
is an early event in breast carcinogenesis. Breast Cancer Res.Treat. 72:163–172.
47. J. Russo, X. Ao, C. Grill, and I. H. Russo (1999). Patternof distribution of cells positive for estrogen receptor alphaand progesterone receptor in relation to proliferating cellsin the mammary gland. Breast Cancer Res. Treat. 53:217–227.
48. G. R. Cunha, P. Young, Y. K. Hom, P. S. Cooke, J. A.Taylor, and D. B. Lubahn (1997). Elucidation of a role forstromal steroid hormone receptors in mammary gland growthand development using tissue recombinants. J. MammaryGland Biol. Neoplasia 2:393–402.
49. S. O. Mueller, J. A. Clark, P. H. Myers, and K. S. Korach(2002). Mammary gland development in adult mice requiresepithelial and stromal estrogen receptor alpha. Endocrinology143:2357–2365.
50. S. A. Bartow (1998). Use of the autopsy to study ontogeny andexpression of the estrogen receptor gene in human breast. J.Mammary Gland Biol. Neoplasia 3:37–48.
51. C. Brisken, S. Park, T. Vass, J. P. Lydon, B. W. O’Malley, andR. A. Weinberg (1998). A paracrine role for the epithelialprogesterone receptor in mammary gland development. Proc.Natl. Acad. Sci. U.S.A. 95:5076–5081.
52. C. Brisken, A. Heineman, T. Chavarria, B. Elenbaas, J. Tan, S.K. Dey, et al. (2000). Essential function of Wnt-4 in mammarygland development downstream of progesterone signaling.Genes Dev. 14:650–654.
53. K. C. Chan, W. F. Knox, J. M. Gee, J. Morris, R. I. Nicholson,C. S. Potten, et al. (2002). Effect of epidermal growth factorreceptor tyrosine kinase inhibition on epithelial proliferationin normal and premalignant breast. Cancer Res. 62:122–128.
54. T. J. Martin and M. T. Gillespie (2001). Receptor activatorof nuclear factor kappa B ligand (RANKL): Another linkbetween breast and bone. Trends. Endocrinol. Metab. 12:2–4.
55. E. A. Kritikou, A. Sharkey, K. Abell, P. J. Came, E. Anderson,R. W. Clarkson, et al. (2003). A dual, non-redundant, rolefor LIF as a regulator of development and STAT3-mediatedcell death in mammary gland. Development 130:3459–3468.
56. R. C. Hovey, J. Harris, D. L. Hadsell, A. V. Lee, C. J. Ormandy,and B. K. Vonderhaar (2003). Local insulin-like growth factor-II mediates prolactin-induced mammary gland development.Mol. Endocrinol. 17:460–471.
57. C. Palmieri, D. Roberts-Clark, A. Assadi-Sabet, R. C. Coope,M. O’Hare, A. Sunters, et al. (2003). Fibroblast growth factor 7,secreted by breast fibroblasts, is an interleukin-1beta-inducedparacrine growth factor for human breast cells. J. Endocrinol.177:65–81.
58. D. C. Allred, S. K. Mohsin, and S. A. Fuqua (2001). Histolog-ical and biological evolution of human premalignant breastdisease. Endocr. Relat. Cancer 8:47–61.
59. B. S. Shoker, C. Jarvis, D. R. Sibson, C. Walker, and J. P. Sloane(1999). Oestrogen receptor expression in the normal andpre-cancerous breast. J. Pathol. 188:237–244.
60. B. S. Shoker, C. Jarvis, R. B. Clarke, E. Anderson, J. Hewlett, M.P. Davies, et al. (1999). Estrogen receptor-positive proliferatingcells in the normal and precancerous breast. Am. J. Pathol.155:1811–1815.
61. E. Anderson, R. B. Clarke, and A. Howell (1998). Estro-gen responsiveness and control of normal human breastproliferation. J. Mammary Gland Biol. Neoplasia 3:23–35.

P1: GAD
Journal of Mammary Gland Biology and Neoplasia (JMGBN) pp1152-jmgbn-483560 March 30, 2004 21:41 Style file version June 22, 2002
Steroids and Normal Mammary Epithelium 13
62. V. Fantl, G. Stamp, A. Andrews, I. Rosewell, and C. Dickson(1995). Mice lacking cyclin D1 are small and show defects ineye and mammary gland development. Genes Dev. 9:2364–2372.
63. Q. Yu, Y. Geng, and P. Sicinski (2001). Specific protec-tion against breast cancers by cyclin D1 ablation. Nature411:1017–1021.
64. T. C. Wang, R. D. Cardiff, L. Zukerberg, E. Lees, A. Arnold, andE. V. Schmidt (1994). Mammary hyperplasia and carcinoma inMMTV-cyclin D1 transgenic mice. Nature 369:669–671.
65. D. M. Barnes and C. E. Gillett (1998). Cyclin D1 in breastcancer. Breast Cancer Res. Treat 52:1–15.
66. X. L. Zhu , W. Hartwick, T. Rohan, and R. Kandel (1998).Cyclin D1 gene amplification and protein expression in benignbreast disease and breast carcinoma. Mod. Pathol. 11:1082–1088.
67. B. S. Shoker, C. Jarvis, M. P. Davies, M. Iqbal, D. R. Sibson, andJ. P. Sloane (2001). Immunodetectable cyclin D(1)is associatedwith oestrogen receptor but not Ki67 in normal, cancerousand precancerous breast lesions. Br. J. Cancer 84:1064–1069.
68. M. D. Planas-Silva, J. L. Donaher, and R. A. Weinberg (1999).Functional activity of ectopically expressed estrogen receptoris not sufficient for estrogen-mediated cyclin D1 expression.Cancer Res. 59:4788–4792.
69. D. A. Zajchowski, R. Sager, and L. Webster (1993). Estrogeninhibits the growth of estrogen receptor-negative, but notestrogen receptor-positive, human mammary epithelial cellsexpressing a recombinant estrogen receptor. Cancer Res.53:5004–5011.
70. M. H. Barcellos-Hoff (2003). Transforming growth factorbeta’s role in mammary gland development and carcinogene-sis. Breast Cancer Res. 5(Suppl. 1):33.