Embed Size (px)
Citation preview

State of the art treatment
of hypertension:
established and
new drugs
Prof. M. BurnierService of Nephrology and HypertensionLausanne, Switzerland

ACE inhibitorsAT1-receptor blockers Calcium antagonists
Diureticsß-blockers
Adapted from the 2009 Reappraisal of ESH/ESC Hypertension Guidelines
First-line therapies
First line therapies in hypertension

Law et al, BMJ 2003
Standard
dose
Twice
standard
dose
Half
standard
dose
-blockers
ACE inhibitors
Thiazides
Calcium antagonists
AT1-receptor blockers
0
-5
-10
-15
Ch
an
ge
s in
SB
P, m
mH
g
Placebo-corrected changes in SBP

Law et al, BMJ 2003
Pe
rce
nta
ge
of p
atie
nts
with
AE
Standard
dose
Twice
standard
dose
Half
standard
dose
-blockers
ACE inhibitors
Thiazides
Calcium antagonists
AT1-receptor blockers
20
15
10
5
0
-5
N° of trials :
59
96
62
9644

Isolated systolic hypertension
Hypertension in blacks
Angina pectoris
Post-myocardial infarction
Left ventricular hypertrophy
Atrial fibrillation
Heart failure
Carotid/coronary atherosclerosis
Metabolic syndrome
Non diabetic nephropathy
Diabetic nephropathy
Proteinuria/microalbuminuria
Blockers of the RAS
Dihydropyridines
Thiazides
Adapted from ESH/ESC Hypertension Guidelines

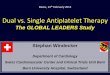
Baseline Control Rates
37.2 37.9
ACCOMPLISH: Exceptional Control Rates
with Initial Combination Therapy
ACEI / HCTZN=5733
Co
ntr
ol r
ate
(%
)
CCB / ACEIN=5713
10
20
30
40
50
60
70
80
90
78.581.7
P<0.001 at 30 months follow-up
Control defined as <140/90 mmHg

One topic of debate: ACEI or ARB ?
Arguments regarding:
Impact on morbidity and mortality
Tolerability profile and risk of SAE

ONTARGETRamipril vs Telmisartan
Time to Primary Outcome
Years of Follow-up
Cu
mu
lative
Ha
za
rd R
ate
s
0.0
0.0
50
.10
0.1
50
.20
0.2
5
0 1 2 3 4
Telmisartan
Ramipril
# at Risk Yr 1 Yr 2 Yr 3 Yr 4 Yr 4.5
T 8542 8177 7778 7420 7051 4575R 8576 8214 7832 7472 7093 4562
N Engl JMed 2008;358:1547-59

ONTARGET Non-Inferiority
Comparison
0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3 1.4
RR (95% CI)
Note that the outcomes are presented as point estimates with confidence intervals. The solid line
is the 95% CI representing 1.96 SD for each outcome
CV Death
MI
Stroke
CHF Hosp
All Death
Telmisartan better Ramipril better
ONTARGET
N Engl JMed 2008;358:1547-59
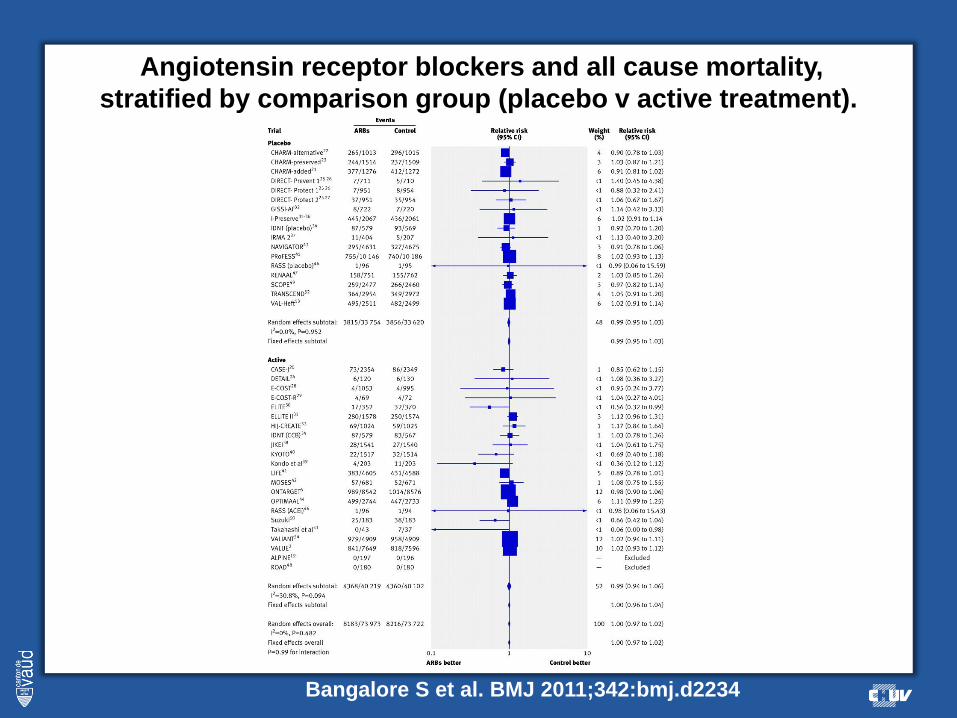
Angiotensin receptor blockers and all cause mortality,
stratified by comparison group (placebo v active treatment).
Bangalore S et al. BMJ 2011;342:bmj.d2234

Angiotensin receptor blockers and myocardial infarction,
stratified by comparison group (placebo v active treatment).
Bangalore S et al. BMJ 2011;342:bmj.d2234
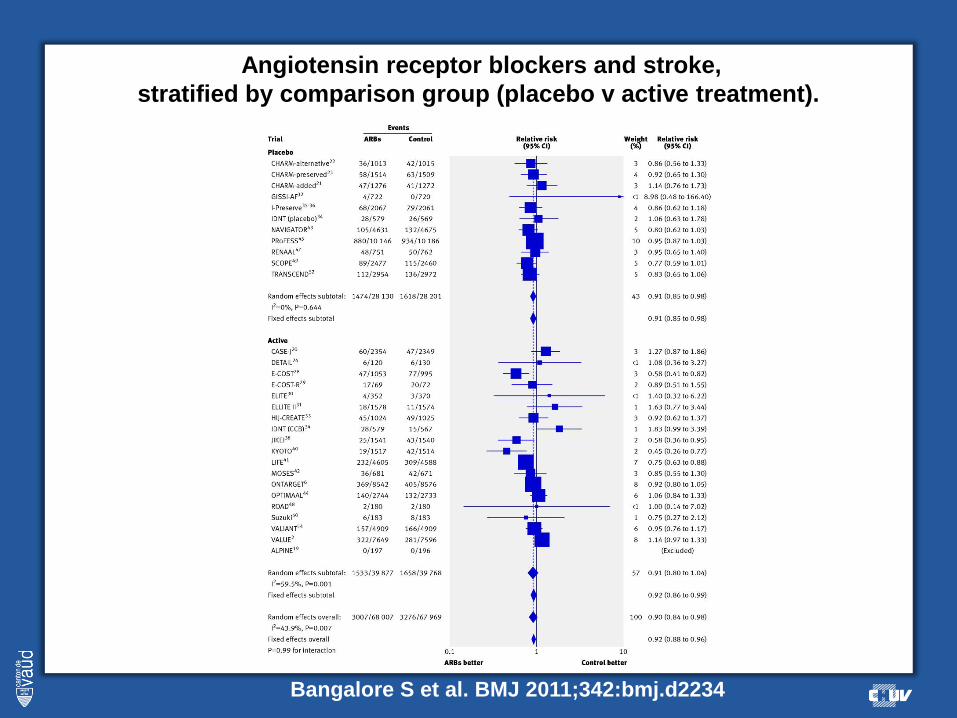
Angiotensin receptor blockers and stroke,
stratified by comparison group (placebo v active treatment).
Bangalore S et al. BMJ 2011;342:bmj.d2234

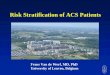
ONTARGETReasons for Permanently
Stopping Study Medications
Ram
N=8576
Tel
N=8542
Tel vs. Ram
RR P
Hypotension 149 224 1.51 0.0001
Syncope 15 18 1.20 0.593
Cough 359 93 0.26 <0.0001
Diarrhea 12 19 1.59 0.20
Angioedema 25 10 0.40 0.0115
Renal
Impairment
59 68 1.16 0.41
Any
Discontinuation
2098 1962 0.94 0.02
N Engl JMed 2008;358:1547-59
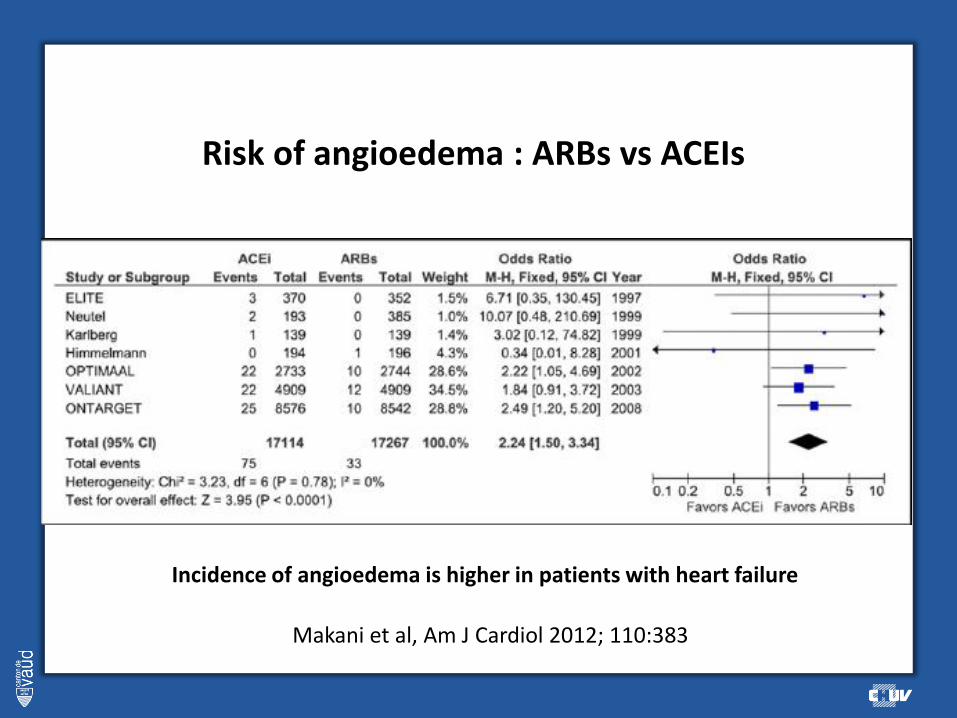
Risk of angioedema : ARBs vs ACEIs
Makani et al, Am J Cardiol 2012; 110:383
Incidence of angioedema is higher in patients with heart failure

Losartan
Eprosartan
Telmisartan
Irbesartan
Candesartan
Valsartan
Olmesartan
0 2 6 10 124 8
Standardised discontinuation rate(100 patients/month)
ARBs
Captopril
Moexipril
Spirapril
Fosinopril
Quinapril
Benazepril
Trandolapril
Delapril
Cilazapril
Lisinopril
Enalapril
Perindopril
Zofenopril
Ramipril
0 10 20 30 40
Standardised discontinuation rate(100 patients/month)
ACEIs
The importance of tolerability is reflected by within-class differences in discontinuation rates
Mancia et al. J Hypertens 2011;29:1012-1018.
Another question: which calcium antagonist ?

ACCOMPLISH: RAS-blocker/CCB combined
therapy offers benefits in higher-risk patients
20% lower
The primary cardiovascular composite end point was significantly lower with an ACEI/CCB than an ACEI/diuretic combination
Jamerson et al. N Engl J Med 2008;359:2417-28
16
14
12
10
8
6
4
2
0
Pati
ents
wit
h p
rim
ary
even
ts (
%)
No. at risk:
Benazepril / AML
Benazepril / HCTZ
Benazepril plus hydrocholorthiazide
Benazepril plus amlodipine
0 6 12 18 24 30 36 42Months
5512 5317 5141 4959 4739 2826 1447
5483 5274 5082 4892 4655 2749 1390

Incidence of adverse responses to different
classes of drugs as reported by physicians
0
5
10
15
20
25
Diur ß-block CCB ACEi Alpha-
block
other
E.Ambrosioni et al, J Hypertens ;18 , 2000
%
**

Adherence to cardiovascular drugs in primary prevention
Naderi et al, The American Journal of Medicine (2012) 125, 882-887

Peripheral edema:

Adverse events in the VALUE trial
Valsartan
(n=7622)
Amlodipine
(n=7576)P
Pre-specified adverse events
Peripheral edema 1135 (14.9%) 2492 (32.9%) <0.0001
Dizziness 1257 (16.5%) 1083 (14.3%) <0.0001
Headache 1120 (14.7%) 947 (12.5%) <0.0001
Fatigue 739 (9.7%) 674 (8.9%) 0.0750
Additional common adverse events
Diarrhea* 670 (8.8%) 515 (6.8%) <0.0001
Edema other* 243 (3.2%) 462 (6.1%) <0.0001
Hypokaliemia* 266 (3.5%) 469 (6.2%) <0.0001
*With an incidence >3% and a difference between treatment groups >1%
Julius et al. Lancet. 2004;363:2022-2031.

Adverse events in the ASCOT trial
Adverse event*
Amlodipine
perindopril
n (%)
Atenolol
thiazide
n (%)
p-value
Bradycardia 34 (0.4) 536 (6) <0.0001
Chest pain 740 (8) 849 (9) 0.0040
Cough 1859 (19) 782 (8) <0.0001
Diarrhoea 377 (4) 548 (6) <0.0001
Dizziness 1183 (12) 1555 (16) <0.0001
Dyspnoea 599 (6) 987 (10) <0.0001
Eczema 493 (5) 383 (4) 0.0002
Erectile
dysfunction556 (6) 707 (7) <0.0001
Fatigue 782 (8) 1556 (16) <0.0001
Joint swelling 1371 (14) 308 (3) <0.0001
Lethargy 202 (2) 525 (6) <0.0001
Oedema peripheral 2188 (23) 588 (6) <0.0001
Peripheral coldness 81 (1) 579 (6) <0.0001
Vertigo 642 (7) 745 (8) 0.0039
37 % of edema

PREVALENCE OF DRUG-SPECIFIC AE’s IN THE
LERCANIDIPINE CHALLENGE STUDY.
96
52
87
0
20
40
60
80
100
CCB Lercanidipine CCB
yesno
% p
atie
nts
wit
h
S.E
.s
P<0.001
P<0.001
Ankle edema
Borghi C et al, Blood Pressure, 2003

% o
f pa
tient
s
02468
101214161820
Baseline 1 month 2 months 3 months 6 months End of
study
Lercanidipine
Amlodipine
Lacidipine
% OF PTS WITH ANKLE EDEMA OVER TIME
COHORT Study, Am J Hypertens, 2002
P<0.001

Initiation
(n=683)
Add-on
(n=844)
Substitution
(n=672)
Premature treatment
interruption due to
adverse events4.4 7.8 8.8
Ankle edema
Headache
Flush
Others
0.6
0.6
0.4
2.8
1.9
1.1
1.3
3.8
3.0
1.1
0.6
4.3
Impact of lercanidipine on peripheral edema in 2199 patients
followed by GPs in Switzerland
Burnier and Gasser, 2007

Last question: which diuretic ?
Hydrochlorothiazide
Chlorthalidone
Indapamide

Dose-response relationships for thiazides vs BP (A and B)
(C) serum potassium; and (D) serum urate.
Peterzan M A et al. Hypertension 2012;59:1104-1109

Risk of cardiovascular events in patients receiving HCTZ or chlorthalidone
according to the changes in systolic BP
Roush G C et al. Hypertension 2012;59:1110-1117
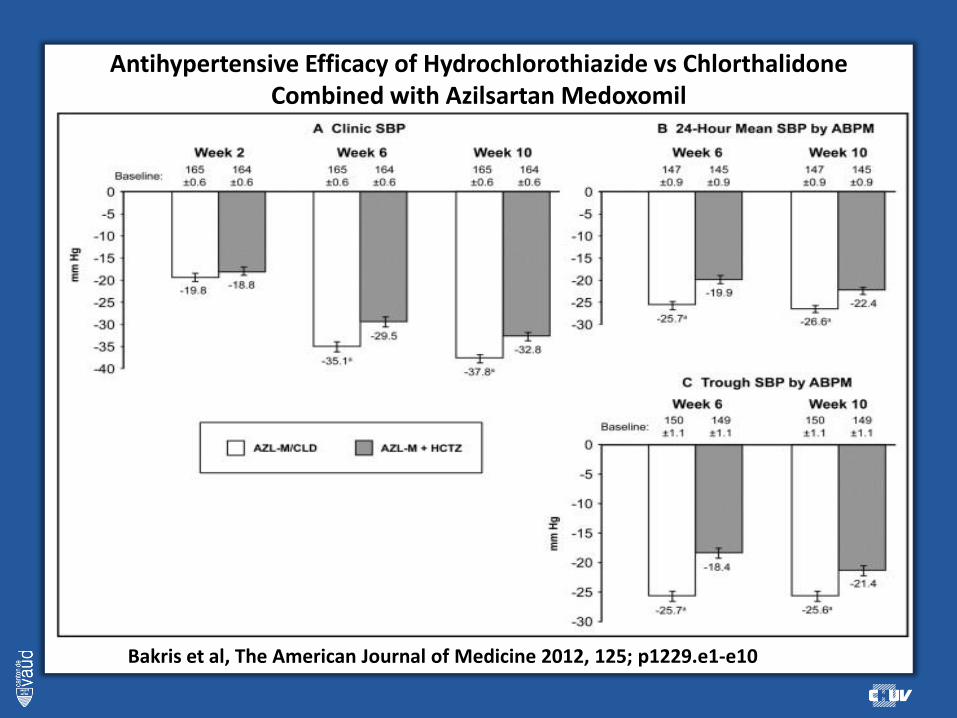
Antihypertensive Efficacy of Hydrochlorothiazide vs ChlorthalidoneCombined with Azilsartan Medoxomil
Bakris et al, The American Journal of Medicine 2012, 125; p1229.e1-e10

Cushman W C et al. Hypertension 2012;60:310-318
Azilsartan + CLD vs olmesartan + HCTZ

Change in systolic blood pressure by ABPM at week 12.
Cushman W C et al. Hypertension 2012;60:310-318

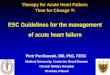
Over one year, compliance and persistence with
anti-hypertensive therapy typically falls to <50%
Vrijens et al. BMJ 2008;336:1114-7.
• Study of hypertensive patients in clinical studies
• 4783 patients in 21 Phase IV trials
• Evaluated by medication event monitoring system
Fall in persistencebecause of discontinuation of treatment
Fall in adherencebecause of
poor execution of dosing regimen
100
90
80
70
60
50
00 50 100 150 200 250 300 350
Time (days)
3108 980 828 618 474 400 331No of patientsremaining in study
Pe
rce
nta
ge o
f p
atie
nts
PersistenceAdherence/compliancePerfect adherence

Adherence to cardiovascular drugs
Naderi et al, The American Journal of Medicine (2012) 125, 882-887