Embed Size (px)
Citation preview
Sola et al.
1
Emergence and Dissemination of a Community-Associated Methicillin resistant
Staphylococcus aureus clone - Panton-Valentin Leucocidin positive sharing the ST5 lineage
with the most prevalent nosocomial clone in the same region of Argentina
Sola Claudia1, Saka Hector A.
1, Cordoba MRSA Collaborative Study Group
2, Vindel Ana
3 5
and Bocco José Luis1*.
1Departamento de Bioquímica Clínica, Facultad de Ciencias Químicas, Universidad
Nacional de Cordoba. Ciudad Universitaria, Pabellon Argentina, 5000 Cordoba,
ARGENTINA. 10
2 Members of the Cordoba MRSA Collaborative Study Group.
Monterisi, Aida and Rocchi, Marta (Hospital Nacional de Clínicas); Perlo-Morales, Olga and
Aiassa, María S, (Hospital Córdoba); Vilaro, Mario and Bongiovanni, María E. (Hospital Privado
de Córdoba); Mangiaterra, Sandra (Hospital Italiano de Córdoba); Diaz, Elda and Lamberghini
Ricardo (Hospital Militar de Córdoba); Littvik Ana, Lopez Teresa (Hospital Rawson); Yudowsky 15
Silvia (Hospital Infantil); Carvajal Lydia and Culasso Catalina (Hospital de Niños); Wolff Lidia
and Vercelli B, (Clínica Privada Velez Sarsfield); D’Andrea Elena M., Lopez Adriana (Hospital
de Urgencias); Pino Gladys, Muñoz Veronica (Hospital San Roque); Bottiglieri Marina (Clínica
Reina Fabiola); Gonzalez Patricia and Lamberghini Ricardo (Hospital Español Medical Plaza);
Cortes Paulo (Hospital Pediátrico del Niño Jesús); Gribaudo Germán (Sanatorio Nosti–Rafaela-20
Santa Fe
3 Laboratorio de Infecciones Nosocomiales, Instituto de Salud Carlos III, Centro Nacional
de Microbiología, 28220 Majadahonda, Madrid, Spain
Running title: Dissemination of a PVL-positive ST5-IVa CA-MRSA clone
ACCEPTED
Copyright © 2008, American Society for Microbiology and/or the Listed Authors/Institutions. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.01949-07 JCM Accepts, published online ahead of print on 5 March 2008
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
2
Keywords: CA-MRSA, HA-MRSA, Cordoba-Argentina, ST5; Panton-Valentine Leukocidin.
*Corresponding author:
Bocco José Luis. 1 Departamento de Bioquímica Clínica, Facultad de Ciencias Químicas, 5
Universidad Nacional de Córdoba. CIBICI – CONICET. Haya de la Torre y M. Allende. 5000
Córdoba – ARGENTINA. Tel.: 54 351 433 4164. Fax: 54 351 433 3048
E-mail: [email protected]
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
3
ABSTRACT:
Epidemiological surveillance for Community-associated Methicillin resistant Staphylococcus
aureus-(CA-MRSA) revealed 33% and 13% of prevalence in paediatric and adults patients
respectively in Cordoba-Argentina-2005. This study describe for the first time the emergence and
dissemination of ST5 lineage as the most prevalent (89%) clone (pulsotypeI-ST5-SCCmecIVa-5
t311) harbouring Panton-Valentine leukocidin and enterotoxin A genes.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
4
Methicillin-resistant Staphylococcus aureus (MRSA) is a traditionally established nosocomial
pathogen. Furthermore, virulent and non-multiresistant community–associated MRSA (CA-
MRSA) strains have been reported in many countries since 1993.
CA-MRSA strains are commonly associated with skin and soft tissue (SST) infections though
invasive infections as osteomyelitis and necrotizing pneumonia have been described (9). These 5
strains frequently harbor staphylococcal cassette chromosome (SCCmec) type IV or V, and the
Panton-Valentine leukocidin (PVL) genes along with a particular repertoire of virulence genes
(4). Moreover, the simultaneous assessment of the genetic background, virulence gene profiles
and accessory gene regulator locus (agr), increases the discriminatory power of genetic
investigations into S. aureus pathogenesis (4;6) 10
In Argentina, MRSA is one of the most important pathogens causing healthcare associated
infections (HA-MRSA) showing 48% of prevalence in 2005 (15), whereas no data about CA-
MRSA prevalence are still available. The Cordobes/Chilean clone was reported as the most
prevalent among HA-MRSA isolates (53% in 2001) in Córdoba, the second most populated city
of Argentina (18). Additionally, one sporadic isolate susceptible to Gentamicin, non-15
multiresistant and characterized as PFGE type I-ST5-IVa were recovered in 2001 (18). Other
four isolates with I1 pulsotype were also detected in other study carried out in 2004 (CS and JLB,
unpublished).
In this work, the prevalence of CA-MRSA infections was investigated during a 2005
surveillance period in Córdoba. The molecular genetic characteristics and virulence gene content 20
of CA-MRSA strains were analyzed and compared to those of HA-MRSA isolated during the
same period of time, including the patient’s clinical features.
This prospective study of laboratory-based surveillance for the MRSA infections in 14
hospitals (H1-H14; 1878 beds) of Cordoba, Argentina, was conducted in two steps; i) single
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
5
patient HA and CA-MRSA isolates were recollected during April to June 2005. ii) single patient
CA-MRSA isolates were recovered during January to June 2006. Three tertiary care community
hospitals (H11-H13) and a primary care pediatric hospital (H14-49 beds) were included in this
study in addition those previously reported (18). Since none HA-MRSA was recovered in H14
from 2002 and it had a high prevalence of CA-MRSA in 2005, all S aureus strains, MRSA and 5
MSSA, were analyzed to determine the genetic relationship between them during 2006 period.
All isolates were identified by standard microbiologic procedures and were characterized by
antibiotic susceptibility (2) and pulsed-field gel electrophoresis (PFGE) (18). The mecA and pvl
genes were determined in all strains by PCR (19). Representative isolates of CA-MRSA (all
PFGE subtypes) and HA-MRSA (more prevalent subtypes) were characterized by MLST, 10
SCCmec and spaA typing, as previously described (18). The sequences obtained by spaA typing
were compared to those held on the SpaServer (http://spaserver.ridom.de) (5). Representative
isolates of main major pulsotypes of MSSA recovered in H14 were also characterized by MLST
and spaA typing. The agr group (1 to 4) (14) and virulence genes content (4;7;14) were detected
by PCR (Table 2). 15
A total of 376 isolates of S. aureus were collected during the 2005 period. The proportions for
HA-MRSA and CA-MRSA infections were 57% (134 MRSA/235 HA-S. aureus) and 16 % (22
MRSA/141 CA-S. aureus), respectively. The prevalence of CA-MRSA differed significantly
between pediatrics and adults patients (33%, 7 CA-MRSA /21 CA-S. aureus vs 13%, 15 CA-
MRSA /120 CA-S. aureus -P=0.02). Twenty-five episodes of CA-MRSA infections were 20
detected during the 2006 period. In H14, 11 CA-MRSA and 10 CA-MSSA isolates were
recovered (52% of prevalence). These results revealed the emergence of CA-MRSA in the
community, moreover this is the first report of prevalence of CA-MRSA in Argentina.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
6
Different definitions to distinguish CA-MRSA and HA-MRSA as well as differences about
the settings and populations analyzed could explain how the prevalence rates of CA-MRSA
informed so far vary widely among different studies and countries. The high prevalence (31% in
2005 and 52% in 2006) observed in H14 could reflect the true prevalence of CA-MRSA in this
region due to patients attended in this hospital were pediatric outpatients affected by non-severe 5
infections. In fact, patients with mild S. aureus skin diseases are often treated empirically and
more frequently attended in primary or intermediate-care institutions (H14) than in tertiary-care
community hospitals (H11-H13). In conclusion, results from H14 during 2005-2006 strongly
suggest that the current prevalence of CA-MRSA in Argentina may be higher than it detected in
all hospitals in 2005, and thus call for closer systematic surveillance. 10
The CA-MRSA strains have been shown to be continent-specific for some ST types although
the results of a recent study suggest intercontinental exchanges of these PVL-positive clones and
detection of new ones since 2003. Among the latter ST5 was only described in sporadic isolates
of Europe and United States (1;10;11;16;20). Nevertheless, in this study, within all the CA-
MRSA isolates, a predominant (89%) [(91%-2005)-(88%-2006)] I major pulsotype was detected 15
(Table 2) belonging to the ST5 lineage. All isolates of this pulsotype were characterized as 2-agr
type and carried the IVa-SCCmec type, except one isolate (IVc). Most of them have spa type
311 (88%) and harbor pvl and sea genes (94%) (Table 2). Therefore, the emergence in 2001 (18)
and dissemination of the ST5 lineage as the most prevalent clone among CA-MRSA is described
for the first time in this study. Muller and co-workers reported ST5 lineage harboring pvl genes 20
but associated to I-SCCmec type-spa t002 instead of IVa-spa t311 (12). Acquisition of pvl genes
by this lineage is of extreme epidemiological importance for two relevant features: i) high
epidemic potential was demonstrated at hospital settings by the New York/Japan/ST5-II and
Pediatric/ST5-IV pandemic clones and ii) to its ability to acquire Vancomycin resistance (18).
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
7
In addition, two ST (ST917/CC8 and ST918 singleton), were described in this study for the
first time along with the ST100 (3 isolates) among CA-MRSA strains (Table 2).
The distribution of CA-MRSA and HA-MRSA respect to patient’s clinical features, age and
sex are shown in the Table 1. In agreement with several reports (13), the results of this work
showed that most CA-MRSA were from SST infections and occurred with higher frequency 5
among children and young adults (Table 1). Invasive and severe infections (3 cases) as sepsis
with pulmonary involvement and bone and joint infections were also detected. This support the
high virulence of the new CA-MRSA clone detected in Argentina. The presence of PVL appears
to be associated with increased severity (9) and the sea genes were linked to severe and invasive
S. aureus infections (3). Thus, the presence of both pvl and sea genes, as observed for the clone 10
described here, seems to be a genetic signature of highly toxic/superantigenic strains involved in
CA-MRSA infections.
Importantly, the CA-MRSA strain as cause of HA-MRSA has been reported in the world (11).
In our study, four patients from different hospitals with surgical site infections were considered
as CA-MRSA according to the molecular characterization. Hence, the systematic follow-up of 15
infections caused by CA-MRSA and HA-MRSA in this region is necessary to determine weather
this new virulent CA-MRSA clone could also emerge as cause of HA-MRSA infections. The
eventual spread of this CA-MRSA clone in hospitals and in the community could be a serious
public-health challenge in coming years.
On the other hand, among the HA-MRSA strains, the Cordobes/Chilean clone is still the most 20
prevalent (64%-2005) (18) since 1999 and it behaves at present like an endemic clone. Although
the total number of HA-S. aureus infections did not vary significantly (data not shown) a
significant increase in the prevalence of HA-MRSA infections was observed in 2005 (43% in
2001 vs 57% in 2005) (P< 0.0001). Thus, this clone gained this dominant behavior not only at
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
8
expenses of the other epidemic strains (e.g. the Brazilian clone) but also enhancing the burden of
HA-MRSA infections.
The ST30 and ST5 lineages were the most prevalent among invasive MSSA strains at
nosocomial and community settings in this region during 1999-2002 with capacity to acquire pvl
genes (19). In this study, most strains of MRSA and MSSA belonged to the same I pulsotype 5
and had similar molecular characteristics (Table 2 and Fig. 1A and 1B). Comparative analysis of
virulence genes content, genetic background among those local strains along with sequential
emergence of different genotypes of the I pulsotype (Fig. 1C), allow us to delineate the possible
evolutionary pathway within CC5 (Fig. 1D). Therefore, the new epidemic CA-MRSA clone
likely arose from insertion of SCCmec-IVa into a pvl and sea positive successful MSSA clone 10
(Fig 1B and 1D). The type diversity of the SCCmec elements (IVa, IVc, IVNv and I) identified
in ST5/ST100-CC5 indicates that their integration occurred independently in different time
periods. This observation argue in favor of the existence of a successful MSSA clone having a
genomic background (pulsotype M, ST5-t002) with capacity to acquire pvl genes, adapted to the
local ecological niche and more receptive to different types of SCCmec. These characteristics 15
could confer a selective advantage for its dissemination in this country. According to these
results, it is interesting to hypothesize that both CA-MRSA and HA-MRSA prevalent clones
could have evolved from the same MSSA successful ancestor (Figure 1D).
Our results reveal that PVL-producing MRSA strains must now be considered as a possible
cause of CA infections at the moment to choice the therapeutic option in this country. Most CA-20
MRSA strains were only resistant to β-lactam antibiotics, including susceptibility to Mupirocin
and Fusidic Acid (only 10% of resistance to clindamycin was detected).
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
9
In conclusion, the emergence of CA-MRSA in Cordoba, Argentina was due to the expansion,
for the first time, of a virulent clone belonging to ST5 lineage associated to SCCmec IVa
element, thus, differing from the ST30-IVc clone disseminated in Uruguay bordering country
since 2003.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
10
ACKNOWLEDGMENTS.
This work was supported by the National Council for Scientific Research and Technology of
Argentina (CONICET), Agencia Nacional de Promoción Científica y Tecnológica (ANPCyT –
PICT 05-13446 to JLB), Secretaría de Ciencia y Técnica–Universidad Nacional de Córdoba 5
(SECyT-UNC) and Agencia Córdoba Ciencia. CS is a fellow recipient of the SECyT-UNC. JLB
is a career investigator member of CONICET.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from

Sola et al.
11
REFERENCES
1. Bhattacharya, D., H. Carleton, C. J. Tsai, E. J. Baron, and F. Perdreau-Remington. 2007. Differences in
clinical and molecular characteristics of skin and soft tissue methicillin-resistant Staphylococcus aureus
isolates between two hospitals in Northern California. J Clin Microbiol 45:1798-803. 5
2. Clinical and Laboratory Standards Institute . 2005. Performance standards for antimicrobial susceptibility
testing. Fifteenth informational supplement. CLSI, Wayne, Pennsylvania. M100-S15.
3. Dauwalder, O., D. Thomas, T. Ferry, A. L. Debard, C. Badiou, F. Vandenesch, J. Etienne, G. Lina, and
G. Monneret. 2006. Comparative inflammatory properties of staphylococcal superantigenic enterotoxins
SEA and SEG: implications for septic shock. J Leukoc Biol 80:753-8. 10
4. Diep, B. A., H. A. Carleton, R. F. Chang, G. F. Sensabaugh, and F. Perdreau-Remington. 2006. Roles of
34 virulence genes in the evolution of hospital- and community-associated strains of methicillin-resistant
Staphylococcus aureus. J Infect Dis 193:1495-503.
5. Harmsen, D., H. Claus, W. Witte, J. Rothganger, H. Claus, D. Turnwald, and U. Vogel. 2003. Typing of
methicillin-resistant Staphylococcus aureus in a university hospital setting by using novel software for spa 15
repeat determination and database management. J Clin Microbiol 41:5442-8.
6. Holtfreter, S., D. Grumann, M. Schmudde, H. T. Nguyen, P. Eichler, B. Strommenger, K. Kopron, J.
Kolata, S. Giedrys-Kalemba, I. Steinmetz, W. Witte, and B. M. Broker. 2007. Clonal distribution of
superantigen genes in clinical S. aureus isolates. J Clin Microbiol .
7. Jarraud, S., C. Mougel, J. Thioulouse, G. Lina, H. Meugnier, F. Forey, X. Nesme, J. Etienne, and F. 20
Vandenesch. 2002. Relationships between Staphylococcus aureus genetic background, virulence factors, agr
groups (alleles), and human disease. Infect Immun 70:631-41.
8. Klevens, R. M., M. A. Morrison, S. K. Fridkin, A. Reingold, S. Petit, K. Gershman, S. Ray, L. H.
Harrison, R. Lynfield, G. Dumyati, J. M. Townes, A. S. Craig, G. Fosheim, L. K. McDougal, and F. C. Tenover. 2006. Community-associated methicillin-resistant Staphylococcus aureus and healthcare risk 25
factors. Emerg Infect Dis 12:1991-3.
Notes: CORPORATE NAME: Active Bacterial Core Surveillance of the Emerging Infections Program
Network.
9. Labandeira-Rey, M., F. Couzon, S. Boisset, E. L. Brown, M. Bes, Y. Benito, E. M. Barbu, V. Vazquez,
M. Hook, J. Etienne, F. Vandenesch, and M. G. Bowden. 2007. Staphylococcus aureus Panton-Valentine 30
leukocidin causes necrotizing pneumonia. Science 315:1130-3.
10. Ma, X. X., A. Galiana, W. Pedreira, M. Mowszowicz, I. Christophersen, S. Machiavello, L. Lope, S.
Benaderet, F. Buela, W. Vincentino, M. Albini, O. Bertaux, I. Constenla, H. Bagnulo, L. Llosa, T. Ito, and K. Hiramatsu. 2005. Community-acquired methicillin-resistant Staphylococcus aureus, Uruguay. Emerg
Infect Dis 11:973-6. 35
11. Monecke, S., B. Berger-Bachi, G. Coombs, A. Holmes, I. Kay, A. Kearns, H. J. Linde, F. O'Brien, P.
Slickers, and R. Ehricht. 2007. Comparative genomics and DNA array-based genotyping of pandemic
Staphylococcus aureus strains encoding Panton-Valentine leukocidin. Clin Microbiol Infect 13:236-49.
12. Muller-Premru, M., B. Strommenger, N. Alikadic, W. Witte, A. W. Friedrich, K. Seme, N. S. Kucina, D. Smrke, V. Spik, and M. Gubina. 2005. New strains of community-acquired methicillin-resistant 40
Staphylococcus aureus with Panton-Valentine leukocidin causing an outbreak of severe soft tissue infection in
a football team. Eur J Clin Microbiol Infect Dis 24:848-50.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from

Sola et al.
12
13. Naimi, T. S., K. H. LeDell, K. Como-Sabetti, S. M. Borchardt, D. J. Boxrud, J. Etienne, S. K. Johnson,
F. Vandenesch, S. Fridkin, C. O'Boyle, R. N. Danila, and R. Lynfield. 2003. Comparison of community-
and health care-associated methicillin-resistant Staphylococcus aureus infection. JAMA 290 :2976-84.
14. Peacock, S. J., C. E. Moore, A. Justice, M. Kantzanou, L. Story, K. Mackie, G. O'Neill, and N. P. Day.
2002. Virulent combinations of adhesin and toxin genes in natural populations of Staphylococcus aureus. 5
Infect Immun 70:4987-96.
15. Quinteros M, Radice M Famiglietti A Marín M Nicola F Casellas JM Kovensky J Couto E Golberg M
Gutkind G Pasterán F Soloaga R Galas M Bantar C and SIR Group. 2006. Comparative analysis during
two periods during 2004 and 2005. Bulletin 172. Asociación Argentina de Microbiología. Buenos Aires
Argentina. 10
16. Ramdani-Bouguessa, N., M. Bes, H. Meugnier, F. Forey, M. E. Reverdy, G. Lina, F. Vandenesch, M.
Tazir, and J. Etienne. 2006. Detection of methicillin-resistant Staphylococcus aureus strains resistant to
multiple antibiotics and carrying the Panton-Valentine leukocidin genes in an Algiers hospital. Antimicrob
Agents Chemother 50:1083-5.
17. Salgado, C. D., B. M. Farr, and D. P. Calfee. 2003. Community-acquired methicillin-resistant 15
Staphylococcus aureus: a meta-analysis of prevalence and risk factors. Clin Infect Dis 36:131-9.
18. Sola, C., P. Cortes, H. A. Saka, A. Vindel, and J. L. Bocco. 2006. Evolution and molecular characterization
of methicillin-resistant Staphylococcus aureus epidemic and sporadic clones in Cordoba, Argentina. J Clin
Microbiol 44:192-200.
19. Sola, C., H. A. Saka, A. Vindel, and J. L. Bocco. 2007. High frequency of Panton-Valentine leukocidin 20
genes in invasive methicillin-susceptible Staphylococcus aureus strains and the relationship with methicillin-
resistant Staphylococcus aureus in Cordoba, Argentina. Eur J Clin Microbiol Infect Dis 26:281-286.
Notes: CORPORATE NAME: Cordoba S. aureus Collaborative Study Group.
20. Tristan, A., M. Bes, H. Meugnier, G. Lina, B. Bozdogan, P. Courvalin, ME. Reverdy, M. Enright, F.
Vandenesch, and J. Etienne. 2007. Global Distribution of Panton-Valentine Leukocidin-positive Methicillin-25
resistant Staphylococcus aureus, 2006. Emerg Infect Dis 13:594-600.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
13
Figure Legends
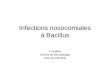
Figure 1
A. SmaI restriction patterns from representative CA-MRSA and CA-MSSA strains of each
subtype and representative HA-MRSA strains of more prevalent subtypes were digitalized, 5
schematized (middle) and analyzed to calculate Dice coefficient of correlation and to generate a
dendrogram (left) by unweighted-pair group method using average linkage clustering. Isolates
differing by up to six fragments were considered to be subtypes of a given clonal type and the
similarity cut-off was of 80%. Genotypes are denoted as: subtype (PFGE)-Sequence Type (ST by
MLST)-MRSA/MSSA-SCCmec type (right). Gs and Gr are representative strains of the A1 10
subtype showing susceptibility and resistance to Gentamicin, respectively. NC-8325 refers to
NCTC 8325 control strain.
B. PFGE DNA pattern of representative subtypes of the I major clone comparing MRSA (I1, I2
and I4) and MSSA (I5 and I6) strains isolated in Córdoba, Argentina during 2006. White arrows
indicates a single band of difference between I6 (CA-MSSA) and I2 (CA-MRSA) as well as 15
between I5 (CA-MSSA) and I1 (CA-MRSA). The SCCmec IVa element was detected by PCR
within the 190-kb band, found in the CA-MRSA strains but not in the CA-MSSA-derived 150-kb
band (data not shown). Subtypes are indicated at the top by numbers at the right side of the
letters. L: DNA molecular size markers in kb (lambda DNA ladder, Promega). NC: NCTC 8325
control strain. 20
C. Annual distribution of infections caused by CA-MRSA strains belonging to the I clonal family
from 2001 to 2006. n: total number of strains characterized as I pulsotype recovered in each year,
as indicated. Each genotype was named as: subtype (PFGE)-Sequence Type (ST by MLST)-
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
14
SCCmec type- spa type and they are indicated at the bottom of the figure. The more prevalent
genotype among CA-MRSA strains is shaded in gray in the legend.
D. Proposed genetic events leading to the emergence of different Community- and healthcare-
associated Methicillin resistant Staphylococcus aureus (CA-MRSA and HA-MRSA respectively)
clones within the CC5 lineage in Cordoba, Argentina. 5
Different HA-MRSA and CA-MRSA are indicated by boxes. Gray-shaded and white boxes
represent MSSA and MRSA, respectively. Full genotypes are given for their sequence type (ST),
SCCmec type, spaA repeats/ RIDOM spa type, PFGE type or subtypes, as indicated (I1- I6) and
presence of pvl and sea genes. Proposed evolutionary pathways are indicated by filled arrows.
Strains diversification through the horizontal transfer of pvl and sea genes and SCCmec allotypes 10
as well as minor changes detected in spa type (only differs by deletion or duplication of one
repeat) and in the PFGE type/subtype are indicated at the side of the arrows. The boxes having
dotted border indicate CA-MRSA and CA-MSSA clones PVL positive derived from the ancestral
MSSA-PVL negative clone (double lined box). The new CA-MRSA clone emerged and
disseminated in this region is indicated by a double dotted box border. Dotted lined arrows 15
represent evolutionary pathway of MRSA clones already proposed (18). ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
1
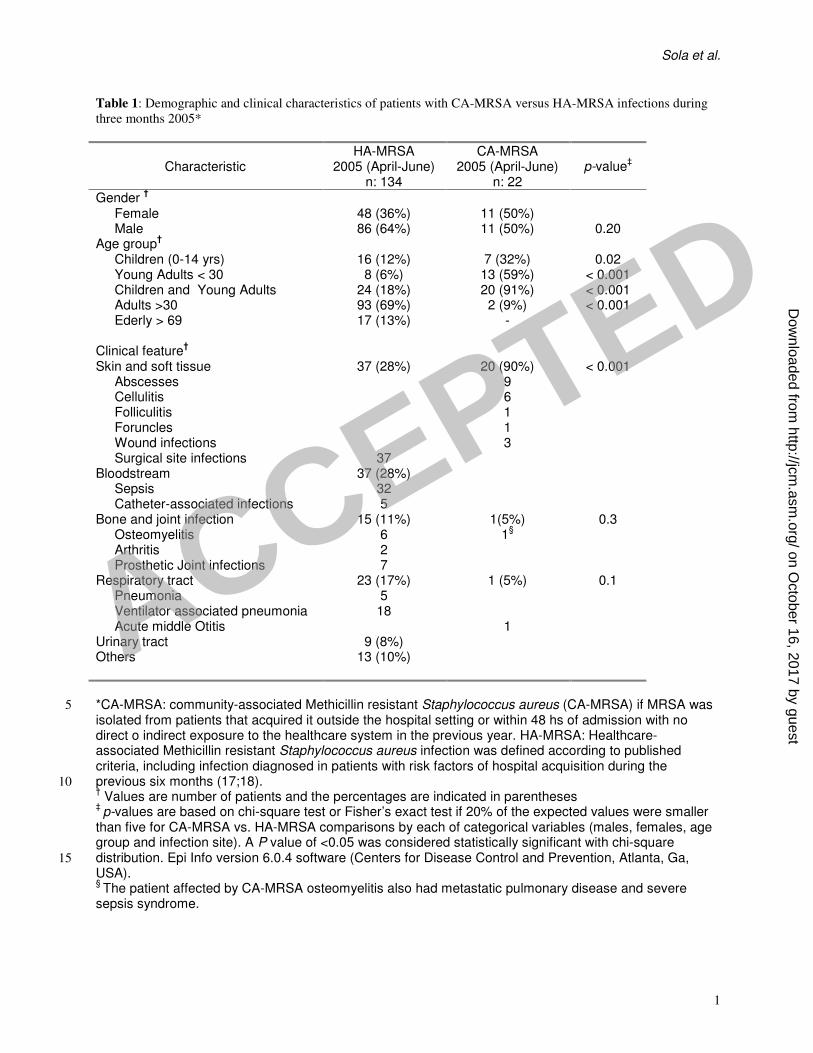
Table 1: Demographic and clinical characteristics of patients with CA-MRSA versus HA-MRSA infections during
three months 2005*
Characteristic
HA-MRSA 2005 (April-June)
n: 134
CA-MRSA 2005 (April-June)
n: 22
p-value
‡
Gender †
Female 48 (36%) 11 (50%) Male 86 (64%) 11 (50%) 0.20
Age group†
Children (0-14 yrs) 16 (12%) 7 (32%) 0.02 Young Adults < 30 8 (6%) 13 (59%) < 0.001 Children and Young Adults 24 (18%) 20 (91%) < 0.001 Adults >30 93 (69%) 2 (9%) < 0.001 Ederly > 69
17 (13%) -
Clinical feature†
Skin and soft tissue 37 (28%) 20 (90%) < 0.001 Abscesses 9 Cellulitis 6 Folliculitis 1 Foruncles 1 Wound infections 3 Surgical site infections 37
Bloodstream 37 (28%) Sepsis 32 Catheter-associated infections 5
Bone and joint infection 15 (11%) 1(5%) 0.3 Osteomyelitis 6 1
§
Arthritis 2 Prosthetic Joint infections 7
Respiratory tract 23 (17%) 1 (5%) 0.1 Pneumonia 5 Ventilator associated pneumonia 18 Acute middle Otitis 1
Urinary tract 9 (8%) Others 13 (10%)
*CA-MRSA: community-associated Methicillin resistant Staphylococcus aureus (CA-MRSA) if MRSA was 5
isolated from patients that acquired it outside the hospital setting or within 48 hs of admission with no direct o indirect exposure to the healthcare system in the previous year. HA-MRSA: Healthcare-associated Methicillin resistant Staphylococcus aureus infection was defined according to published criteria, including infection diagnosed in patients with risk factors of hospital acquisition during the previous six months (17;18). 10 † Values are number of patients and the percentages are indicated in parentheses
‡ p-values are based on chi-square test or Fisher’s exact test if 20% of the expected values were smaller
than five for CA-MRSA vs. HA-MRSA comparisons by each of categorical variables (males, females, age group and infection site). A P value of <0.05 was considered statistically significant with chi-square distribution. Epi Info version 6.0.4 software (Centers for Disease Control and Prevention, Atlanta, Ga, 15
USA). § The patient affected by CA-MRSA osteomyelitis also had metastatic pulmonary disease and severe
sepsis syndrome.
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from
Sola et al.
1
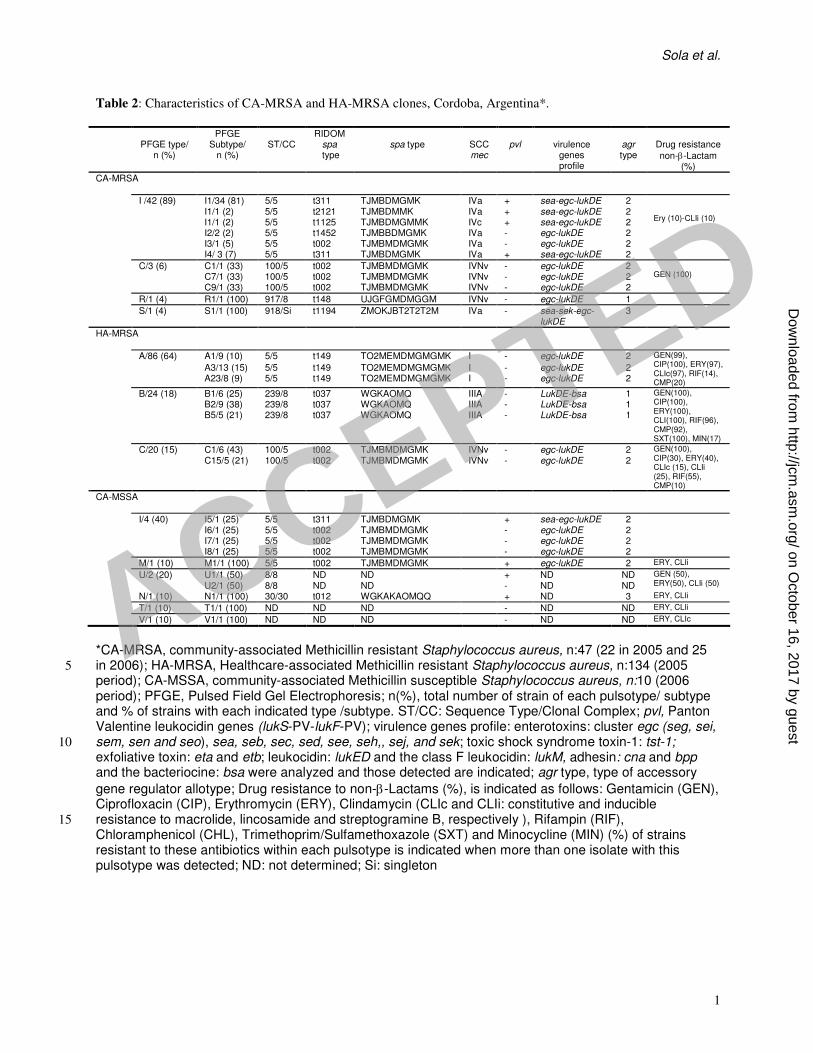
Table 2: Characteristics of CA-MRSA and HA-MRSA clones, Cordoba, Argentina*.
PFGE type/ n (%)
PFGE Subtype/
n (%)
ST/CC
RIDOM spa type
spa type
SCCmec
pvl
virulence
genes profile
agr type
Drug resistance
non-β-Lactam (%)
CA-MRSA
I /42 (89) I1/34 (81) 5/5 t311 TJMBDMGMK IVa + sea-egc-lukDE 2 I1/1 (2) 5/5 t2121 TJMBDMMK IVa + sea-egc-lukDE 2
I1/1 (2) 5/5 t1125 TJMBDMGMMK IVc + sea-egc-lukDE 2 I2/2 (2) 5/5 t1452 TJMBBDMGMK IVa - egc-lukDE 2 I3/1 (5) 5/5 t002 TJMBMDMGMK IVa - egc-lukDE 2 I4/ 3 (7) 5/5 t311 TJMBDMGMK IVa + sea-egc-lukDE 2
Ery (10)-CLIi (10)
C/3 (6) C1/1 (33) 100/5 t002 TJMBMDMGMK IVNv - egc-lukDE 2 C7/1 (33) 100/5 t002 TJMBMDMGMK IVNv - egc-lukDE 2 C9/1 (33) 100/5 t002 TJMBMDMGMK IVNv - egc-lukDE 2
GEN (100)
R/1 (4) R1/1 (100) 917/8 t148 UJGFGMDMGGM IVNv - egc-lukDE 1
S/1 (4) S1/1 (100) 918/Si t1194 ZMOKJBT2T2T2M IVa - sea-sek-egc-lukDE
3
HA-MRSA
A/86 (64) A1/9 (10) 5/5 t149 TO2MEMDMGMGMK I - egc-lukDE 2
A3/13 (15) 5/5 t149 TO2MEMDMGMGMK I - egc-lukDE 2 A23/8 (9) 5/5 t149 TO2MEMDMGMGMK I - egc-lukDE 2
GEN(99), CIP(100), ERY(97), CLIc(97), RIF(14), CMP(20)
B/24 (18) B1/6 (25) 239/8 t037 WGKAOMQ IIIA - LukDE-bsa 1 B2/9 (38) 239/8 t037 WGKAOMQ IIIA - LukDE-bsa 1 B5/5 (21) 239/8 t037 WGKAOMQ IIIA - LukDE-bsa 1
GEN(100), CIP(100), ERY(100), CLI(100), RIF(96), CMP(92), SXT(100), MIN(17)
C/20 (15) C1/6 (43) 100/5 t002 TJMBMDMGMK IVNv - egc-lukDE 2 C15/5 (21) 100/5 t002 TJMBMDMGMK IVNv - egc-lukDE 2
GEN(100), CIP(30), ERY(40), CLIc (15), CLIi (25), RIF(55), CMP(10)
CA-MSSA
I/4 (40) I5/1 (25) 5/5 t311 TJMBDMGMK + sea-egc-lukDE 2
I6/1 (25) 5/5 t002 TJMBMDMGMK - egc-lukDE 2
I7/1 (25) 5/5 t002 TJMBMDMGMK - egc-lukDE 2
I8/1 (25) 5/5 t002 TJMBMDMGMK - egc-lukDE 2
M/1 (10) M1/1 (100) 5/5 t002 TJMBMDMGMK + egc-lukDE 2 ERY, CLIi
U/2 (20) U1/1 (50) 8/8 ND ND + ND ND U2/1 (50) 8/8 ND ND - ND ND
GEN (50), ERY(50), CLIi (50)
N/1 (10) N1/1 (100) 30/30 t012 WGKAKAOMQQ + ND 3 ERY, CLIi
T/1 (10) T1/1 (100) ND ND ND - ND ND ERY, CLIi
V/1 (10) V1/1 (100) ND ND ND - ND ND ERY, CLIc
*CA-MRSA, community-associated Methicillin resistant Staphylococcus aureus, n:47 (22 in 2005 and 25 in 2006); HA-MRSA, Healthcare-associated Methicillin resistant Staphylococcus aureus, n:134 (2005 5
period); CA-MSSA, community-associated Methicillin susceptible Staphylococcus aureus, n:10 (2006 period); PFGE, Pulsed Field Gel Electrophoresis; n(%), total number of strain of each pulsotype/ subtype and % of strains with each indicated type /subtype. ST/CC: Sequence Type/Clonal Complex; pvl, Panton Valentine leukocidin genes (lukS-PV-lukF-PV); virulence genes profile: enterotoxins: cluster egc (seg, sei, sem, sen and seo), sea, seb, sec, sed, see, seh,, sej, and sek; toxic shock syndrome toxin-1: tst-1; 10
exfoliative toxin: eta and etb; leukocidin: lukED and the class F leukocidin: lukM, adhesin: cna and bpp and the bacteriocine: bsa were analyzed and those detected are indicated; agr type, type of accessory
gene regulator allotype; Drug resistance to non-β-Lactams (%), is indicated as follows: Gentamicin (GEN), Ciprofloxacin (CIP), Erythromycin (ERY), Clindamycin (CLIc and CLIi: constitutive and inducible resistance to macrolide, lincosamide and streptogramine B, respectively ), Rifampin (RIF), 15
Chloramphenicol (CHL), Trimethoprim/Sulfamethoxazole (SXT) and Minocycline (MIN) (%) of strains resistant to these antibiotics within each pulsotype is indicated when more than one isolate with this pulsotype was detected; ND: not determined; Si: singleton
ACCEPTED
on October 16, 2017 by guest
http://jcm.asm
.org/D
ownloaded from