Embed Size (px)
Citation preview

Integrating Staging of
Colorectal Cancer
Paul Finan
John Goligher Colorectal Unit
Leeds General Infirmary

Staging of Colorectal Cancer
• Prediction of survival
• Allows appropriate international comparisons of
outcome
• Determination of treatment
• Entry into trials
• Response to different therapeutic modalities

Staging of Colorectal Cancer

Staging of Colorectal Cancer
• Confusion for nearly 80 years
• Some attempt at uniformity
• Opportunity to standardise staging

Dukes‟ Classification
A
B
C

Staging of Colorectal Cancer
• 1932 Dukes‟ classification
• 1949 Kirklin‟s classification
• 1954 Astler-Coller system
• 1988 TNM (now version 7)
• (not to mention SEER, Stage I-IV etc)

Staging of Colorectal CancerDukes‟ Stage

Staging of Colorectal CancerAstler-Coller

Evolution of Dukes‟ Classification

Dukes‟ ClassificationC1
• Dukes 1929 – extension into perirectal tissues withoutnodal involvement
• Dukes 1932 – metastases present within lymph nodes
• Dukes 1935 – lymph node involvement but excludingthe apical node
• Astler 1954 – limited to bowel wall and positive nodes
• GITSG 1975 – less than or equal to four involved nodes
Fitzgerald 1982

“Modified” Dukes‟ Classification
• Introduction of stage D
• “extensive local spread or with distant
metastases”
• Some discussion over “incomplete
removal of the primary tumour”
Whittaker and Goligher 1976

Staging of Colorectal CancerTNM Staging

Staging of Colorectal Cancer
Stage T N M
0 Tis N0 M0
I T1-2 N0 M0
II T3-4 N0 M0
III Any T N1-2 M0
IV Any T Any N M1

Staging of Colorectal Cancer
Stage T N M
I T1-2 N0 M0
IIA T3 N0 M0
IIB T4 N0 M0
III A T1-2 N1 M0
IIIB T3-4 N1 M0
IIIC Any T N2 M0

Staging of Colorectal CancerTNM Staging
• Clinical TNM
• Pathological TNM
• Integrated (clinico-pathological) TNM

Staging of Colorectal CancerClinical T-stage
•Major
advances with
rectal cancer
•Less accuracy
with colonic
cancers

Submucosa intact but loss part deep mucosal layer
SM
DM
uT1

uT2
Submucosal reflection lost- outer border MP intact

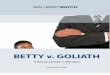
MR Imaging for Rectal Cancer
Accurate analysis of depth of invasion, relationship to mesorectal
fascia and selection for pre-operative therapy

Staging of Colorectal CancerClinical N-stage
• Certainly operator dependent
• Loose relationship with size
• Some relationship with contour
• Loose relationship with sonographic
appearances
• Hope for lymph node specific agents

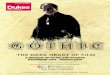
Staging of Colorectal CancerClinical M-stage
Solitary hepatic
metastasis

Staging of Colorectal CancerProblems with Clinical TNM
• Accurate assessment of T-stage pre-
operatively
• Always difficulty with nodal disease
• Refined scanning with MR, CT and PET
• Involvement of RCR

Staging of Colorectal CancerProblems with Pathological TNM
• Poor clinical evidence for change
• Classification of mesorectal deposits
• Influence of pre-operative therapy
• Stage migration and influence on
treatment
• Settling on an agreed version (5,6 or 7)
Quirke et al 2007

Staging of Colorectal CancerProblems with Pathological TNM
• Define and agree R0, R1 and R2 status
• Attempt to resolve issues around
mesorectal deposits (N or T) including size
and contour
• Ensure that “y” prefix is used
• Work with agreed proformas from R.C.
Path

Staging of Colorectal CancerTNM Staging
• Pre-op MDT – clinical TNM stage
• Post-op MDT – pathological TNM stage
• Pre-op treatment – “y” prefix
• Overall integrated TNM stage(e.g. pT2, pN1, cM1, R0, V1)

Staging of Colorectal Cancer

National Colorectal Cancer Dataset
Hospital
Episode
Statistics
Linked national
dataset
English cancer
registry information
De-duplication
A B
A
De-duplication
C D
C

Staging fields requested in the NCDR
• Clinical T stage
• Clinical N stage
• Clinical M stage
• Combined clinical TNM stage
• Pathological T stage
• Pathological N stage
• Pathological M stage
• Combined pathological TNM
stage
• Integrated T stage
• Integrated; N stage
• Integrated M stage
• Combined integrated TNM
stage
• Dukes‟ stage
• Metastases at diagnosis
• Number of nodes examined
• Number of positive nodes
• Tumour size
• TNM version
• Neo-adjuvant treatment flag
• Nottingham prognostic index
• Breslow thickness
• Gleason score
• FIGO score

Rules used to derive stage across the multiple
staging fields in the NCDR
• The information in each staging field was „cleaned‟ to ensure only valid staging information was present
• For each TNM class (i.e. clinical, pathological or integrated) the individual T, N and M information were combined to give an overall TNM stage of 1 to 4. If information conflicted between the combined form of a TNM stage and the individual component the highest overall stage was retained.
• All the TNM stage categories were then converted to Dukes‟ stage. If both a Dukes and a pathological or integrated TNM were provided for an individual but the information conflicted then the highest stage was taken

Rules used to derive stage across the multiple
staging fields in the NCDR
• If no Dukes‟ stage or pathological/integrated stage was available for an individual but a clinical TNM stage was provided then the clinical stage was used.
• If the presence of positive nodes was recorded in the dataset then empty or lower stages were upgraded to Dukes‟ C
• If the presence of metastases was recorded in the dataset then empty of lower stages were upgraded to Dukes D

Staging information submitted into the NCDR
Cancer
Registry
Clinical
TNM
Pathological
TNM
Integrated
TNM
Dukes‟
ECRIC X X
NWCIS X X X
NYCRIS X
OCIU X X X
SWCIS X X X
ThCR X X X
TrCR X X
WMCIU x x x X

Percentage distribution of Dukes Stage
between 1995 - 2008
Cancer
Registry
Dukes‟ Stage
A B C D Unknown
ECRIC 9.1 20.0 22.4 12.1 36.3
NWCIS 6.6 20.7 22.4 2.2 48.1
NYCRIS 9.6 22.8 20.4 21.1 26.1
OCIU 9.2 24.1 24.3 12.0 30.4
SWCIS 7.9 21.8 21.1 6.5 42.7
ThCR 6.7 21.0 19.4 20.2 32.7
TrCR 6.8 16.3 16.6 5.7 54.5
WMCIU 9.2 26.2 24.6 14.5 25.6
Total 8.0 21.5 21.1 12.2 37.2

Percentage distribution of Dukes Stage in
2008
Cancer
Registry
Dukes‟ Stage
A B C D Unknown
ECRIC 12.6 22.7 21.6 15.8 27.3
NWCIS 9.0 20.5 25.0 4.1 41.4
NYCRIS 8.9 20.6 19.6 22.2 28.6
OCIU 9.1 21.4 22.3 5.0 42.1
SWCIS 11.2 22.6 22.5 15.5 28.2
ThCR 9.1 23.0 22.0 19.6 26.3
TrCR 12.7 21.4 22.3 7.6 36.0
WMCIU 11.1 25.6 24.4 15.9 23.0
Total 10.4 22.3 22.5 14.3 30.6

Staging of Colorectal CancerProposal from NYCRIS
• Continue with 5th edition of TNM
• Modify databases to record clinical,
pathological and integrated TNM stage
• A need for pre-treatment AND post-
treatment stage
• Advice needed on position of stage after
pre-operative (“y”) treatment
• Links with NBOCAP audit and NCIN

Staging of Colorectal CancerIssues for Discussion
• Agree on an integrated clinico-pathological
stage
• Confirm version of TNM
• Particular problems with very early lesions
and those that have no resection
• Standardise pre-operative stage requiring
non-surgical treatment
• Agree the lines of responsibility