Embed Size (px)
Citation preview

1
Staging of colorectal and appendiceal cancers
Keeping the pathologists sane and the surgeons happ y
Sanjay Kakar, MD
2015 UCSF CURRENT ISSUES IN SURGICAL PATHOLOGY
Staging of colorectal and appendiceal cancers
Keeping the pathologists sane and the surgeons happ y
Sanjay Kakar, MD
2015 UCSF CURRENT ISSUES IN SURGICAL PATHOLOGY
Neils Bohr: Nobel Prize 1922Prognostication is very difficult, especially if it is about the future
Einstein: Nobel Prize 1921God does not play dice with the universe

2
Challenges in AJCC staging
Colorectal AdenocarcinomapT3 vs. pT4a
Satellite tumor deposits: pN1c
Tis vs. T1 tumor
CAP Protocol elements:Tumor regression, mesorectal excision, sigmoid vs. rectal location, peritoneal reflection
Appendiceal carcinomaLow grade mucinous neoplasm
Goblet cell carcinoid
pT3 and pT4AJCC 7 th edition
pTclassification
Definition
pT3 Tumor invades through the muscularis propria into pericolorectal tissues
pT4a Tumor penetrates the visceral peritoneum
pT4b Tumor directly invades or is adherent to other organs or structures
T4 staging
• Widely underreported• Cytology from serosal surface of
pT3 tumors: 19% positive *
• Review of pT3 cases: 20% restaged as pT4 **
*Panarelli, AJSP 2013**Hosseini/Kakar, USCAP 2014
Problems in pT4 staging
• Varying terminology• Anatomic differences in subsites• Criteria used to define peritoneal
involvement• Challenges in interpretation

3
T stage Definition
pT3 Pericolorectal tissueSubserosal connective tissueAdventitia
pT4a Visceral peritoneumSerosal surfacePeritoneal surface
pT4b Extramural involvementIntramural extension: no change in TMicroscopically proven
Margin: terminology
Commonly used termsRadial marginDeep marginCircumferential marginNonperitonealized circumferential margin
Positive margin: tumor <1 mm
Anatomic subsite Relation to peritoneumCecum Peritoneal
Transverse colon Peritoneal
Sigmoid colon Peritoneal
Ascending colon Anterior, lateral: peritonealPosterior: retroperitoneal
Descending colon Anterior, lateral: peritonealPosterior: retroperitoneal
Rectum, upper 1/3 Anterior, lateral: peritonealPosterior: retroperitoneal
Rectum, middle 1/3 Anterior: peritonealPosterior, lateral: retroperitoneal
Rectum, lower 1/3 Retroperitoneal
CAP staging protocol
CecumTransverseSigmoid
Ant-lateralAscendingDescending
RectumUpper 1/3Mid 1/3
PosteriorAscendingDescending
RectumPosteriorLower 1/3

4
pT3 vs. pT4AJCC 7 th edition
Site pT classificationPeritonealizedsites
pT3: subserosapT4a: serosal surfacepT4b: directly into adjacent organRadial margin: not applicable
Retroperitonealsites
pT3: adventitia pT4a: not applicablepT4b: directly into adjacent organRadial margin: involved <1mm
Rectum: posterior view
• Non-peritonealizedCRM is inked
Problems in pT4 staging
• Varying terminology• Anatomic differences in subsites• Morphologic features of peritoneal
involvement• Challenges in interpretation
Criteria for serosal involvement pT4a: CAP/AJCC staging
• Tumor at serosal surface Reaction: mesothelial hyperplasia, inflammation, erosion/ulceration
• Free tumor cells on serosal surfaceUlceration of visceral peritoneum

5
Serosal involvement
Tumor at serosal surface
Disrupted serosal surface with free floating tumor c ells Free floating tumor cells in clefts

6
Additional sections: obvious pT4a
Criteria for serosal involvement pT4a: CAP/AJCC staging
• Tumor at serosal surface • Free tumor cells on serosal surface
(esp. in clefts with tissue reaction)
Perforation: Tumor contiguous with serosalsurface through inflammation
Criteria for serosal involvement pT4a: CAP/AJCC staging
• Tumor at serosal surface • Free tumor cells on serosal surface• Tumor continuous with serosal surface
through perforation (inflammatory reaction)
• Cytology smears

7
Tumor <1 mm from serosal surface with mesothelial reaction
Serosal hemorrhage, acute inflammation
Criteria for serosal involvement
AJCC: tumor at or on serosalsurface • Tumor <1 mm: not T4a• Nonperitonealized radial margin:
Tumor <1 mm: positive
Tumor <1mm with reaction
• 13 (46%) pT3 <1 mm from serosalsurface had +ve cytology
• All had serosal reaction• Peritoneal recurrence same as
conventional pT4a tumors
Panarelli, AJSP 2013

8
pT4a: suspicious features
• Tumor <1 mm with reaction• Tumor >1 mm with reaction• Tumor <1 mm, no reaction• Acellular mucin at or <1mm from surface
Not considered as pT4aDeeper levels, additional sections
pT3 or pT4a: significance
• Prognosis• Peritoneal recurrence• Choice of therapy
Additional radiotherapy for T4 disease
pT4a in practice
• Margin vs. peritoneal involvement• Use AJCC criteria• Additional work-up for suspicious
cases

9
Challenges in AJCC staging
Colorectal AdenocarcinomapT3 vs. pT4a
Satellite tumor deposits: pN1c Tis vs. T1 tumor
CAP Protocol elements:Tumor regression, mesorectal excision, sigmoid vs. rectal location, peritoneal reflection
pN Definition
NX Regional lymph nodes cannot be assessed
N1 N1a: metastasis in 1 LNN1b: metastasis in 2-3 LNsN1c: tumor deposit(s) in subserosa, mesentery, or non-peritonealized pericolic/perirecal tissue, without LN metastasis
N2 N2a: metastasis in 4-6 LNN2b: metastasis in >7 LNs
Why N1c?
• AJCC: prior editions3 mm size cutoffVenous invasion: irregular outlineTotally replaced LN: round outline
• Worse prognosis than N0 disease
Outline:Round or irregular

10
Outline:Round or irregular
Orphan artery sign
Elastic stain highlights vein

11
Smooth muscle actin: venous invasion

12
CRC: Extramural venous invasion
• Independent predictor of poor outcome• UK Royal College: 25% rate for audit
Recommendations:• Record separately from small vessel
invasion• 4-5 sections of tumor• Elastic stain: routinely/suspicious areas
Messenger, J Clin Pathol 2011Kirsch, Human Pathol 2012
N1c: conflicting featuresNo positive nodes, 1 TD: N1c3 positive LN, no TD: N1b
1 positive LN, no TD: N1a1 positive LN, 5 TD: N1a
No positive nodes, 1 TD: N1cNo positive nodes, 5 TDs: N1c
• AJCC, 7 th edition, page 151: Discrete foci of tumor away from leading edge of tumor without evidence of residual LN tissue should be regarded as TD
• AJCC, 7 th edition, page 155: Replaced nodes should be separately counted as positive nodes in the N categ ory
N1c in practiceIs it a tumor deposit
Helpful histologic featuresLymph node Thick capsule
Subcapsular sinusRim of lymphocytes
Venous invasion Accompanying arteryElastic stain
Tumor deposit Round outline, no remnant lymph node or vein
Rock, Arch Path Lab Med, 2014
Do not add tumor deposits and lymph nodes for - N stage- Assessing adequacy of LN dissection
Challenges in AJCC staging
Colorectal AdenocarcinomapT3 vs. pT4a
Satellite tumor deposits: pN1c
Tis vs. T1 tumor
CAP Protocol elements:Tumor regression, mesorectal excision, sigmoid vs. rectal location, peritoneal reflection

13
AJCC: T definition
pT DefinitionTis Carcinoma in situ, invasion of lamina
propria/ muscularis mucosa(Intramucosal adenocarcinoma)Virtually no chance of lymph node metastasis
T1 Tumor invades submucosa(Invasive adenocarcinoma)Stromal desmoplasia
Intramucosal (Tis) Invasive (T1)
Pathology report
• Intramucosal adenocarcinoma (pTis )No desmoplasiaSingle cell infiltration in lamina propria
• AJCC 7 th editionTis, not at risk for LN metastasis
• No invasive adenocarcinoma (pT1)
Invasive adenocarcinoma (T1) in polypIndications for colectomy
Prognostic features
Grade: poor differentiation
Lymphovascular: present
Margin: <1 mm
Tumor budding
Depth of submucosal invasion

14
Tumor budding• Individual or small discrete cell
clusters (<5 cells) at the invasive edge• Independent adverse prognostic factor
Adjuvant therapy in stage IIColectomy for malignant polyps
• Recommended: UICC, ADASPNot required by CAP
Tumor budding
2 grades: 20x• High: >10• Low <10
Use of keratin stain
Mitrovic, Mod Pathol 2012
Invasive adenocarcinoma (T1) in polypIndications for colectomy
Prognostic features
Grade: poor differentiation
Lymphovascular: present
Margin: <1 mm
Tumor budding
Depth of submucosal invasion
Haggitt levels

15
Kikuchi levels
SM1, SM2 and SM3
Tis and T1 in practice
• Clarify the term intramucosaladenocarcinoma
• T1 adenocarcinoma in polyp: include prognostic features
CAP colorectal cancer protocol
Frequently asked questions• Tumor regression score• Total mesorectal excision• Sigmoid vs. rectal location• Relationship to peritoneal
reflection
CAP protocol 2015 (upcoming)
Description Tumor regression score
No viable cancer cells 0 (complete response)
Single or rare groups of cancer cells
1 (near complete response)
Residual cancer with evident tumor regression, but more than single or rare groups of cancer cells
2 (partial response)
Extensive residual cancer with little or no evident tumor regression
3 (minimal or no response)
Ryan, Histopathol, 2005

16
Challenges in AJCC staging
Colorectal AdenocarcinomapT3 vs. pT4a
Satellite tumor deposits: pN1c
Tis vs. T1 tumor
CAP Protocol elements:Tumor regression, mesorectal excision, sigmoid vs. rectal location, peritoneal reflection
Appendiceal carcinomaLow grade mucinous neoplasm
Goblet cell carcinoid
LAMN: staging challenges
• Should LAMN be staged?
Should LAMN be staged?
WHO 2010 classification• Low grade carcinoma
WHO 2010.
Appendiceal adenoma: intact muscularis mucosa .
LAMN: rests on fibrous stroma, obliteration of MM

17
Should LAMN be staged?
WHO 2010 classification• Low grade carcinoma
AJCC: YesMost pathologists: No
LAMN: staging problems
• T stage is difficult to apply• Erroneous interpretation as
conventional adenocarcinoma• Acellular mucin
Appendix: AJCC staging
T1 Tumor invades submucosaT2 Tumor invades muscularis propriaT3 Tumor invades through muscularis propria into
subserosa or into mesoappendixT4a Tumor penetrates visceral peritoneum, including
mucinous peritoneal tumor within the right lower quadrant
T4b Tumor directly invades other organs or structure s
M1a Intraperitoneal metastasis beyond the right lower quadrant, including pseudomyxoma peritonei
M1b Nonperitoneal metastasis
Invasive adenocarcinomaLAMN
Hemicolectomy not needed Hemicolectomy for staging

18
Acellular mucin: T4a or T1
LAMN staging
T staging not useful• Assign best possible category• Emphasize diagnosis of LAMN
Appendiceal tumors: significant factors• Extrappendiceal mucin/epithelium• High grade features• Destructive invasion• Resection margin
Appendix: AJCC staging
T1 Tumor invades submucosaT2 Tumor invades muscularis propriaT3 Tumor invades through muscularis propria into
subserosa or into mesoappendixT4a Tumor penetrates visceral peritoneum, including
mucinous peritoneal tumor within the right lower quadrant
T4b Tumor directly invades other organs or structure s
M1a Intraperitoneal metastasis beyond the right lower quadrant, including pseudomyxoma peritonei
M1b Nonperitoneal metastasis
Goblet cell carcinoid
• Staged as adenocarcinoma
• Right hemicolectomywith LN dissection

19
CAP colorectal cancer checklist
• 14 required elements• 4 optional elementsPathology reportAJCC: T3N1cV1R1B0Molecular:
KRAS exon 13 mutationNRAS, BRAF, PIK3CA: wild typePTEN absentP53 mutation presentMicrosatellite stableConsensus molecular subtype 4 (CMS4)Next generation sequencing……….
“Good checklists are precise, to the point, and easy to use. They do not try to spell out everything.”

20
“ the volume and complexity of what we know has exceeded our individual ability to deliver its
benefits correctly, safely or reliably.”
CAP colorectal cancer protocol
Protocol elements
Tumor regression score (for cases with neoadjuvant therapy)
Completeness of mesorectal envelope
Relationship of tumor to peritoneal reflection
Sigmoid vs. rectal location
Total mesorectal excision (TME)
The mesorectal fascia (fascia propria or the pelvic visceral fascia) surrounds the rectum and is separated from the presacral fascia (Waldeyerfascia) by an avascular plane. The two fascia merg e inferiorly at the level of levator ani muscles. Durin g rectal surgery, dissection is performed along this avascular plane. The intactness of the mesorectalexcision is one of the most important features determining local recurrence.
Rectal cancer: surgery
• Local recurrence: quality of surgery• Anterior resection
Without TME: 20-30%With TME: 8-10%Adjuvant therapy: 2-3%
• Pathologic evaluation for quality of TME

21
Descriptor Status of mesorectal excision
Complete Intact bulky mesorectum with smooth surface, only minor irregularities, defects <5 mmNo coningSmooth circumferential margin
Nearly complete Moderate bulkDefects >5 mm, not extending to muscularis
Incomplete Little bulkDefects >5 mm extending to muscularisIrregular circumferential margin
Parfitt, J Clin Pathol 2006
Mesorectal excision
• Assess completeness• Ink the non-peritonealized
circumferential resection margin• Distinguish margin from serosal
surface in submitted sections
TME: tumors of middle and lower third of rectumPartial mesorectal excision: upper rectum
• Avascular plane between mesorectal fascia and presacralfascia
• Fascia propria, pelvic visceral, fascia recti
• Waldeyer fascia (presacral fascia)
Complete Incomplete
Parfitt, J Clin Pathol 2006

22
Tumor regression: problems
• Poor reproducibility• Lack of standardized scoring scheme
Tumor regression scoring
Issues under consideration• Possible two point grading system
Complete/near complete responsePartial or no response
• Sampling4-5 sections or entire tumor bedLevel sections
CAP protocol 2015 (draft)
Description Tumor regression score
No viable cancer cells 0 (complete response)
Single or rare groups of cancer cells
1 (near complete response)
Residual cancer with evident tumor regression, but more than single or rare groups of cancer cells
2 (partial response)
Extensive residual cancer with little or no evident tumor regression
3 (minimal or no response)
Ryan, Histopathol, 2005
Sigmoid vs. rectal location
CAP protocol 2015 (draft):
A tumor is classified as rectal if its lower margin is within 16 cm of the anal verge or if any part of the tumor is located within the supply of the superior rectal artery. Th e rectum commences at the sacral promontory and the junction of sigmoid colon and rectum is anatomically marked by fusion of tenia coli to form the circumferential longitudinal muscle of the rectal wall. Intraoperatively, the rectosigmoid junction corresponds to the sacral promontory. The location is classified as rectosigmoid when differentiation betw een rectum and sigmoid sites cannot be reliably determi ned.
Reference: Wittekind C, Henson DE, Hutter RVP, Sobin L H, eds. TNM Supplement: A Commentary on Uniform Use. 2nd ed. Ne w York, NY: Wiley-Liss; 2001.

23
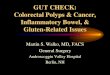
Tumor in relation to the peritoneal reflectionAnteriorly, the peritoneal reflection is located at the junction of middle and lower third of the rectum, while laterally, it is located at th e junction of upper and middle third of the rectum. Posteriorly, the reflection is located higher and most of the posterior rectum does not have a serosal covering. (a) Whether an adenocarcinoma located in the rectum has a circumferential resection (radial) margin (CRM) or a peritoneal (serosal) sur face (with no true circumferential resection margin), depends on its location in relati on to the peritoneal reflections. Tumors below the anterior peritoneal reflection wil l have a 360-degree CRM, while those above it may have (CRM) or a peritoneal (sero sal) surface, or both, depending on the precise location.(b) Neoadjuvant therapy and total mesorectal excision are considered standard of care for rectal adenocarcinomas 'below the anterior peri toneal reflection', while the opinions about use of these modalities vary about r ectal adenocarcinomas located above the anterior peritoneal reflection. Conservat ive options like transanal disc excisions are often considered for location 'below the anterior peritoneal reflection'. In these contexts, the peritoneal reflection refers to the junction of upper and middle third of the rectum. (c) If information about tumor location with respec t to the peritoneal reflection is included in the report, the aspect of rectum in quest ion (posterior, lateral, anterior) should also be noted.Reference:Kenig J, Richter P. Definition of the rectum and lev el of the peritoneal reflection - still a matter of debate? Wideochir Inne Tech Malo Inwazyjne. 2013;8:183-186.

24
LAMN: T stage is difficult to apply

25

26
Is pTis with poor differentiation at higher risk?
Tis or T1
Poor differentiation: word of cautionEnsure complete resection/follow-
up/colectomy
CAP/AJCC protocol
• pT3 vs. pT4• Satellite tumor deposits: pN1c • Adenocarcinoma in polyp: TIS vs. T1
• Mesorectal excision• Tumor regression grading

27
CAP/AJCC protocol
• pT3 vs. pT4• Satellite tumor deposits: pN1c • Adenocarcinoma in polyp: TIS vs. T1 • Mesorectal excision
• Tumor regression grading
Tumor regression grading
• Neoadjuvant therapy and TME• Assess response to treatment
Grade 0: no residual tumor Grade 2 (minimal): tumor outgrown by fibrosis

28
CAP colorectal cancer protocol
Essential elements Optional elementsSite, procedure MSI-related features
Size Type of polyp
Perforation Mesorectal envelope
Histologic type, grade Additional
Lymphovascular, perineural
Treatment effect
Tumor extension (pT)
Margin
Lymph node
Tumor deposits
Stage
Acellular mucin poolsTumor regression grading
• Possible two point grading systemComplete/near complete responsePartial or no response
• Sampling4-5 sections or entire tumor bedLevel sections
• FibrosisTumor regression, necrosis of normal Desmoplasia

29
Mandard tumor regressive grade
Description Tumor regression grade
No viable cancer cells 1
Rare cancer cells 2
Residual cancer outgrown by fibrosis
3
Minimal or no tumor kill; extensive cancer
4
No regressive change 5
Mandard, Cancer, 1994
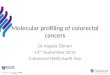
Total mesorectal excision• The Waldeyer's fascia is synonymous with the presacr al fascia and is more commonly described in surgery
textbooks, rather than in anatomy textbooks. Althou gh Waldeyer himself did not actually describe this e xact anatomy, it is credited to him as he was the first to describe the anatomy of pelvic fascia in detail. [1][2]
• The presacral fascia lines the anterior aspect of th e sacrum , enclosing the sacral vessels and nerves . It continues anteriorly as the pelvic parietal fascia , covering the entire pelvic cavity .[3] It has been erroneously described as the posterior aspect of the mesorectal fascia. [4] These two fascias are in fact, separate anatomical entities. During rectal surgery and mesorectum excision, dissection along the avascu lar aveolarplane between these two fascias, facilitates a stra ightforward dissection and preserves the sacral ves sels and hypogastric nerves .
• The presacral fascia is limited postero-inferiorly, as it fuses with the mesorectal fascia, lying above the levator ani muscle, at the level of the anorectal junction. [5] The colloquial term, among colo-rectal surgeons, for this inter-fascial plane, is known as the "holy plane" of dissection first coined by Heald RJ. [6]
• The mesorectal fascia, also known as the fascia prop ria or the pelvic visceral fascia, has been original ly described as the fascia recti in Waldeyer's publicat ion, Das Becken. Fascia recti is also a term common ly used among French surgeons to describe the mesorect al fascia. [7] Confusingly, fascia recti is described in some anatomy books, referring to the fascia of the rectus abdominis muscle .
• Identification and preservation of the Waldeyer’s fa scia is of fundamental importance in preventing complications and reducing local recurrences of rectal cancer .[8] Hence attention to this anatomy is essential in contemporary rectal surgery.
• Background• Total mesorectal excision is a common procedure used in the treat ment of colorectal cancer in which a significant
length of the bowel around the tumor is removed. Total mesorectal e xcision addresses earlier treatment concerns regarding adequate local control of rectal cancer while performing an anterior resection.
• The term total mesorectal excision strictly applies when performing a low anterior resection for tumors of the middle and the lower rectum, wherein it is essential to remov e the rectum along with the mesorectum up to the level of the levators. The principles of total mesorectal exci sion (sharp mesorectal excision) are also applied during an abdominoperineal excision of the rectum and for tumors of th e upper rectum, although these are considered distinct from standard total mesorectal excision. In an abdominoperineal excision of the rectum where the tumor exists below the level of the levators, the late ral margins of the tumor are inferior to the mesorectumand the benefits of total mesorectal excision do not apply. Ante rior resections involving the upper rectum may be completed with mobilization of the rectum to beyond 5 cm of the l ower margin of the tumor, and which is often above the level of the levator and is sometimes referred to as partial mesorectal excision.
• The treatment of rectal cancers is multimodal with adjuvan t radiotherapy and chemotherapy having benefits in some settings. In addition, accurate preoperative staging is depen dent on good radiological support. It is therefore necessary to subject all rectal cancers to multidepa rtment conference and to design individualized treatment plans based on a well-defined protocol. This serves th e dual purpose of maintaining a consistent evidence-based approach as well as creating a dataset for prospecti ve analysis and feedback.
• Indications• Total mesorectal excision is indicated as a part of low anterior resection for patients with adenocarcinoma of the
middle and lower rectum. Total mesorectal excision is now conside red the gold standard for tumors of the middle and the lower rectum.
• Outcomes• Circumferential resection margin positivity rate is about 5% or less for low anterior resections with total
mesorectal excision, whereas it is between 10% and 25% for a bdominoperineal excision of the rectum. There is understandably a higher local recurrence rate following abdominoperinea l excision of the rectum. Five-year survival and disease-free survival rates are significantly lower with total mesorectal excision.
• Evidence suggests that a circumferential resection margin of 1 mm or less adversely affects cancer-specific survival, local recurrence, and distant metastasis. [1]
• http://emedicine.medscape.com/article/1893507-overview
• 13 (46%) pT3 <1 mm from serosal surface had +ve cytology
• All had serosal reaction• Fibroinflammatory: 12• Vascular: 8, abscess:1• Rx mesothelial:6, Hem/fibrin: 11• Hemorrhage/fibrin on serosa

30
Elastic stain
• Shinto: recurrence 35% in tumors that involved elastic lamina vs. 21% that did not
• 5-yr survival 57% vs. 79%• Kojima: 34% with elastic
involvement but not serosa vs23% with serosal involvement
High risk features Microsatellite stable tumors
• Poorly differentiated• Lymphatic/vascular invasion• Perineural invasion• Bowel obstruction, perforation• <12 lymph nodes• Close, indeterminate, positive margin
NCCN guidelines NCCN.org
N1c staging• I've been asked this question several times. The AJ CC stage designations on page 155 clearly
indicate that N1c can be used with any T. However, the text on page 151 is confusing. The message being conveyed on page 151 is that when a satellite tumor deposit occurs with a T1 or T2 tumor (with negative lymph nodes), it should not be inter preted as discontinuous spread and hence should not be classified as T3, but rather as T1/T2 N1c. The way it is written can lead to the mistaken impression that N1c should be used only wi th T1 or T2 tumors.
• why PN1c of colon cancer was put under N stage and not under T stage since it describes the presence of tumor. pN1c: Tumor deposit(s) in the su bserosa, or non-peritonealized pericolic or perirectal tissues without regional lymph node meta stasis
• Kay: The criteria for tumor deposits are more fully elucidated in the text of the AJCC chapter. These deposits are discontinuous, but must be within the lymph node draining basin for the primary tumor and are not clearly entirely replaced lymph n odes. pN1c was chosen as a unique category for these discontinuous tumor deposits because of studi es identifying these deposits as having an adverse outcome on prognosis beyond that seen in pT 3 or pT4 node-negative colon cancers. Prior to the 7th edition designating these as N1c, some p athologists regarded tumor deposits as pT3 or pT4 tumor, others as positive lymph nodes. At the s ame time, many oncologists regarded them as equivalent to positive lymph nodes when making deci sions regarding adjuvant therapy for node-negative tumors.
Focal desmoplasia and submucosal extension

31
Tumor extending into submucosa: true invasion? Tumor extending into submucosa: true invasion?
2 high grade TIS cases(1) recurrence (2) lymphatic invasion. Both desmopl asia Intramucosal adenocarcinoma-high grade

32
Colon: any subsite
T4b
pT4a and pT4b
CAP/AJCC 7th edition
Definition
pT4a Tumor penetrates visceral peritoneum
pT4b Tumor directly invades or is adherent to other organs or structures
CAP/AJCC 6th edition
Definition
pT4a Tumor directly invades or is adherent to other organs or structures
pT4b Tumor penetrates visceral peritoneum
N1c: impact on final stage
Stage T N
IIIA T1-T2T1
N1 or N1cN2a
IIIB T3-T4aT2-T3T1-T2
N1 or N1cN2aN2b
IIIC T4aT3-T4aT4b
N2aN2bN1-2

33
TA with high grade dysplasia

34
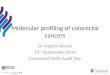
Colon: peritonealized areas
T3 T4a
Peritonealized region
Peritoneal reflection
Non-peritonealized circumferential margin
Parfitt, J Clin Pathol 2006

35
Why do TDs affect N?
• Adverse outcome similar to node-positive disease
• Some TDs are irregular and are not LN metastasis
Should N1c be used only for T1 and T2 tumors?
• AJCC, 7 th edition, page 151: If tumor deposits are seen in lesions that would otherwise be classified as T1 or T2, the T classification is not changed, but nodule is recorded as TD and staged as N1c• Page 155:Stage group table clearly indicates that N1ccan be used with any T

36
Pathology diagnosis
Tubular adenoma with high grade dysplasia and intramucosaladenocarcinoma
I have nothing to disclose

37
Tumor contiguous with serosal surface through inflammation
Tumor >1 mm, serosal reaction

38
Additional sections: tumor cells on serosal surface Tumor <1 mm, no reaction
Mucinous carcinoma <1 mm Muc CA involving peritoneal cleft: pT4a

39
AJCC: T definitions
pT DefinitionTis Carcinoma in situ, intraepithelial, no
invasion of lamina propria(High grade dysplasia)
Tis Carcinoma in situ, invasion of lamina propria/ muscularis mucosa(Intramucosal adenocarcinoma)
T1 Tumor invades submucosa(Invasive adenocarcinoma)

40
Venous invasion IM carcinoma (Tis): Tumor involvement of lamina pro pria