Embed Size (px)
Citation preview

SSTI by POCUS
Miki Watanabe MD

Case 1
58M with DM2 on insulin came to ER with L leg thigh erythema x 2 days. T 37.0, HR 90, BP 100/80.L thigh erythema 5x10cm, tender and warm. WBC 12000. Choose one correct answer. 1- Cellulitis can be detected by ultrasound as subcutaneous tissue cobble stone appearance 2- Cellulitis can be detected by air in the subcutaneous tissue 3- Cellulitis imaging by bedside ultrasound is not different from normal skin tissue 4- None of the above

Case2
42 F with IVDU came to ER with rapidly worsening erythema of the L forearm. T39.0, BP110/80, HR120. L forearm showed 3x3 cm erythema, tender and warm. Choose one correct answer. 1- Skin abscess can be detected by ultrasound with STAFF appearance 2- Skin abscess by POCUS has high sensitivity>80% and specificity >80% 3- Skin abscess is difficult to differentiate by POCUS from cellulitis 4- None of the above

Case3
50M with DM1 came to ER presenting R leg worsening erythema x 1 day. T 38.8. HR 120, BP 90/50. R leg tender with minor erythema but tender to touch. WBC 25000. CRP sky high. Na 129.
Choose one correct answer.
1- Necrotizing fasciitis still cannot be detected by POCUS
2- MRI is the best imaging choice for NF
3- Lab results are of no use to detect NF
4- None of the above

SSTI US
• Fairly Easy Skills
• Great sensitivity
• Good specificity
• Differentiate Cellulitis vs Abscess
• Possible detection of Necrotizing Fasciitis

Skin Pocus Basics
• Transducer
• Anatomy
• Pathology

Transducer: Linear

Skin Anatomy

Skin Anatomy

Skin infections

SSTI by POCUS

Skin infections: Cellulitis

Cellulitis: subcutaneous edema(Cobblestoning)

Skin infections:Abscess

Abscess


Abscess - Sens 97% - Speci 83%

Skin infections

Necrotizing Fasciitis

Necrotizing fasciitis


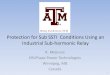
LRINEC SCORE


© 2004 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc.
2
Figure 3.
The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections *. Wong, Chin-Ho; MD, MRCS; Khin, Lay-Wai; MD, MSC; Heng, Kien-Seng; MD, FRCS; Tan, Kok-Chai; MD, FRCS; Low, Cheng-Ooi; MD, FRSC Critical Care Medicine. 32(7):1535-1541, July 2004. DOI: 10.1097/01.CCM.0000129486.35458.7D
Figure 3. Suggested clinical pathway in the management of soft tissue infections. LRINEC, Laboratory Risk Indicator for Necrotizing Fasciitis; IV, intravenous; CBC, complete blood count; CRP, C-reactive protein; MRI, magnetic resonance imaging.

© 2004 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc.
2
Table 4.

© 2004 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc.
2
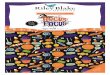
Figure 2.
The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft tissue infections *. Wong, Chin-Ho; MD, MRCS; Khin, Lay-Wai; MD, MSC; Heng, Kien-Seng; MD, FRCS; Tan, Kok-Chai; MD, FRCS; Low, Cheng-Ooi; MD, FRSC Critical Care Medicine. 32(7):1535-1541, July 2004. DOI: 10.1097/01.CCM.0000129486.35458.7D
Figure 2. Plot of probability of necrotizing fasciitis against the ascending categories of Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score. Cases of necrotizing fasciitis (n = 145) are represented by boxes and control patients are represented by crosses (n = 309). From the graph, a probability of necrotizing infections of 75% corresponds to a score of >=8.

LRINEC score <=5, - NF development <50% LRI-NEC score 6–7 - NF development 50-75% LRINEC score >=8 - NF development >75% - positive predictive value, 93.4%; 95% CI, 85.5–97.2


• Magnetic resonance imaging has a sensitivity of 93% in detecting necrotizing fasciitis.
• Computed tomography has an estimated sensitivity of 80% in detecting necrotizing fasciitis.
• In one study, sonography revealed a sensitivity of 88.2%, specificity of 93.3%, positive predictive value of 83.3%, negative predictive value of 95.4%, and accuracy of 91.9% in the diagnosis of NF


- Prospective observational study in the National Taiwan University Hospital in 1996-1998
- 62 cases with suspected NF( fever/WBC, skin infection)
POCUS Dx:
Diffuse thickening of the subcutaneous tissue
+
Fluid accumulation along the fascia(4mm)
Compaired with
Inope diagnoses + Biopsy diagnoses



STAFF
• Subcutaneous Thickening and Air
• Fascial Fluid

- 32 cases - Subcutaneous change(87.5%) - Fascia change ( 56%)

Case 1
58M with DM2 on insulin came to ER with L leg thigh erythema x 2 days. T 37.0, HR 90, BP 100/80.L thigh erythema 5x10cm, tender and warm. WBC 12000. Choose one correct answer. 1- Cellulitis can be detected by ultrasound as subcutaneous tissue cobble stone appearance 2- Cellulitis can be detected by air in the subcutaneous tissue 3- Cellulitis imaging by bedside ultrasound is not different from normal skin tissue 4- None of the above

Case 1
58M with DM2 on insulin came to ER with L leg thigh erythema x 2 days. T 37.0, HR 90, BP 100/80.L thigh erythema 5x10cm, tender and warm. WBC 12000. Choose one correct answer. 1- Cellulitis can be detected by ultrasound as subcutaneous tissue cobble stone appearance 2- Cellulitis can be detected by air in the subcutaneous tissue 3- Cellulitis imaging by bedside ultrasound is not different from normal skin tissue 4- None of the above

Case2
42 F with IVDU came to ER with rapidly worsening erythema of the L forearm. T39.0, BP110/80, HR120. L forearm showed 3x3 cm erythema, tender and warm. Choose one correct answer. 1- Skin abscess can be detected by ultrasound with STAFF appearance 2- Skin abscess by POCUS has high sensitivty>80% and specificity >80% 3- Skin abscess is difficult to differenciate by POCUS from cellulitis 4- None of the above

Case2
42 F with IVDU came to ER with rapidly worsening erythema of the L forearm. T39.0, BP110/80, HR120. L forearm showed 3x3 cm erythema, tender and warm. Choose one correct answer. 1- Skin abscess can be detected by ultrasound with STAFF appearance 2- Skin abscess by POCUS has high sensitivty>80% and specificity >80% 3- Skin abscess is difficult to differenciate by POCUS from cellulitis 4- None of the above

Case3
50M with DM1 came to ER presenting R leg worsening erythema x 1 day. T 38.8. HR 120, BP 90/50. R leg tender with minor erythema but tender to touch. WBC 25000. CRP sky high. Na 129. Choose one correct answer. 1- Necrotizing fasciitis still cannot be detected by POCUS 2- MRI is the best imaging choice for NF 3- Lab results are of no use to detect NF 4- None of the above

Case3
50M with DM1 came to ER presenting R leg worsening erythema x 1 day. T 38.8. HR 120, BP 90/50. R leg tender with minor erythema but tender to touch. WBC 25000. CRP sky high. Na 129. Choose one correct answer. 1- Necrotizing fasciitis still cannot be detected by POCUS 2- MRI is the best imaging choice for NF 3- Lab results are of no use to detect NF 4- None of the above