Embed Size (px)
Citation preview
American Journal of Medical Genetics 37:427-428 (1990)
Letter To the Editor
Sporadic Occurrence of Spondylocostal Dysplasia and Mesocardia in a Japanese Girl
To the Editor:
Most of the reported cases of spondylocostal dysplasia (SCD) are autosomal recessive [Lavy et al., 1966; Moseley and Bonforte, 1969; Cantu et al., 1971; F’ran- ceschini et al., 1974; Gellis and Feingold, 1976; Beighton and Horan, 1981; Casammassimma et al., 1981; David and Glass, 1983; Poor et al., 19831 and associated with more severe manifestations as compared to the domi- nant type [Rimoin et al., 19681. Small numbers of spo- radic cases of SCD were also reported though phe- notypes vary from mild [Ayme and Preus, 19861 to rather severe [Pochaczevsky et al., 19713. To date SCD has not been documented in Orientals.
CLINICAL REPORT Our patient was born a t term to a 26-year-old pri-
migravida mother after an uneventful pregnancy. Birth weight was 3,004 g. The pregnancy was uncomplicated; family history was negative for skeletal anomalies.
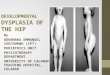
Body length of the patient had been nearly -1.5 SD of the standard of Japanese girls. At age 7,10112 years, the patient was 114.5 cm tall (height age: 6,5112 years) and she weighed 19.2 kg (weight age: 6, 2/12 years).
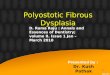
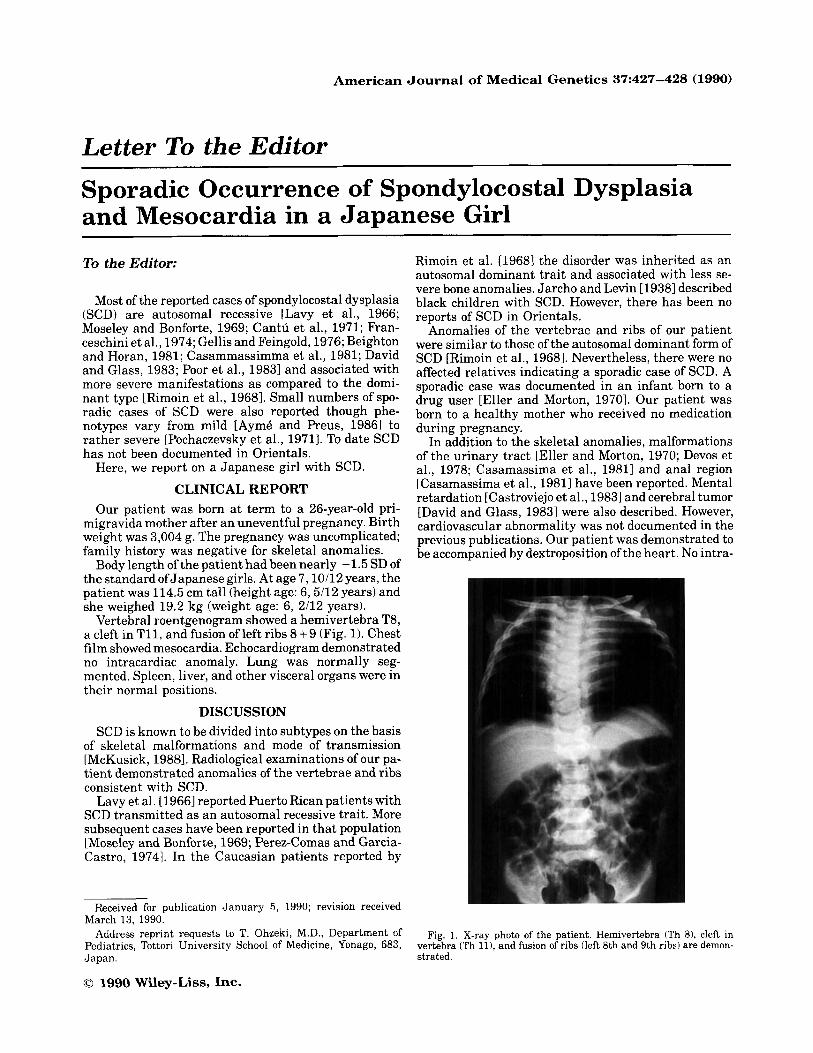
Vertebral roentgenogram showed a hemivertebra T8, a cleft in T11, and fusion of left ribs 8 + 9 (Fig. 1). Chest film showed mesocardia. Echocardiogram demonstrated no intracardiac anomaly. Lung was normally seg- mented. Spleen, liver, and other visceral organs were in their normal positions.
DISCUSSION SCD is known to be divided into subtypes on the basis
of skeletal malformations and mode of transmission [McKusick, 19881. Radiological examinations of our pa- tient demonstrated anomalies of the vertebrae and ribs consistent with SCD.
Lavy et al. [1966] reported Puerto Rican patients with SCD transmitted as an autosomal recessive trait. More subsequent cases have been reported in that population [Moseley and Bonforte, 1969; Perez-Comas and Garcia- Castro, 19741. In the Caucasian patients reported by
Here, we report on a Japanese girl with SCD.
Received for publication January 5, 1990; revision received March 13, 1990.
Address reprint requests to T. Ohzeki, M.D., Department of Pediatrics, Tottori University School of Medicine, Yonago, 683, Japan.
0 1990 Wiley-Liss, Inc.
Rimoin et al. [19681 the disorder was inherited as an autosomal dominant trait and associated with less se- vere bone anomalies. Jarcho and Levin [ 19381 described black children with SCD. However, there has been no reports of SCD in Orientals.
Anomalies of the vertebrae and ribs of our patient were similar to those of the autosomal dominant form of SCD [Rimoin et al., 19681. Nevertheless, there were no affected relatives indicating a sporadic case of SCD. A sporadic case was documented in an infant born to a drug user [Eller and Morton, 19701. Our patient was born to a healthy mother who received no medication during pregnancy.
In addition to the skeletal anomalies, malformations of the urinary tract [Eller and Morton, 1970; Devos et al., 1978; Casamassima et al., 19811 and anal region [Casamassima et al., 19811 have been reported. Mental retardation [Castroviejo et al., 19831 and cerebral tumor [David and Glass, 19831 were also described. However, cardiovascular abnormality was not documented in the previous publications. Our patient was demonstrated to be accompanied by dextroposition of the heart. No intra-
Fig. 1. X-ray photo of the patient. Hemivertebra (Th 81, cleft in vertebra (Th 111, and fusion of ribs (left 8th and 9th ribs) are demon- strated.
428 Ohzeki et al.
cardiac anomaly was present. A deformed rib cage was considered as one of the causes of the cardiac disorder though the skeleton of the patient was less severely deformed as compared to the reported cases which were not associated with an abnormal heart position.
Our patient with SCD is the first report of occurrence in Asians. Mesocardia may be a component manifesta- tion but coincidence cannot be ruled out.
REFERENCES Ayme S, Preus M (1986): Spondylocostalispondylothoracic dysostosis:
The clinical basis for prognosticating and genetic counseling. Am J Med Genet 24599-606.
Beighton P, Horan FT (1981): Spondylocostal dysostosis in South Afri- can sisters. Clin Genet 19:23-25.
CantuJM, Urrusti J,Rosales G, FbjasAI1971): Evidence for autosomal recessive inheritance of costovertebral dysplasia. Clin Genet 2:149-154.
Casamassima AC, Morton CC, Nance WE, Kodroff M, Caldwell M, Kelly T, Wolf B (1981): Spondyloco$tal dysostosis associated with anal and urogenital anomalies in a Mennonite sibship. Am J Med Genet 8:117-128.
Castroviejo IP, Rodriguez-Costa T, Castillo F (1983): Spondylo-thoracic dysplasia in three sisters. Dev Med Child Neurol 15:348-354.
David TJ, Glass A (1983): Hereditary costovertebral dysplasia with malignant cerebral tumour. J Med Genet 20:441-444.
Devos EA, Leroy JG, Braeckman JJ, Vanden Bulcke LJ, Langer LO (1978): Spondylocostal dysostosis and urinary tract anomaly: Defi- nition and review of an entity. Eur J Pediatr 128:7-15.
Eller JL, Morton JM (1970): Bizarre deformities in offspring of user of lysergic acid diethylamide. N Engl J Med 283:395-397.
Franceschini P, Gassi E, Fabris C, Bogetti G, Randaccio M (1974): The autosomal recessive form of spondylocostal dysostosis. Pediatr Ra- dlol 112:673-675.
Gellis SS, Feingold M (1976): Spondylothoracic dysplasia (costover- tebral dysplasia, Jarcho-Levin syndrome). Am J Dis Child 130513, 514.
Jarcho S, Levin PM (1938): Hereditary malformation of the vertebral bodies. Bull John Hopkins Hosp 62:216-226.
Lavy NW, Palmer CG, Merritt AD (1966): A syndrome of bizarre vertebral anomalies. J Pediatr 69:1121-1125.
McKusick VA (1988): “Mendelian Inheritance in Man. Catalogs of Autosomal Dominant, Autosomal Recessive. and X-Linked Phe- notypes.” Baltimore: Johns Hopkins Univ Press.
Moseley JE , Bonforte R J (1969): Spondylothoracic dysplasia-a syn- drome of congenital anomalies. Am J Roentgen01 106:166-169.
Perez-Comas A, Garcia-Castro JM (1974): Occipito-facial-cervico- thoracic-abdomino-digital dysplasia: Jarcho-Levin syndrome of vertebral anomalies. J Pediatr 85:388-391.
Pochaczevsky R, Ratner H, Perles D, Kassner G, Naysan P (1971): Spondylothoracic dysplasia. Radiology 98:53-58.
Poor MA, Alberti 0, Griscom NT, Driscoll SG, Holmes JB (1983): Nonskeletal malformations in one of three siblings with Jarcho- Levin syndrome of vertebral anomalies. J Pediatr 103:270-272.
Rimoin DL, Fletcher BD, McKusick VA (1968): Spondylocostal dyspla- sia. Am J Med 45:948-93.
Takehiko Ohzeki Masahiro Shiraishi Yoshihiro Matsumoto Junji Takagi Hiroko Motozumi Keiichi Hanaki Nobuo Ishitani Hiroko Matsuda-Ohtahara Hirofumi Okuda Tadataka Hoshika Yoshihiro Ogihara Kazuo Shiraki Department of Pediatrics Kichizo Yamamoto Department of Orthopedics Tottori University School of Medicine, Yonago, Japan