Embed Size (px)
Citation preview

Sponsored By:

SABCS 2011 Review:HER2-Directed Therapy in
Breast CancerChau Dang, MD
Assistant Professor of Medicine
Weill Cornell Medical College
Breast Cancer Medicine Service
Memorial Sloan-Kettering Cancer Center
January 28, 2012

Objectives• Overview on Trastuzumab• Lapatinib
– Goss et al (abstract # S4-7)
• Neratinib– Martin et al (abstract # S5-7)
• Pertuzumab– Baselga et al (abstract # S5-5)– Schneeweiss et al (abstract # S5-6)
• pCR as predictor of outcomes– Loibl et al (abstract # S5-4)

HER2-“Positive” Breast Cancer• 20-25% of invasive breast cancers• Overexpression can activate signaling• Promotes cell proliferation and survival
Hudis NEJM 2007

Studies Slamon et al,
20011
Vogel et al,
20022
Burstein et al, 20033
Marty et al, 20054
Kaufman et al, 20095
Valero et al 20116
N 469 114 54 186 207 263
Treatment AC/EC + H or T+H vs chemo
H VH D+H vs
D
Anas + H vs
Anas DCbH vsD+H
Response Rate
50% vs 32%* 35% (IHC 3+)
34% (FISH+)68% 61% vs
34%*20.3% vs 6.8%*
72% vs 72%
Median TTP
7.4 vs 4.6 mo*
3.8 mo (H at 4 mg/kg)
3.5 mo
(H at 2 mg/kg)
NR 11.7 vs 6.1 mo*
4.8 vs
2.4 mo*10.3 vs 11.1 mo
Median PFS
NR NR NR NR 4.8 vs
2.4 mo*NR
Median OS 25.1 vs 20.3 mo*
24.4 mo NR 31.2 vs 22.7 mo*
28.5 vs 23.9 mo
37.4 vs 37.1 mo
Trastuzumab in First-Line Treatment
AC, anthracycline + cyclophosphamide; Anas, anastrozole; T, paclitaxel; D, docetaxel; EC, epirubicin + cyclophosphamide; H, trastuzumab; mo, months; PFS, progression-free survival; OS, overall survival; RR, response rate; TTP, time to progression; VH, vinorelbine + trastuzumab; *statistically significant1Slamon DJ et al. N Engl J Med. 2001:344(11):783-792; 2Vogel CL et al. J Clin Oncol. 2002;20:719-726; 3Burstein HJ et al. J Clin Oncol. 2003;21(15):2889-2895; 4Marty M et al. J Clin Oncol. 2005;23(19):4265-4274; 5Kaufman B et al. J Clin Oncol. 2009;27(33):5529-5537; 6Valero V et al. J Clin Oncol. 2011;29:149-156.

6

“Other” HER Targeted Strategies
HER dimerizationinhibitors
pertuzumab
Anti-EGFRblocking
antibodies
cetuximab
Anti-ligandblocking
antibodiesTyrosinekinase
Inhibitors
neratiniblapatiniberlotinib gefitinib
Ligand- or Ab-toxin
conjugates
T-DM1Adapted from Noonberg and Benz. Drugs. 2000;59:753.

Lapatinib

Lapatinib
• Targets intracellular kinase domain of HER1 and HER2
• Reversible inhibition of HER1 and HER2 homo and heterodimer formation
• Inhibits growth in trastuzumab conditioned cell lines
1+1 2+2 1+2
Courtesy of E. Winer

Clinical Activity of Lapatinib in HER2+ MBC
ORR
Monotherapy in trastuzumab-refractory MBC1,2
4-8%
Monotherapy in trastuzumab-naive MBC3
≈24%
With chemo (capecitabine) in chemo & trastuzumab-refractory MBC4,5
24% (vs 14% with X alone)
With chemo (paclitaxel) in first-line MBC setting6
63% (vs 38% with T alone)
1Blackwell 2004 (abs 103); 2Burstein Ann Oncol 2008; 3Gomez JCO 2008; 4Geyer NEJM 2006; 5Cameron BrCancerResTreat 2008; 6Di leo JCO 2008

TEACH trial: Tykerb Evaluation After
Chemotherapy• Randomized, double-blind, placebo-controlled, phase III
trial to evaluate the effects of delayed adjuvant lapatinib monotherapy
• More than 3000 women– completed neo-adjuvant or adjuvant chemotherapy, – did not receive trastuzumab and – NED
• Randomized to lapatinib or placebo for up to 12 months or until a DFS event
• Median time from diagnosis to study entry: 3 years
Goss abs S4-7

Delayed Adjuvant Lapatinib Results
• Median follow up of 4 years
• DFS events were 13% vs. 17% in favor of lapatinib vs placebo (HR = 0.83 95% CI, 0.70 to 1.00; 2 sided p=0.053), but not statistically significant.
• No role for “delayed” lapatinib in the adjuvant setting !
• What about “upfront” lapatinib in ALTTO ?
Goss abs S4-7

•Patients with ER or PgR-positive tumors receive endocrine therapy selected accordingly to menopausal status; endocrine therapy will be started Patients with ER or PgR-positive tumors receive endocrine therapy selected accordingly to menopausal status; endocrine therapy will be started after the end of chemotherapy, will be administered concurrently with targeted therapies and will be planned for at least 5 yearsafter the end of chemotherapy, will be administered concurrently with targeted therapies and will be planned for at least 5 years• Radiotherapy if indicatedRadiotherapy if indicated
ALTTOALTTO
TH (12 wks)TH (12 wks)
H (40 wks)H (40 wks)
TL (12 wks)TL (12 wks)
L (40 wks)L (40 wks)
(L =1500 mg qd) (L =1500 mg qd)
TH (12 wks)TH (12 wks) THL (12 wks)THL (12 wks)
HL (40 wks)HL (40 wks)
(L =1000 mg qd)(L =1000 mg qd)
Washout (6 wks)Washout (6 wks)
L (34 wks)L (34 wks)
(L =1500 mg qd)(L =1500 mg qd)
Adjuvant Lapatinib and/or Trastuzumab Treatment
Optimization
Neo (adj) anthracycline-based chemo
T=paclitaxel, H=trastuzumab, L=lapatinib

Neratinib

Lapatinib vs Neratinibin HER2+ MBC
Lapatinib ORR Neratinib ORR
Monotherapy in H-refractory MBC
4-8%1,2 24%4
Monotherapy in H-naive MBC
≈24%3 56%4
1Blackwell 2004 (abs 103); 2Burstein Ann Oncol 2008; 3Gomez JCO 2008; 4 Burstein JCO 2010

Phase 2, open-label trial in HER2+ locally
advanced or metastatic BC
patients
Neratinib 240 mg/day
n = 117
L + CL 1,250 mg/day +
C 2,000 mg/m2 per day n = 116
RANDOMIZE
Study Design
Neratinib was administered orally at 240 mg/day continuously
L 1,250 mg/day was administered orally continuously;
C 2,000 mg/m2 was administered orally on D1 to 14 of each 21-day cycle
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.
Martin et al, SABC 2011 abstract # S5-7
1○- PFS2○ - ORR, CBR, OS, Safety G 3/4 Diarrhea and PPE

Key Eligibility Criteria• Women with HER2+ locally advanced or metastatic BC not
amenable to curative therapy
• Disease progression on or following 1 to 2 prior trastuzumab-based regimens
• Prior treatment with a taxane regimen
• Prior anthracycline treatments at or below the maximum cumulative dose of 400 mg/m2 for doxorubicin, 800 mg/m2 for epirubicin, or equivalent dose for other anthracycline derivatives
• Measurable disease (≥1 measurable lesion), as defined by Response Evaluation Criteria in Solid Tumors (RECIST)
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

Baseline Characteristics
CharacteristicNeratinib(n = 117)
L + C(n = 116)
Median age (range), y 52 (28–79) 56 (30–79)ER–positive, %b 44 40PR–positive, %c 27 28No. of prior anti-cancer regimens, % 1 14 14 2 33 33 ≥3 53 53Prior trastuzumab therapy, % Adjuvant/neoadjuvant settings 20 32 Metastatic setting 79 68
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

0 305 10 15 20 250
10203040506070809010
0
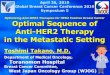
PFS: ITT Population
n Median PFS 95% CI P valueNeratinib 117 4.5 mo 3.1–5.7 mo
0.231L + C 116 6.8 mo 5.9–8.2 moL, lapatinib; C, capecitabine; PFS, progression-free survival; CI, confidence interval.
Time since randomization (mo)
Pro
babi
lity
of P
FS
(%
)NeratinibL + C
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.
Non-inferiority of neratinib vsL+C could not be demonstrated.

010203040506070809010
0
0 5 10 15 20 25 30
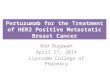
Overall Survival: ITT Population
n Median OS 95% CI P valueNeratinib 117 19.7 mo 18.2 mo–NE
0.280L + C 116 23.6 mo 18.0 mo–NEL, lapatinib; C, capecitabine; OS, overall survival; CI, confidence interval; NE, not estimable.
Time since randomization (mo)
Pro
babi
lity
of O
S (
%)
NeratinibL + C
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

Best Overall Response: ITT
NeratinibN = 117
L + CN = 116
CR 2% 4%
PR 27% 36%
SD > 24 wks 15% 23%
SD < 24 wks 29% 24%
POD 17% 7%
Unknown/missing 9% 5%
L=lapatinib, C=capecitabine
The ORR was 40% in L+C arm vs 29% in neratinib arm.The CBR was 63% in L+C arm vs 44% in neratinib arm.

Selected Treatment-related AEs (All Grades)
Neratinib (n = 116)
L + C (n = 115)
Adverse event, %
Diarrhea
85%
(28% G 3/4)
68%
(10% G 3/4)
PPE
5%
(0% G 3/4)
65%
(14% G 3/4)
Nausea 35% 38%Vomiting 24% 17%Rash 19% 34%Fatigue 16% 23%Hyperbilirubinemia 1% 23%Increased ALT 7% 13%Neutropenia 5% 12% There was a low incidence of cardiac events in both treatment arms:
neratinib, 7%; L + C, 6%
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.
Diarrhea was transient and manageable.

Conclusions• Neratinib did not demonstrate non-inferiority for PFS
against L+C.
• Med PFS was numerically (not statistically) superior with L+C (6.8 mo vs 4.5 mo).
• Diarrhea was the most frequently reported AE.
• The ORR of neratinib in heavily pretreated patients was 29%, consistent with results from the preceding single-arm trial.1
• Continued development of neratinib as monotherapy and in combination with other agents for treatment of recurrent HER2+ BC ?
1. Burstein HJ, et al. J Clin Oncol. 2010;28(8):1301-1307.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6–10, 2011
This presentation is the intellectual property of the authors/presenter. Contact them at mmartin@geicamorg for permission to reprint and/or distribute.

Pertuzumab

HER2-Targeted Therapy with Pertuzumab
• Monoclonal antibody and pan-HER inhibitor
• Binds to a distinct epitope on the HER2 extracellular domain
• Prevents dimerization
Trastuzumab Pertuzumab

Pertuzumab Activity
1. Baselga, JCO 2010; 2. Cortés, ASCO 2009 Abst # 1022
With trastuzumabN= 661
Monotherapy N= 292
% %
Best Objective Response
CR 8% 0%
PR 17% 7%
SD 6 months
26% 4%
ORR 24% 7%
Clinical Benefit Rate
50% 11%

Pertuzumab ActivityWith
trastuzumabN= 661
Monotherapy N= 292
Trastuzumab added back in
N=142
% % %
Best Objective Response
CR 8% 0%
PR 17% 7% 14%
SD 6 months
26% 4%
ORR 24% 7% 14%
Clinical Benefit Rate
50% 11%
1. Baselga, JCO 2010; 2. Cortés, ASCO 2009 Abst # 1022

CLEOPATRACLEOPATRA: CLinical Evaluation Of
Pertuzumab And TRAstuzumab

Eligibility Criteria
• Centrally confirmed HER2+ (IHC 3+ and/or FISH > 2.0)• Locally recurrent, un-resectable, or MBC• Measurable and/or non-measurable• 1 prior hormone Rx for MBC allowed• Prior neoadj/adj chemo and trastuzumab allowed if DFI >
12 mo• LVEF > 50%• No h/o CHF or LVEF < 50% during/after prior
trastuzumab

Patient CharacteristicsPlacebo +
trastuzumab + docetaxel(n = 406)
Pertuzumab + trastuzumab +
docetaxel(n = 402)
Median age, years 54y 54y
ER- and/or PR-positive
199 (49%) 189 (47%)
Prior (neo)adjuvant chemotherapy
192 (47%) 184 (46%)
Components of neoadj/adj therapy Anthracycline Hormones Taxane Trastuzumab
164 (40%)97 (24%)94 (23%)41 (10%)
150 (37%)106 (26%)91 (23%)47 (12%)

Baselga abs #S5-5

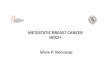
PFS in predefined subgroups

Baselga abs #S5-5

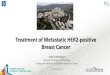
Data immature but
Baselga abs #S5-5

Grade 3/4 Adverse Events(incidence > 5%)
Adverse Events Placebo + Trastuzumab +
DoceN=397
Pertuzumab + Trastuzumab +
DoceN=407
Neutropenia 182 (45.8%) 199 (48.9%)
Febrile neutropenia 30 (7.6%) 56 (13.8%)
Leukopenia 58 (14.6%) 50 (12.3%)
Diarrhea 20 (5.0%) 32 (7.9%)
G 3/4 diarrhea was low !

Cardiac Safety
Placebo + Trastuzumab + Doce
Pertuzumab + Trastuzumab + Doce
Investigator-assessedsymptomatic LVSD*
1.8% 1.0%
Independently adjudicatedsymptomatic LVSD*
1.0% 1.0%
Decline in LVEF to < 50% and by > 10% from baseline
6.6% 3.8%
*LVSD=left ventricular systolic dysfunction, defined as NYHA class III/IV

Conclusions• CLEOPATRA met its primary endpoint w/ a statistically
significant PFS improvement from 12.4 to 18.5 months w/ addition of pertuzumab (HR 0.62, p < 0.0001).
• OS data immature
• Pertuzumab well tolerated
• No increased cardiac toxicity
• May be practice changing !

Questions
• Safe in combination with other chemotherapy foundations?
• Adjuvant/neoadjuvant studies ?
• Continuation beyond progression ?

MSKCC IRB# 10-142THP Schema
Accrual Goal = 69 patients
♥ ♥ every 4 cycles………………….. TNI, BNP, NRG-1ß every 2 cycles…………………………
q week ……………………………
q 3 weeks………………………….
q 3 weeks………………………….
Paclitaxel at 80 mg/m2
Pertuzumab at 840mg load → 420 mg q 3 w
Trastuzumab at 8 mg/kg load → 6 mg/kg q 3 w
N = 69HER2 +0-1 prior RxTissue bx optional1° endpoint=6 mo PFS
♥ ECHO w/strain imaging
PI: Dang

APHINITY: Adjuvant PertuzumabAnthracycline-Based
S R
FOLLOWUP
10yrs
T x 3-4AC/EC x 4 orFEC/FEC x 3-4
Trastuzumab q 3 wks x 52 wks
Pertuzumab q 3 wks x 52 wks
AC/EC x 4 orFEC/FEC x 3-4
T x 3-4
Trastuzumab q 3 wks x 52 wks
Placebo q 3 wks x 52 wks
SURGERY
RANDOMIZE
CentrallyConfirm HER2
Randomize w/i 7 wks of surgeryStart w/i 1 wk of randomization
Breast/chest RT and endocrine Rx as appropriate after chemo completion

APHINITY: Adjuvant PertuzumabNon-Anthracycline Based
S R
FOLLOWUP
10yrs
TC x 6
Trastuzumab q 3 wks x 52 wks
Pertuzumab q 3 wks x 52 wks
TC x 6
Trastuzumab q 3 wks x 52 wks
Placebo q 3 wks x 52 wks
SURGERY
RANDOMIZE
CentrallyConfirm HER2
Randomize w/i 7 wks of surgeryStart w/i 1 wk of randomization
Breast/chest RT and endocrine Rx as appropriate after chemo completion

Can HER2-targeted antibody therapies be administered
safely with anthracyclines?

TRYPHAENA

Study Endpoints• Primary endpoint:
– Cardiac safety• Symptomatic LVSD (grade ≥3)• LVEF declines (≥10 percentage points and below
50%)• Secondary endpoints:
– Toxicity
– pCR
– Clinical response rate
– Rate of BCS
– DFS, OS
– Biomarker evaluation
Schneeweiss abs #S5-6

Eligibility Criteria
• Centrally confirmed HER2-positive locally advanced, inflammatory, or early-stage breast cancer
• Primary tumor ≥2 cm• Baseline LVEF ≥55%• ECOG PS 0 or 1• No previous anticancer therapy or radiotherapy
for any malignancy• Adequate bone marrow, liver, and renal function
Schneeweiss abs #S5-6

Baseline CharacteristicsFEC/HP →THP
N=72FEC →THP
N=75TCHPN=76
Med age, yrs (range) 49 (27-77) 49 (24-75) 50 (30-81)
ECOG 0 65 (91.5%) 66 (88.0%) 67 (88.2%)
ECOG 1 6 (8.5%) 9 (12.0%) 9 (11.8%)
ER and/or PR + 39 (53.4%) 35 (46.7%) 40 (51.9%)
ER and/or PR- 34 (46.6%) 40 (53.3%) 36 (48.1%)
Disease Type
Operable 53 (72.6%) 54 (72.0%) 49 (63.6%)
LABC 15 (20.5%) 17 (22.7%) 24 (31.2%)
IBC 5 (6.8%) 4 (5.3%) 4 (5.2%)
HER2 IHC 0 and 1+ 1 (1.4%) 0 (0.0%) 0 (0.0%)
HER2 IHC 2+ 5 (6.8%) 1 (1.3%) 2 (2.6%)
HER2 IHC 3+ 67 (91.8%) 74 (98.7%) 75 (97.4%)
HER2 FISH + 69 (94.5%) 69 (92.0%) 73 (94.8%)
HER2 FISH- 0 (0.0%) 1 (1.3%) 2 (2.6%)
HER2 unknown 4 (5.5%) 5 (6.7%) 2 (2.6%)

Schneeweiss abs #S5-6

Other Notable G 3/4 AEs
Adverse events
FEC/HP →THPN=72
FEC →THPN=75
TCHPN=76
Neutropenia 34 (47.2%) 32 (42.7%) 35 (46.1%)
Febrile neutropenia
13 (18.1%) 7 (9.3%) 13 (17.1%)
Leukopenia 14 (19.4%) 9 (12.0%) 9 (11.8%)
Diarrhea 3 (4.2%) 4 (5.3%) 9 (11.8%)


Breast Conserving Surgery When Mastectomy Was Planned*
FEC/HP →THPN=46
FEC →THPN=36
TCHPN=37
Achieved(95% CI)
10 (21.7%)(10.9-36.4)
6 (16.7%)(6.4-32.8)
10 (27.0%)(13.8-44.1)
Not Achieved 36 (78.3%) 30 (83.3%) 27 (73.0%)
* Patients in ITT population w/ T2-3 tumors for whom mastectomy was planned.

Conclusions• Low incidence of symptomatic/asymptomatic LVSD across
all arms:– Concurrent admin of HP w/ Epi resulted in similar cardiac
tolerability compared with sequential admin or the anthracycline-free regimen
• Neutropenia, FN, leukopenia, and diarrhea were the most frequent G 3/4 AEs across all arms.
• High pCR rates (57- 66%) w/ HP, regardless of chemotherapy chosen
• TRYPHAENA supports ongoing APHINITY study, a Phase III trial to evaluate HP + standard chemo in adjuvant setting.
Schneeweiss abs #S5-6

Comparison of OS according to pCR in Pts w/ HER2+ BCA
Receiving Neoadjuvant Chemo w/ and w/o Trastuzumab Compared
w/ Pts w/ HER2- Tumors
Loibl et al for GBG and AGO-B Study groups

pCR in HER2 + BCA
• pCR is a surrogate for DFS and OS in pts w/ HER2+ BCA treated w/ neoadjuvant chemo w/ or w/o trastuzumab.1
• Pts w/ pCR after neoadjuvant chemo + trastuzumab have excellent DFS and OS.2
1. Gianni, Lancet 2010; 2. Untch, JCO 2011


Objectives
• Define 3 subgroups:– HER2+ w/ trastuzumab– HER2+ w/o trastuzumab– HER2-
• Compare DDFS and OS in these subgroups– pCR vs no pCR– Hormone receptor + vs -tumors


Patients’ Characteristics
Age 49 (22-81) yrs
cT1-3 87%
cN+ 53%
IDC 82%
Grade 3 40%
Hormone Receptor + 66%
HER2- 70%

pCR > No pCR
• DDFS and OS were better in pCR vs no pCR groups in all 3 subgroups:
– HER2+ w/ tras– HER2+ w/o tras– HER2-

Loibl abs #S5-4



Author’s Conclusions• HER2+ pts w/ tras + chemo had higher pCR.
• DDFS and OS was better in pCR group than no pCR group in all 3 subgroups (HER2+ w/ tras, HER2+ w/o tras, HER2-).
• In pCR pts, OS was better in HER2+ pts w/ tras than HER2+ pts w/o tras.
• In hormone receptor- group, HER2+ pts w/ tras have better outcomes than HER2+ w/o tras and HER2- groups. Trastuzumab is effective !
• pCR can be surrogate marker for HER2+ disease.

Summary• No role for “delayed” adjuvant lapatinib
– ALTTO may define role of lapatinib ?
• Neratinib did not demonstrate non-inferiority for PFS against L+C. – Main toxicity was diarrhea.
• Pertuzumab added to standard docetaxel + trastuzumab improves PFS ! – Maybe new standard of care !
– Adjuvant study APHINITY open !

Summary
• No increased cardiac toxicity when HP given concurrently w/ epi-taxane Rx and carbo-taxane Rx.– However, concurrent anthracycline with trastuzumab
or pertuzumab should not be given outside of clinical trial.
• What to do for those w/ no PCR?– Need trials designed to assess utility of novel or
optimal Rx for those w/o pCR

Thank You !

Sponsored By: