Embed Size (px)
Citation preview
1
HER2 in Breast CancerHistory and Future Directions
Sandra M. Swain, M.D.
Director, Washington Cancer Institute
Washington Hospital Center
Professor of Medicine
Georgetown University
Washington DC
Outline
• History
• EGFR/HER2 signaling pathway
• HER2 as a target for anticancer therapy
• Studies targeting HER2
• Metastatic
• Neoadjuvant
• Key messages
2
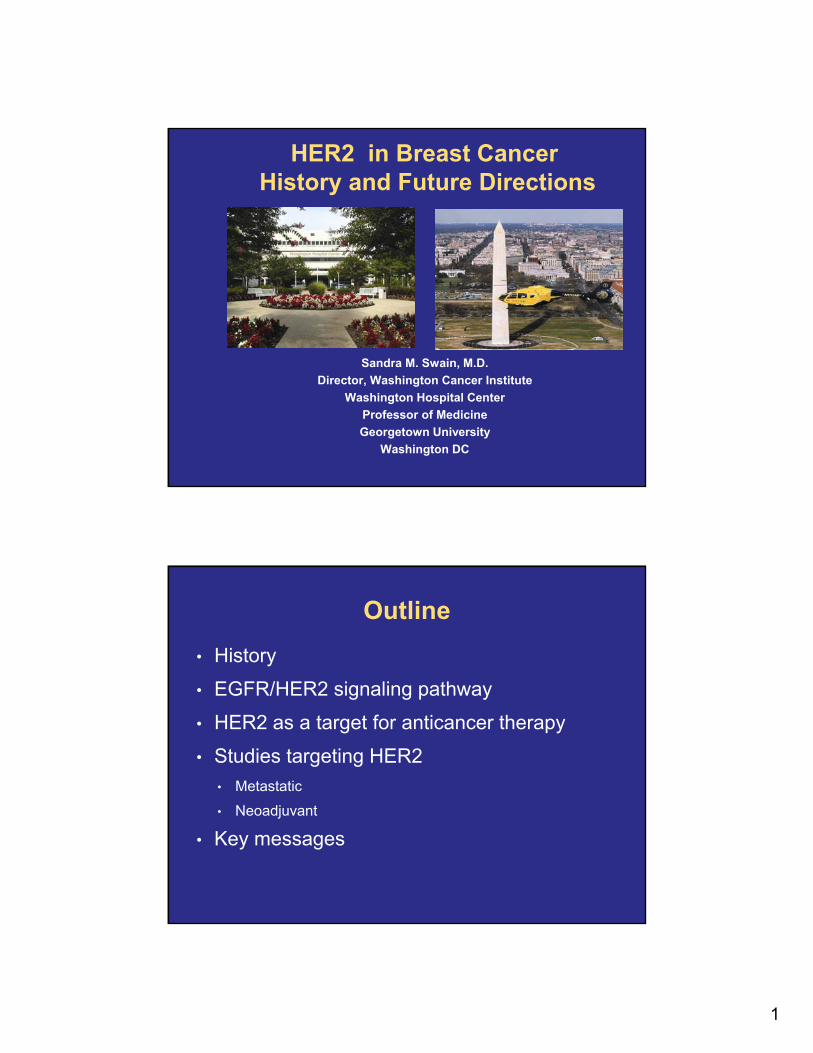
Milestones of Her2/anti-Her2 therapies in BC
EGFR discovery
Cohen
neu oncogene discovery Weinberg
EGFR MoAb inhibited growth
MendelsohnFDA approves
trastuzumab in adjuvant setting
1982 19851978 1984 1998 2006 2007 2010
Her2 amplification in breast cancer
Aaronson
FDA approves single agent trastuzumab for 2nd line and in combination with paclitaxel for 1st line MBC
FDA approves lapatinib + letrozole
for MBC
FDA approves lapatinib+ capecitabine for MBC
1987
Amplification of Her2/neu correlates with shorter survival
Slamon
MBC : metastatic breast cancerMoAb : monoclonal antibody
Her2 cloned Ullrich and Coussens
1983
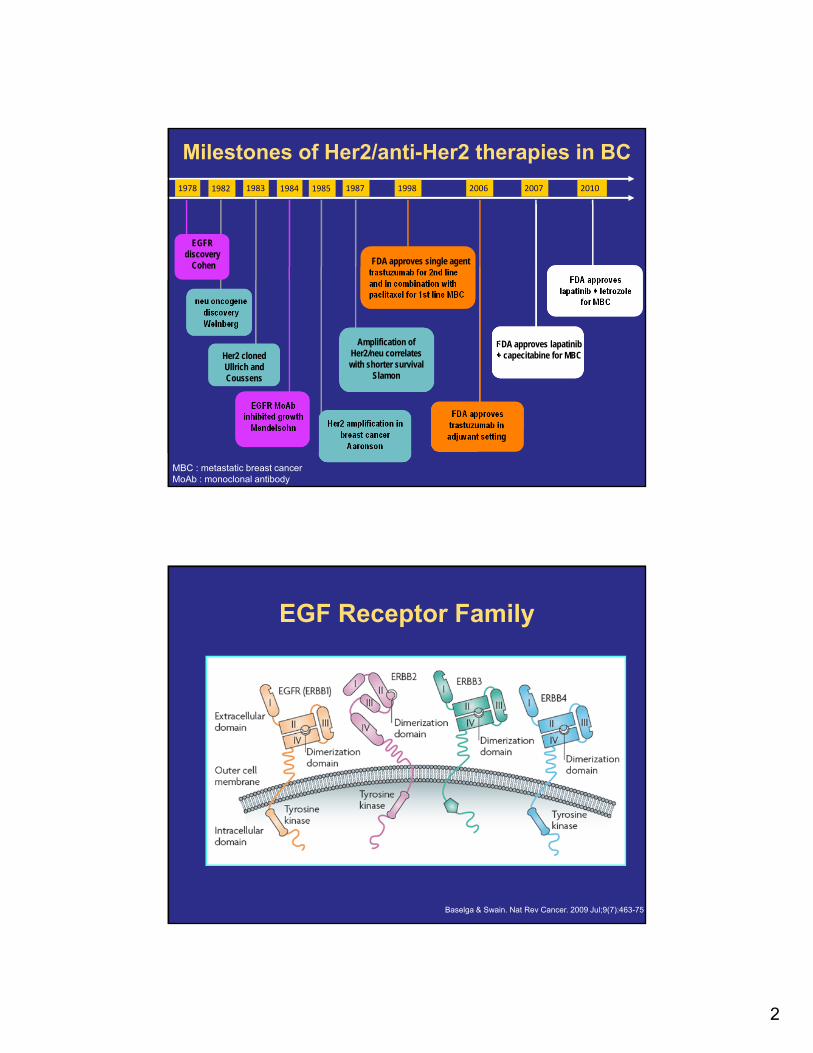
EGF Receptor Family
Baselga & Swain. Nat Rev Cancer. 2009 Jul;9(7):463-75
3
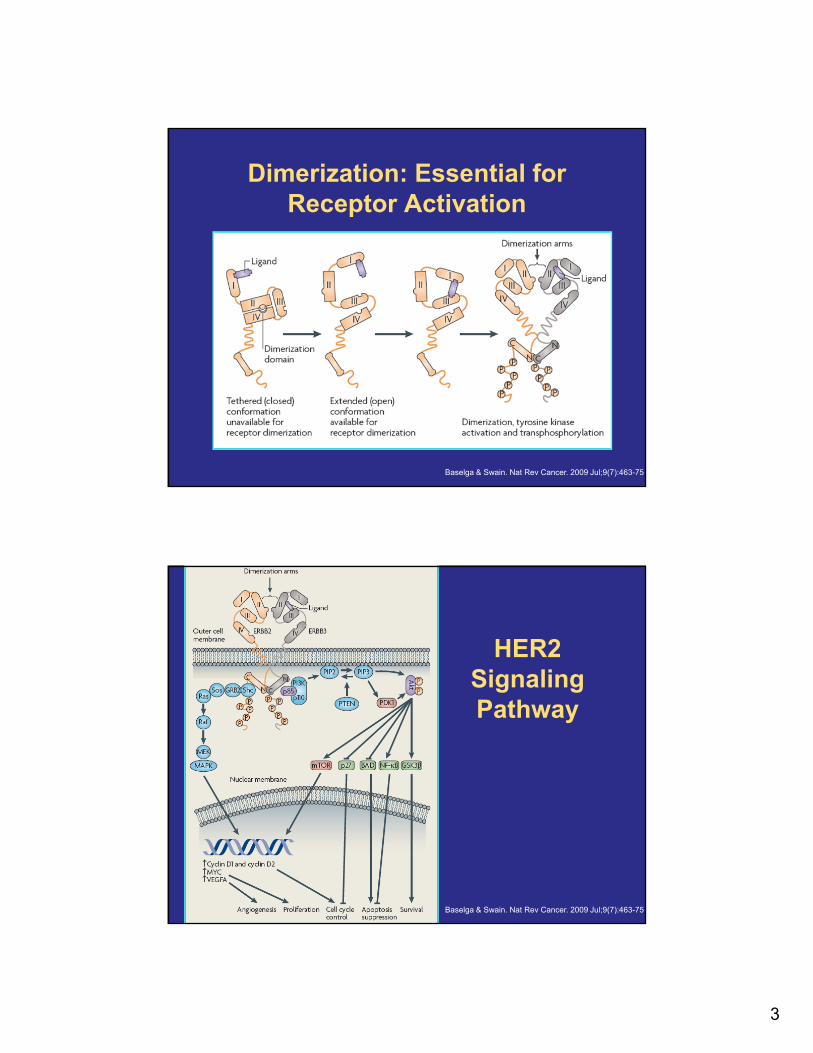
Dimerization: Essential for Receptor Activation
Baselga & Swain. Nat Rev Cancer. 2009 Jul;9(7):463-75
HER2 SignalingPathway
Baselga & Swain. Nat Rev Cancer. 2009 Jul;9(7):463-75
4
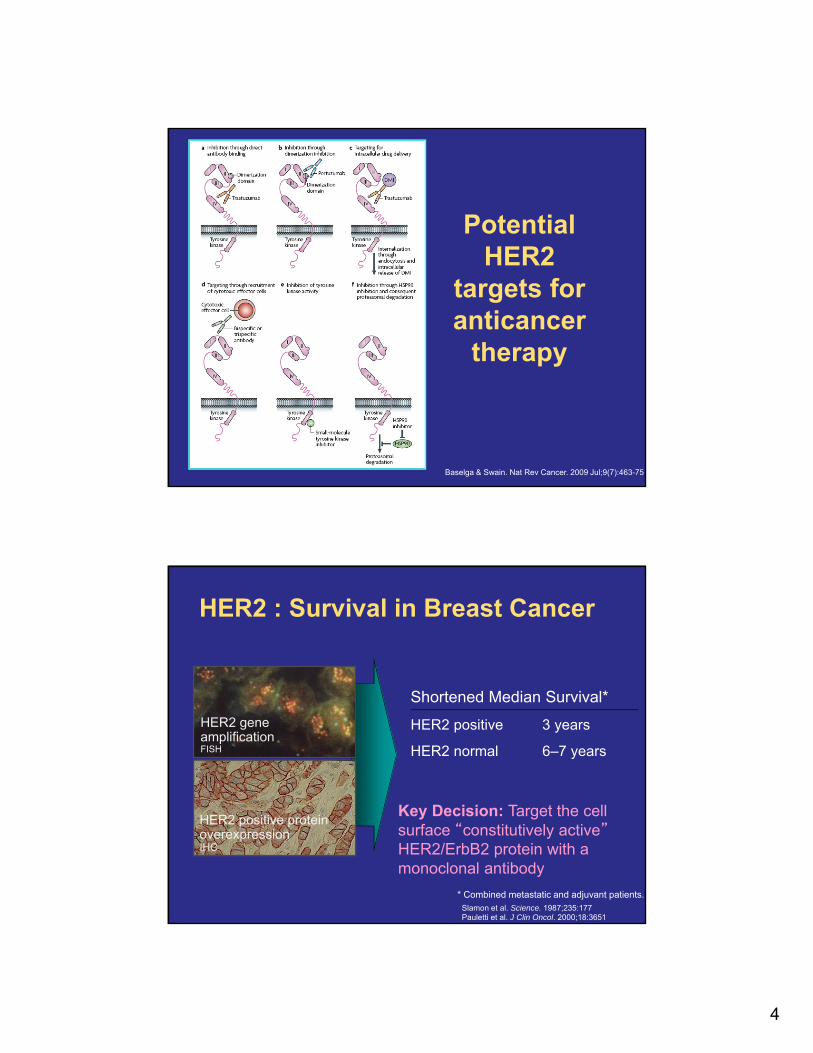
Potential HER2
targets for anticancer
therapy
Baselga & Swain. Nat Rev Cancer. 2009 Jul;9(7):463-75
* Combined metastatic and adjuvant patients.Slamon et al. Science. 1987;235:177Pauletti et al. J Clin Oncol. 2000;18:3651
Shortened Median Survival*
HER2 positive 3 years
HER2 normal 6–7 years
HER2 positive protein overexpressionIHC
HER2 : Survival in Breast Cancer
HER2 geneamplificationFISH
Key Decision: Target the cell surface “constitutively active”HER2/ErbB2 protein with a monoclonal antibody
5
HER2+ MBC• Occurs in 20%–25% of invasive breast carcinomas
• First-line agents
• Trastuzumab with
• Paclitaxel ± carboplatin
• Docetaxel
• Vinorelbine
• Second-line agents
• Lapatinib + capecitabine
• Trastuzumab + other first-line agents
• Trastuzumab + capecitabine
• Trastuzumab + lapatinib (without cytotoxic therapy)Hudis N Engl J Med. 2007 Jul 5;357(1):39-51.NCCN 2011 V.2
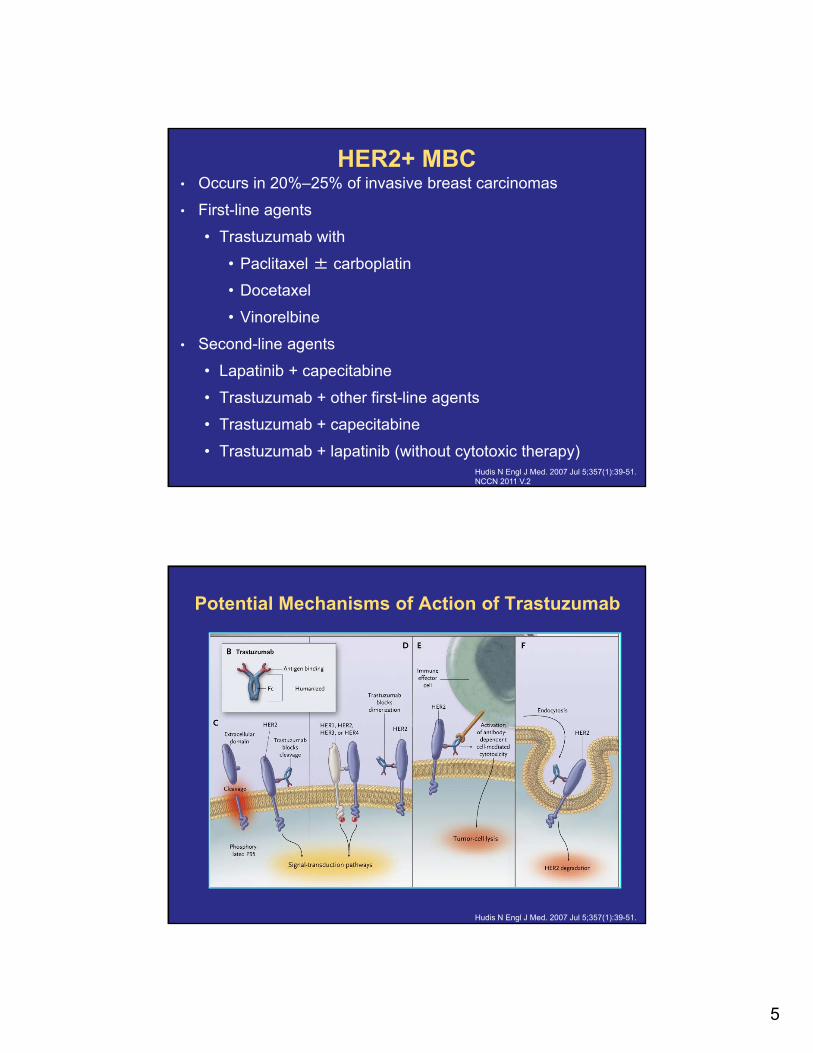
Potential Mechanisms of Action of Trastuzumab
Hudis N Engl J Med. 2007 Jul 5;357(1):39-51.
6
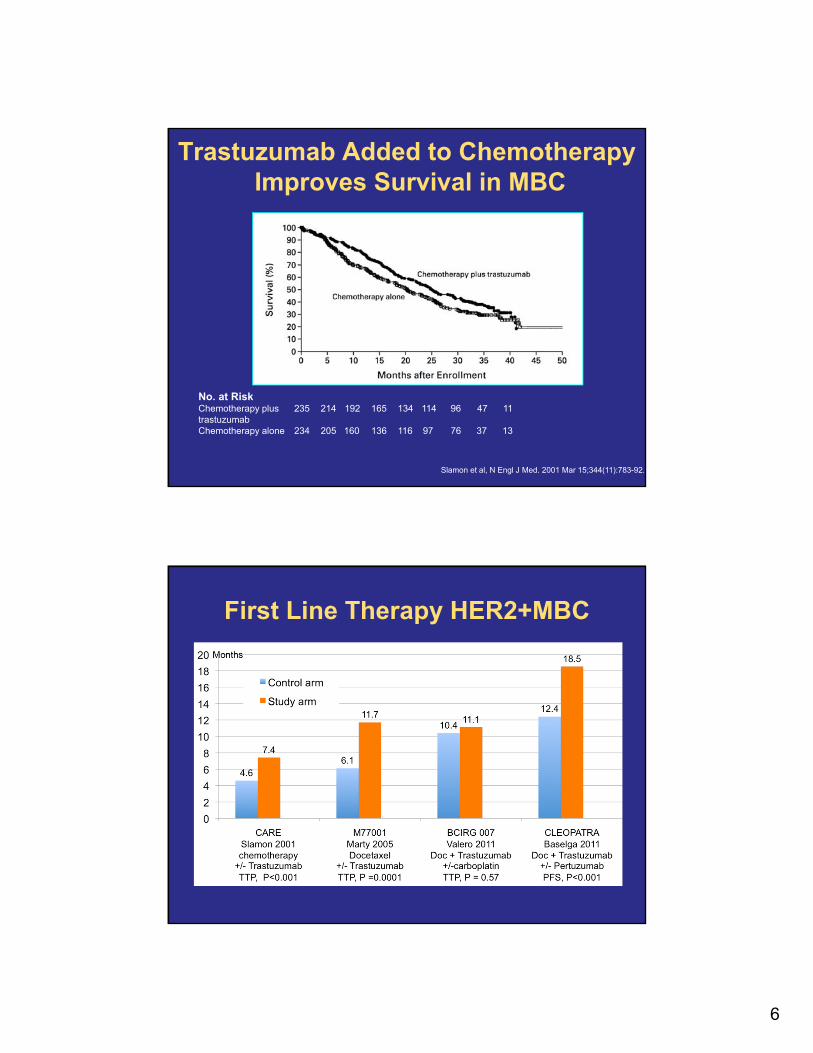
Trastuzumab Added to ChemotherapyImproves Survival in MBC
Slamon et al, N Engl J Med. 2001 Mar 15;344(11):783-92.
No. at RiskChemotherapy plus 235 214 192 165 134 114 96 47 11trastuzumabChemotherapy alone 234 205 160 136 116 97 76 37 13
First Line Therapy HER2+MBC
7
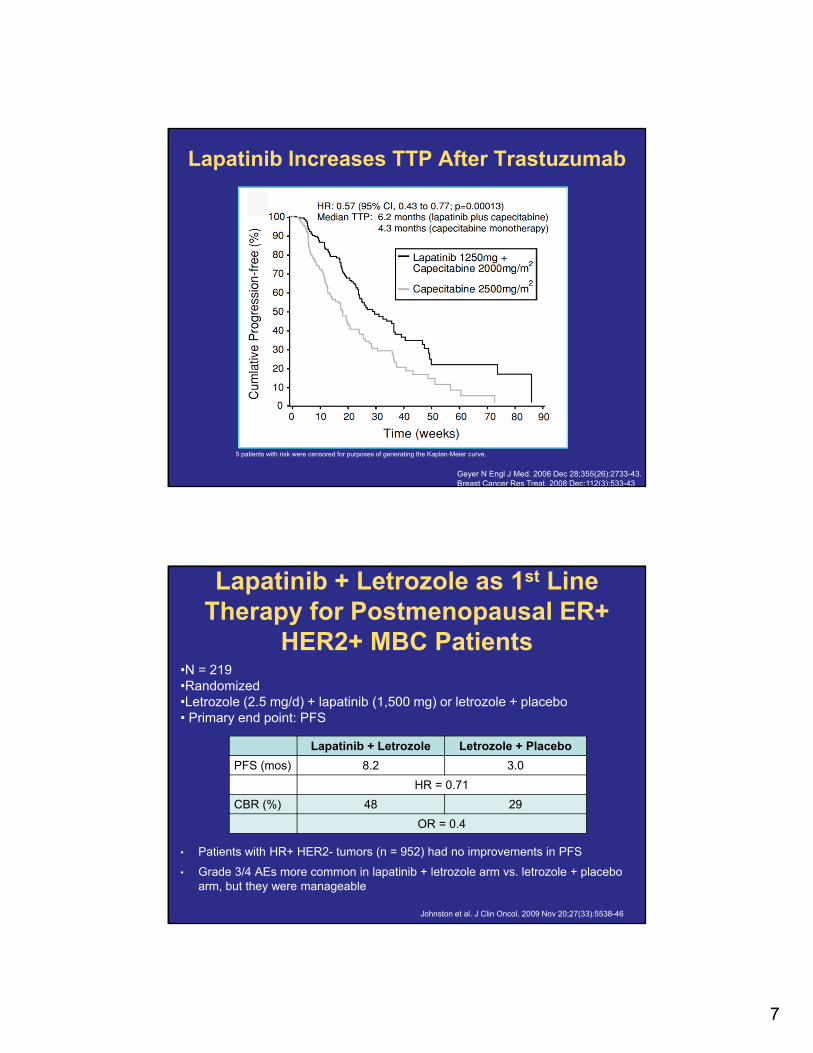
Lapatinib Increases TTP After Trastuzumab
5 patients with risk were censored for purposes of generating the Kaplan-Meier curve.
Geyer N Engl J Med. 2006 Dec 28;355(26):2733-43.Breast Cancer Res Treat. 2008 Dec;112(3):533-43
Lapatinib + Letrozole as 1st Line Therapy for Postmenopausal ER+
HER2+ MBC Patients
• Patients with HR+ HER2- tumors (n = 952) had no improvements in PFS
• Grade 3/4 AEs more common in lapatinib + letrozole arm vs. letrozole + placebo arm, but they were manageable
Lapatinib + Letrozole Letrozole + Placebo
PFS (mos) 8.2 3.0
HR = 0.71
CBR (%) 48 29
OR = 0.4
Johnston et al. J Clin Oncol. 2009 Nov 20;27(33):5538-46
•N = 219•Randomized •Letrozole (2.5 mg/d) + lapatinib (1,500 mg) or letrozole + placebo• Primary end point: PFS
8
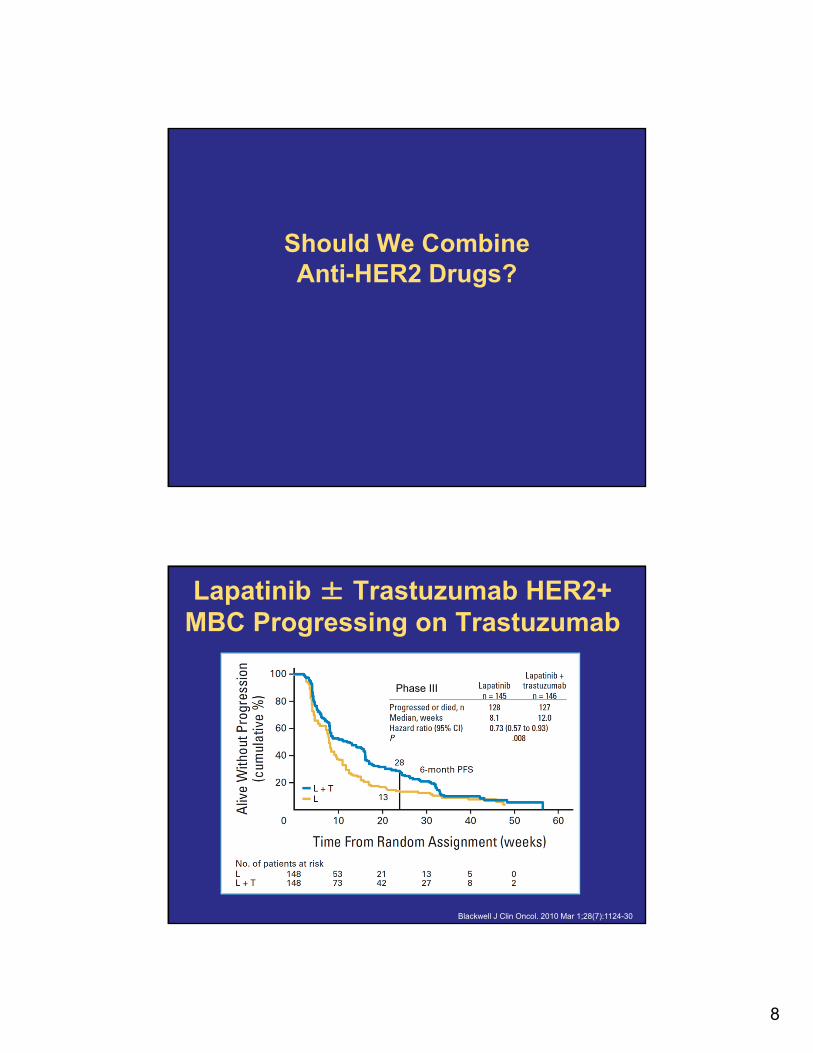
Should We Combine Anti-HER2 Drugs?
Blackwell J Clin Oncol. 2010 Mar 1;28(7):1124-30
Lapatinib ± Trastuzumab HER2+ MBC Progressing on Trastuzumab
Phase III
9
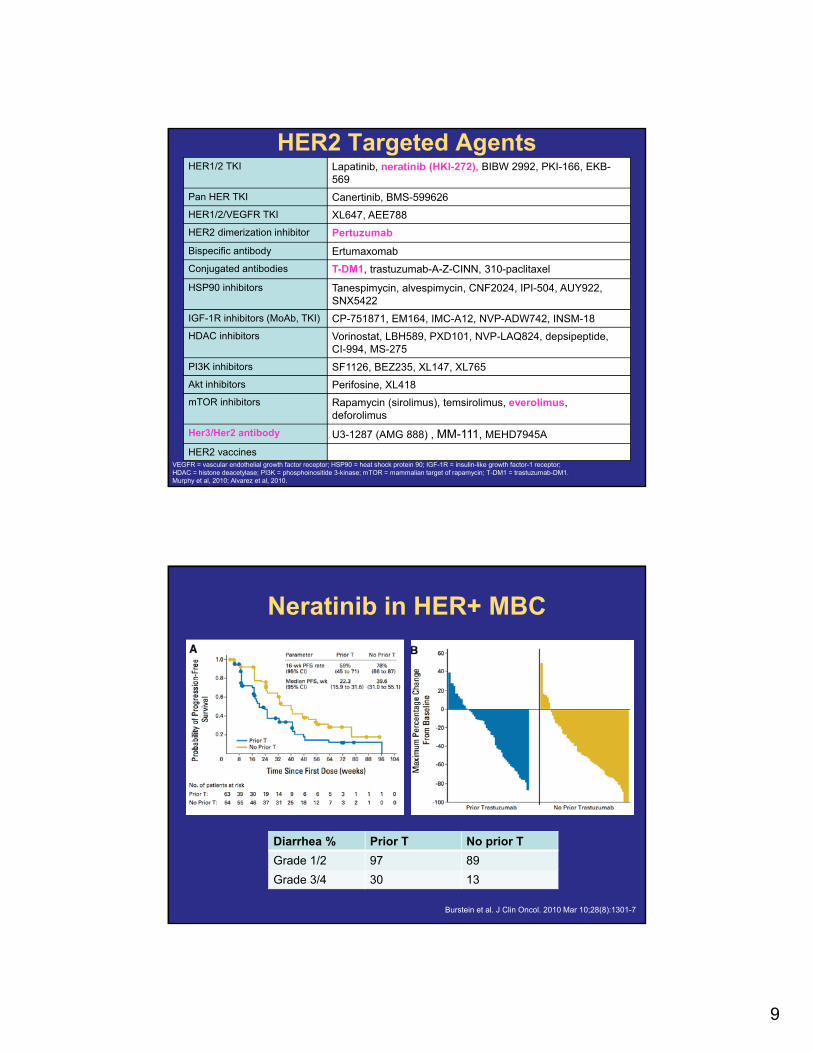
HER2 Targeted Agents
VEGFR = vascular endothelial growth factor receptor; HSP90 = heat shock protein 90; IGF-1R = insulin-like growth factor-1 receptor; HDAC = histone deacetylase; PI3K = phosphoinositide 3-kinase; mTOR = mammalian target of rapamycin; T-DM1 = trastuzumab-DM1.Murphy et al, 2010; Alvarez et al, 2010.
HER1/2 TKI Lapatinib, neratinib (HKI-272), BIBW 2992, PKI-166, EKB-569
Pan HER TKI Canertinib, BMS-599626
HER1/2/VEGFR TKI XL647, AEE788
HER2 dimerization inhibitor Pertuzumab
Bispecific antibody Ertumaxomab
Conjugated antibodies T-DM1, trastuzumab-A-Z-CINN, 310-paclitaxel
HSP90 inhibitors Tanespimycin, alvespimycin, CNF2024, IPI-504, AUY922, SNX5422
IGF-1R inhibitors (MoAb, TKI) CP-751871, EM164, IMC-A12, NVP-ADW742, INSM-18
HDAC inhibitors Vorinostat, LBH589, PXD101, NVP-LAQ824, depsipeptide, CI-994, MS-275
PI3K inhibitors SF1126, BEZ235, XL147, XL765
Akt inhibitors Perifosine, XL418
mTOR inhibitors Rapamycin (sirolimus), temsirolimus, everolimus, deforolimus
Her3/Her2 antibody U3-1287 (AMG 888) , MM-111, MEHD7945A
HER2 vaccines
Neratinib in HER+ MBC
Burstein et al. J Clin Oncol. 2010 Mar 10;28(8):1301-7
Diarrhea % Prior T No prior T
Grade 1/2 97 89
Grade 3/4 30 13
10
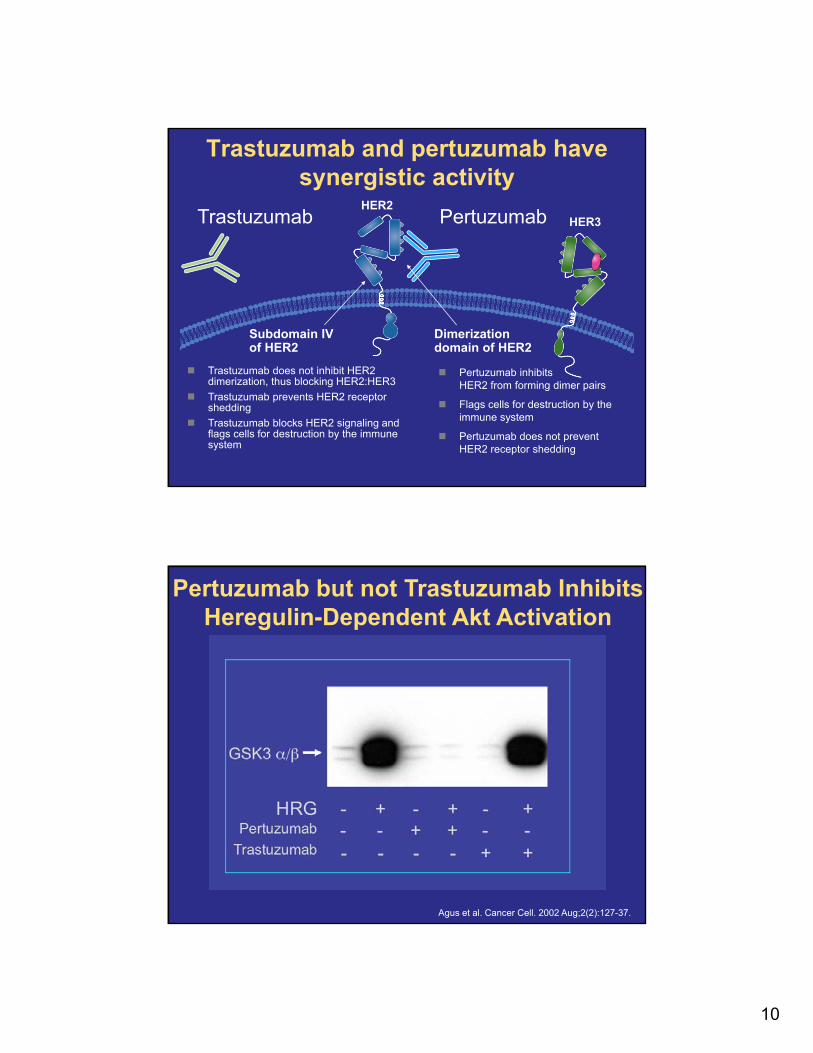
Trastuzumab and pertuzumab have synergistic activity
HER2Trastuzumab Pertuzumab
Subdomain IV of HER2
Trastuzumab does not inhibit HER2 dimerization, thus blocking HER2:HER3
Trastuzumab prevents HER2 receptor shedding
Trastuzumab blocks HER2 signaling and flags cells for destruction by the immune system
Pertuzumab inhibits HER2 from forming dimer pairs
Flags cells for destruction by the immune system
Pertuzumab does not prevent HER2 receptor shedding
Dimerization domain of HER2
HER3
Pertuzumab but not Trastuzumab Inhibits Heregulin-Dependent Akt Activation
Agus et al. Cancer Cell. 2002 Aug;2(2):127-37.
11
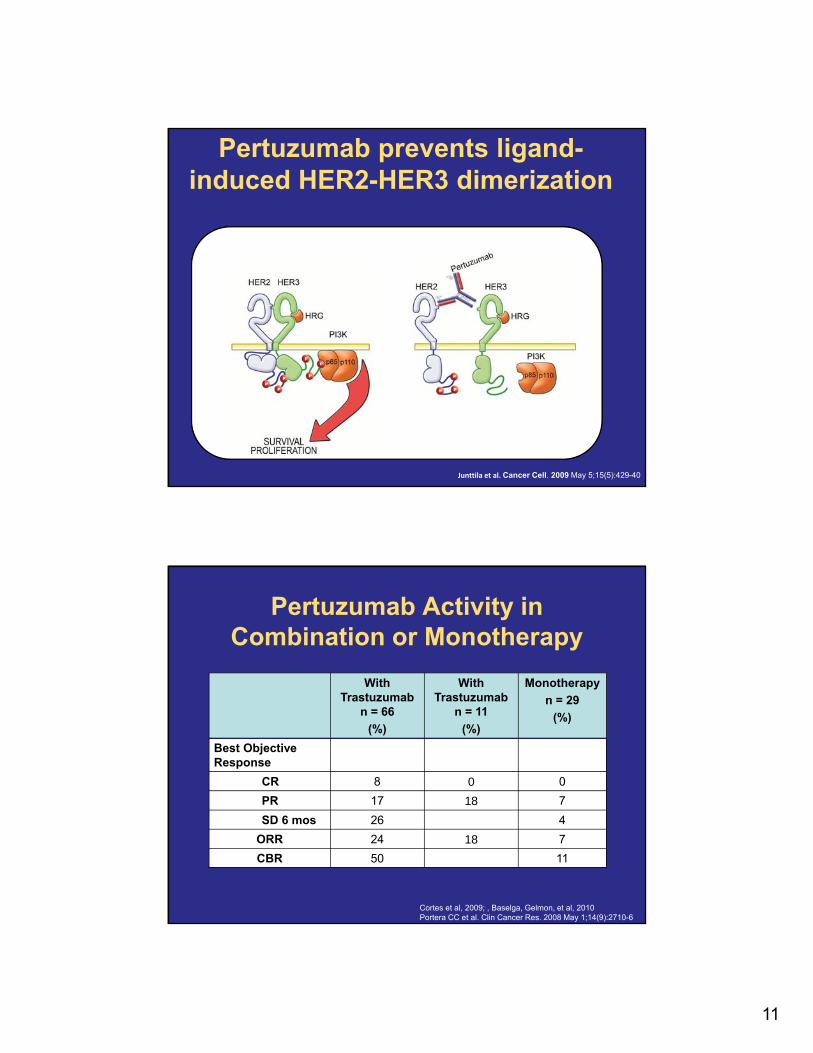
Pertuzumab prevents ligand-induced HER2-HER3 dimerization
Junttila et al. Cancer Cell. 2009 May 5;15(5):429-40
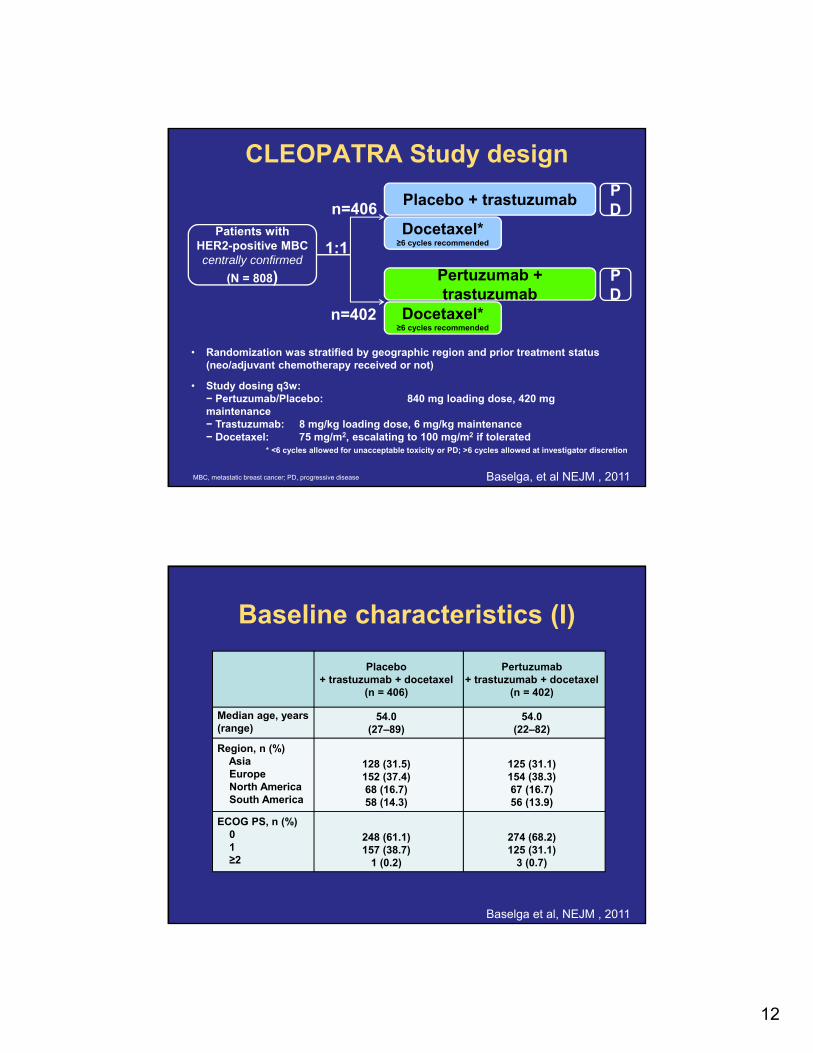
Pertuzumab Activity in Combination or Monotherapy
With Trastuzumab
n = 66
(%)
With Trastuzumab
n = 11
(%)
Monotherapy
n = 29
(%)
Best Objective Response
CR 8 0 0
PR 17 18 7
SD 6 mos 26 4
ORR 24 18 7
CBR 50 11
Cortes et al, 2009; , Baselga, Gelmon, et al, 2010Portera CC et al. Clin Cancer Res. 2008 May 1;14(9):2710-6
12
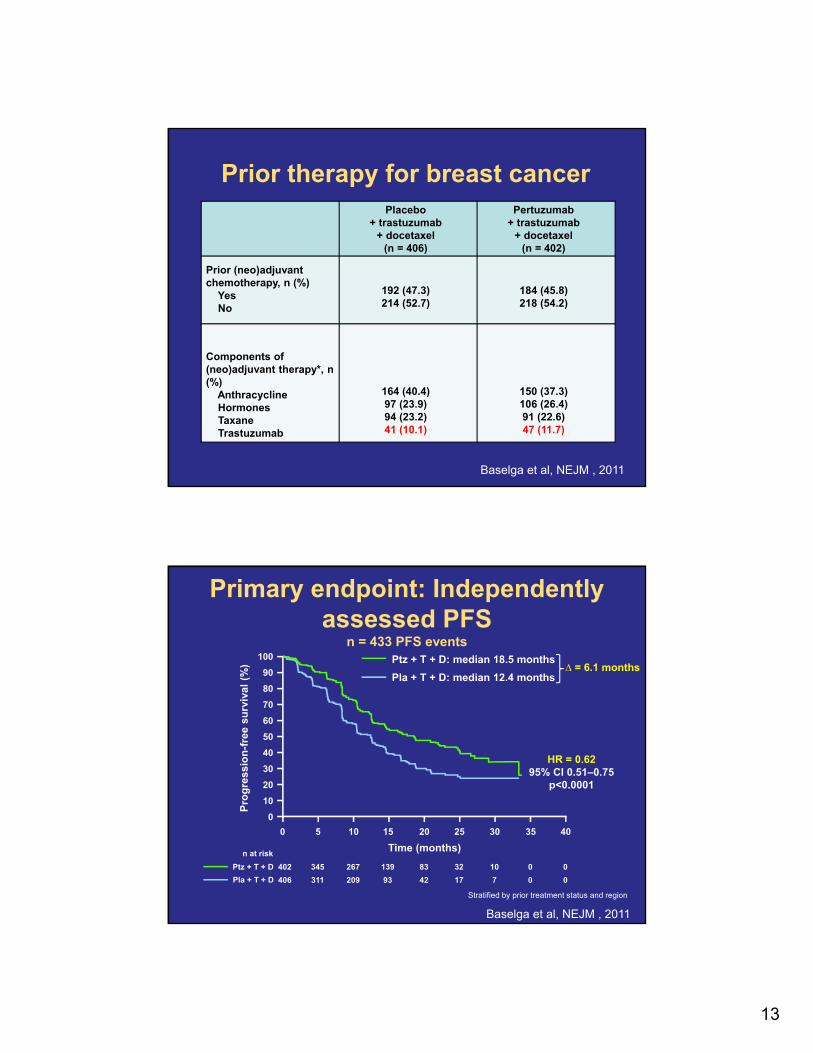
CLEOPATRA Study design
MBC, metastatic breast cancer; PD, progressive disease
Patients withHER2-positive MBCcentrally confirmed
(N = 808)
Placebo + trastuzumabn=406
• Randomization was stratified by geographic region and prior treatment status (neo/adjuvant chemotherapy received or not)
• Study dosing q3w:− Pertuzumab/Placebo: 840 mg loading dose, 420 mg maintenance− Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance− Docetaxel: 75 mg/m2, escalating to 100 mg/m2 if tolerated
1:1
n=402
Docetaxel*≥6 cycles recommended
PD
Pertuzumab + trastuzumab
Docetaxel*≥6 cycles recommended
PD
* <6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion
Baselga, et al NEJM , 2011
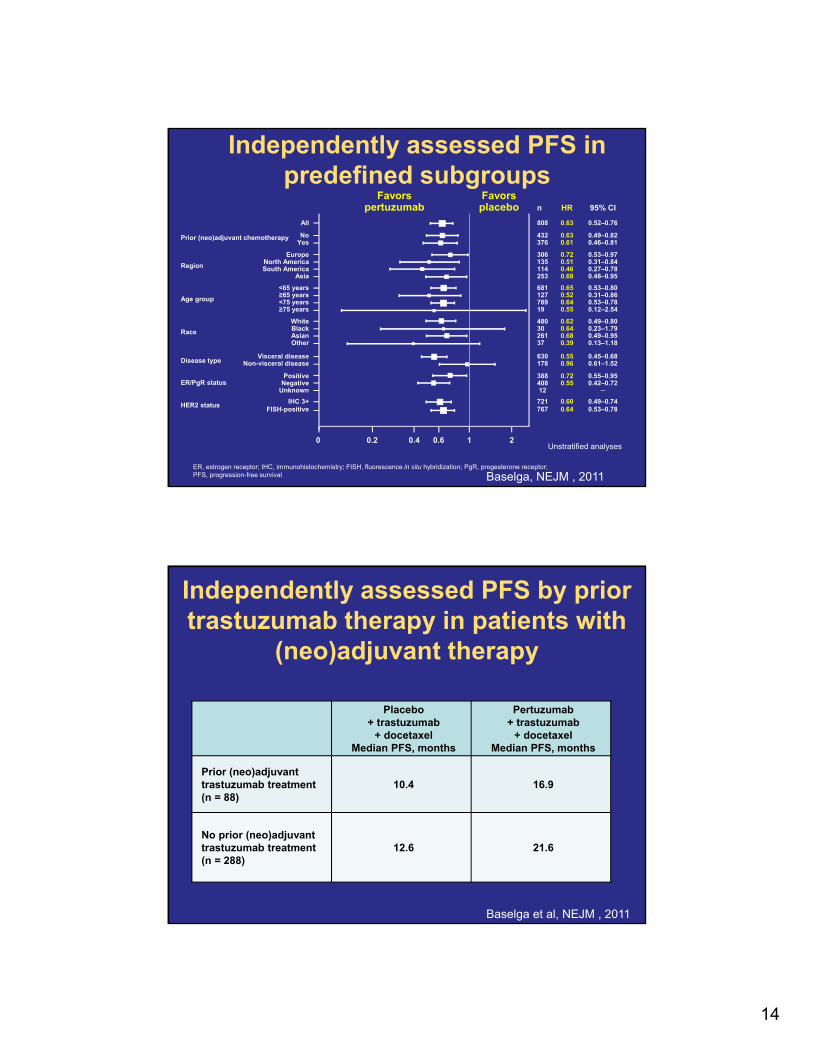
Baseline characteristics (I)
Placebo+ trastuzumab + docetaxel
(n = 406)
Pertuzumab+ trastuzumab + docetaxel
(n = 402)
Median age, years(range)
54.0 (27–89)
54.0 (22–82)
Region, n (%)AsiaEuropeNorth AmericaSouth America
128 (31.5)152 (37.4)68 (16.7)58 (14.3)
125 (31.1)154 (38.3)67 (16.7)56 (13.9)
ECOG PS, n (%)01≥2
248 (61.1)157 (38.7)
1 (0.2)
274 (68.2)125 (31.1)
3 (0.7)
Baselga et al, NEJM , 2011
13
Prior therapy for breast cancerPlacebo
+ trastuzumab+ docetaxel
(n = 406)
Pertuzumab+ trastuzumab
+ docetaxel(n = 402)
Prior (neo)adjuvant chemotherapy, n (%)
YesNo
192 (47.3)214 (52.7)
184 (45.8)218 (54.2)
Components of (neo)adjuvant therapy*, n (%)
AnthracyclineHormonesTaxaneTrastuzumab
164 (40.4)97 (23.9)94 (23.2)41 (10.1)
150 (37.3)106 (26.4)91 (22.6)47 (11.7)
Baselga et al, NEJM , 2011
Primary endpoint: Independently assessed PFS
n = 433 PFS events
0 5 10 15 20 25 30 35 40
0
10
20
30
40
50
60
70
80
90
100
n at risk
402 345 267 139 83 32 10 0 0Ptz + T + D
406 311 209 93 42 17 7 0 0Pla + T + D
Time (months)
Ptz + T + D: median 18.5 months
Pla + T + D: median 12.4 months
HR = 0.6295% CI 0.51‒0.75
p<0.0001
∆ = 6.1 months
Pro
gre
ssio
n-f
ree
surv
ival
(%
)
Stratified by prior treatment status and region
Baselga et al, NEJM , 2011
14
808 0.63 0.52‒0.76
432 0.63 0.49‒0.82376 0.61 0.46‒0.81
306 0.72 0.53‒0.97135 0.51 0.31‒0.84114 0.46 0.27‒0.78253 0.68 0.48‒0.95
681 0.65 0.53‒0.80127 0.52 0.31‒0.86789 0.64 0.53‒0.7819 0.55 0.12‒2.54
480 0.62 0.49‒0.8030 0.64 0.23‒1.79261 0.68 0.49‒0.9537 0.39 0.13‒1.18
630 0.55 0.45‒0.68178 0.96 0.61‒1.52
388 0.72 0.55‒0.95408 0.55 0.42‒0.7212 ─
721 0.60 0.49‒0.74767 0.64 0.53‒0.78
n HR 95% CI
All
NoYes
EuropeNorth AmericaSouth America
Asia
<65 years≥65 years<75 years≥75 years
WhiteBlackAsianOther
Visceral diseaseNon-visceral disease
PositiveNegative
Unknown
IHC 3+FISH-positive
0 0.2
ER/PgR status
Disease type
Race
Age group
Region
HER2 status
Prior (neo)adjuvant chemotherapy
0.4 0.6 1 2
Independently assessed PFS in predefined subgroups
ER, estrogen receptor; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization; PgR, progesterone receptor;PFS, progression-free survival
Favorsplacebo
Favorspertuzumab
Unstratified analyses
Baselga, NEJM , 2011
Independently assessed PFS by prior trastuzumab therapy in patients with
(neo)adjuvant therapy
Placebo+ trastuzumab
+ docetaxelMedian PFS, months
Pertuzumab+ trastuzumab
+ docetaxelMedian PFS, months
Prior (neo)adjuvant trastuzumab treatment(n = 88)
10.4 16.9
No prior (neo)adjuvanttrastuzumab treatment(n = 288)
12.6 21.6
Baselga et al, NEJM , 2011
15
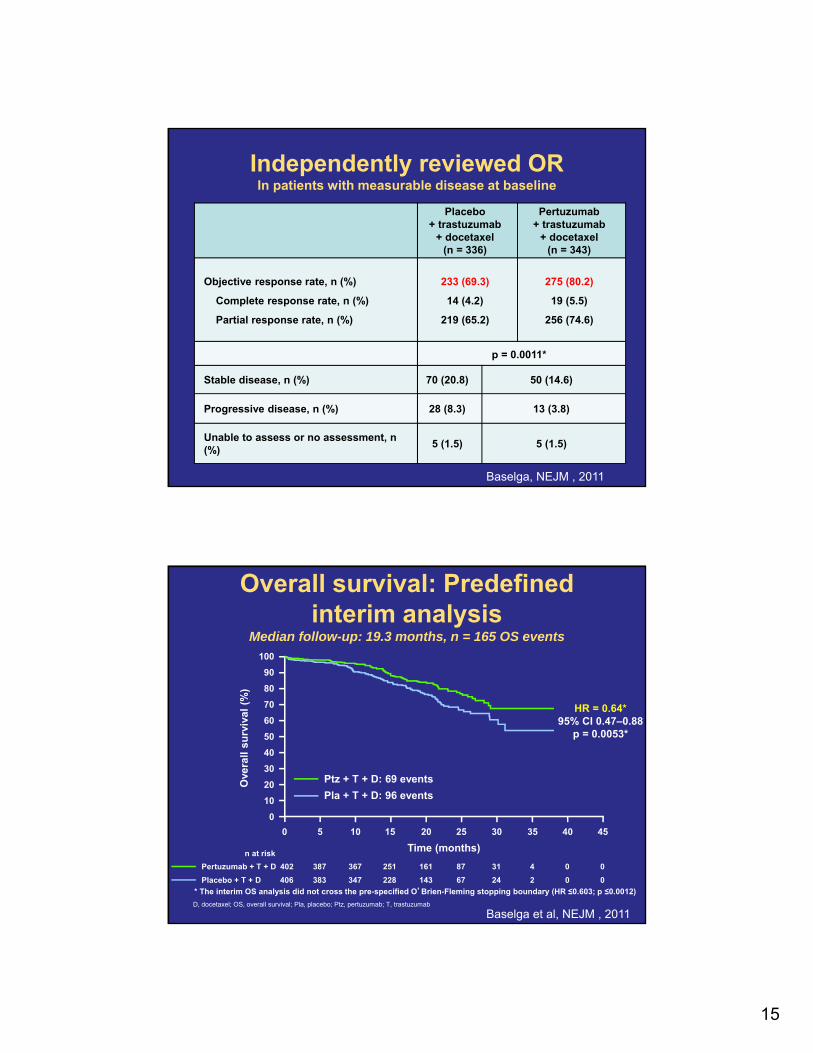
Independently reviewed ORIn patients with measurable disease at baseline
Placebo+ trastuzumab
+ docetaxel(n = 336)
Pertuzumab+ trastuzumab
+ docetaxel(n = 343)
Objective response rate, n (%)
Complete response rate, n (%)
Partial response rate, n (%)
233 (69.3)
14 (4.2)
219 (65.2)
275 (80.2)
19 (5.5)
256 (74.6)
p = 0.0011*
Stable disease, n (%) 70 (20.8) 50 (14.6)
Progressive disease, n (%) 28 (8.3) 13 (3.8)
Unable to assess or no assessment, n (%)
5 (1.5) 5 (1.5)
Baselga, NEJM , 2011
Overall survival: Predefined interim analysis
Median follow-up: 19.3 months, n = 165 OS events
D, docetaxel; OS, overall survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
0 5 10 15 20 25 30 35 40 45
0
10
20
30
40
50
60
70
80
90
100
n at risk
Pertuzumab + T + D 402 387 367 251 161 87 31 4 0 0
406 383 347 228 143 67 24 2 0 0Placebo + T + D
Time (months)
Ptz + T + D: 69 events
Pla + T + D: 96 events
HR = 0.64*95% CI 0.47‒0.88
p = 0.0053*
* The interim OS analysis did not cross the pre-specified O’Brien-Fleming stopping boundary (HR ≤0.603; p ≤0.0012)
Ove
rall
surv
iva
l (%
)
Baselga et al, NEJM , 2011
16
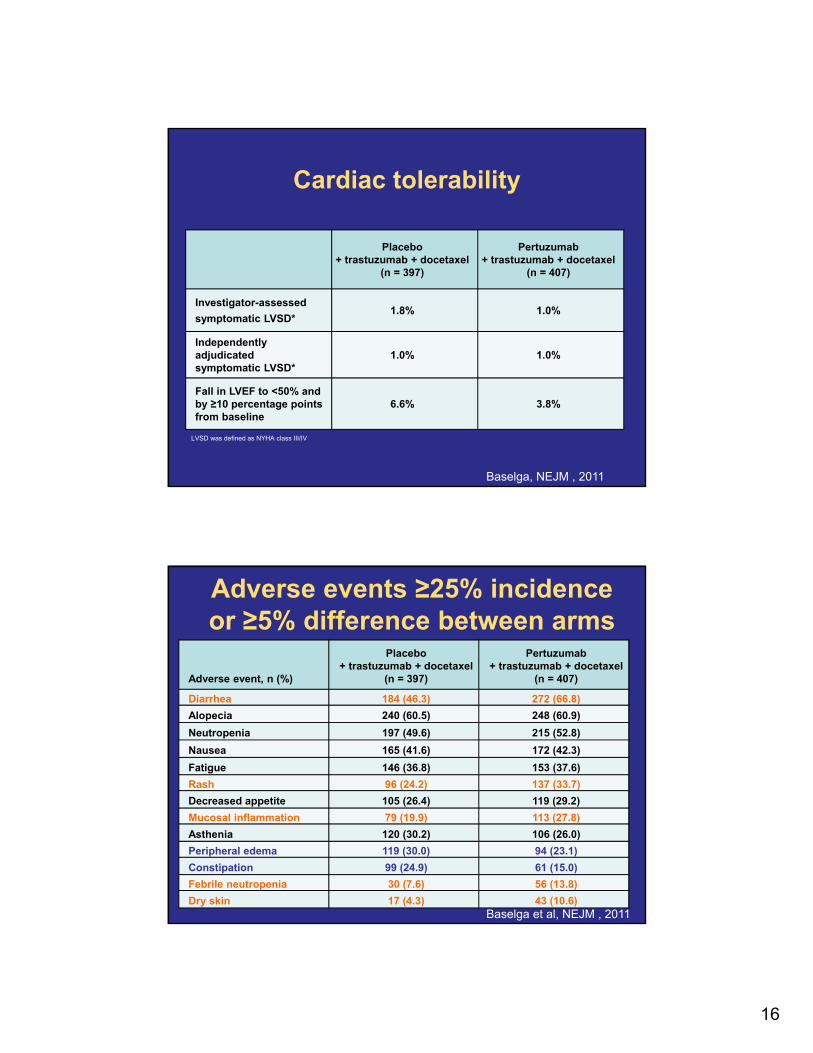
Cardiac tolerability
LVSD was defined as NYHA class III/IV
Placebo+ trastuzumab + docetaxel
(n = 397)
Pertuzumab+ trastuzumab + docetaxel
(n = 407)
Investigator-assessed
symptomatic LVSD*1.8% 1.0%
Independently adjudicatedsymptomatic LVSD*
1.0% 1.0%
Fall in LVEF to <50% and by ≥10 percentage points from baseline
6.6% 3.8%
Baselga, NEJM , 2011
Adverse events ≥25% incidence or ≥5% difference between arms
Adverse event, n (%)
Placebo+ trastuzumab + docetaxel
(n = 397)
Pertuzumab+ trastuzumab + docetaxel
(n = 407)
Diarrhea 184 (46.3) 272 (66.8)
Alopecia 240 (60.5) 248 (60.9)
Neutropenia 197 (49.6) 215 (52.8)
Nausea 165 (41.6) 172 (42.3)
Fatigue 146 (36.8) 153 (37.6)
Rash 96 (24.2) 137 (33.7)
Decreased appetite 105 (26.4) 119 (29.2)
Mucosal inflammation 79 (19.9) 113 (27.8)
Asthenia 120 (30.2) 106 (26.0)
Peripheral edema 119 (30.0) 94 (23.1)
Constipation 99 (24.9) 61 (15.0)
Febrile neutropenia 30 (7.6) 56 (13.8)
Dry skin 17 (4.3) 43 (10.6)Baselga et al, NEJM , 2011
17
Summary and conclusions
• CLEOPATRA met its primary endpoint and demonstrated a statistically significant improvement in PFS (HR = 0.62) in patients with HER2-positive MBC
• Median PFS increased by 6.1 months
• The combination of pertuzumab and trastuzumab plus docetaxel increased rates of diarrhea, rash, mucosal inflammation, febrile neutropenia, and dry skin
• There was no increase in cardiac adverse events or LVSD
Baselga et al, NEJM , 2011
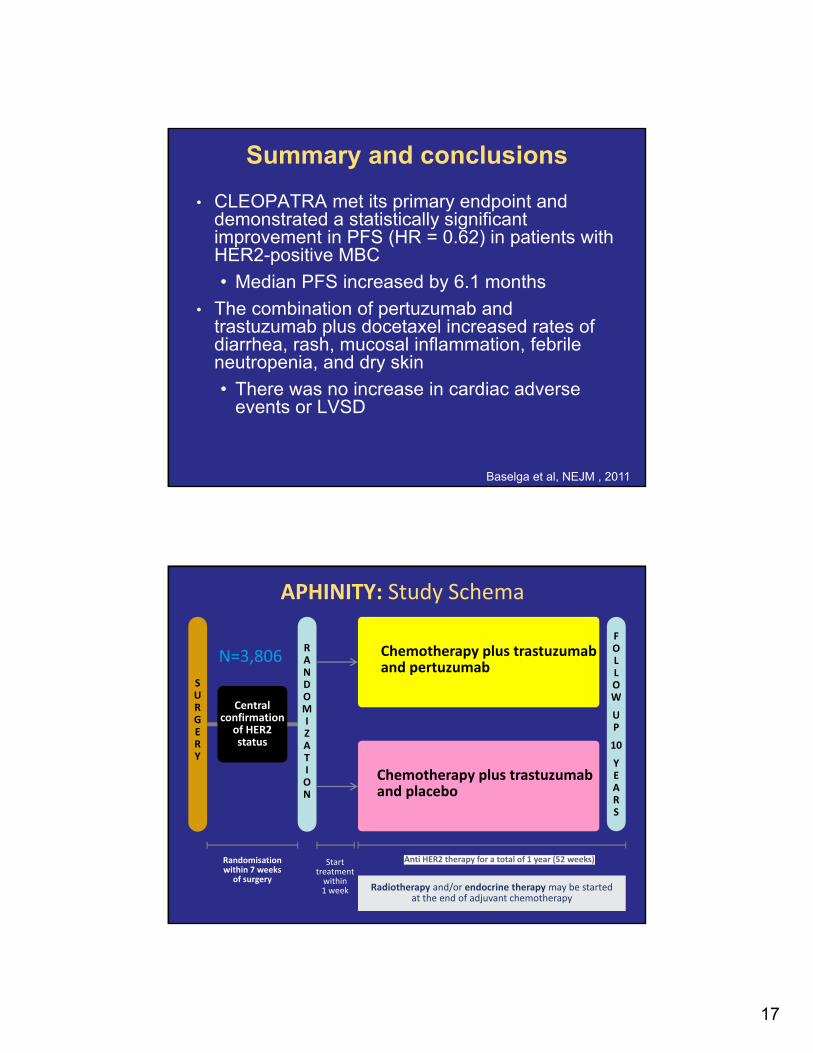
APHINITY: Study Schema
N=3,806SURGERY
Central confirmation
of HER2 status
Randomisationwithin 7 weeks
of surgery
Starttreatment
within1 week
FOLLOWUP
10YEARS
RANDOMIZATION
Chemotherapy plus trastuzumab and pertuzumab
Chemotherapy plus trastuzumab and placebo
Radiotherapy and/or endocrine therapy may be startedat the end of adjuvant chemotherapy
Anti HER2 therapy for a total of 1 year (52 weeks)
18
Should We add anti-VEGF to Anti-HER2 Drugs?
AVEREL Background
• Strong preclinical rationale for combining trastuzumab (H) and bevacizumab (BEV):
• VEGF expression is positively regulated by HER21,2
• VEGF levels correlate with HER2 overexpression3,4
• H and BEV are synergistic in in vivo models5
• Single-arm phase II studies of H + BEV (± chemotherapy) in LR/mBC showed encouraging activity6,7
1. Klos et al. Cancer Res 2008; 2. Loureiro et al. Biochem Biophys Res Comm2005; 3. Yang et al. Cancer 2002
4. Konecny et al. Clin Cancer Res 2004; 5. Pegram et al. SABCS 2004;6. Hurvitz et al. SABCS 2009; 7. Tjulandin et al. ASCO 2011
19
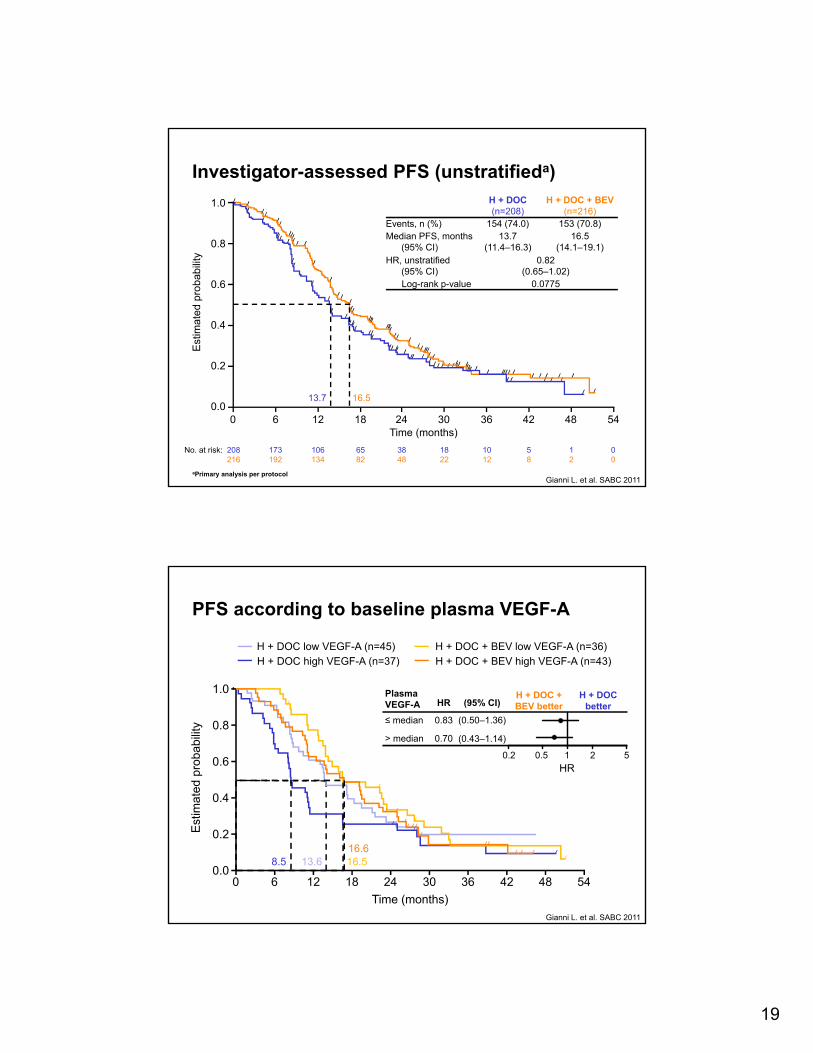
Investigator-assessed PFS (unstratifieda)E
stim
ated
pro
babi
lity
Time (months)0 6 12 18 24 30 36 42 48 54
1.0
0.8
0.6
0.4
0.2
0.0
No. at risk: 208 173 106 65 38 18 10 5 1 0216 192 134 82 48 22 12 8 2 0
13.7 16.5
H + DOC(n=208)
H + DOC + BEV(n=216)
Events, n (%) 154 (74.0) 153 (70.8)Median PFS, months
(95% CI)13.7
(11.4‒16.3)16.5
(14.1‒19.1)HR, unstratified
(95% CI)0.82
(0.65‒1.02)Log-rank p-value 0.0775
aPrimary analysis per protocolGianni L. et al. SABC 2011
PFS according to baseline plasma VEGF-A
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24 30 36 42 48 54
PlasmaVEGF-A HR (95% CI)
≤ median 0.83 (0.50‒1.36)
> median 0.70 (0.43‒1.14)
0.2 0.5 1 2 5
H + DOC + BEV better
HR
H + DOC better
Est
imat
ed p
roba
bilit
y
Time (months)
H + DOC low VEGF-A (n=45)
13.68.5
H + DOC high VEGF-A (n=37)
16.5
H + DOC + BEV low VEGF-A (n=36)
16.6
H + DOC + BEV high VEGF-A (n=43)
Gianni L. et al. SABC 2011
20
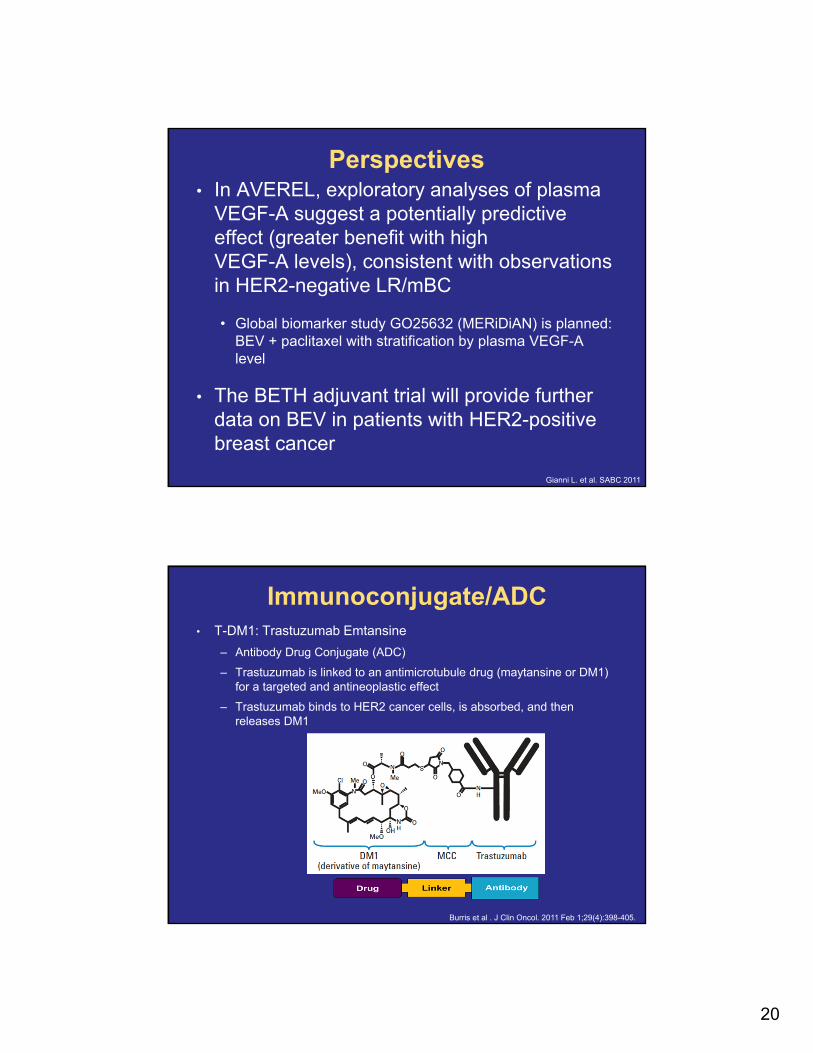
Perspectives• In AVEREL, exploratory analyses of plasma
VEGF-A suggest a potentially predictive effect (greater benefit with high VEGF-A levels), consistent with observations in HER2-negative LR/mBC
• Global biomarker study GO25632 (MERiDiAN) is planned: BEV + paclitaxel with stratification by plasma VEGF-A level
• The BETH adjuvant trial will provide further data on BEV in patients with HER2-positive breast cancer
Gianni L. et al. SABC 2011
Immunoconjugate/ADC• T-DM1: Trastuzumab Emtansine
– Antibody Drug Conjugate (ADC)
– Trastuzumab is linked to an antimicrotubule drug (maytansine or DM1) for a targeted and antineoplastic effect
– Trastuzumab binds to HER2 cancer cells, is absorbed, and then releases DM1
Burris et al . J Clin Oncol. 2011 Feb 1;29(4):398-405.
21
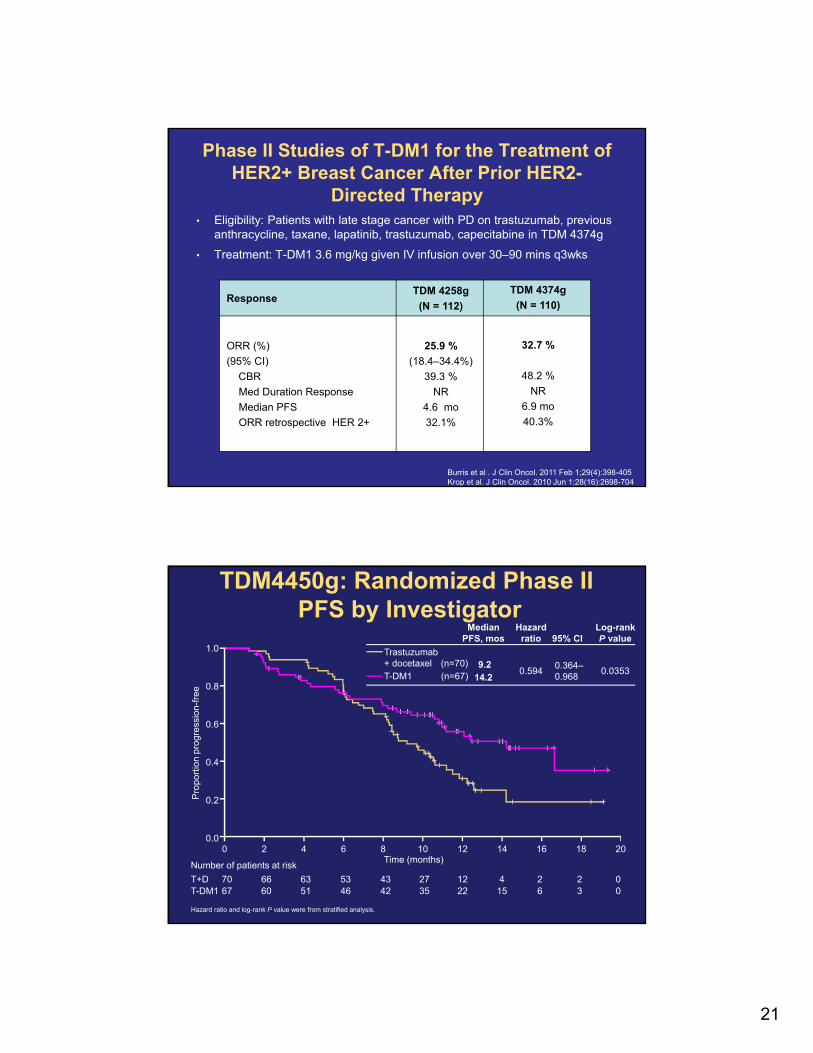
Phase II Studies of T-DM1 for the Treatment of HER2+ Breast Cancer After Prior HER2-
Directed Therapy• Eligibility: Patients with late stage cancer with PD on trastuzumab, previous
anthracycline, taxane, lapatinib, trastuzumab, capecitabine in TDM 4374g
• Treatment: T-DM1 3.6 mg/kg given IV infusion over 30–90 mins q3wks
ResponseTDM 4258g
(N = 112)
TDM 4374g
(N = 110)
ORR (%)
(95% CI)
CBR
Med Duration Response
Median PFS
ORR retrospective HER 2+
25.9 %
(18.4–34.4%)
39.3 %
NR
4.6 mo
32.1%
32.7 %
48.2 %
NR
6.9 mo
40.3%
Burris et al . J Clin Oncol. 2011 Feb 1;29(4):398-405Krop et al. J Clin Oncol. 2010 Jun 1;28(16):2698-704
Time (months)
TDM4450g: Randomized Phase IIPFS by Investigator
Pro
port
ion
prog
ress
ion-
free
1.0
0.8
0.6
0.4
0.2
0.00 2 4 6 8 10 12 14 16 18 20
Number of patients at risk
T+D 70 66 63 53 43 27 12 4 2 2 0T-DM1 67 60 51 46 42 35 22 15 6 3 0
Hazard ratio and log-rank P value were from stratified analysis.
Trastuzumab + docetaxel (n=70)T-DM1 (n=67)
MedianPFS, mos
Hazard ratio 95% CI
Log-rank P value
9.214.2
0.5940.364–0.968
0.0353
22
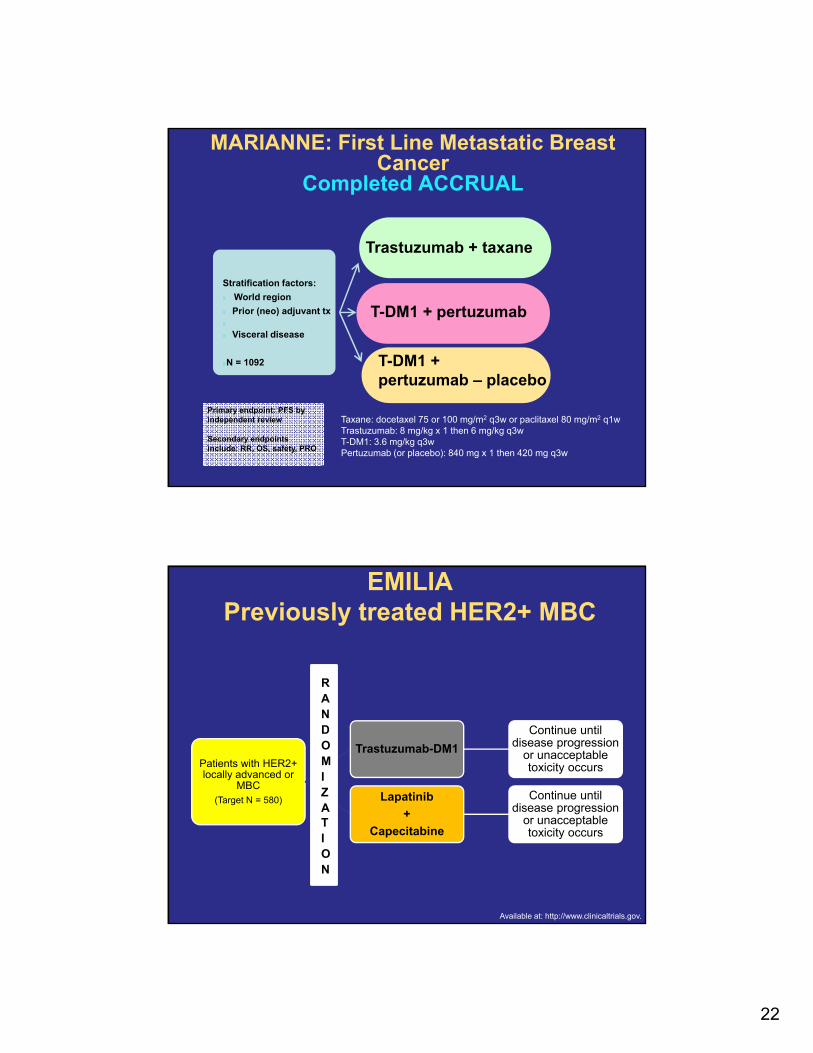
MARIANNE: First Line Metastatic Breast Cancer
Completed ACCRUAL
Trastuzumab + taxane
T-DM1 + pertuzumab
T-DM1 + pertuzumab – placebo
Stratification factors:
World region
Prior (neo) adjuvant tx
Visceral disease
N = 1092
Primary endpoint: PFS by independent review
Secondary endpoints include: RR, OS, safety, PRO
Taxane: docetaxel 75 or 100 mg/m2 q3w or paclitaxel 80 mg/m2 q1wTrastuzumab: 8 mg/kg x 1 then 6 mg/kg q3wT-DM1: 3.6 mg/kg q3wPertuzumab (or placebo): 840 mg x 1 then 420 mg q3w
EMILIAPreviously treated HER2+ MBC
Patients with HER2+ locally advanced or
MBC(Target N = 580)
Trastuzumab-DM1
Continue until disease progression
or unacceptable toxicity occurs
Lapatinib
+
Capecitabine
Continue until disease progression
or unacceptable toxicity occurs
RANDOMIZATION
Available at: http://www.clinicaltrials.gov.
23
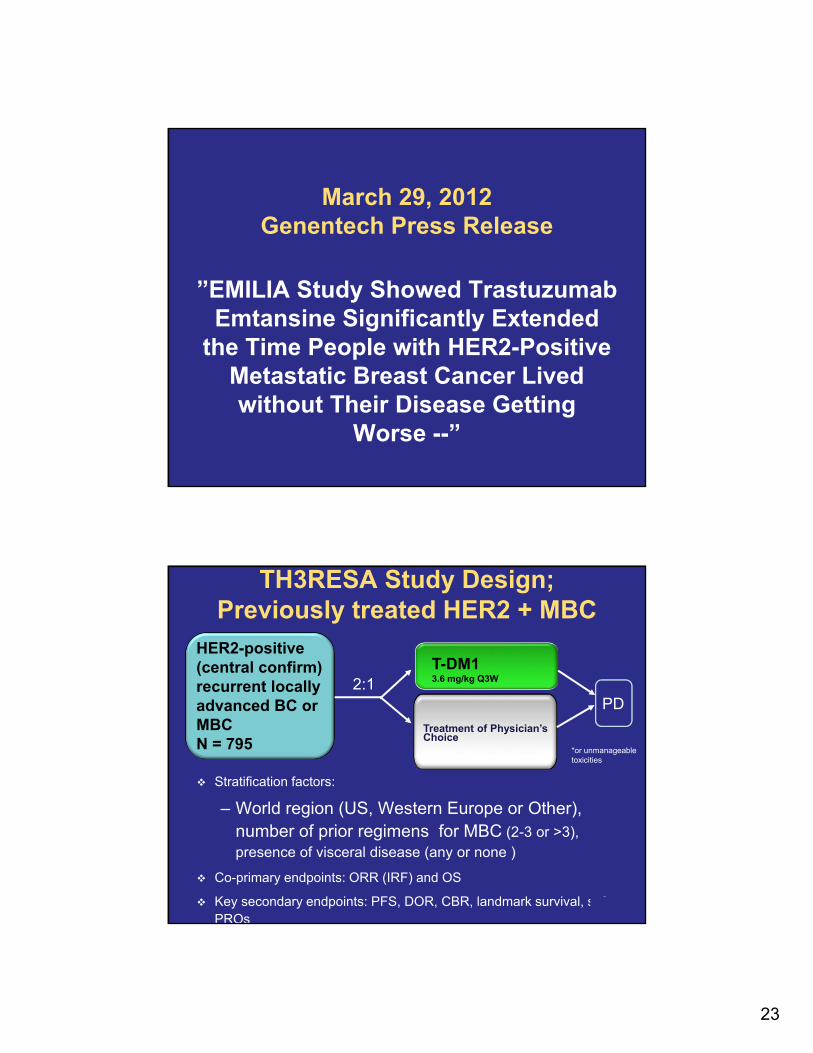
March 29, 2012 Genentech Press Release
”EMILIA Study Showed TrastuzumabEmtansine Significantly Extended
the Time People with HER2-Positive Metastatic Breast Cancer Lived without Their Disease Getting
Worse --”
Stratification factors:
– World region (US, Western Europe or Other), number of prior regimens for MBC (2-3 or >3), presence of visceral disease (any or none )
Co-primary endpoints: ORR (IRF) and OS
Key secondary endpoints: PFS, DOR, CBR, landmark survival, safety, PROs
TH3RESA Study Design; Previously treated HER2 + MBC
2:1
HER2-positive(central confirm) recurrent locally advanced BC or MBCN = 795
T-DM13.6 mg/kg Q3W
Treatment of Physician’s Choice
PD
*or unmanageable toxicities
24
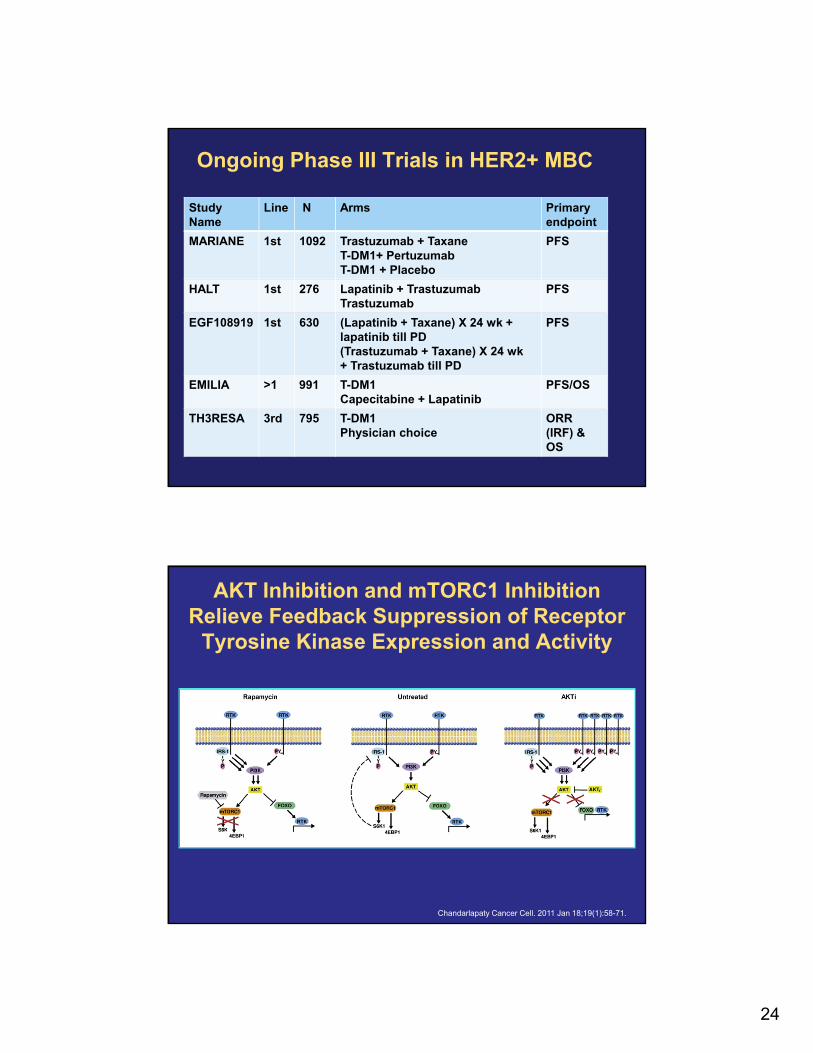
Ongoing Phase III Trials in HER2+ MBC
Study Name
Line N Arms Primary endpoint
MARIANE 1st 1092 Trastuzumab + TaxaneT-DM1+ PertuzumabT-DM1 + Placebo
PFS
HALT 1st 276 Lapatinib + TrastuzumabTrastuzumab
PFS
EGF108919 1st 630 (Lapatinib + Taxane) X 24 wk + lapatinib till PD(Trastuzumab + Taxane) X 24 wk + Trastuzumab till PD
PFS
EMILIA >1 991 T-DM1Capecitabine + Lapatinib
PFS/OS
TH3RESA 3rd 795 T-DM1Physician choice
ORR (IRF) & OS
AKT Inhibition and mTORC1 Inhibition Relieve Feedback Suppression of Receptor
Tyrosine Kinase Expression and Activity
Chandarlapaty Cancer Cell. 2011 Jan 18;19(1):58-71.
25
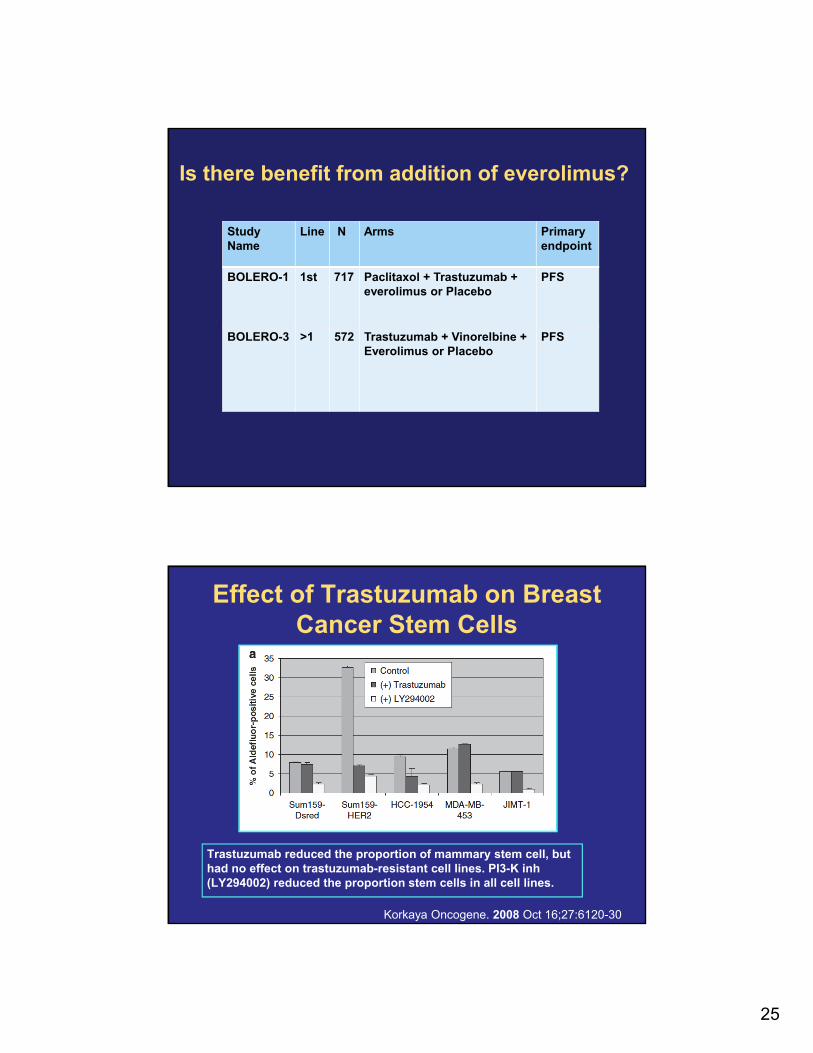
Is there benefit from addition of everolimus?
Study Name
Line N Arms Primary endpoint
BOLERO-1 1st 717 Paclitaxol + Trastuzumab + everolimus or Placebo
PFS
BOLERO-3 >1 572 Trastuzumab + Vinorelbine + Everolimus or Placebo
PFS
Effect of Trastuzumab on Breast Cancer Stem Cells
Trastuzumab reduced the proportion of mammary stem cell, but had no effect on trastuzumab-resistant cell lines. PI3-K inh (LY294002) reduced the proportion stem cells in all cell lines.
Korkaya Oncogene. 2008 Oct 16;27:6120-30
26
Adjuvant Therapy
Phase II Trial of Adjuvant TC (Docetaxel/Cyclophosphamide) Plus
Trastuzumab (HER TC) in HER2 Positive Early Stage Breast Cancer Patients
Steve Jones, MD1,2; Rufus Collea, MD1,3; Devchand Paul, DO, PhD1,4; Ruth Ortiz, MD1,5; Scot Sedlacek, MD1,4; Anne Favret, MD1,6; Ira Gore, Jr, MD1,7; Deborah Lindquist, MD1,8; Frankie
Ann Holmes, MD1,9; Mary Ann K. Allison, MD10; Michael S. Steinberg, MD1,11; Christopher Stokoe, MD1,12; Raul M. Portillo, MD1,13; Maria W. Crockett, CCRP1; Yunfei Wang, MS1;
Lina Asmar, PhD1; Nicholas Robert, MD1,6; Joyce O’Shaughnessy, MD1,2
1US Oncology Research, McKesson Specialty Health, The Woodlands, TX; 2Texas Oncology, Baylor-Sammons Cancer Center, Dallas TX ; 3New York Oncology Hematology,
Albany, NY; 4Rocky Mountain Cancer, Denver CO; 5New York, NY; 6Virginia Cancer Specialists, PC, Fairfax, VA; 7Birmingham Hematology and Oncology, Birmingham, AL; 8Arizona Oncology Associates,
Sedona AZ; 9Texas Oncology, Houston, TX; 10Comprehensive Cancer Center, Henderson, NV; 11Virginia Oncology Associates, Virginia Beach, VA, 12Texas Oncology, Plano, TX,
13Texas Oncology, El Paso, TX
This study was supported by sanofi.
Poster #PD07-03, San Antonio Breast Cancer Symposium; December 6–10, 2011, San Antonio, TX, USA
27
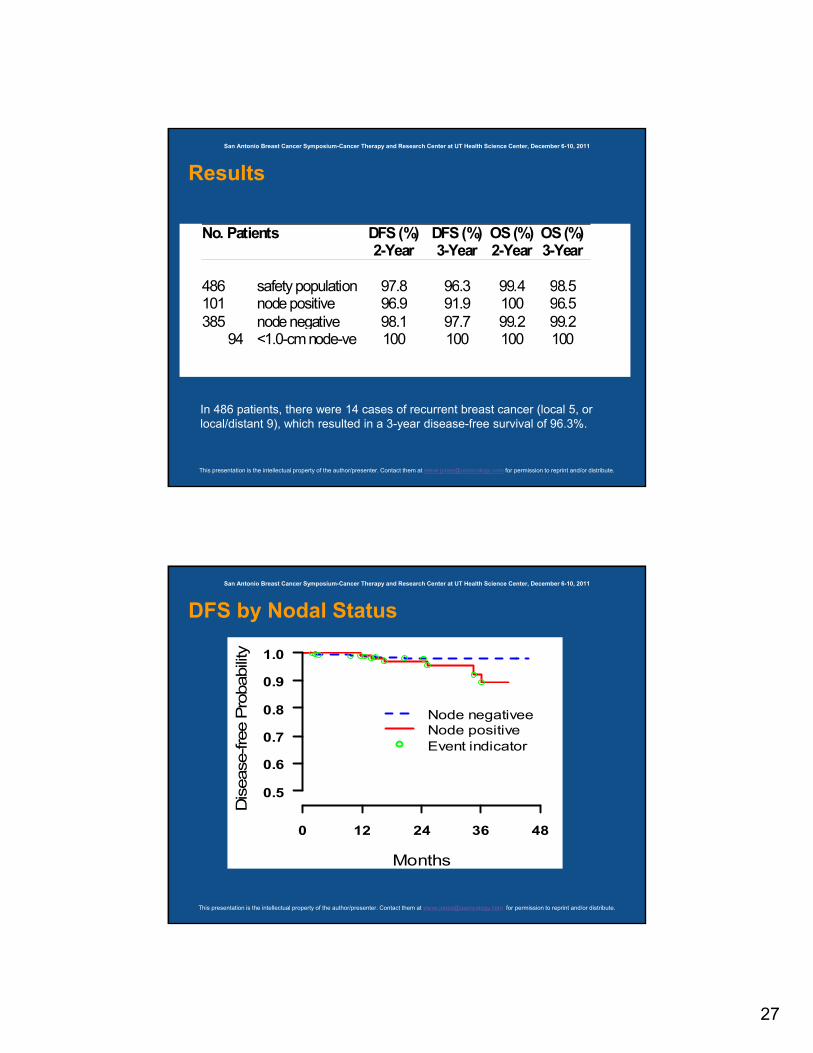
Results
San Antonio Breast Cancer Symposium-Cancer Therapy and Research Center at UT Health Science Center, December 6-10, 2011
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
In 486 patients, there were 14 cases of recurrent breast cancer (local 5, or local/distant 9), which resulted in a 3-year disease-free survival of 96.3%.
No. Patients DFS (%)2-Year
DFS (%)3-Year
OS (%)2-Year
OS (%) 3-Year
486 safety population 97.8 96.3 99.4 98.5 101 node positive 96.9 91.9 100 96.5 385 node negative 98.1 97.7 99.2 99.2 94 <1.0-cm node-ve
100 100 100 100
DFS by Nodal Status
San Antonio Breast Cancer Symposium-Cancer Therapy and Research Center at UT Health Science Center, December 6-10, 2011
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
0 12 24 36 48
0.5
0.6
0.7
0.8
0.9
1.0
Months
Dis
ease
-fre
e P
robability
Node negativeeNode positiveEvent indicator
28
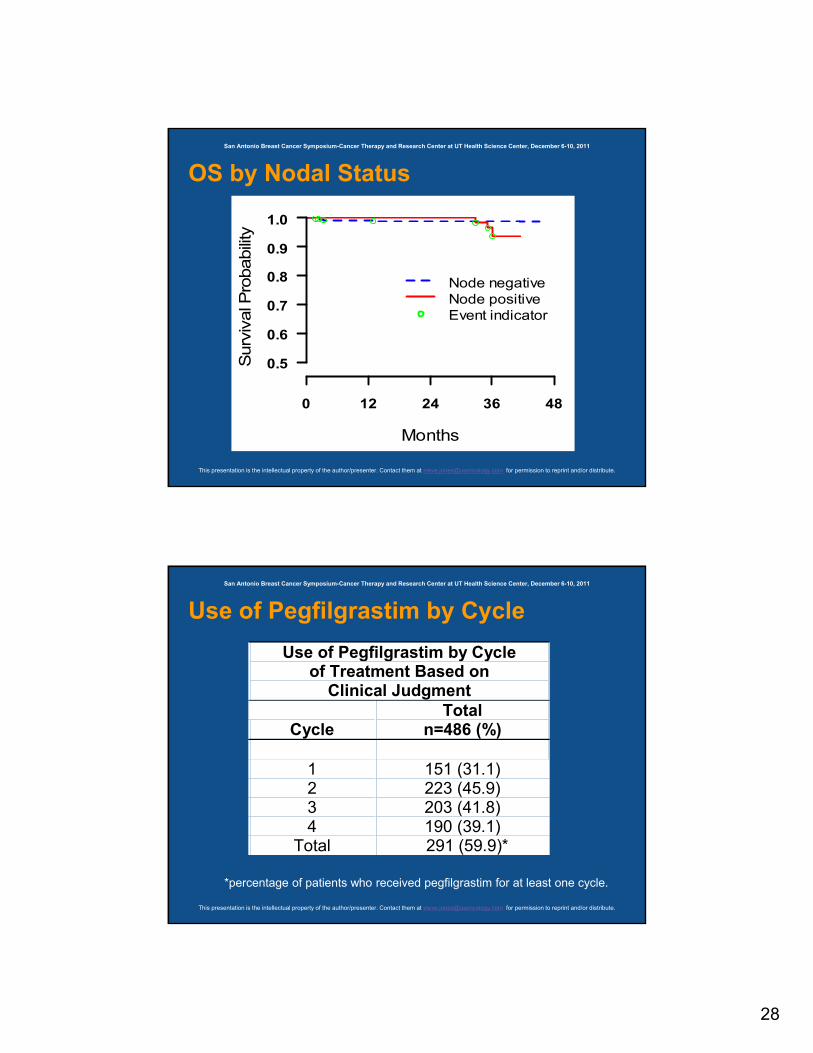
OS by Nodal Status
0 12 24 36 48
0.5
0.6
0.7
0.8
0.9
1.0
Months
Surv
ival P
robabili
ty
Node negativeNode positiveEvent indicator
San Antonio Breast Cancer Symposium-Cancer Therapy and Research Center at UT Health Science Center, December 6-10, 2011
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
Use of Pegfilgrastim by Cycle
Use of Pegfilgrastim by Cycle of Treatment Based on
Clinical Judgment
Cycle Total
n=486 (%)
1 151 (31.1) 2 223 (45.9) 3 203 (41.8) 4 190 (39.1)
Total 291 (59.9)*
*percentage of patients who received pegfilgrastim for at least one cycle.
San Antonio Breast Cancer Symposium-Cancer Therapy and Research Center at UT Health Science Center, December 6-10, 2011
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
29
Conclusion
1) 486 patients with HER2+ ESBC in a Phase II, non-comparative, open-label study received HER TC as adjuvant chemotherapy with trastuzumab.
2) DFS was 96.3% and OS was 98.5% at 3 years.
3) In comparison with other published regimens at 2-3 years, HER TC appears to be effective.
San Antonio Breast Cancer Symposium-Cancer Therapy and Research Center at UT Health Science Center, December 6-10, 2011
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
Conclusions continued
4) Toxicity was as expected for this combination and was mainly hematologic with a low rate of cardiac dysfunction, mainly reversible.
5) The HER TC regimen is an option for patients with lower risk HER2+ ESBC.
San Antonio Breast Cancer Symposium-Cancer Therapy and Research Center at UT Health Science Center, December 6-10, 2011
30
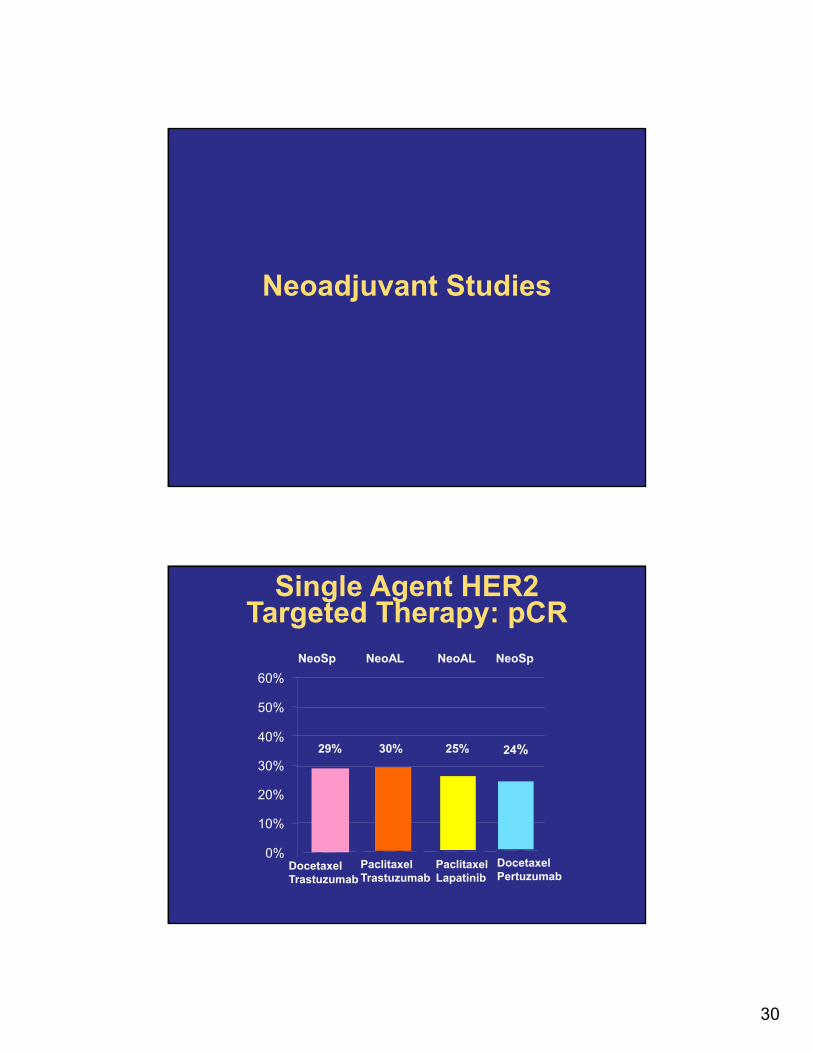
Neoadjuvant Studies
29% 30%
0%
10%
20%
30%
40%
50%
60%
DocetaxelTrastuzumab
PaclitaxelTrastuzumab
25%
NeoSp NeoAL NeoAL NeoSp
PaclitaxelLapatinib
Single Agent HER2 Targeted Therapy: pCR
24%
DocetaxelPertuzumab
31
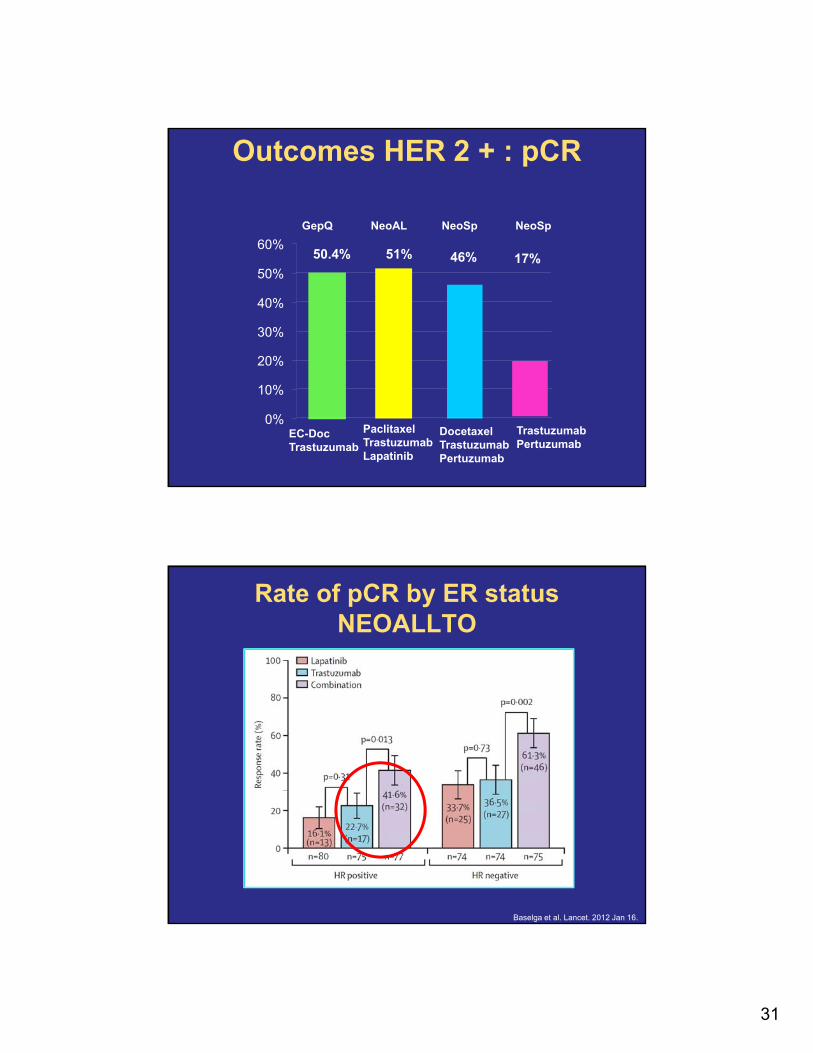
50.4% 51%
0%
10%
20%
30%
40%
50%
60%
EC-DocTrastuzumab
DocetaxelTrastuzumabPertuzumab
46%
Outcomes HER 2 + : pCR
PaclitaxelTrastuzumabLapatinib
GepQ NeoAL NeoSp NeoSp
17%
TrastuzumabPertuzumab
Rate of pCR by ER statusNEOALLTO
Baselga et al. Lancet. 2012 Jan 16.
32
Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6‒10, 2011
63
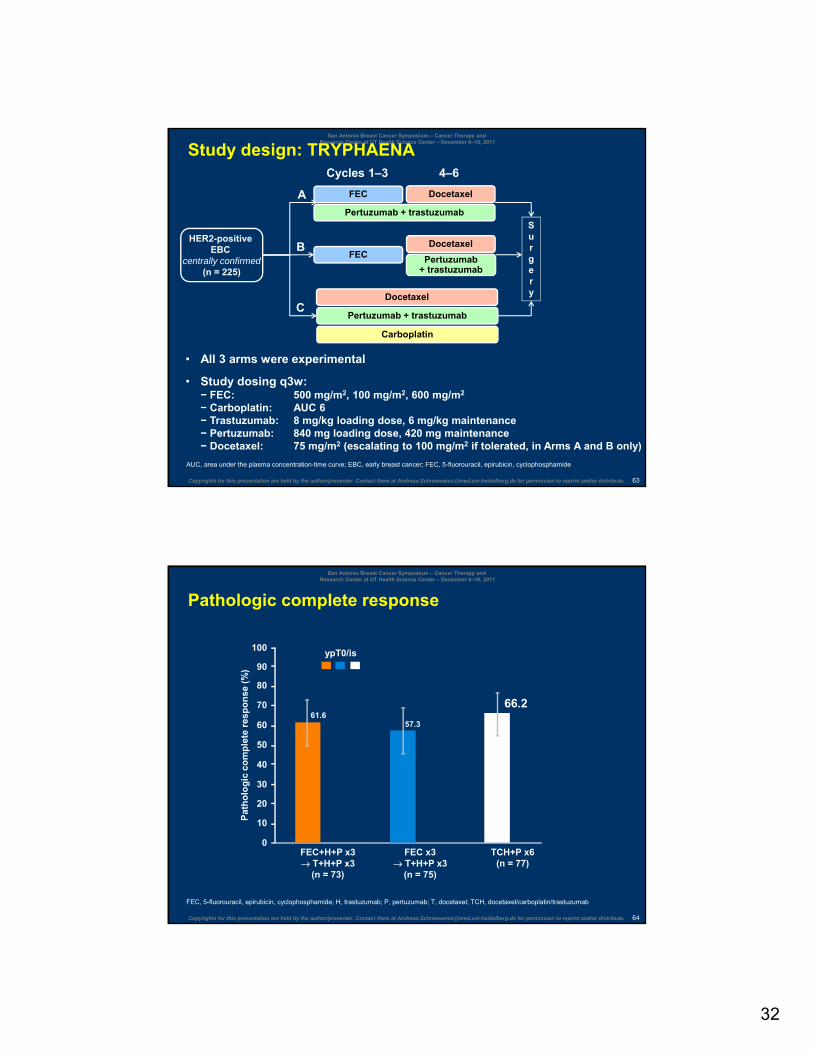
Study design: TRYPHAENA
AUC, area under the plasma concentration-time curve; EBC, early breast cancer; FEC, 5-fluorouracil, epirubicin, cyclophosphamide
HER2-positive EBC
centrally confirmed(n = 225)
FEC
Surgery
• All 3 arms were experimental
• Study dosing q3w:− FEC: 500 mg/m2, 100 mg/m2, 600 mg/m2
− Carboplatin: AUC 6− Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance− Pertuzumab: 840 mg loading dose, 420 mg maintenance− Docetaxel: 75 mg/m2 (escalating to 100 mg/m2 if tolerated, in Arms A and B only)
Docetaxel
Cycles 1‒3 4‒6
Pertuzumab+ trastuzumab
Pertuzumab + trastuzumab
FECDocetaxel
Carboplatin
Docetaxel
Pertuzumab + trastuzumabC
B
A
Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6‒10, 2011
64
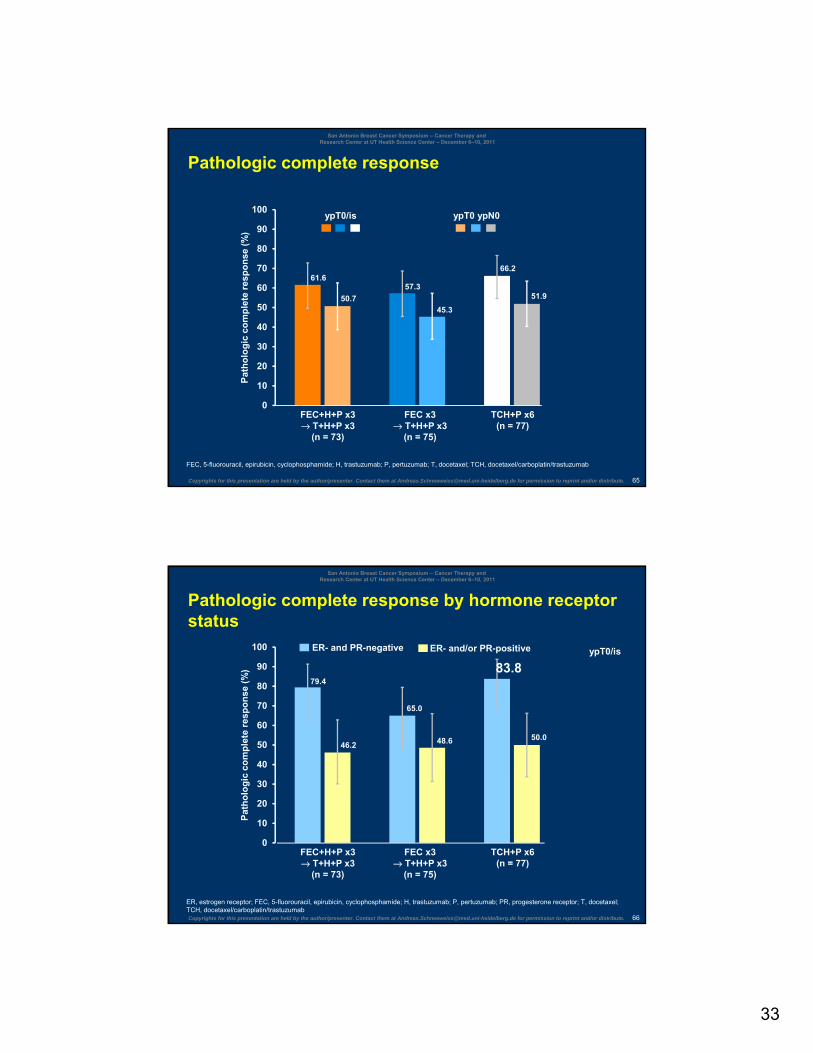
Pathologic complete response
FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
Pat
ho
log
ic c
om
ple
te r
esp
on
se (
%)
FEC+H+P x3→ T+H+P x3
(n = 73)
FEC x3→ T+H+P x3
(n = 75)
TCH+P x6(n = 77)
ypT0/is100
90
80
70
60
50
40
30
20
10
0
61.666.2
57.3
33
Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6‒10, 2011
65
0
10
20
30
40
50
60
70
80
90
100
Pathologic complete response
FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
Pat
ho
log
ic c
om
ple
te r
esp
on
se (
%)
FEC+H+P x3→ T+H+P x3
(n = 73)
FEC x3→ T+H+P x3
(n = 75)
TCH+P x6(n = 77)
50.7
45.3
51.9
ypT0/is ypT0 ypN0
61.666.2
57.3
Copyrights for this presentation are held by the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute.
San Antonio Breast Cancer Symposium – Cancer Therapy and Research Center at UT Health Science Center – December 6‒10, 2011
66
0
10
20
30
40
50
60
70
80
90
100
Pathologic complete response by hormone receptor status
ER, estrogen receptor; FEC, 5-fluorouracil, epirubicin, cyclophosphamide; H, trastuzumab; P, pertuzumab; PR, progesterone receptor; T, docetaxel; TCH, docetaxel/carboplatin/trastuzumab
Pat
ho
log
ic c
om
ple
te r
esp
on
se (
%)
ER- and PR-negative ER- and/or PR-positive
79.4
65.0
46.2 48.6
83.8
50.0
ypT0/is
FEC+H+P x3→ T+H+P x3
(n = 73)
FEC x3→ T+H+P x3
(n = 75)
TCH+P x6(n = 77)
34
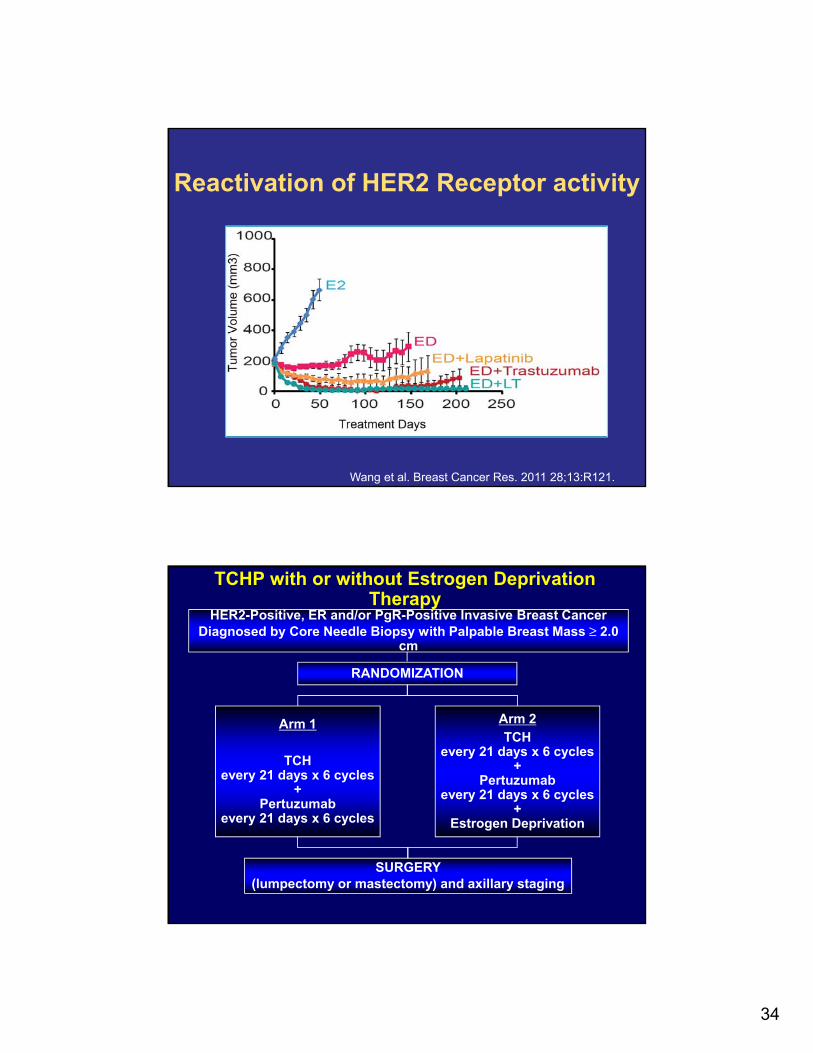
Reactivation of HER2 Receptor activity
Wang et al. Breast Cancer Res. 2011 28;13:R121.
HER2-Positive, ER and/or PgR-Positive Invasive Breast CancerDiagnosed by Core Needle Biopsy with Palpable Breast Mass ≥ 2.0
cm
RANDOMIZATION
Arm 1
TCHevery 21 days x 6 cycles
+Pertuzumab
every 21 days x 6 cycles
Arm 2TCH
every 21 days x 6 cycles+
Pertuzumabevery 21 days x 6 cycles
+Estrogen Deprivation
SURGERY (lumpectomy or mastectomy) and axillary staging
TCHP with or without Estrogen Deprivation Therapy
35
Key Messages• Large number of active agents
• TKIs (HER2 and/or others)
• MoAbs
• T-DM1
• HSP90 inhibitors
• AKTi (PI3Ki, mTORi, etc…)
• Resistance to HER2 therapy an important area of investigation
• ER positive
• Stem cells
Everolimus for postmenopausal women with advanced breast cancer:
updated results of the BOLERO-2 trial
G. N. Hortobagyi, M. Piccart, H. Rugo, H. Burris, M. Campone, S. Noguchi, M. Gnant, K. I. Pritchard, L. Vittori, P.
Mukhopadhyay, T. Sahmoud, D. Lebwohl, J. Baselga
On behalf of the BOLERO-2 Investigators
Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7) 70
36
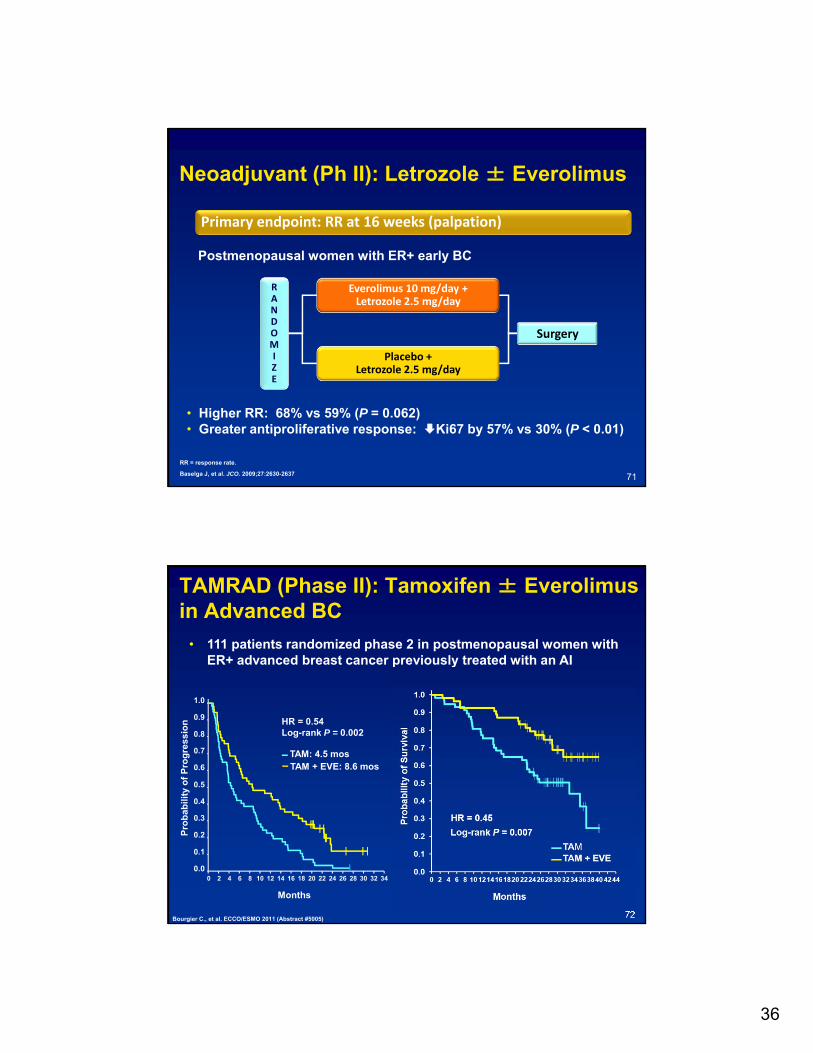
Neoadjuvant (Ph II): Letrozole ± Everolimus
RR = response rate.
Baselga J, et al. JCO. 2009;27:2630-2637
Primary endpoint: RR at 16 weeks (palpation)
Postmenopausal women with ER+ early BC
Everolimus 10 mg/day +Letrozole 2.5 mg/day
Placebo +Letrozole 2.5 mg/day
Surgery
RANDOMIZE
• Higher RR: 68% vs 59% (P = 0.062)• Greater antiproliferative response: Ki67 by 57% vs 30% (P < 0.01)
71
TAMRAD (Phase II): Tamoxifen ± Everolimus in Advanced BC
72
• 111 patients randomized phase 2 in postmenopausal women with ER+ advanced breast cancer previously treated with an AI
Bourgier C., et al. ECCO/ESMO 2011 (Abstract #5005)
1.0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
Pro
bab
ilit
y o
f P
rog
res
sio
n
TAM: 4.5 mosTAM + EVE: 8.6 mos
Months
HR = 0.54Log-rank P = 0.002
37
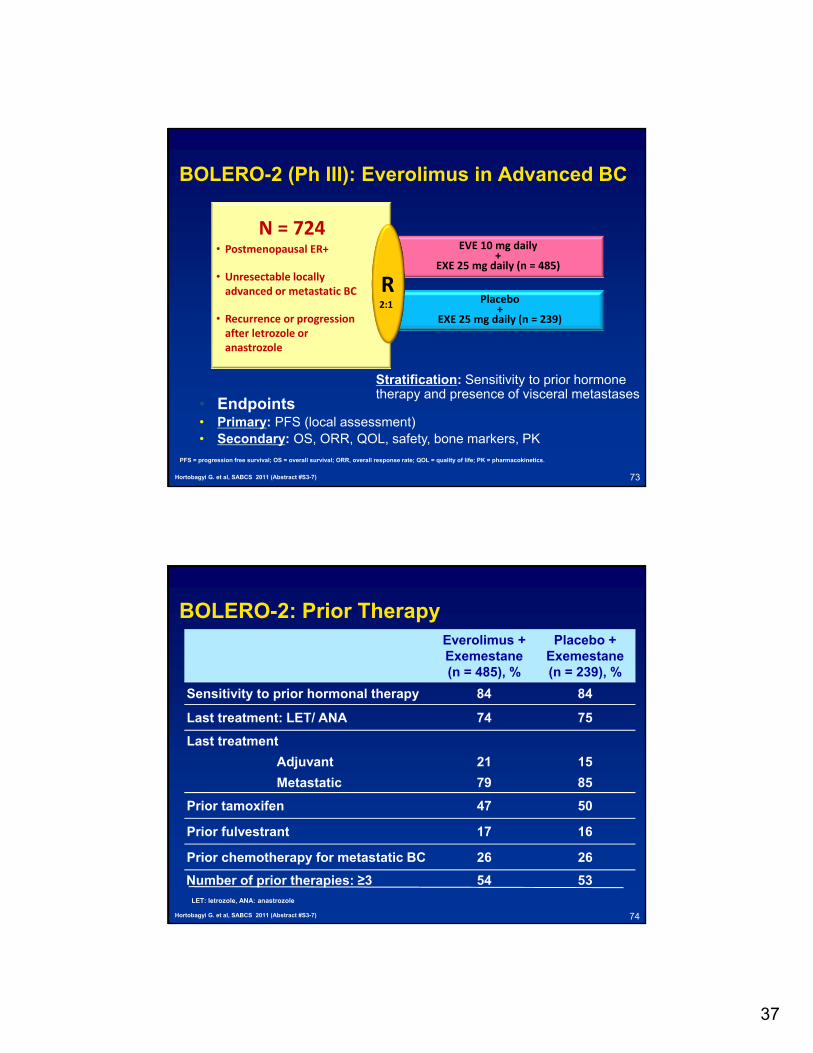
BOLERO-2 (Ph III): Everolimus in Advanced BC
EVE 10 mg daily+
EXE 25 mg daily (n = 485)
Placebo+
EXE 25 mg daily (n = 239)
R
• Endpoints• Primary: PFS (local assessment)• Secondary: OS, ORR, QOL, safety, bone markers, PK
2:1
N = 724• Postmenopausal ER+
• Unresectable locally advanced or metastatic BC
• Recurrence or progression after letrozole or anastrozole
Stratification: Sensitivity to prior hormone therapy and presence of visceral metastases
Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7) 73
PFS = progression free survival; OS = overall survival; ORR, overall response rate; QOL = quality of life; PK = pharmacokinetics.
BOLERO-2: Prior Therapy Everolimus + Exemestane(n = 485), %
Placebo +Exemestane(n = 239), %
Sensitivity to prior hormonal therapy 84 84
Last treatment: LET/ ANA 74 75
Last treatment
Adjuvant 21 15
Metastatic 79 85
Prior tamoxifen 47 50
Prior fulvestrant 17 16
Prior chemotherapy for metastatic BC 26 26
Number of prior therapies: ≥3 54 53LET: letrozole, ANA: anastrozole
74Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
38
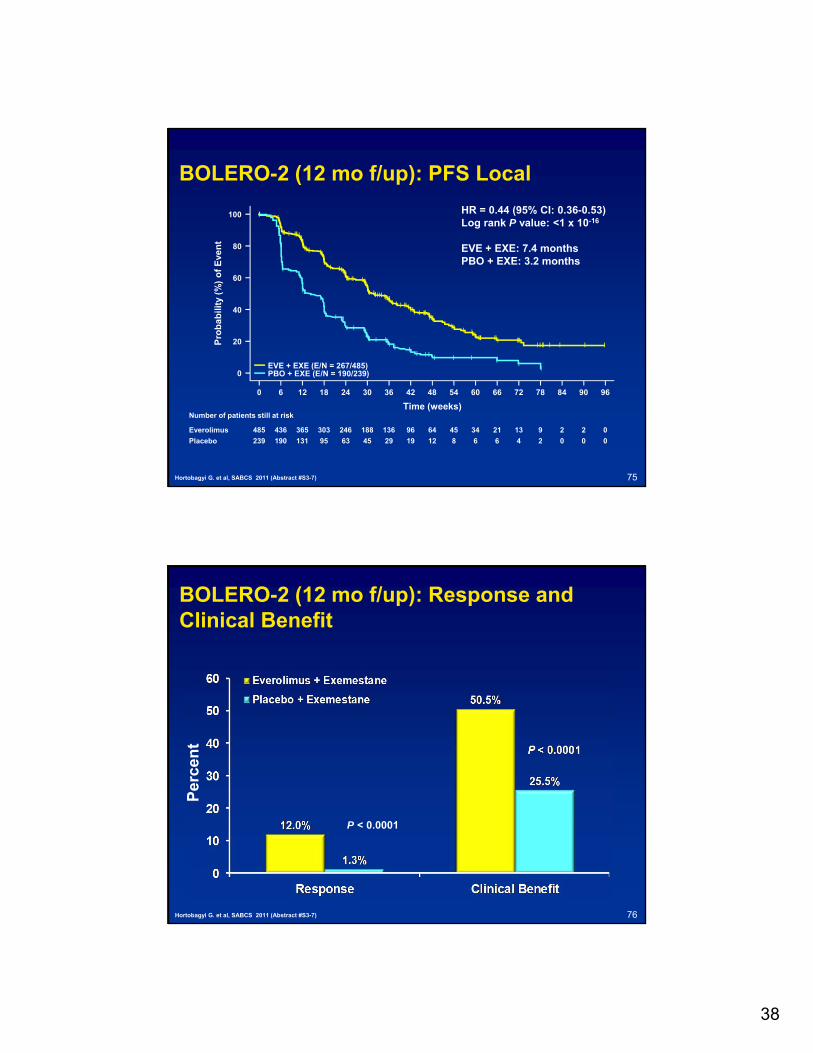
BOLERO-2 (12 mo f/up): PFS Local
75Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
0
20
40
60
80
100
0 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96
Time (weeks)
Pro
bab
ilit
y (%
) o
f E
ven
tHR = 0.44 (95% CI: 0.36-0.53)Log rank P value: <1 x 10-16
EVE + EXE: 7.4 monthsPBO + EXE: 3.2 months
EVE + EXE (E/N = 267/485)PBO + EXE (E/N = 190/239)
Everolimus
Placebo
Number of patients still at risk
485 436 365 303 246 188 136 96 64 45 34 21 13 9 2 2 0
239 190 131 95 63 45 29 19 12 8 6 6 4 2 0 0 0
BOLERO-2 (12 mo f/up): Response and Clinical Benefit
76
P < 0.0001
Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
Per
cen
t
39
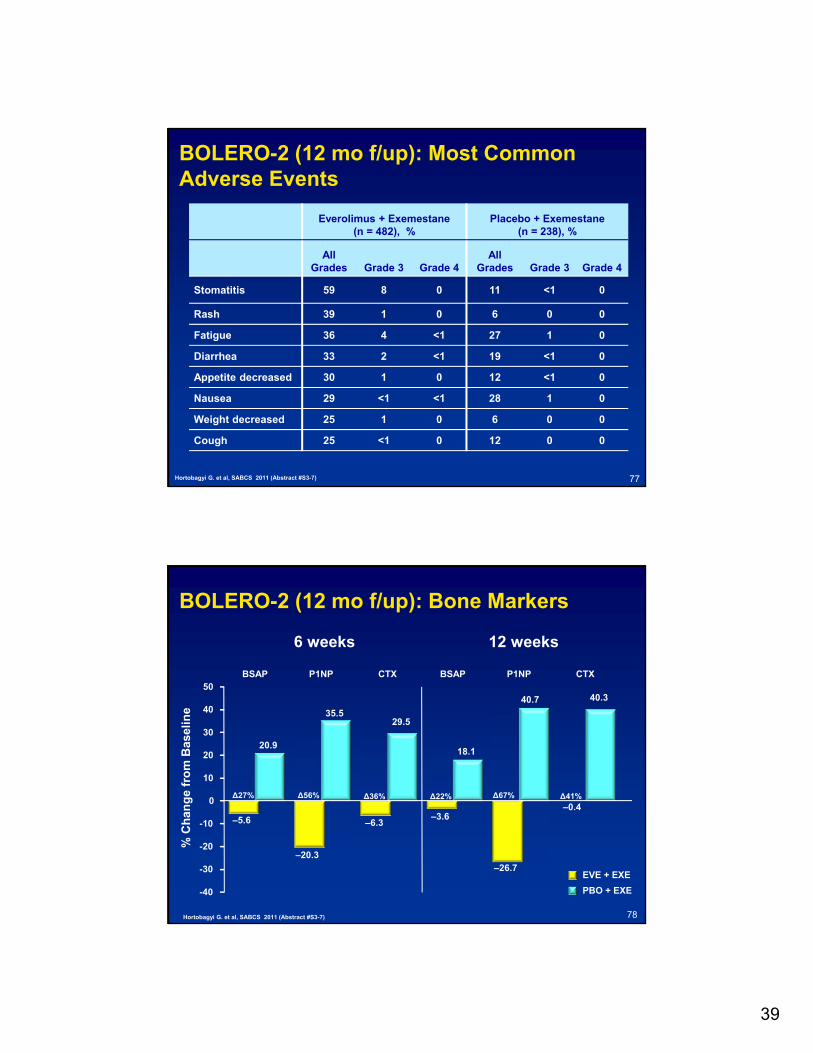
BOLERO-2 (12 mo f/up): Most Common Adverse Events
Everolimus + Exemestane (n = 482), %
Placebo + Exemestane (n = 238), %
All Grades Grade 3 Grade 4
All Grades Grade 3 Grade 4
Stomatitis 59 8 0 11 <1 0
Rash 39 1 0 6 0 0
Fatigue 36 4 <1 27 1 0
Diarrhea 33 2 <1 19 <1 0
Appetite decreased 30 1 0 12 <1 0
Nausea 29 <1 <1 28 1 0
Weight decreased 25 1 0 6 0 0
Cough 25 <1 0 12 0 0
77Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
BOLERO-2 (12 mo f/up): Bone Markers
78Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
% C
han
ge
fro
m B
asel
ine
–5.6
–20.3
–6.3–3.6
–26.7
–0.4
20.9
35.529.5
18.1
40.7 40.3
-40
-30
-20
-10
0
10
20
30
40
50BSAP P1NP CTX BSAP P1NP CTX
6 weeks 12 weeks
EVE + EXE
PBO + EXE
∆27% ∆56% ∆36% ∆22% ∆67% ∆41%
40
BOLERO-2 (12 mo f/up): Summary
• Addition of everolimus to exemestane prolongs PFS in patients with ER+ HER2- breast cancer refractory to non-steroidal aromatase inhibitors
– Local: median 7.4 vs 3.2 months, HR = 0.44, P < 1 x 10-16
– Bone resorption and formation markers increased in the exemestane arm, and decreased in the combination arm
– Toxicities: Mucositis and pneumonitis
79Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
BOLERO-2 (12 mo f/up): Summary
• Time to deterioration of QOL was similar in the two arms
• Bone resorption and formation markers increased in the exemestane arm, and decreased in the combination arm
• Adverse events are consistent with previous experience with everolimus
80Hortobagyi G. et al, SABCS 2011 (Abstract #S3-7)
41
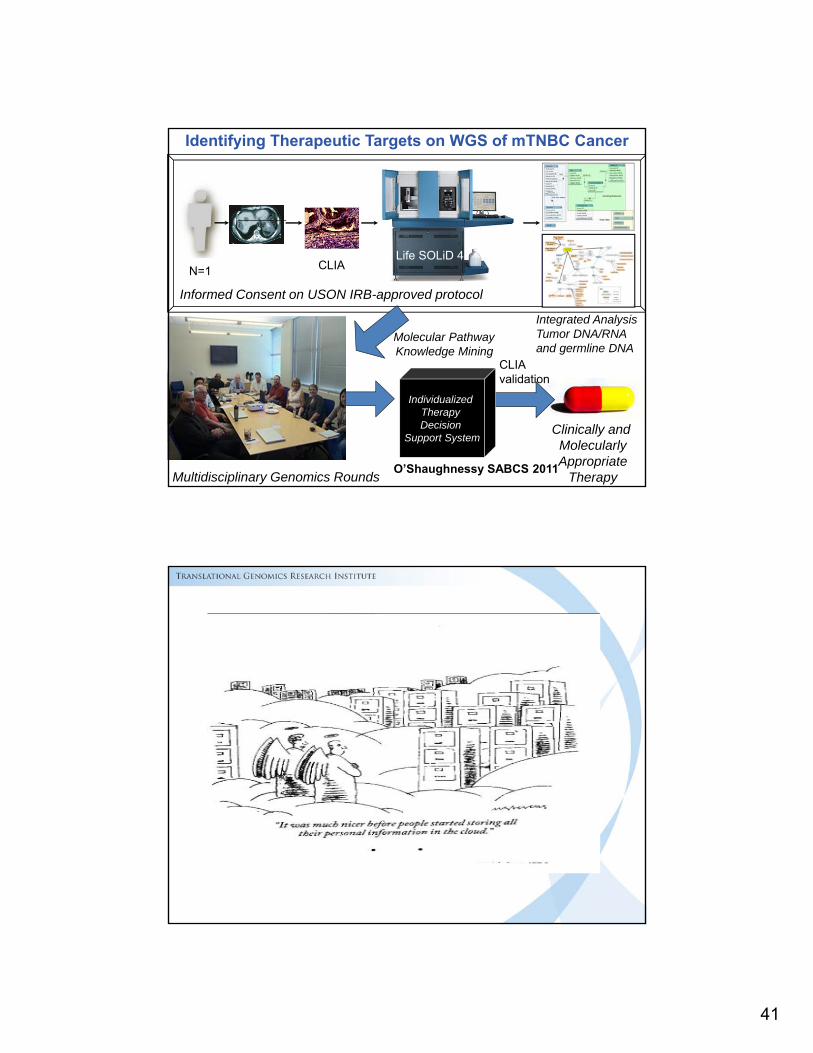
Individualized Therapy Decision
Support SystemClinically and MolecularlyAppropriate
TherapyMultidisciplinary Genomics Rounds
Molecular Pathway Knowledge Mining
Informed Consent on USON IRB-approved protocol
N=1 CLIA
CLIAvalidation
Identifying Therapeutic Targets on WGS of mTNBC Cancer
Integrated Analysis Tumor DNA/RNAand germline DNA
Life SOLiD 4
O’Shaughnessy SABCS 2011
42