Embed Size (px)
Citation preview

Spinal TractionSpinal Traction
Jennifer Doherty-Restrepo, ATC, LAT
Entry-Level Athletic Training Education Program
PET 4995: Therapeutic Modalities

TractionTraction
Process of drawing, or pulling apart, of a body segment
Mechanical Traction - using a traction machine or ropes/ pulleys to apply a traction force
Manual Traction - clinician positions patient and applies traction force to joints of the spine or extremities

Effects of Traction: Effects of Traction: SpineSpine
Encourages movement between Encourages movement between each individual spinal segment each individual spinal segment
Amount of movement varies Amount of movement varies according to…according to… Position of spine, Position of spine, Amount of force, and Amount of force, and Length of time the Length of time the
force is applied force is applied
Transient effectTransient effect

Effects of Traction: Effects of Traction: SpineSpine
pain, paresthesia, or tingling pain, paresthesia, or tingling Due to physical separation of vertebral Due to physical separation of vertebral
segments thus decreasing pressure on segments thus decreasing pressure on sensitive structuressensitive structures
As long as positive physiologic As long as positive physiologic effects occur, effects occur, traction should traction should be continued be continued

Effects ofof Traction: Bone
No immediate effects due to traction May result in increased spinal
movement that reverses bone weakness associated with immobilization
May assist with increasing or maintaining bone density

Effects ofof Traction: Ligaments
Stretching effect Structural changes occur slowly due to
viscoelastic properties Ligaments resist shear forces and return to
original form following removal of a deforming load
Sensitivity to rate of loading Ligament deformation results in
lengthening of a ligament caused by traction loading Slow loading rates allow for more
deformation

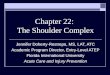
Effects ofof Traction: Disks
Normal disk in non-compressed position Internal pressure (indicated by arrows)
is exerted equally in all directions Internal annular fibers contain nuclear
materials

Effects ofof Traction: Disks
In an injured disk, sitting or standing compresses the disk causing the nucleus to become flatter
Pressure in this instance still remains relatively equal in all directions

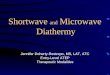
Effects ofof Traction: Disks
In an injured disk, movement in weight-bearing causes a horizontal shift in nuclear material
If this was forward bending, the bulge would occur in the posterior annular fibers Anterior annular fibers would be slackened and
narrow

Effects ofof Traction: Disks
Herniation of the nuclear material occurs if the annular wall becomes weak
Herniation may possibly put pressure on sensitive structures in the area

Effects ofof Traction: Disks
When placed under traction, intervertebral space expands thereby decreasing pressure on the disk
Taut annular fibers create a centripetally directed force Decreases herniation and pressure on sensitive
structures in the area

Effects ofof Traction: Articular Facet Joints
Facet joints are separated releasing impinged structures Dramatic reduction in symptoms
Joint separation decompresses articular cartilage allowing synovial fluid exchange to nourish cartilage Decreases rate of degenerative changes
Increased proprioception from facet joint structures provide sensation of pain relief

Effects ofof Traction: Muscles
Vertebral muscles can be stretched Initial stretch should come from body
positioning Stretch lengthens tight muscle Allows for better muscular blood flow Activates muscle proprioceptors
providing sensation of pain relief Gate Control Theory

Effects ofof Traction: Nerves
Focus of most traction treatments Pressure on nerves or nerve roots often
associated with spinal pain Unrelieved pressure on a nerve will
cause Slowing, eventual loss of impulse
conduction Motor weakness, numbness, and loss of
reflex Pain, tenderness, and muscular spasm

Traction Treatment Techniques
Lumbar Positional Traction Inversion traction
Manual Lumbar Traction Level-specific Unilateral leg pull
Mechanical Lumbar Traction Manual Cervical Traction Mechanical Cervical Traction

Lumbar Positional Traction
Patient typically on restricted activity program
“Trial and error” process to determine position that offers maximum comfort

Side-lying Position: Unilateral Foramen Opening Lateral Herniation
Patient leaning away from painful side
Lie painful side up Lie on right side
over blanket roll

Side-lying Position: Unilateral Foramen Opening Lateral Herniation
Patient leaning away from painful side
Lie painful side up Lie on right side
over blanket roll Medial Herniation
Patient leaning toward painful side
Lie painful side down
Lie on right side over blanket roll

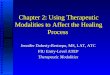
Side-lying Position: Unilateral Foramen Opening
Side-lying with a blanket roll between iliac crest and rib cage
Increases intervertebral foramen size of superior side of lumbar spine

Side-lying Position: Unilateral Foramen Opening
Maximum opening of intervertebral foramen
Achieved by flexing upper hip and knee and rotating shoulders in opposite directions
Maximum opening of left side

Supine Position: Bilateral Foramen Opening
Knees to chest position
increases size of lumbar intervertebral foramen bilaterally
Separation of spinous processes

Inversion Traction
Hang upside down Lengthens spinal
column due to stretch provided by weight of trunk
Repeat inversion 2-3 times
Observe for signs of vertigo, dizziness, or nausea

Manual Lumbar Traction
Used prior to mechanical traction Helps determine degree of lumbar
flexion, extension, or side-bending that is most comfortable
Most comfortable position is usually best therapeutic position

Level-Specific Manual Traction
Position patient for maximum effect at a specific spinal level
Lumbar spine flexed using upper leg as lever
Palpate interspinous space
Upper spinous process is where maximum effect is desired

Level-Specific Manual Traction
When motion of lower spinous process can be palpated, place foot against opposite leg to prevent further flexion
Trunk is then rotated toward the upper shoulder until motion of upper spinous process can be palpated

Level-Specific Manual Traction
Place chest against ASIS and upper hip
Lean toward patient’s feet
Use enough force to cause a palpable separation of the spinous processes at desired level

Unilateral Leg Pull Manual Traction
Hip joint problems or difficult lateral shift corrections
Thoracic counter-traction harness is used
Hold ankle and move hip into 30o flexion, 30o abduction, and full external rotation
Apply steady traction force until noticeable distraction occurs

Unilateral Leg Pull Manual Traction
Sacroiliac problems In addition to
thoracic counter-traction harness, strap is placed through groin and secured to table
Hold ankle and move hip into 30o flexion and 15o abduction
Apply steady traction force

Mechanical Lumbar Traction: Equipment Use split table to eliminate friction
between body segments Non-slip traction harness stabilizes trunk

Mechanical Lumbar Traction: Setup Pelvic harness
Applied while standing
Contact pads and upper belt placed at, or just above, iliac crest
Rib pads Positioned over
lower rib cage

Mechanical Lumbar Traction: Body Positioning
Neutral spinal position
Allows for largest intervertebral foramen opening before traction is applied
Usually position of choice whether prone or supine

Mechanical Lumbar Traction: Body Positioning
Flexion Increases
posterior opening Puts pressure on
disk nucleus to move posterior
Other soft tissue may also close foramen opening

Mechanical Lumbar Traction: Body Positioning
Extension Closes foramen
because bony arches come closer together

Mechanical Lumbar Traction: Body Positioning Prone position Used with normal to
slightly flattened lumbar lordosis
Best for disk protrusions Place pillows under
abdomen Other modalities may be
applied Allows for assessment of
spinous process separation

Mechanical Lumbar Traction: Body Positioning
Supine position Produces posterior intervertebral
separation Optimal at 90o hip flexion Unilateral pelvic traction recommended if
stronger force is desired Scoliosis, Unilateral joint
dysfunction, or Unilateral lumbar
muscle spasm

Traction Force
No lumbar vertebral separation will occur with traction forces less than 1/4 of body weight Effective traction force ranges between
65 and 200 pounds Traction force recommended = 1/2
body weight Must use progressive steps to
comfortably reach therapeutic loads

Intermittent vs. Sustained Traction
Intermittent Traction Effective for posterior intervertebral
separation No firm recommendations for on/off times
Sustained Traction Recommended for disk protrusion and
rupture

Treatment Duration
With suspected disk protrusions, total treatment time should be relatively short
10 minutes or less
If treatment reduces symptoms, treatment time should remain at 10 min or less
If the treatment is partially successful or unsuccessful in relieving symptoms, gradually increase time over several treatments up to 30 min

Progressive and Regressive Steps
Traction equipment may be built with progressive and regressive modes
Progressive mode Increases traction force in a pre-
selected number of steps Allows slow accommodation to traction
Regressive mode Decreases traction force in a pre-
selected number of steps
Patient comfort is primary consideration!

Manual Cervical Traction
Stretches muscles and joint structures Enlarges intervertebral spaces and foramen Creates centripetally directed forces on
disk and surrounding soft tissue Mobilizes vertebral joints Increases joint proprioception Relieves compressive effects of normal
posture Improves arterial, venous, and lymphatic
flow

Manual Cervical Traction
Variety of head and neck positions
Hand should cradle neck contacting one mastoid process
Other hand on chin Gentle pull, < 20 pounds Intermittent pull, 3 - 10
sec Treatment time, 3 - 10
min

Mechanical Cervical Traction
Supine Neck flexed 20 - 30o
Traction harness pulls on occiput
Intermittent pull > 20 pounds Minimum of 7 seconds Adequate rest time for
recovery
Treatment time, 20 - 25 min
Forces up to 50 pounds may produce increased intervertebral separation.

Mechanical Cervical Traction
Wall-mounted device Inexpensive
Static traction most easily employed Use weight plates, sand bags, or
water bags
Intermittent traction may be used
Sitting or prone Gentle pull, 10 - 20 pounds Treatment time, 20 - 25 min

Indications for Spinal Traction
Nerve root impingement
Disk herniation Spondylolisthesis Narrowing within
intervertebral foramen
Osteophyte formation
Degenerative joint diseases
Subacute pain
Joint hypomobility Discogenic pain Muscle spasm or
guarding Muscle strain Spinal ligament or
capsular contractures
Improvement in arterial, venous, and lymphatic flow

Contraindications for Spinal Traction
Acute sprains or strains
Acute inflammation Fractures Vertebral joint
instability Any condition in
which movement exacerbates existing problem
Bone diseases Osteoporosis Infections in bones
or joints Vascular conditions Pregnant females Cardiac or
pulmonary problems