Embed Size (px)
Citation preview

Project Name:
Grantee Organization:
Grantee Contact Information:
Primary Project Contact :
LEARNING QUESTION
Identify the Learning Question(s) your project addressed.
1. How do in-reach efforts that connect residents of board and care homes, single room occupancy
(SRO) hotels and unlicensed boarding houses to social and recreational opportunities in and
outside of the facility reduce social isolation and improve quality of life for isolated adults and
older adults with serious mental illness?
2. How does a place-based outreach program by trained peers to public locations in the
community, such as parks, coffee shops, and libraries where otherwise isolated persons may go,
be effective in reducing social isolation and increasing participation in mental health services
among isolated adults and older adults with serious mental illness?
3. How does a telephone- or telephone- and internet-based program that provides social
interaction and individual support reduce isolation among adults and older adults with serious
mental illness and lead to greater in-person social interaction over time?
1. Address your selected Learning Question(s) based on your project findings and final project
desired outcomes. Explain how your strategies address the learning question(s).
Our project used several strategies to obtain participants who receive special messages from SROs and
Board and Care homes, our first learning question. These strategies include: 1) passing out flyers to
locations where residents in these locations are likely to frequent; 2) direct emails to the facilities; 3)
partnering with social service agencies and providing groups at those sites; 4) providing presentations
and groups in a long term inpatient setting where individuals who get discharged are likely to return to
these settings; 5) outreaching to the homeless population who may one day resort to seek refuge in
these housing resources; 6) presenting to Saint Vincent De Paul Shelter; 7) presenting at Pacific Care
Senior Center; 8) presenting to Fairmont Partial Hospitalization Program, presenting to Villa Fairmont.
Initially, we envisioned providing individual services to people who responded to flyers and
presentations in board and care homes and SRO hotels; however we adjusted our strategy.
Our Program Manager considered the contexts of marching directly into board and care homes and SRO
and providing groups to be too unstable for our trainees who needed transition to peer support type of
experiences. Instead, she initiated the process of gaining visibility in the community and training via
general outreach to agencies and outreach to the homeless; then, once we started presentations and

got invited to conduct groups in more staffed and protective settings, our trainees ran groups and
initiated one on one relationships with individuals who were receptive.
Direct responses that we got from fliers were limited compared to the vast number of them that we
outputted; however, once with individuals who did respond we were able to use strategies from our
curriculum and personal experiences and once the relationship was built, they become willing to go on
outings with us. In several cases, providing one-on-one services resulted in a massive increase in the
participant’s willingness to partake in therapeutic activities available to them in the community. It was
also resulted in very good training experiences for out Specialists who learned a lot about how to
provide services under the tutelage of our Program Manager.
Our process of partnering with service agencies who serve these residents of SROs and Board and Care
homes was aided by completing presentations at conferences to gain exposure and making rounds at
agencies. Our presentations were so affective that initially all who were responsive to us invited to reach
their participants. By the time the grant was closing down, we got blitzed by these opportunities.
In following a one-on-one client we worked with in the community into a board and care center, we
were able to support the staff, help the individual maintain housing, and receive a referral from that
board and care. This was the only way we were able to in reach to a board and care; however, it
suggests that over time we may be able to have a significant impact in some board and care settings by
following the strategies outlined here.
We also believe that our time in inpatient settings and outreaching to the homeless involved
opportunities to plant seeds to let message receivers know they were not alone. Once homeless
individuals move indoors they may end up in SROs and board and care homes; additionally our
Specialists developed counseling skills sharing stories of hope to those who either are not willing to
receive services or who are waiting for services. Indeed within the message receiving population there
is often a great deal of self-stigma that prevents those isolated by reaching out, and this became
pronouncedly apparent in our experience. We found partnering with agencies and adding a valuable
service to be the most effective way to get the word out.
In addressing learning question two, we found that although two of our specialists had completed Best
Now, that what we were doing in asking peers to be mindful and open about experiences with psychosis
was so different, that we functioned not only as a service but also as a training program. Balancing
being open and public about “psychosis” with teaching professional and administrative skills was a
focus. Thus, outreaching into the community as a team and passing out flyers was a necessary step that
was very supportive to our Specialists as it did a lot to build confidence and decrease shame associated
with “psychosis.” Additionally, active process of training peers did a lot to add to their level of structure
and even, one might add recreation. Not only did they have more money to take care of themselves,
they were increasingly able to model being open and talk about their message experiences and they
enjoyed initiating relationships in the community. By demonstrating their own gains made they passed
on hope to those they served. This was especially meaningful in the homeless community. In fact,
several of our Specialists were continuing to struggle with housing issues throughout the period of the

grant and although the effects of this training opportunity might not be measured to the full extent that
it helped, spreading hope and heroism and a cultural view of the issues of “psychosis” did a lot of good
both in the community and in the training experience of our Specialists. It helped prepare them to be
presenters at agencies and ready them for group work.
There was a homeless individuals who came to our training sessions on Thursday Night and was
astounded by how helpful the group was to him, though he did not become a regular attender due to
the fact that we met late in the day, this is an example of some of the magic we were able to create
trolling through the community with cultural stories of hope providing benefit that is hard to measure.
However, to really move forward as professionals and obtain a regular clientele, once we developed as a
team we moved to presentations at conferences and then to agencies and we worked with people who
responded to us. We learned to use our stories in presentations and transitioned to transmitting group
facilitation skills we gained through training to individuals in the community. Then, we started getting
more referrals to work with people one-on-one.
When we first started outreach, we received warm line calls, many from individuals who considered
themselves “psychics” in the community who were interested in talking but not so much in services. As
our services developed, our phones became very important of the training and development of our staff
as professionals. We went out in teams and the teams often sought supervision and support from our
highly experienced Program Manager. Seeking out support in a responsible way helped us develop
professionally and as team members; and also benefited the community as our participants had a clear
sense that the team was behind the support they received. Thus, our Specialists modeled the use of
phones even early in training. Our Specialists then, as they began running groups in the community,
were expected to retain participants by calling individuals and to maintain participation and gently move
the group participation towards individual support and connecting with individuals over the phone
initially we addressed the third learning question and helped pave the way for our team to increase a
sense of social support and a promotion of social support. Indeed, responsible phone contact
complimented by caring greeting card outreach did a lot to maintain group participation and help
groups grow and thrive, particularly towards the close of the grant so much so that we will be able to
maintain these groups for a period extending beyond the period of the grant thanks to some money
received by PEERS. Additionally, we found that by keeping in phone contact several individuals who
were receiving our one on one support were interested in coming to our open Thursday Night Training
and had a major increase in receptiveness to social communication and contact.
2. Any other ideas or interventions employed to help decrease consumer isolation? Please explain.
We developed a strategy to of reaching out to less isolated message receivers who might be interested
in taking a training to help them learn to reach out to other message receivers. We did this in part to
add to the training of our peer specialists and in part to help individuals specialize in supporting those
with special messages. Advertising in the POCC, the Hearing Voices Network, and through PEERS
website we have held almost four twelve week series aimed at training those who attend how to
identify the universal aspects of their message experience (or “psychosis”) and use them to teach and
promote coping skills. We have found that many less isolated individuals do benefit astronomically from

this endeavor. Additionally, individuals who get introduced to us in the community; then have the
option of coming to this training group; on occasions when this happened in our project, the gains made
were really notable.
Also as was already mentioned, public presentations at conferences and at provider sites was an
extremely important strategy to reaching in towards people who are isolated in their treatment by the
fact that “psychosis” is not always seen and dealt with in community agencies and treatment. Indeed,
agencies are already doing notable work to reach out to those isolated, and we feel their efforts would
be greatly enhanced if they had components that acknowledged and addressed the concerns of those
who have experiences with “psychosis.” Much like our referrals increased when we started getting the
word out in agencies, so too will in reach efforts when Message Receivers are taught to see themselves
as a culture and reach out to others who remain isolated. In effect, part of what needs to be done is a
massive anti-stigma campaign within and outside the system. Much as there is a sense of self help in
addictions traditions, so too does there need to be that mentality in “psychosis” treatment. If this is
done the in reach efforts will follow. And our efforts among the homeless remain extremely important
as our Specialists have stressed and demonstrated.
PROGRAM DESIGN
3. What are the goals of the program?
The goal of the program is two-fold: 1) Help those individuals isolated by “psychosis” become motivated
to associate with each other and seek services that can help them integrate and engage in community
activities; and 2) use an experienced Program Manager and an innovative curriculum to prepare peer
specialists who have lived experience with “psychosis” to use that experience as an asset and get hired
onto service teams where they can effectively take the lead in connecting with those isolated by
“psychosis.” Ultimately we want to plant the seeds for creating an inclusive, local culture that teaches
people to accept and thrive in spite of their message experiences, where message receivers work to
support each other in succeeding in the community. In doing this the stigma of “psychosis” will be
markedly reduced and voluntary participation in the Hearing Voices Network will flourish
4. Describe the Program Design, including the essential program components (e.g., outreach &
engagement, interventions, treatment, evaluation, etc.)
The program is designed to train message receivers to be community builders and to help build a sense
of community for message receiving participants. The essential program components involve: training
about universal components of “psychosis” and coping skills; community outreach to build visibility;
teaching team building skills; gaining necessary administration skills; distributing flyers and selling the
program peer to peer; providing phone warm-line and tele-support; teaching public presentation and
story-telling skills; training in group facilitation that involves personal disclosure; providing public
presentations to service providers and family members; providing peer-to-peer via group facilitation;

and providing peer to peer with individuals in the community in teams, using a survey to evaluate the
impact of our work; and conducting field testing in collaboration with a family-centered program.
5. How did the program impact the population served by this project?
The program helped normalize the trauma-sensitive strategy of going toward experiences that make up
“psychosis” and using spiritual, cognitive, behavioral and collaborative skills led by individuals who can
demonstrate mastery of them to motivate isolated individuals to reduce self-stigma and join in
community. Indeed, often message receivers learn that it is not safe to discuss or socialize over their
symptoms because usually they will get punished for doing so. Learning that it is safe to discuss with
others who have been through similar experience is an extremely important step towards drawing
people out of isolation and inactivity. And finding ways to do this that teach recovery and social
rehabilitation skills is something that the curriculum helps with. Many people who learned about our
work supported us in field testing and expressed a desire to be more involved to spread the word. As
the grant writer, I heard many snippets of successes from many sources. For example in advertising for
qualitative interview with Stanford researcher, a respondent who I never had the opportunity to meet,
reported that the groups had revolutionized his sense of self in a way that he couldn’t wait to discuss
more. In the field study, I heard that a client who repeatedly refuse to have anything to do with our
outreach, had been inexplicably helped in a revolutionary way by that individual’s parent. This
individual, who now openly communicates with us, went through an unspoken transformation. An
individual who was nearly mute, internally preoccupied, restless, and angry in our Thursday Evening
training, heard the leader quote a rap lyric to teach a concept and started to talk about how he hears
rap lyrics. Now he has told his whole story. But what is most notable is that our services fit right into
what already exists in a way that empowered and motivated people. We were only successful in
reaching into one board and care, via following a one-on-one participant there and supporting the staff
there and receiving other referrals there. What this tell me is that it is clear that our strategies to reach
in would take a great deal of time, but that teaching others that they are dealing with a culture bears
the potential of impacting these environments. Additionally, we did the work in ways that planted seeds
in the homeless and hospitalized communities in addition to ways that are measurable because message
culture often involves these experiences.
Program Strategies 6. Describe the strategies, methods of implementation and timeframe.
We went through a rapid hiring process initially and got straight to work during the first four months.
The training from the curriculum ultimately lasted the duration of the grant: started with a review of the
curriculum which the specialists were willing to explore intellectually without sharing their personal
experiences. Also during these first four months as we completed a review of the curriculum, the office
was set up and organized and administration skills such as filling out our TT time cards and filling out
transportation reimbursement forms and the team worked to share one computer in a very small space.
Additionally the program manager worked extensively on team building and maintaining professional

expectations and boundaries and helping the team become visible in the community by going out and
learning where services are at, and initiating conversations with service providers. Moving around the
community as a team proved to be very important as it initiated willingness to be visible as message
receivers. We went to a Hearing Voices Network meeting to initiate collaboration.
During the next four months, the outreach phase, we trained with local peer Leaders reviewing the
curriculum and filling in stories for the different components of the “psychosis;” we learned
presentation skills with ongoing team building. We handed out flyers and had personal conversations
with people explaining the cultural view of the problem with individual message receivers we connected
with in homeless circumstances; with people who responded on a warm line to posted advertisements
at SROs and other community sites. We started our presentations at conferences. Professional skills
and administrative work was really a focus as well and the presentations in the community became a
feature of growth. We opened up the training to the community and completed it with significant shifts
in attendance, but we had a total of six-eight individuals graduate.
The next four months involved field work in which we started to learn how to be in one-on-one
relationships, and to make presentations to service providers while continuing to sort through team
dynamics and increased the scope of conference presentations. We started running groups at a few
supportive agencies while continuing outreach to homeless and persisted making presentations at
agencies to start up even more groups. We worked to establish trust with a particular one on one
relationship working in teams, bringing food from a food pantry and learned to reflect on our work with
the team and grow as professionals. Our referrals started to grow.
The final four months of the grant we completed series of groups in agencies and contacted individuals
we made connections with on the phone. We had a staff retreat. We continued with outreach to
homeless and we managed an influx of requests for presentations. We started to prepare for closure
and the hardships of this by focusing on gaining job interview and job search skills. We completed mock
interviews. We credited our Specialists for making volunteer efforts to get their name out and network,
for completing scholastic efforts, and for taking training opportunities that we provided. We focused on
measuring our success with a survey and a field test. We advertised for longer qualitative interviews
with a Stanford researcher. And we continued our training being open and resilient about our message
process and own struggles and using them to inspire disclosure and recovery in the regular participants
who continued to come and support us.
Target Subpopulation 7. Identify the subpopulation of isolated adult and / or older adult consumers for whom this
program was most effective. Please include age, culture/ ethnicity, language, and other factors.
How was this determined?
This program did our best to work with individuals who have experienced “psychosis” across cultural
divides. We carefully selected our staff so that we could be inclusive of youth and elders; male, female

and LGBT2S individuals; we provided cultural representatives from African American, Caucasian, Latino,
Chicano, Caribbean and immigrant communities. We made a specific effort to include Spanish speakers,
homeless, individuals with a history of incarceration, and those with differing spiritual backgrounds
including individuals accustomed to working with natural healers. Our broad reach was by design and
much of it was due to the development of a team that was experienced with a wide array of experience
and cultural determinants. Our Program Manager used the resources on our team to maximize
inclusion in a very diverse target population
The qualitative population that we sought to be effective with was people who had experienced
“psychosis” who were willing to talk about it and receive acknowledgement for belonging to an
oppressed culture that often does not get recognized. Once we were able to use our experience and
training to break through the isolation and invite people to be open and aware of the nature of
“psychosis” we found participants were usually motivated, like our Specialists, to improve their social
circumstances and enhance their social networks or engage in social rehabilitation. What we found
though was meeting people where they were at, even if they were already in treatment, wielded the
best results. Referrals took time as did the training of our staff to be ready for them and we tended to
take them as they come and in many ways we had to close down just as we were starting to rapidly
spread out.
Describe the involvement with BHCS stakeholders (e.g., clients/ consumers, family members, and
BHCS contracted providers).
In addition to message receivers, we also significantly served service providers and family members. We
found both interest groups very important to obtaining access to our message receiving population. We
had several family members who heard about us reach out and advocate for services for their younger
message receivers and we followed up with a family support group through one of our provider sites,
PREP. Additionally, the majority of our referrals came from successfully partnering with providers who
let us start up series of groups for their clients. In particular, these were successful and grew when
participants were already in program or the hospital and could chose to have these groups in addition to
other services. In these cases the groups really took off and the groups grew and remained strong. In
situations where group members were asked to come in particularly for our groups, we were successful
when we had support from the agency and followed up with phone contact (as happened at PREP.)
In the field testing, providers gave us mostly positive feedback and were only concerned about issues as
to whether services like this would take off, whether they were publicized enough, and whether more
could have been accomplished in the presentation to teach more about the practice. There seemed to
be no doubt that these kinds of innovations were necessary in the system. A Ph.D. from La Clinical
actually gave us the exceptional compliment that we were essentially creating a modern effort to return
to affective indigenous ways of working with madness.
We included consumers by hiring peers, and advertising through the POCC for our jobs and for our
facilitator training. In the facilitator training, we got a significant number of providers and peer leaders
as well. We also included the providers and consumers by speaking at a number of conferences such as

the ACNMHC 25th Anniversary, the Spirituality Conference, CASRA, CIIS Spiritual Emergence group, Heart
and Soul Consumer group, and the POCC Conference. Additionally as stated above we provided
provider trainings and peer to peer groups at four sites. In the field testing, Consumers were more
communicative with us in terms of providing us with critical feedback and pointing out that this
information needs to permeate throughout our social institutions, including schools.
We also worked with ten family members most of who we have met through PREP collaborating with
them to enhance the success of our participants. We also partnered with a family focused innovations
grant program for the field testing to reach family networks and get their feedback. A family advocate
from PREP gave us compliments at the field testing event, but was very concerned that our work was
shutting down; an associate of the grant writer, she pointed out that continuing the work in the
agencies needed to be his top priority. We did have five family members we worked with come and
support our Field testing and they provided feedback: that we would benefit from establishing scientific
proof of our work, and that we needed to include hospice clientele because many message receiving
individual’s die alone. Additionally, one of the parents was very complementary of the work we did with
her son.
8. How are the strategies culturally responsive to the target population?
The training that the grant writer brought into this work is essentially an effort to acculturate individuals
who have had experiences with “psychosis” across diagnostic categories and cultural divides, teaching
them to belong to and identify with universal components of these experiences. Essentially the grant
writer has identified eight components of “psychosis” that lead to common processes and experiences
that once disclosed, that message receiving individual can relate to. By emphasizing what they have in
common with others instead of how different their experiences are, individuals can work with each
other to emphasize solutions and live successfully with some degree of social rehabilitation.
Additionally, using peer role models and bringing people together in various stages of recovery and a
variety of walks of life is important so that message receivers can see that what is happening to them is
in fact happening to others in different cultural contexts. The ability of a worker to say: “I’ve
experienced this, in fact I still experience this,” is so essential to motivating individuals who are in
isolation to try new things and make the monumental efforts to promote their own social rehabilitation.
The challenge is that each participant has unique cultural characteristics which is exactly why we tried to
pick individuals with powerful lived experience who represented distinct aspects of cultural experience.
The ability to connect with others by going towards “psychosis” and making collective meaning of it is
such an important need that doesn’t exist in treatment as we currently engage in it. A great deal of
isolation will be reduced if we can simply destigmatize the collection of associated experiences and add
this to our treatment protocols. Additionally, it might be noted that the material was developed among
individuals who largely populate board and care homes and SRO facilities and was rearranged based on
the learning that happened from the participants in the project.
Effectiveness of Strategies

9. How do you know these strategies are effective in achieving the goal of reducing isolation for the
target population?
We feel that this strategy works because we were able to reach so many participants and witness first-
hand significant growth. Admittedly, early in the grant we focused a lot on training and development to
be successful and on bringing in referrals and partnering with family members and providers. But once
we were ready, we served a lot of individuals with the simple message that the problem needs to be
redefined and that isolation is largely caused by having the experiences of “psychosis” coercively
suppressed. Some we touched briefly, and some we touched more intensively. In total we reached: 54
individuals out in the community and many through opening up our training to the community. We
consider the number of people we served one-on one to be: 9; and the number in group to be 45. Add
to this the 26 individuals who were willing to come and contribute to our field testing. And sixty
providers who heard our presentations, 10 parents whose youth we worked with, many dozens of
individuals who heard us speak at conferences, and a high number of homeless individuals we reached
out to on the streets and you get a feel for the scope and effectiveness of our work.
We feel that our success rate is demonstrated not only by these numbers but also by qualitative
comments and individual experiences with satisfied individuals who were willing to open up and share
their most private experiences with us. Much of this happened in confidential groups and involved the
telling of stories of Special Messages Crisis, the most powerful healing determinant, in my opinion, and
the hardest thing to document.
Additionally, we feel that the growth we have observed in our staff. In particular, our peer specialists
grew in their ability to be transparent about their psychosis experience while at the same time making
gains in being professional, public and less isolated is a testament to the practice. At the end of the
grant, all of our workers were encouraged to take their learning and move forward in career directions
they chose themselves and all were able to sustain career growth in terms of volunteer or getting hired.
One of our workers obtained a full time position outside the field. Another got hired on at PEERS.
Others are gaining volunteer positions and one got a contract position with the county. Additionally the
growth in the Project Manager and Grant Writer in their ability to work with each other across cultural
divides, learn to coordinate their roles, trust and cooperation has been significant. This relationship has
clearly been strained perhaps because so much responsibility has fallen on the Program Manager, who
has been the anchor and driving force of the project; and perhaps because each socially rehabilitated
individual has very different sets of strengths and survival skills. It has been each of our drive and
determination to help our culture that has helped us, both strained by intense schedules, to work
together for the good of the grant. Speaking for myself, I, the Grant Writer, feel I have learned a great
deal from this relationship. I have been forced to grow and develop new skills and abilities that I would
not have otherwise gained. And I hope when the dust settles that the feeling is mutual.
10. Describe the process for arriving at the Program Design supported by evidence-based or
community defined best practice findings.
Much of the success of this as a treatment strategy has been observed by the successful running of
groups at Highland Hospital Outpatient Psychiatric Unit over the past six years and the known successes
of the Hearing Voices Network across European Nations. Much of the qualitative observations that
inform this work have been documented in the grant writer’s personal time. Though this has also
involved an inductive process, the efforts of this grant have been to see if these experiences can play out
in the wider community in a successful manner.
Additionally, a problem oriented path for counseling theory as has been started by the eclectic
approaches of the evidence based DBT has been a large personal motivator to creating such a system for
“psychosis.” In fact, making the curriculum both trauma and spiritually sensitive is part of the work,
much as Marsh Linnehan has done with DBT.
Another major aspect of what we have done has been pioneered by our Program Manager, which
involves a training program that teaches professional development to individuals who have experienced
catastrophic loss, trauma and isolation as a result of their Special Message Process. Much of this is built
on her inductive strategies for professional survival and her strong work has resulted in enormous
growth for our Specialists. The Program Manager identified the needs of Specialists and created very
amazing teaching and learning experiences to foster such growth. Some small examples of all of her
monumental work is her decisions to create a sense of visibility by moving through the community as a
unified team and her initiative in focusing on job development at the end of the grant. There were so
many wise and affective strategies employed that I documented under the project design, I was only
able to document the decisions and the leadership that she brought to the project.
Also there has been significant work done to make peer support a best practice that has influenced the
hiring and training of the Specialists. Grant writer, has been through WRAP and PET provided by Mary
Ellen Copeland and Lori Ashcroft and seen the power of “I am the evidence,” stories that serve to
motivate not only the audience but also the speaker. And as the Program Manager implemented the
very important community practice of reflection, I heard Specialists talk about how sharing their stories
with homeless helped monumentally spread hope and add to personal commitments to wellness for our
Specialists who were underpaid (in my opinion) and endured much through our eighteen months
together.
11. Provide quantitative and qualitative data that show the effectiveness of the strategies. Include
assessment tools and measures of effectiveness and data sources used.
We made a formal effort to measure success qualitatively and quantitatively by utilizing a Stanford
researcher who sought to support us. Initially, the qualitative interviews that would have involved 1-1/2
hour sessions reimbursed with twenty dollars resulted in only three responses after dispersing fliers
throughout the people we supported. By the time we observed that this response was not going to give
us an accurate reflection of our work we decided to send out a survey to those who participated in
events to let them identify how they were positively affected. Unfortunately, because of the intense
amount of work that piled up completing the field testing and closing down the effort, this effort

wielded only 19 responses, but we still feel this is significant. And the results and survey are duplicated
below.
I does stand to be noted that it was observed that many message receivers had an aversion to
completing the surveys. The surveys were seven pages long and appeared to be great measures,
however, some message receivers may have an aversion to filling out an entire survey because of a
variety of reasons that include focus and tolerance of the task and perhaps mixed feelings about or
willingness to be part of a study.
The grant writer is responsible for initiating this measuring process late in the course of the grant and
acknowledges responsibility for getting a late start. Grant writer’s desire was to provide quality service
and change lives more so than quantitative measuring of the impact; and this admittedly reflects some
of his own ambivalence about the role of research.
It is also arguable that the numbers in terms of the amount of participants and the success and
increasing demand for the service that is documented above is a powerful measure of our success. We
have worked hard locally and learned that the best way to battle the self-stigma is to provide groups in
addition to services that are otherwise being applied and follow up with one-on-one support. We have
learned that we can train amazing individuals who can develop and socially rehabilitate and effectively
cut through the stigma and develop special relationships. We feel they would be an excellent addition
to service teams.
Finally our two field tests yielded strong and supportive results. Out of 26 attendees, there were 11
providers from: HHREC, BACS, PREP, the Liberation Institute, Telecare, La Familia, Center for Family
Counseling, and FERC. We also hosted 10 consumers with a variety of affiliations, and 5 family
members. We received the most positive feedback from Providers who were primarily complimentary
and concerned about whether these services will be able to stay in the community, given the limitations
of the grant. Consumers had a little more to say and were a little more critical, wanting to see the
information inserted into schools and church settings along with being taught to providers. And family
members wanted scientific proof and to see the service expanded to include hospice programs.
Below is the report prepared by our Stanford Researcher:
SUMMARY FINDINGS
POST-INTERVENTION SURVEY: ALAMEDA COUNTY SPECIAL MESSAGES PROJECT
Description & Methods

In order to better understand the impact of client participation in the Special Messages (SM)
project, we administered an online survey to clients following participation in one or more SM activities
(including trainings, support groups and one-on-one consultations). The survey combined novel and
adapted close-ended questions as well as optional open-ended questions. Attempts were made to
reach both past and current SM clients as well as clinicians and family members.
Survey Participants
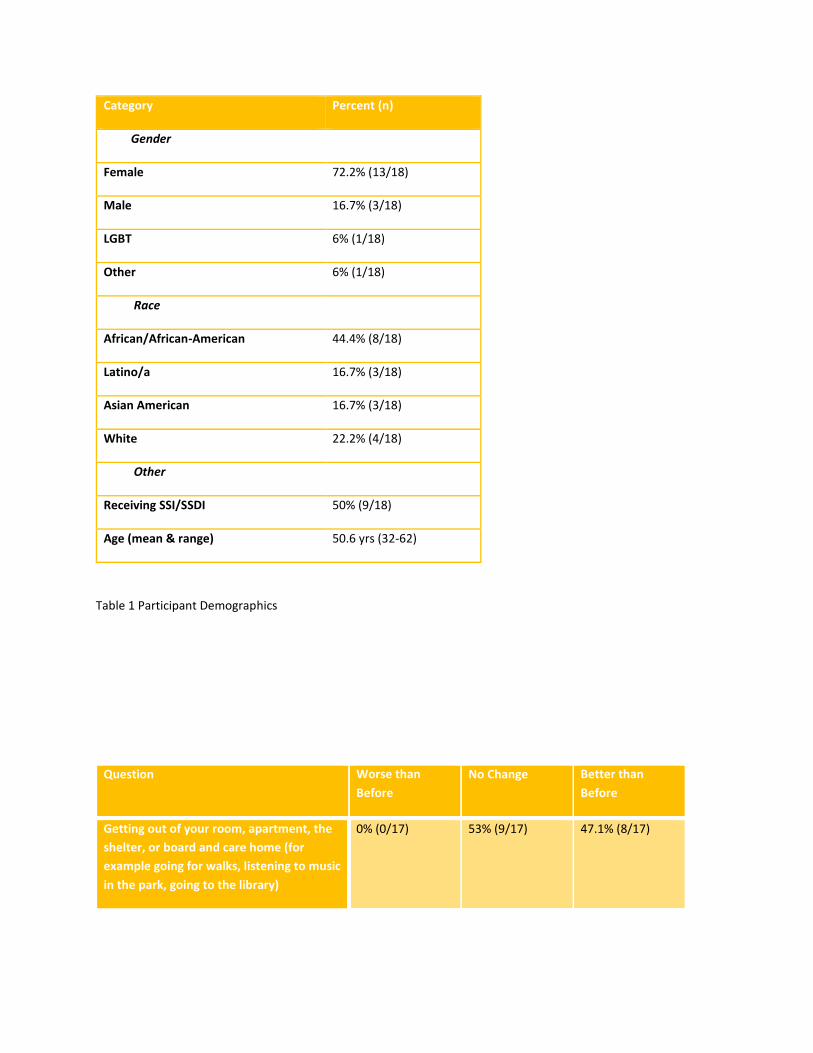
In total, 18 participants completed a post-intervention survey regarding their experiences. Participants
included one clinician, one family member, and one friend in addition to 15 peers. 11/15 peers were
directly involved in SM groups and/or 1:1 meetings and the remainder had attended a training or
workshop. See Table 1 for additional participant demographics.
Survey Highlights: Impact
For the full sample, including participants who had attended a presentation or training but not
participated directly in a SM services, the majority of participants reported improvement in one or
more community engagement or recovery domain. Individual items ranged from 6/17 (35%) of
participants reporting a diminished sense of “not fitting in” to 13/17 (76.5%) reporting increased
communication or connection with friends and/or peers. See Table 3 for full results.
Of those participants who were involved in a Special Messages group and/or met one-on-one with SM
staff, 10/10 (100%; 1 missing) reported improvement in one or more community engagement or
recovery domains. For example, 9/10 (90%) reported increases in time spent “talking to or connecting
with friends or peers” and 8/10 (80%) increased time “reflecting on [their] experiences of psychosis in a
helpful way.” Only 1/11 (10%) participants reported negative changes post-contact (including increased
loneliness and feelings of not fitting in). See table 4 for full results.
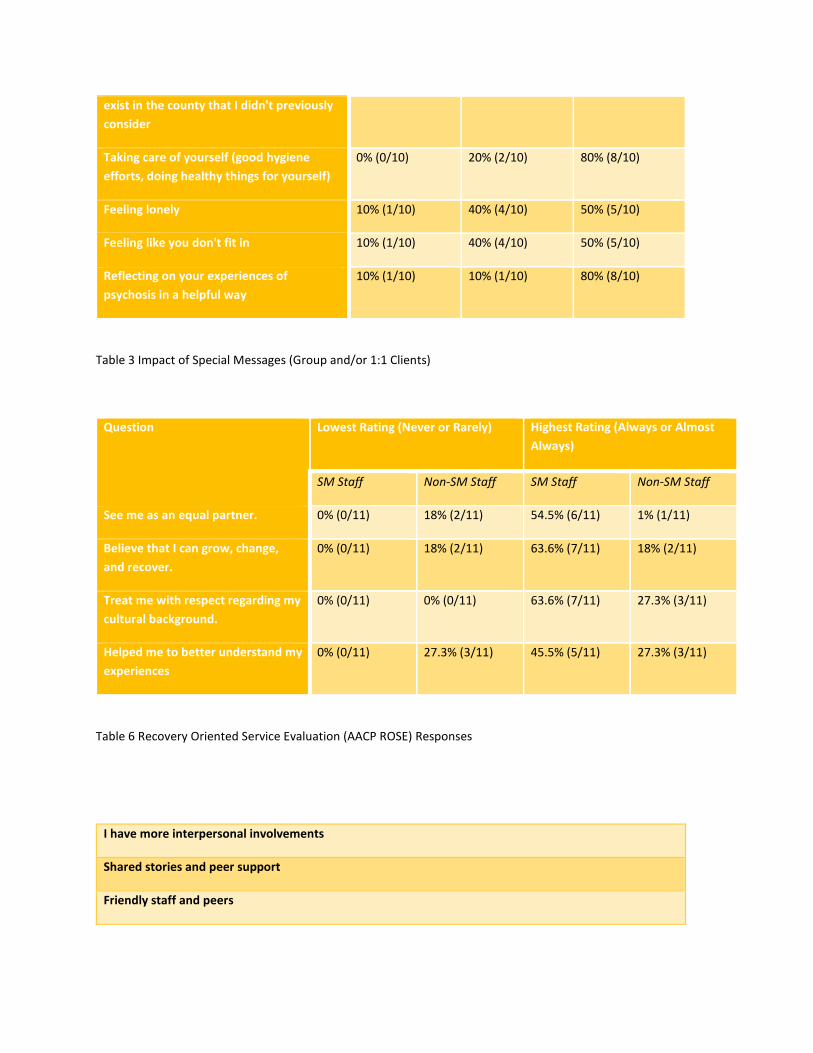
Survey Highlights: Comparing Special Messages Peer Staff with Non-SM Community Mental Health
Staff
While the differences in participants’ experiences of the recovery-orientation of SM staff and non-SM
community mental health staff did not reach statistical significance (almost certainly due to the sample

size; data was missing for 8 participants), ratings of SM staff exceeded those of non-SM staff on every
item (e.g. “staff see me as an equal partner;” “staff believe that I can grow, change and recovery;”
“staff have helped me to better understand my experiences of psychosis”). On the 4 staff-focused
questions taken from the American Association of Community Psychiatry’s Recovery Oriented Service
Evaluation (AACP ROSE), 20-30% (2-3 out of 10) of participants consistently listed non-SM staff as never
or rarely engaging in recovery-oriented behaviors, while no (0%) SM staff were listed as never or rarely
engaging in the same behaviors. The highest ratings were assigned to SM staff at consistently higher
rates. For instance, 6/10 (60%) participants listed SM staff as “always or almost always” ‘seeing them
as an equal partner’ whereas only 1/10 (10%) gave non-SM staff the same rating. See Table 4 for
additional details.
Qualitative (Open Ended) Responses
All comments regarding additional perceptions of participation in SM activities are listed in
Tables 5 and 6. Overall, open-ended responses suggest that at least some participants felt that SM
activities increased their sense of self-worth and validated their experiences in additional to more
interpersonal and/or community and treatment-focused effects.
Limitations & Conclusions
Participant sample size was limited and it is consequently unclear how the responses reported
here generalize to the full population of clients who came in contact with Special Messages (SM). It is
also possible that participants with a more favorable impression of SM were more likely to complete the
survey. In addition, our survey was cross-sectional and lacked a control group limiting our ability to
make strong claims about intervention effects. We nevertheless see the survey as helping establish the
feasibility of the SM project and participants’ favorable views.
For those who filled out the survey, results suggest that SM was generally perceived as effective
in reducing isolation and increasing personal and community engagement and well-liked by
participants. In addition, comparisons between SM and non-SM staff using the Recovery Oriented
Services Evaluation (AACP ROSE), suggest that SM staff were more likely to be perceived as strongly
recovery-oriented than non-SM staff.
Category Percent (n)
Gender
Female 72.2% (13/18)
Male 16.7% (3/18)
LGBT 6% (1/18)
Other 6% (1/18)
Race
African/African-American 44.4% (8/18)
Latino/a 16.7% (3/18)
Asian American 16.7% (3/18)
White 22.2% (4/18)
Other
Receiving SSI/SSDI 50% (9/18)
Age (mean & range) 50.6 yrs (32-62)
Table 1 Participant Demographics
Question Worse than
Before
No Change Better than
Before
Getting out of your room, apartment, the
shelter, or board and care home (for
example going for walks, listening to music
in the park, going to the library)
0% (0/17) 53% (9/17) 47.1% (8/17)

Talking to or connecting with members of
your family
0% (0/17) 64.7% (11/17) 35.3% (6/17)
Talking to or connecting with friends or
peers
0% (0/17) 23.5% (4/17) 76.5% (13/17)
Feeling like you're part of a community of
people with shared experiences
0% (0/17) 47.1% (8/17) 53% (9/17)
Feeling optimistic about the future and
open to explore the other services that
exist in the county that I didn't previously
consider
11.8% (2/17) 29.4% (5/17) 58.8% (10/17)
Taking care of yourself (good hygiene
efforts, doing healthy things for yourself)
0% (0/17) 47.1% (8/17) 53% (9/17)
Feeling lonely 6% (1/17) 53% (9/17) 41.2% (7/17)
Feeling like you don't fit in 11.8% (2/17) 53% (9/17) 35.3% (6/17)
Reflecting on your experiences of
psychosis in a helpful way
6% (1/17) 41.2% (7/17) 53% (9/17)
Table 2 Impact of Special Messages (Full Sample)
Question Worse than
Before
No Change Better than
Before
Getting out of your room, apartment, the
shelter, or board and care home (for
example going for walks, listening to music
in the park, going to the library)
0% (0/10) 30% (3/10) 70% (7/10)
Talking to or connecting with members of
your family
0% (0/10) 60% (6/10) 40% (4/10)
Talking to or connecting with friends or
peers
0% (0/10) 10% (1/10) 90% (9/10)
Feeling like you're part of a community of
people with shared experiences
(0/10) 30% (3/10) 70% (7/10)
Feeling optimistic about the future and
open to explore the other services that
10% (1/10) 20% (2/10) 70% (7/10)
exist in the county that I didn't previously
consider
Taking care of yourself (good hygiene
efforts, doing healthy things for yourself)
0% (0/10) 20% (2/10) 80% (8/10)
Feeling lonely 10% (1/10) 40% (4/10) 50% (5/10)
Feeling like you don't fit in 10% (1/10) 40% (4/10) 50% (5/10)
Reflecting on your experiences of
psychosis in a helpful way
10% (1/10) 10% (1/10) 80% (8/10)
Table 3 Impact of Special Messages (Group and/or 1:1 Clients)
Question Lowest Rating (Never or Rarely) Highest Rating (Always or Almost
Always)
SM Staff Non-SM Staff SM Staff Non-SM Staff
See me as an equal partner. 0% (0/11) 18% (2/11) 54.5% (6/11) 1% (1/11)
Believe that I can grow, change,
and recover.
0% (0/11) 18% (2/11) 63.6% (7/11) 18% (2/11)
Treat me with respect regarding my
cultural background.
0% (0/11) 0% (0/11) 63.6% (7/11) 27.3% (3/11)
Helped me to better understand my
experiences
0% (0/11) 27.3% (3/11) 45.5% (5/11) 27.3% (3/11)
Table 6 Recovery Oriented Service Evaluation (AACP ROSE) Responses
I have more interpersonal involvements
Shared stories and peer support
Friendly staff and peers

My son has been visited by Special Messages. I believe it helped him to feel valued and validated by
speaking to a peer.
This information was not aimed at me. However, I very much appreciated the message that my clients
received from it.
I completed the certification course for special message facilitator
It helped me to validate my message experiences, as well as help me feel more worthwhile. Like I am so
much more capable than I thought I was. It has introduced me to other who understand my
experiences. It has given me hope for the future.it has expanded my viewpoint
Listening the examples you provided made me realize that I was getting some messages too. It was
good because I never thought that way and thought it was just me. It's good to know that this is
something.
Table 5 Additional Benefits of Involvement in Special Messages (Open Ended Responses)
I would like to add that I believe that Special Measures is an organization that is extremely valuable.
There are studies showing peer to peer contact as a portal to recovery.
Special Messages did help to relationships with others, but even more important it helped with self-
esteem and relationship with self. It is difficult to overcome internalized self stigma and Special
Messages is one of the few approaches that really helps.
I’m so glad I was a part of this
I really enjoyed the program.
I just want to say that it is a good program but you looking in the wrong places for individuals in
messages and who are isolated. You need to penetrate the many board and care homes in this county
and beyond. There is where you will the people who need this program the most and would respond to
it the best. Not in the streets or in the parks, Those people are out and about. But the board and care
homes, that is where the peers need the support of peers who understand them. whatever happens,
remember my words. Board and Cares and the recently released peers. from the hospitals needs to be
the focus.
Special Messages has provided an invaluable service to people who receive messages, as well as their
families/caregivers. I have witnessed a young man who was completely disengaged except for showing
up. After about 4-5 weeks of attendance he began saying hi and making eye contact. I have also
witnessed him laughing and engaging with other people more regularly.
Table 6 Additional Comments on Special Messages (Open Ended Responses)

Program Replication 12. What are your recommendations for program replication, including essential elements for
successful replication?
I would recommend that there be two full time leads for the project: one Peer Support and Approach
Trainer; and one Administrative Project Manager. I think it would be good if they both worked under a
Director who was there to support and hold meetings helping to communicate and balance their roles.
Differentiation of these two roles from the beginning and respect for the need for both roles is
important and an ability for each to validate and support each other will result in optimal team
dynamics. For example, the two roles need to be able to share validation and challenge strategies for
the Outreach Specialists. In other word there needs to be a sense of balance so that the Specialist get
challenged to adapt to a professional environment but also feel seen and understood as to where they
are. Thus, the two leads would need to work together to achieve such a balance: one teaching how to
be a vulnerable and authentic peer supporter, and one teaching professional skills standards and
maintaining hierarchy and expectations. This is essentially what we worked with; however, I, the
Approach Trainer, was not available full time and a lot of my, would be, duties were assumed by the
Program Manager which ultimately resulted in a hard relationship.
Additionally, we raced to get started and hire Specialists, and although the hires were good, a sense of
hurry and the differing skills needed for training were not taken into account; and that wasn’t a fair start
for the Manager. Time needs to be taken for each leader to develop a relationship and understand each
other’s’ skills and strengths. And it needs to be clearly understood that time is necessary to train the
staff to be visible in the community as representing “psychosis.” This was an innovation established by
the Program Manager and is vital to the success of the program that I, the grant writer, may not have
supported enough. While hitting the ground running the way we did helped us accomplish an enormous
amount, there was tension and conflict because the two roles were not well defined and there was no
time devoted to relationship development. The Approach Leader role was not defined well enough and
needed to include more hands on experience in setting up the office and in being in relationship with
the Specialists in the field. Additionally, the project at sometimes strained because the Approach Leader
was tired at the end of an intense day and not fresh to address important aspects of peer support and
be in relationship with all the staff.
An important element that we had to work with is having a high tolerance for each other and a flexible
way of addressing unprofessional behavior. This is not to say that all Specialists were always
unprofessional, but there was a lot of healing that understandably needed to be done. Choosing people
who are already healed may have limited important aspects of the peer element. Additionally, our high

level of cultural diversity also made it necessary for differing strengths and perspectives on
professionalism to be taken into account so that one culture did not dominate or result in unfair
treatment. As a result of this, we approached these relationships with a failure is not an option attitude
and this is pertinent because of the vast amount of social vulnerability that our Specialists had starting
out. We viewed this as a cultural trait that is often the result of a background of catastrophic loss or
hardship that we have all experienced. The discipline and direction needs to be there and
communicated, but poor performance would be optimally managed by not promoting or requiring more
time, not by exclusion. Relapse into Message Crisis needs to not result in job loss but wellness time off
and support. Investing in people and holding faith that they can transition into professional behavior is
essential and was well managed.
Also ongoing supportive training was essential in which our Specialists had the opportunity to be
vulnerable without reprise, referencing their struggles with messages and demonstrating to community
participants that this kind of stress can be authentically managed and overcome. Especially in the end of
the grant, the Specialists needed to express their upcoming loss and work through separation and
simultaneously keep up professional growth supported in getting them their next position. Since the
training was run by the employer it took a long time for Specialists to open up and share stories, but as
they did they were able to improve their professionalism. Hence, the need for two different types of
leaders. Ideally, however, the training would be at a more convenient hour to encourage participants
that specialists work with to come and decrease their isolation and learn more about the training. This
enables the Specialist to balance leading and participating openly.
Although our crew had a sense of pride making due with a very small space and just one computer, many operating costs proved to be smaller than anticipated and I would definitely recommend having a larger space and more computer availability. There were times when staff conflicts were resolved simply by spreading out into space that was temporarily available at PEERS. It was a lot to ask for a workforce of five to be crowded into a very small office and I would definitely recommend doing this differently. Finally, outsourcing training opportunities which we did intensely towards the end of the project, might
have been better spaced out throughout the duration of the grant and can be seen as important
professional development opportunities. In the case of our grant, I was not experienced with running a
budget and the Program Manager was; it would have been better if both worked together and spaced
out training opportunities throughout the duration of the grant. At the same time there was a lot to
accomplish and there was strain.
Additionally measurement of the effectiveness of services needs to either be initiated earlier in the
process or there needs to be more time in the project to collect it. Because quantitative measurements
will be viewed with scrutiny it is important to first establish trust and then, more time is required to
really get those results. It is my hope the reader will see that the training and team development were
absolutely necessary before the implementation of services, but that more time is needed to obtain
quantitative surveys. Even reimbursed qualitative interviews are likely to be viewed with scrutiny due to
stigma and mixed feelings about opening up and sharing cultural experiences. I feel we put the
participant and participant’s success and am personally proud that we took that tact.

13. Identify staffing requirements:
a) Job title; b) Role/ responsibilities with Full Time Employment (FTE);
Program Manager: Roles and Responsibilities:
Oversee the search for isolated individuals who have experienced “psychosis” via interfacing with and outreaching to community agencies
Uphold a sense of professional expectations for the project that helps staff develop and reach their full potential
Adjust the initial vision of the program so that it reflects the strengths of project personnel and the community response.
Create innovative, strength based professional development trainings that help individuals work with each other in a diverse work setting
Responsible for implementing disciplinary action so that employees have the opportunity to optimize their professional capacity in a safe environment.
Responsible for overseeing and training for time tracking efforts and communicating with business manager over payroll issues
Document and maintain bi-monthly individual supervision with Outreach specialists to assist with professional development.
Able to use and provide supportive feedback for presentation skills.
Able to track the budget and make decisions about where and when resources will be allocated
Organize an office and lead documentation efforts aimed at recording outreach efforts, group participation, and individual support services.
Create outreach strategies to help market the project
Create and disperse flyers that can prompt engagement
Lead safe groups in which stories of experiences in “psychosis” can be demonstrated and reflected upon in order to prompt others to tell stories about their experiences in “psychosis”
Teach group facilitation Skills
Shadow training and lead group supervision.
Ability to accompany Outreach Specialists and provide leadership support.
Seek feedback and support and work collaboratively with the Approach Trainer
Exemplify professional conduct and communication respecting all team members and their diverse backgrounds.
Approach Trainer: Roles and Responsibilities:
Responsible for knowing and be able to teach and adjust the curriculum in training groups that involve the Outreach Specialists and Community Collaborators
Use and exemplify use of their own story in working mutually with Outreach Specialists and Community Partners
Travel with the Outreach Specialists and model good boundaries, yet transparency, authenticity, and mutuality in Peer Support
Provide weekly individual supervision that is supportive but that upholds the professional expectations set by the Program Manager

Support and help develop Specialists innovative ideas and represent them in meetings with the Program Manager and Director.
Create quantitative and qualitative means for measuring the success of the program
Work collaboratively with Program Manager to represent concerns of the Specialists yet have a willingness to support and enforce professional expectations created by the Program Manager.
Help problem solve with regard to disciplinary actions and help make sure professional development occur
Lead presentations aimed at educating providers, residential providers and a wide array of community partners towards a cultural view of “psychosis.”
Seek mediation and function as a mediator when staff conflicts impede the progress of the project
Provide and lead safe training sessions aimed at reconstructing and telling stories about experiences with “psychosis” exemplifying leadership and meaningful reflection.
Inspire individuals to create innovative ways to connect with individuals when they are in “psychosis”
Help address diversity issues in a fair and equitable manner having respect for differences.
Responsible for writing project reports and overseeing writing projects associated with our
marketing campaign.
Responsible for knowing the local system and helping Project Manager make contact with
individuals who can make events happen.
Work with Project Manager to establish safety, structure and rules that are appropriate for a
diverse team
Outreach Specialists Roles and Responsibilities:
Willingness to reflect and represent lived experience with “psychosis”
Ability to participate and contribute to training that seeks to redefine psychosis
Learn administrative skills and function as a collaborative team member
Accept the professional direction of the Program Manager
Learn and teach peer support outreach with support Approach Trainer
Ability to meet professional expectations while learning to authentically relate your story and hardships
Support Community presentations with an ability to represent personal story
Structure own time and use phone to track participants and encourage them out to events
Invite participants eventually to communicate about “psychosis” and come to support groups aimed at that very task.
Learn to Lead support groups and outreach to individuals on a team
b) Required qualifications, certification and / or licensure
Project Manager: Strong employment history that includes some management experience: Bachelors or Master’s Degree.
Approach Trainer: Strong Employment History, experience leading safe groups with message receivers, familiarity with the curriculum, Peer Support training, Licensure level training on counseling theory.

Specialists: Peer Support Training; knowledge of local services, evidence of volunteer involvement in recovery services and significant recovery efforts
14. Identify the collaborators necessary to the success of the program.
Our work has pioneered the marketing necessary to get invitations into collaborating agencies. We have found that this proves to be a very important strategy for reaching isolated message receivers as flyer outreach strategies (though important and fruitful) do not result in high levels of voluntary referrals in Oakland. I feel our findings reflect that there is a high degree of self-stigma and a high level of hardships that prevents many isolated individuals from voluntary responses. That said, some of our most successful one-on-one partners have come to us through voluntary means, meaning that this is still a worthwhile endeavor and a great way to train Outreach Specialists. We included all stakeholders in our outreach efforts: providers, consumers, and family members. Though we did get some responses from consumers and family members, clearly our largest referral sources came from provider agencies. We have found that as we have had success partnering with service agencies that more service agencies are interested in hearing our presentation and inviting us in to run groups. Our biggest success in involving families has come through our partnership with PREP. We have had significant success utilizing family members to start up one-on-one relationships. We also received significant support from consumers through the POCC and were able to have four rounds of 12 week training sessions with volunteers in the community coming into help us train and ultimately get support. My feeling is that had these events been at more opportune times, that we would have gotten more participation through these circuits. We also used consumer and consumer/provider conferences to get the word out. 15. Recommendations for resource, facilities, and infrastructure requirements needed for support:
Technology and equipment needs
We made do with a very small space and one computer and four mobile phones. I would
recommend investing in a larger space with at least three computers each with a desk for this
project at least one printer. We were able to use a printing service, so a copy machine was not
necessary. Also required was a laptop and projector that were donated by both of our project
leads at various times. We also needed access to a conference room. Using a round table as a
place for four desks was made necessary by the small space but this set up was whimsical and
gave the team a sense of community, so in addition to the computer stations an open work
space can definitely work. We did need a locking filing cabinet to remain HIPPA compliant.
White boards, calendars, cork boards, and some simple organizing materials was enough to
make this fly.
Systems and services needs (e.g., billing, interpreter, etc.)
We did need to utilize a PEERS computer technician to get our computer system set up and our
internet; however, because we partnered with PEERS we were able to use what they have in

place, like their TT system and mileage and other reimbursement forms. This project is very
cheap to run with the support of an agency that is already in place. We were able to hire a
Spanish speaking individual and utilized her skills so interpretation skills. We did lean heavily on
the PEERS finance office and did need to include some expenditure for this for administrative
support; additionally we were very supported by the PEERS Executive Director who helped the
lead two roles grow through some struggles. We initially sought out free mediation services but
found PEERS ED support to be far superior particularly because she was onsite
Budget requirements
This program could operate on a grant budget of approximately $250,000.00 -$275,000.00
yearly. The primary costs would go to the salaries of the two leads including benefits and might
involve the Specialists graduating to a salary increase. I, the grant writer, provided services pro
bono and much of the problems we encountered were there because, in my opinion, my role
couldn’t be fulfilled to its fullest because of my need to work another job.
One - time costs (e.g., implementation and training)
We had to print Powerpoint Books for our Training Manuals which was at considerable cost
because I have yet to publish a manual. Moreover, I continued to reform the curriculum based
on feedback and I we had to pay for a second addition. Trainings like CPR and First Aid,
Compass Point to improve administrative skills, and Hearing Voices Network were training
investments to help our Specialists be work ready. Additional trainings, like WRAP also were
utilized and make a lot of sense. Additionally Specialists found the practice of traveling together
and making the team visible to the community services and tracking those services to be very
valuable. This required some expense without creating immediate results but was thought to be
important for team development. Our Program Manager used her own books on Team
Development during this time. I am aware that more money could’ve be spent on team
development, but our Program Manager is very gifted and talented. Additionally small issues
like purchasing transit cards is a condideration.
Other resources required for infrastructure support
0
















![Special Messages ACIM Urtext E-text · 2018-07-19 · ACIM URTEXT Special Messages in Chronological Sequence 4 4 Miracles Pathway Fellowship E-text 4 . 1d) 65 [UR_F 50] 65. This is](https://img.pdfslide.us/doc/110x75/5e992f6c230bd04633085ee4/special-messages-acim-urtext-e-text-2018-07-19-acim-urtext-special-messages-in.jpg)