Embed Size (px)
Citation preview

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
1
Solent Healthcare Community Health Services
CRS RiO Standard Operating Procedures Guidelines for the management of electronic patient care records in CRS RiO October 2010 Version Date Author Summary of
amendment Requested by:
V0.1 09/08/10 Transformation Team First Draft Transformation Manager V0.1 08/09/10 Transformation Team Completion of first draft
document Transformation Manager
V1.0 10/09/10 Transformation Team Amendments - Overview Assessment minimum recording
Operational Management Group
V2.0 14/09/10 Transformation Team SALT KPI’s added Judith Williams V3.0 04/10/10 Transformation Team Review of Physio KPI’s Sallyann Smith V4.0 04/10/10 Transformation Team OT & Physio Minimum
Data Set requirements Sallyann Smith Elaine Hoysted
V4.0 07/10/10 Transformation Team Appointment Outcome Activities added
Sallyann Smith Elaine Hoysted

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
2
Solent Healthcare Subject and version of document:
CRS RiO Standard Operating Procedure and Guidance V0.1
Author:
Transformation Team
Groups to be consulted whilst document in draft:
CRS RiO Operational Management Group CRS RiO Clinical Reference Group Information Governance and Records Manager CRS RiO Programme Board
Return date from group:
Date document issued:
Date when this version was uploaded to the website and distributed to Service Leads
Responsibility for dissemination to new staff:
Service Leads
Target audience:
All staff using RiO
Training implications:
To be included in the RiO end user training
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
3
1 INTRODUCTION......................................................................................................................................................................5
2 OBJECTIVES.............................................................................................................................................................................5
3 USE OF OTHER INFORMATION SYSTEMS, E.G. PAS, HHR.........................................................................................5
4 RELATED POLICIES...............................................................................................................................................................5
5 DEFINITION OF TERMS ........................................................................................................................................................6
6 DEFINITIONS RELATING TO RECORDS:.........................................................................................................................7
7 PERSONAL/DEMOGRAPHIC DETAILS..............................................................................................................................8
CLIENT SEARCH ................................................................................................................................................................................8
8 SEARCHING FOR EXISTING PAPER CLINICAL RECORDS ...... ..................................................................................8
9 CRS RIO CASE RECORD ACCESS:......................................................................................................................................9
10 KEY PERFORMANCE INDICATORS (KPI’S): ................ .................................................................................................10
11 REFERRAL TO TREATMENT 18 WEEK WAIT ................. .............................................................................................17
12 DUPLICATE CASE RECORDS ............................................................................................................................................18
13 UPDATING CLIENT DEMOGRAPHICS ............................................................................................................................18
14 CLIENT PERSONAL CONTACTS.......................................................................................................................................19
15 CLIENT NAMES .....................................................................................................................................................................20
16 ADDITIONAL PERSONAL INFORMATION.................... .................................................................................................20
17 CARERS RECORDS ...............................................................................................................................................................21
CARER ASSESSMENT......................................................................................................................................................................21
18 REFERRALS TO COMMUNITY SERVICES.....................................................................................................................22
RECORDING REFERRALS.................................................................................................................................................................22
19 TRANSFERS OF REFERRALS.............................................................................................................................................23
20 DISCHARGING REFERRALS..............................................................................................................................................24
21 DEATH OF A CLIENT ...........................................................................................................................................................24
22 RECORDING ALERTS ..........................................................................................................................................................24
MRSA .............................................................................................................................................................................................25 CHECKING ALERTS .........................................................................................................................................................................25
23 MEDICINES MANAGEMENT..............................................................................................................................................25
24 CRS RIO FORMS/ASSESSMENTS ......................................................................................................................................25
25 SAFEGUARDING....................................................................................................................................................................26
SAFEGUARDING CHILDREN .............................................................................................................................................................26 SAFEGUARDING ADULTS.................................................................................................................................................................26
26 CARE PLANNING, TREATMENT AND REVIEW ............................................................................................................27
27 PROGRESS NOTES................................................................................................................................................................27
ENTRIES BY ADMINISTRATORS ON BEHALF OF HCP’S ...................................................................................................................29
28 INPATIENT ADMISSION......................................................................................................................................................30
29 DEATH OF INPATIENT/NOTIFICATION OF DEATH ........... ........................................................................................30

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
4
30 COMMUNITY CONTACTS AND OUTPATIENT CLINIC RECORDING. ....................................................................30
RECORDING CONTACTS/APPOINTMENTS .......................................................................................................................................31 RECORDING AN OUTCOME FROM CONTACTS/APPOINTMENTS .......................................................................................................32
31 EDITABLE LETTERS............................................................................................................................................................33
32 PRINTING CLINICAL INFORMATION FROM CRS RIO......... .....................................................................................33
33 ACCESS TO RIO FOR BANK STAFF AND STAFF EMPLOYED ON A NON-REGULAR BASIS ............................33
34 LOGGING ON CRS RIO ........................................................................................................................................................33
35 LOGGING OFF FROM CRS RIO.........................................................................................................................................34
36 WHAT TO DO WHEN CRS RIO IS NOT AVAILABLE........... .........................................................................................34
37 BUSINESS CONTINUITY......................................................................................................................................................34
PLANNED DOWNTIME ......................................................................................................................................................................34 UNPLANNED DOWNTIME .................................................................................................................................................................34
38 APPENDIX 1 THE SECONDARY CARE RECORD ..........................................................................................................35
39 APPENDIX 2 NEW STARTER PROCESS..........................................................................................................................37
40 APPENDIX 3 LEAVER PROCESS .......................................................................................................................................38
41 APPENDIX 4 BUSINESS CONTINUITY PROCESS..........................................................................................................39
42 APPENDIX 5 GENERIC FLOW ............................................................................................................................................40
43 APPENDIX 6 GENERIC IP WORKFLOW - FOR PHT IP PROCESSES REFER TO YOUR LOCAL TEAM WORKFLOWS ....................................................................................................................................................................................41
44 APPENDIX 7 COMMUNITY NURSING - FIRST INITIAL OVERVI EW ASSESSMENT MINIMUM DATA SET RECORDING REQUIREMENTS...................................................................................................................................................42
45 APPENDIX 8 OCCUPATIONAL THERAPY OVERVIEW ASSESSMENT (SAP) MINIMUM DATA SET RECORDING REQUIREMENTS...................................................................................................................................................43
46 APPENDIX 9 PHYSIOTHERAPY OVERVIEW ASSESSMENT (SAP) MINIMUM DATA SET RECORDING REQUIREMENTS ............................................................................................................................................................................44
47 APPENDIX 10 APPOINTMENT OUTCOME ACTIVITIES BY SERVI CE DISTRICT NURSING.............................45
48 APPENDIX 11 APPOINTMENT OUTCOME ACTIVITIES BY SERVI CE THERAPISTS..........................................50

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
5
1 Introduction
CRS RiO is the primary care record for clients of Solent Healthcare (East). The paper record is the secondary record and should only contain information that cannot be recorded on CRS RiO (e.g. medication charts, specialist assessments) and copies of key documents that are required to provide a safe service if RiO is not available. See Appendix 1: Secondary Paper Record This document provides a framework for all authorised CRS RiO users including seconded and temporary staff and must be followed by all services using CRS RiO. Specific service addendums may be developed and attached to this document over time. However, these must first be submitted for agreement to Solent Healthcare’s CRS Clinical Reference Group and the CRS RiO Operational Transformation Group.
It is essential that all staff ensure they are familiar with this document and any other related policies.
2 Objectives The objectives of this document are to: • Ensure all relevant staff have sufficient guidance to use CRS RiO consistently • Ensure all relevant staff adhere to agreed recording procedures • Ensure that information is available to support effective care provision • Ensure that information is available to enable the provision of accurate National and Local SLA
reporting.
3 Use of Other Information Systems, e.g. PAS, HHR PAS HHR will not be used to record any patient information. PAS, HHR will continue to be available for viewing a client’s historical records. One admin member of each DN Cluster will retain read & write access to PAS to highlight Community matron Alerts, to enable the PHT to identify any patients involved with the Community Matrons ( KPI)
4 Related Policies
Records Management Policy Data Protection Policy Safe Haven Policy IT Security Policy Portable Devices Policy Personal Identifiable Information Policy

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
6
5 Definition of Terms
Term Definition
Alias Also known as
Care Plan The written framework that provides direction for the delivery of care
Carer A carer is anyone who provides a great deal of care on a regular basis for a member of their family or a friend – but is not employed to do so
Client PCT service user
Hampshire Health Record (HHR)
Interim electronic health record, created by the contribution of a number of systems
HCP Healthcare Professional (HCP), i.e. any registered person that holds a professional registration for the provision of healthcare
SHT Solent Healthcare Trust
IG Information Governance
Lead HCP The healthcare professional who has the lead responsibility for client care
Legacy systems Systems that were operational prior to the deployment of RiO
Named Nurse Lead nurse
Next of Kin ‘next of kin’ is not defined by the law and can be whoever the client or patient chooses
RiO Is the system that Solent Healthcare has chosen to implement as their client electronic record database
SOP Standard Operating Procedures
Spine A National Database containing a summary of patient records, this database synchronises demographic information with RiO
PAS Patient Administration System currently used by Services
Validation Electronically validating an entry in the patient record. The equivalent of signing an entry in the paper notes.
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
7
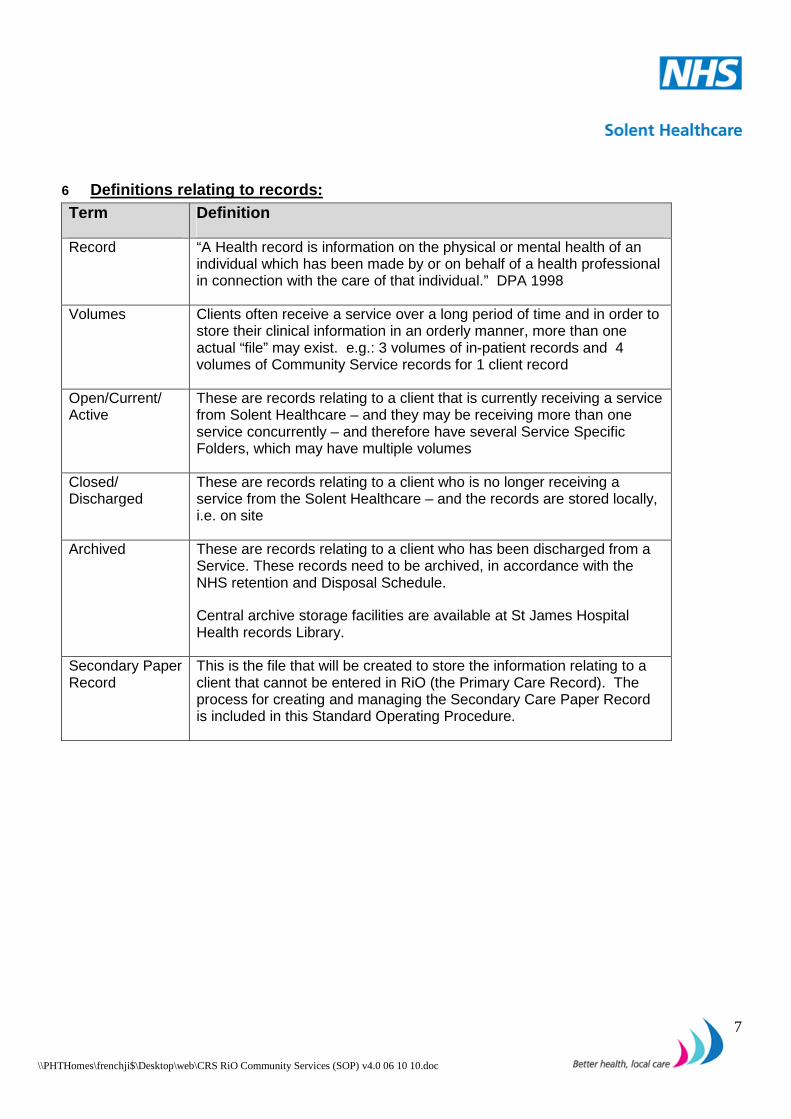
6 Definitions relating to records: Term Definition
Record “A Health record is information on the physical or mental health of an individual which has been made by or on behalf of a health professional in connection with the care of that individual.” DPA 1998
Volumes Clients often receive a service over a long period of time and in order to store their clinical information in an orderly manner, more than one actual “file” may exist. e.g.: 3 volumes of in-patient records and 4 volumes of Community Service records for 1 client record
Open/Current/ Active
These are records relating to a client that is currently receiving a service from Solent Healthcare – and they may be receiving more than one service concurrently – and therefore have several Service Specific Folders, which may have multiple volumes
Closed/ Discharged
These are records relating to a client who is no longer receiving a service from the Solent Healthcare – and the records are stored locally, i.e. on site
Archived These are records relating to a client who has been discharged from a Service. These records need to be archived, in accordance with the NHS retention and Disposal Schedule.
Central archive storage facilities are available at St James Hospital Health records Library.
Secondary Paper Record
This is the file that will be created to store the information relating to a client that cannot be entered in RiO (the Primary Care Record). The process for creating and managing the Secondary Care Paper Record is included in this Standard Operating Procedure.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
8
7 Personal/Demographic Details
Client Search
A client should be asked to provide the following information to enable a thorough search to be made on CRS RiO:
• Any previous names • Date of birth • Address history • GP details • NHS number
A thorough search should be carried out on CRS RiO using the following guidance and taking care with spelling and numbers:
• Search for client using NHS number (if known) If not known, search for client using: • Family Name, Given Name, Gender and Date of Birth Sound alike (e.g. Davies will find Davis), alternat ive spelling(s) and wildcard (e.g. Peter* will find Peters, Peterson and Petersen) Additional Search options: Client can be searched for by using any known previous ID’s; Military and PAS numbers will be electronically migrated into RiO as an alternative id. • If client is not found:
o Check any existing paper records, for any provided identity documents o Client’s GP practice for more information
If the client is not found on a local search; carry out a national search, following the same search criteria. If the client is not found on the National search, DO NOT create a new registration. All new registrations will be carried out by the centralised Back Office Team. Back Office contact details: [email protected]
8 Searching for Existing Paper Clinical Records
Every effort should be made to identify any existing paper records the organisation holds that relate to a client to ensure continuity of care and to reduce clinical risk.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
9
9 CRS RiO case record access: For the purpose of Data Protection CRS RiO will interrogate any individual searching for/attempting to access a case record for whom (from a CRS RiO perspective) they do not have a legitimate relationship with; there is no open referral to that individual’s team . In this instance the end user will be presented with a window that must be completed, requesting the reason the record is being accessed. All end users must select the reason from the drop down menu and complete the Comment field (free text box) expanding on their reason for accessing the case record. List of drop down options:
• Add Clinical Details • Administration • Audit/Investigation • Clinical Emergency • Formal Complaint • IT Support • Manage Carer Information • Quality/compliance assurance • Referral • Research Purposes
CRS RiO will provide a report identifying all end users who have accessed case records for whom they did not have a legitimate relationship. Regular audits will be carried out to identify any users who have “self claimed” a relationship with a case record; this report will be provided to Service Leads and Solent Healthcare’s Privacy officer and Caldicott Guardian.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
10
10 Key Performance Indicators (KPI’s): The tables below identify whether a KPI is reportable from CRS RiO and the field in which the data needs
to be recorded. Initially the CHIMERA (Data warehouse) Development Team will be creating reporting universes to mirror current reports generated via CHIMERA, pre Go Live. Additional reports will be prioritised and implemented in phases in Post Go Live KPI District Nursing – Specialist Palliative Care Reportable
in RiO RiO Field/Form
1 Non Malignant Disease - At least 55% of patients using the service should be suffering from non-malignant disease
Yes Diagnosis
2a Preferred Place of Death – At least 85% of patients should be able to die where they originally choose
Yes Library Care Plan
2b Place of Death – Less than 30% of people should die in hospital
Yes Library Care Plan
3 Gold Standard Framework – At least 80% of patients receive an end of life plan through GSF
Yes Library Care Plan
4 Patients receive appropriate support – All patients/carers should be asked to complete a questionnaire about the care received
No Manually as now
5 Prevention of Hospital/Hospice Emergency Admissions - Less than 40% of patients should be admitted to hospital/hospice
Yes Activity Code : Prevention of Admission to hospital or institutional care
6 Complaints – Rate of complaints from clients/carers should be less than 5% of all patients referred
No Manually as now
7 Complaints - Maximum of 1 incident of a complaint not handled within relevant time scale
No Manually as now
8 Reportable Incidents – Incidents which are reportable to NPSA or other statutory body set at a maximum of 1
No Manually as now
KPI District Nursing – Community Nursing Reportable in RiO
RiO field/Form
1 100% of service users to receive a comprehensive Community nursing assessment and, where appropriate, a care/intervention plan which is shared with the service user (and their family/carer)
Yes Referral to First Assessment/Care Plan
2 >80% Compliance with the Liverpool Care Pathway (LCP) in the last 72 hours of life
Yes Library Care Plan
3 >80% of adults to be able to demonstrate an increase in independence / health outcomes through the provision of Community nursing services, and as demonstrated through meeting individualised SMART goals.
Yes Care Plan
4 Percentage of VHIU’s on Community Nursing total caseload reported at quarterly intervals during 2009/10
No Manually as now
5 Count of number of admissions avoided during 2009/10
Yes Appointment Activity Code Prevention of Admission to hospital

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
11
KPI District Nursing – Intermediate Care Reportable in RiO
RiO field/Form
1 >85% of patients have a response time within 2 hours after a referral is received
Yes Referral to Assessment
2(i) >85% of patients with an Expected Discharge Date set within 24 hours
Yes Expected date of discharge to be set on admission
2(ii) 80% of Expected discharge dates met Yes Discharge on or before EDD 3 90% of service users to receive comprehensive
Intermediate care assessment Yes Referral – Completed Assessments
4 >95% of patients have LOS of 14 days or less Yes Admission to Discharge 5 >75% of service users are able to remain within, or
return to, their own home Yes Appointment Activity Code
Prevention of Admission to hospital 6(i) 100% of people referred by South Central
Ambulance Service are followed up by PAAFAS Yes Referral Source
6(ii) 85% of patients accept assessment by the PAAFAS Service
Yes Discharge Outcome – Patient requested discharge for those who do not accept assessment
7(i) Count number of falls/repeat falls, and repeat attendances by ambulance service, during 2009/10
No Manually as now
7(ii) Count number of referrals to Specialist Falls Service (PHT)
No Manually as now
8 Count of Unplanned and Emergency Hospital admissions during Intermediate Care treatment/stay during 2009/10
Yes Discharge outcome – Admitted to hospital
9 Count of early discharges to Rembrandt Unit and Rapid Response
Yes Discharge before EDD
KPI District Nursing – Jubilee House Reportable in RiO
RiO field/Form
1 MDT Assessment - 90% of service users to receive a MDT assessment and, where appropriate, a care/intervention plan shared with service user (& carer/family)
Yes Library Care Plan/creation of care plan
2 Liverpool Care Pathway - At least 80% compliance with Liverpool Care Pathway in the last 72 hours of life.
Yes Library Care Plan
3 Reason For Admission
Yes Referral source/ reason for referral

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
12
KPI Speech and Language Therapy Reportable
in RiO
RiO Form/Field
1(i)a At Least 90% of service users to receive a comprehensive assessment to be undertaken in the first 6 months
Yes Referrals/Assessments
1(i)b At least 90% of service users to receive a comprehensive assessment to be undertaken in the second half of the year
Yes Referrals/Assessments
1(ii)a All service users receive an intervention/ care plan where it is appropriate to be undertaken in the first 6 months
Yes Referrals/Care Plan
1(ii)b All service users receive an intervention/ care plan where it is appropriate to be undertaken in the second half of the year
Yes Referrals/Care Plan
2a At least 80% of service users demonstrate Increase/maintenance in communication and/or swallowing ability through provision of SLT Services to be undertaken in the first 6 months
Yes Care Plan outcomes
2b At least 80% of service users demonstrate Increase/maintenance in communication and/or swallowing ability through provision of SLT Services to be undertaken in the second half of the year
Yes Care Plan outcomes
3(i) Improving health outcomes through the provision of awareness raising, information giving and education to professionals, carers, members of the public
No
Manually as now
3(ii) Sub Service specific – people reporting a Benefit from education, an increase in knowledge and health outcomes
No
Manually as now
4 Information leaflets on the service will be Given to all users
No
Manually as now
KPI Occupational Therapy Reportable in RiO
RiO field/Form
1 Comprehensive assessment and intervention plan - >85% of patients receiving an occupational therapy assessment and intervention plan
Yes Completion of Assessment/MOHOST/Care Plan
2 Outcomes of OT intervention - 80% of referrals should have recorded having achieved the OT objectives as set following the initial assessment or subsequent reviews
Yes MOHOST/Care Plan
3 Provision of effective training and education - To provide an annual report of education and training undertaken
No Manually as now
4 Provision of effective training and education -Annual Audit of one element of training provided. To include course evaluation.
No Manually as Now

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
13
KPI Podiatry – MSK Lower Limb
Physio/Podiatry Reportable in RiO
RiO field/Form
1 % of patients referred by GP returned as inappropriate (under 5%)
Yes Discharge outcome - Inappropriate
2 % of patients offered assessment within 10 working days from contacting service (100%)
Yes Referral Status action of Contact Patient should be selected when client contacted.
3 % of patients referred to Specialist Physio/Podiatrist offered assessment within 5 working days (100%)
Yes Referral Status action of Contact Patient should be selected when client contacted.
4(i) % of patients referred to Specialist Physio/Podiatry Yes Number of referrals to Service 4(ii) % referred by Specialist Physiotherapist to
secondary care returned as inappropriate (under5%)
No Manually as now
4(iii) % of total patients referred to Primary care who are referred to Secondary Care
No Manually as now
5 % of patients who did not complete treatment (under20%)
Yes Discharge outcome – Dropped out/left
6 % satisfied from patient satisfactory survey (over 80%)
No Manually as now
7 Reduction of referrals to Orthopaedics/Rheumatology
Yes Discharge outcome – Treatment completed
KPI
Podiatry Reportable in RiO
RiO field/Form
1 Assessment and Intervention Plan - At least 95% of patients receiving an assessment and intervention plan
Yes Referrals/Assessments and Care Plans
2 Improvement in Pain - At least 80% of patients reported an improvement in pain based on VAS pain scale
Yes Library Care Plan
3 Wound Management - At least 50% of patients reported an improvement in wound management using Texas wound classification for at risk team
Yes Library Care Plan
4 Improved Mobility and Independence - At least 70% of patients reported an improvement in mobility and independence using Podiatry Outcome score for Community Podiatry team
Yes Care Plan
5 Count number of admissions avoided Yes Appointment Activity Code Prevention of Admission to hospital
6 Count number of outpatient appointments avoided Yes Discharge outcome – Treatment completed

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
14
KPI
Physiotherapy - Community Reportable in RiO
RiO Form/Field
1a 90% of service users to receive a comprehensive Physiotherapy assessment and, where appropriate, a care/intervention plan in first 6 months
Yes Referrals and appointment activity of Initial Referral
1b 90% of service users to receive a comprehensive Physiotherapy assessment and, where appropriate, a care/intervention plan in second half of year
Yes Referrals and appointment activity of Initial Referral
2a >80% of adults able to demonstrate an increase in independence/health outcomes in first 6 months
Yes Library Care Plan
2b >80% of adults able to demonstrate an increase in independence/health outcomes in second half of year
Yes Library Care Plan
3a FES: 90% of patients receive an assessment within 1 working week in the first 6 months
Yes Referrals and appointment activity of Initial Referral
3b FES: 90% of patients receive an assessment within 1 working week in second half of the year
Yes Referrals and appointment activity of Initial Referral
4a FES: 70% of patients demonstrate an improvement in first 6 months
Yes Library Care Plan
4b FES: 70% of patients demonstrate an improvement in second half of the year
Yes Library Care Plan
KPI Physiotherapy - Outpatients Reportable in RiO
RiO Form/Field
1a 90% of service users to receive a comprehensive Physiotherapy assessment and, where appropriate, a care/intervention plan in first 6 months
Yes Referrals and appointment activity of Initial Referral
1b 90% of service users to receive a comprehensive Physiotherapy assessment and, where appropriate, a care/intervention plan in second half of year
Yes Referrals and appointment activity of Initial Referral
2a >80% of adults able to demonstrate an increase in independence/health outcomes in first 6 months
Yes Library Care Plan
2b >80% of adults able to demonstrate an increase in independence/health outcomes in second half of year
Yes Library Care Plan
KPI Physiotherapy - Neurology Reportable in RiO
RiO Form/Field
1a 90% of service users to receive a comprehensive Physiotherapy assessment and, where appropriate, a care/intervention plan in first 6 months
Yes Referrals and appointment activity of Initial Referral
1b 90% of service users to receive a comprehensive Physiotherapy assessment and, where appropriate, a care/intervention plan in second half of year
Yes Referrals and appointment activity of Initial Referral
2a >80% of adults able to demonstrate an increase in independence/health outcomes in first 6 months
Yes Library Care Plan
2b >80% of adults able to demonstrate an increase in independence/health outcomes in second half of year
Yes Library Care Plan

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
15
KPI Physio - MSK Shoulder Reportable in RiO
RiO Form/Field
1 % of patients referred to Primary Care Physio (by their GP returned as inappropriate =>5%
Yes Discharge outcome - Inappropriate
2 % of patients referred to Primary Care Physio offered and assessment within 10 working days = 100%
Yes Referral Status action of Contact Patient should be selected when client contacted.
3 % of patients referred to Specialist Physio (by Primary Care Physio) offered an assessment within 5 working days =100%
Yes Referral Status action of Contact Patient should be selected when client contacted.
4(i) % of patients referred to Specialist Physiotherapy managed by Specialist Physiotherapy. Base line KPI
Yes Number of referrals to Service
4(ii) % referred by Specialist Physiotherapist to Secondary Care returned as inappropriate =<5%
No Manually as now
4(iii) % of total patients referred to Primary Care Physiotherapy who are referred to Secondary Care Base line KPI
No Manually as now
5 % of patients who did not complete treatment =<20%
Yes Discharge outcome – Dropped out/left
6 % of patients satisfied with service =>80% No Manually as now
KPI Physio - MSK Lower Limb Physio/Podiatry Reportable in RiO
RiO Form/Field
1 Percentage of patients referred by GP returned as inappropriate (under 5%)
Yes Discharge outcome - Inappropriate
2 Percentage of patients offered assessment within 10 working days from contacting service (100%)
Yes Referral Status action of Contact Patient should be selected when client contacted.
3 Percentage of patients referred to Specialist Physio/Podiatrist offered assessment within 5 working days (100%)
Yes Referral Status action of Contact Patient should be selected when client contacted.
4(i) Percentage of patients referred to Specialist Physio/Podiatry
Yes Number of referrals to Service
4(ii) Percentage referred by Specialist Physiotherapist to secondary care returned as inappropriate (under5%)
No Manually as now
4(iii) Percentage of total patients referred to Primary care who are referred to Secondary Care
No Manually as now
5 Percentage of patients who did not complete treatment (under20%)
Yes Discharge outcome – Dropped out/left
6 Percentage satisfied from patient satisfactory survey (over 80%)
No Manually as now

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
16
KPI Physio – Pulmonary Rehab Reportable
in RiO RiO Form/Field
1a • BMI,BP,Medical Research Council(MRC) dyspnoea(breathing difficulty) score pre/post programme
• 6 minute walk test (SWT) pre/post programme
• Borg score(raint perceived exertion) pre/post programme
• Hospital Anxiety and Depression (HAD) score pre/post programme
• Chronic Respiratory Disease Quality of Life Score (CRDQ) pre.post programme
in first 6 months
No Manually as now
1b • BMI,BP,Medical Research Council(MRC) dyspnoea(breathing difficulty) score pre/post programme
• 6 minute walk test (SWT) pre/post programme
• Borg score(raint perceived exertion) pre/post programme
• Hospital Anxiety and Depression (HAD) score pre/post programme
• Chronic Respiratory Disease Quality of Life Score (CRDQ) pre.post programme
in second half of the year
No Manually as now
2a 50% of patients exercising independently at 6 month follow up in first 6 months
No Manually as now
2b 50% of patients exercising independently at 6 month follow up in first second half of the year
No Manually as now

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
17
11 Referral to Treatment 18 Week Wait
Function Code
Code Code Description When & how to use RiO Workaround
SGD 18RI 18ww Referral Inappropriate
Code to be used when the referral is classified as inappropriate
Referral is discharged as: Inappropriate Referral
CCC 18TC 18ww Treatment Code to used when Treatment has commenced (Clock Stop)
Use outcome Activity: RTT First Appointment(treatment Given)
CCC 18AM 18ww Actively Monitoring
Code to be used when patient is being actively monitoring but no treatment given (Clock Stop)
As Above
SGD 18CP 18ww Referral Cancelled by Patient
Referral Cancelled by Patient not seen by Service - returned back to Referrer (Clock Stop)
Use Discharge reason of: Patient requested
SGD 18NC 18ww No Contact from Patient
Patient contacted by service and no response tpo either letter or telephone call - returned back to referrer (Clock Stop)
Use Discharge reason of: Did not respond to be seen
CCC 18DN 18ww 1st DNA First DNA by Patient (Clock Stop ) Use outcome code of: RTT 1st Appointment (DNA)
CCC 18RC 18ww Restart Clock after 1st DNA & Suspension
When the patient DNAs first appt and then is subsequently offered a further appt the Clock will restart on the date that the new appt was offered to the patient. (Clock Restart)
Add Referral action: Appointment invite sent
CCC 18WW 18ww Appointment Cancelled by Patient
Appointment cancelled by patient .This does not stop clock. Further appointment offered
Outcome of cancellation: Cancelled by client
CCC 18PS 18ww Patient Suspended Contact
Patient has suspended contact with service due to medical or social reasons this will (Pause the Clock) Suspension should not last more than 6 months. PTP should be put in place after 3 months. Pause to be communicated to patient.
These numbers are small as they are likely to be discharged back to the referrer: To be collected manually and review
CCC 18AA 18ww Appointment Arranged
Patient contacted by service to arrange appointment by letter or telephone
Appointment booked within 18 weeks of referral date
CCC 18IA 18ww Inpatient Admission Same Service or Other Provider
Patient inpatient admission to either same service or other provider e.g. HPT (Clock Stop)
Patient admitted to another provider: Patient should be discharged from original referral Patient admitted to same service: Patient should be discharged from original referral
CCC 18CB 18ww Choice Breach This is to be recorded when the patient has chosen to be seen within the service over the 18 week timescale.
Appt Comment Field to be populated with: Choice Breach - This will then provide a free report
SGD 18DS 18ww DNA Discharged from Service
2nd DNAs do not stop clock but decision within service whether to offer alternative (Clock will continue
Outcome reason of: RTT subsequent appt DNA discharge to GP -

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
18
from Restart from previous DNA start date). On discharge referrer to be notified.
To be considered in conjunction with service DNA policy
SGR AAA 18ww Referral Outside Provider
This referral code is to be used when the patient has been referred from another provider and the clock has already started with them. Referral date must be the date that the original referral was received.
Referral must be predated to the original referral date. Referral source must be: Permanent transfer from MH services
12 Duplicate case records If a duplicate electronic case record is discovered on CRS RiO send the details in an email to the Back Office Team immediately, via an NHS email account using the NHS address below. [email protected]
13 Updating client demographics
At registration, or at other stages in the client pathway (e.g. review of care plan or where CRS RiO indicates there is a difference between the information recorded on the Spine ((Synchronising the Spine)) and the information given by the client), demographic information will need to be updated. The following guidance should be followed to ensure this is carried out correctly:
Data mismatch Examples
First check Action
Clients permanent address differs from the address on RiO
Confirm the source of information is reliable, e.g. via the client, GP
Record new address on CRS RiO and update the spine
Client has a temporary address
Ensure source of information is reliable
Add as a temporary address on CRS RiO
Client correspondence address is advised
Ensure source of information is reliable
Record new address in client registration 'addresses' and add as a correspondence address on CRS RiO
Client gives a different date of birth
Ensure source of information is reliable - check with GP/referrer
Confirm with documentation, e.g. Birth Certificate, Passport, etc and record the accurate date of birth on CRS RiO and update the spine . Create a progress note informing of the change and mark as a significant event

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
19
Data mismatch Examples
First check Action
Client advises change of GP
Contact new GP to confirm client is now registered with them - advise GP that they need to update the spine
• Record new GP on progress note within CRS RiO and “Tick” Significant Event Box.
• Once new GP has been updated on the spine, record this on a progress note as a significant event.
Client Contact Numbers (telephone)
Ensure the source of information is reliable, Client/GP
• Record in Communications; to ensure the telephone number appears on the front page of the client case record select “office address” as the communication context.
14 Client Personal Contacts The following table provides guidance on the information that must be recorded for all clients, where appropriate, as soon as it is available:
Item Guidance To be
completed on CRS RiO
Next of kin(s)
If known Yes
Dependent children of the client
As required Yes
Clients with carers See Section - Carers Records Yes Professional contacts
Professional contacts should be recorded as a professional contact, when the professional contact ends; complete the end date field of that contact. DO NOT DELETE as this will completely delete the professional contact from CRS RiO.
Yes
Personal Contacts Permission to record personal contacts must be confirmed by the individual before being recorded on CRS RiO and a progress note should be added confirming this.
Yes

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
20
15 Client names
The following table provides guidance on the information that must be recorded for all clients, where appropriate, as soon as it is available:
Item Guidance To be
completed on CRS RiO
Client name changes -
Names which have been formally changed (e.g. as a result of marriage) should be updated on CRS RiO and the former name will remain as an ‘Alias’ (this is purely a CRS RiO term denoting a change in name). A search for the client using either name will bring up the correct record. The ‘Alias’ function may also be used in CRS RiO to record alternative names by which clients are known, other than the name(s) recorded on official documents e.g. a person recorded as Elizabeth who prefers to be known as Betty. A search for the alias (Betty) will find the correct record.
Yes
16 Additional personal information The following table provides guidance on the information that should be recorded for all clients, where appropriate, as soon as it is available: Item Guidance To be
completed on CRS RiO
Mobility and communication difficulties
If yes is selected this will populate the front page of the client’s CRS RiO record
Yes
Preferred name This will show on the front page of the client’s CRS RiO record
Yes

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
21
17 Carers Records
A carer is anyone who provides or intends to provide a substantial amount of care on a regular basis for another individual aged 18 or over and is not employed to do so (Children and Carers Act 2000) Carers should be recorded as personal contacts against the client record: In order to capture activities directly relating to the carer, they will need to have a separate CRS RiO ‘Carer’ record. This is created in the same way as a client record, with the record type set to ‘carer’ instead of ‘client’. Permission to record personal contacts or to create a carer recor d, must be gained from the individual before being recorded on CRS RiO and a progress note shoul d be added to confirm this. Carers who are also clients should have a CRS RiO record created with the record type set to ‘Client and Carer’. A referral is not required in order to record activity directly with a carer. Diary appointments can be booked with a carer who has a CRS RiO ‘carer’ or ‘client and carer’ record. Carer Assessment Item Guidance To be
completed on CRS RiO
Carer’s Health Assessment (this is under the “Generics Assessment”) Hyperlink
To be completed as appropriate. If appropriate
Overview Assessment – Carers Section
To be completed as appropriate. If appropriate
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
22
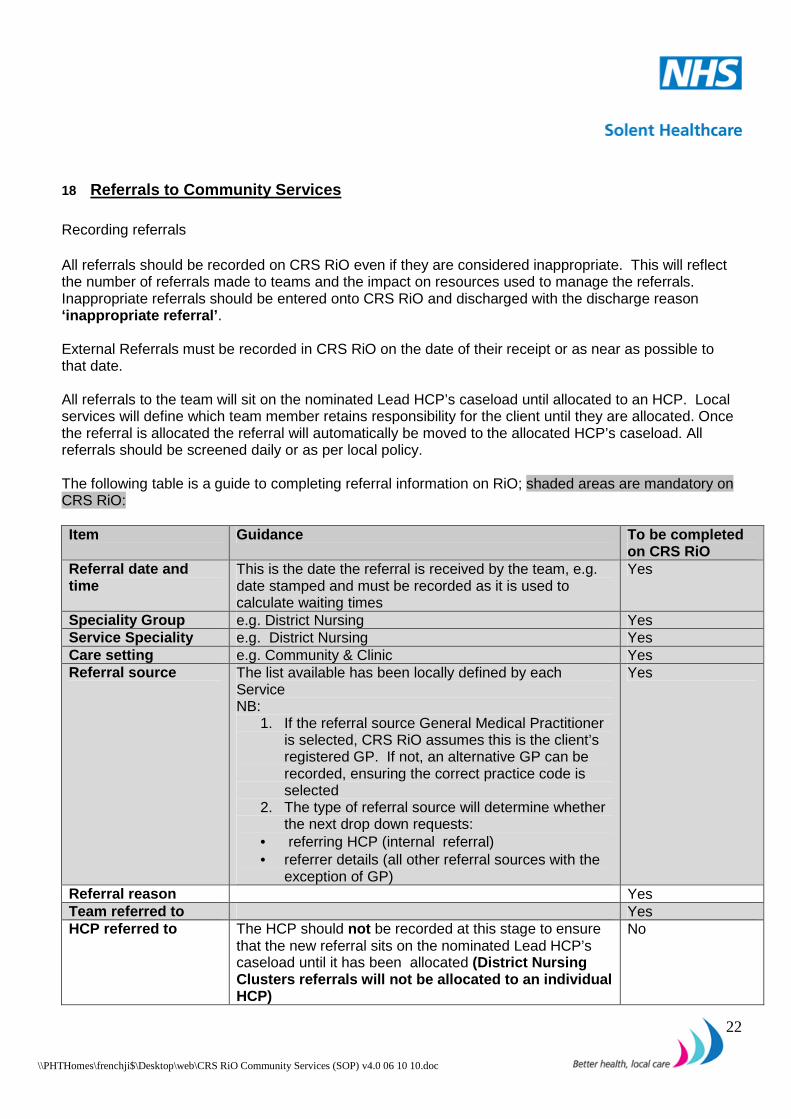
18 Referrals to Community Services
Recording referrals All referrals should be recorded on CRS RiO even if they are considered inappropriate. This will reflect the number of referrals made to teams and the impact on resources used to manage the referrals. Inappropriate referrals should be entered onto CRS RiO and discharged with the discharge reason ‘inappropriate referral’ .
External Referrals must be recorded in CRS RiO on the date of their receipt or as near as possible to that date. All referrals to the team will sit on the nominated Lead HCP’s caseload until allocated to an HCP. Local services will define which team member retains responsibility for the client until they are allocated. Once the referral is allocated the referral will automatically be moved to the allocated HCP’s caseload. All referrals should be screened daily or as per local policy.
The following table is a guide to completing referral information on RiO; shaded areas are mandatory on CRS RiO:
Item Guidance To be completed
on CRS RiO Referral date and time
This is the date the referral is received by the team, e.g. date stamped and must be recorded as it is used to calculate waiting times
Yes
Speciality Group e.g. District Nursing Yes Service Speciality e.g. District Nursing Yes Care setting e.g. Community & Clinic Yes Referral source The list available has been locally defined by each
Service NB:
1. If the referral source General Medical Practitioner is selected, CRS RiO assumes this is the client’s registered GP. If not, an alternative GP can be recorded, ensuring the correct practice code is selected
2. The type of referral source will determine whether the next drop down requests:
• referring HCP (internal referral) • referrer details (all other referral sources with the
exception of GP)
Yes
Referral reason Yes Team referred to Yes HCP referred to The HCP should not be recorded at this stage to ensure
that the new referral sits on the nominated Lead HCP’s caseload until it has been allocated (District Nursing Clusters referrals will not be allocated to an indi vidual HCP)
No

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
23
Item Guidance To be completed on CRS RiO
Referral urgency This list is locally defined, therefore select as appropriate to local policy
Yes
Administrative category
Clients should be recorded as ‘NHS patient, including overseas visitors’. If the client is not a resident of the UK, the Back Office Team should be contacted, via an NHS email account, detailed below: [email protected]
Yes
Referral Received Date
This is the date on the letter/fax or date the telephone call was received.
Yes
Referral Accepted date
This is the date the decision is made to accept the referral. This must be recorded as, on occasion, further information is required before a referral is formally accepted, therefore will calculate waiting times
Yes
19 Transfers of referrals A referral can be transferred between caseloads within a team on CRS RiO. However for additional/concurrent services outside of the team a new referral will be entered on CRS RiO For example:
Example of Scenario’ What to do on CRS
RiO Responsibility
New referral is entered onto RiO to DN Cluster Cosham New referral Team, referral is accepted and prioritised at referral meeting
Transfer referral from DN Cluster Cosham New Referral Team to appropriate sub team e.g. District Nurse Cluster Cosham Blue
HCP
Patient needs to be assessed by the Continence Team
Enter new Referral to the Continence Team
HCP identifying the need for the referral
Patient has an active referral with DN Cluster Cosham Team; the patient has informed the Clinician they are relocating to Southsea.
• Enter new referral to the appropriate DN Cluster Southsea
• Discharge the DN Cluster Cosham referral
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
24
20 Discharging Referrals Patients must be discharged from CRS RiO when there is no further input needed from any member of the team or the referral is deemed as inappropriate or inactive. The duty to discharge a client from a service is the responsibility of the allocated HCP or if the referral has not been allocated the HCP who has determined no further treatment is needed. The management of this function can be delegated to administrative staff but responsibilities for the decision to discharge remain with the Clinician. All appointments must be outcomed before the referral is discharged as any unoutcomed appoints will be automatically cancelled. MDT Discharge – decision to discharge must be made by team to ensure that future activities are not cancelled.
It is the responsibility of all HCP’s to ensure their caseloads are up-to-date and that clients are discharged appropriately. Discharging a client will not remove their details from CRS RiO; it will close their current episode of care for the discharging team. The case record will be removed from the team caseload. The discharged referral will still be viewable within the client’s case record. Subsequent new referrals to the teams can be made at any time.
21 Death of a client
If a client dies whilst under the care of any service, the team should contact the Back Office Team in an email immediately, via an NHS mail, using the address listed below. The Back Office team will initiate the process for communicating this within the Trust see Records Management Policy [email protected]
22 Recording alerts
The CRS RiO ‘alerts’ screen must be used to record and update alerts for the following instances:
•••• Allergy •••• Child in Need •••• Child Protection Plan •••• Client has Medical Alert •••• Do Not Divulge Address • Looked After Child • MARAC • Patient With Same Name • Restrict Patient Contact • Risk In Home Environment • Vulnerable Adult

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
25
MRSA
A positive MRSA result must be recorded; • Add an alert type of “Client has medical Alert” include ‘positive MRSA’ in the comments field. • Record on a progress note and tick the “Significant Event “ box • Screening for MRSA should be recorded in the progress notes as a significant event.
Checking Alerts If the alerts icon on the client’s case record front screen is red it is the responsibility of all staff to check the content and take the necessary action(s) prior to seeing their patients.
23 Medicines management The CRS RiO Prescribing module is currently not being used. All medication should be recorded in the Assessment Overview Form (Medication Section) within CRS RiO. This should include any changes to current medication. Medication cards should continue to be used by teams, as per current practice.
24 CRS RiO forms/assessments
It is important that clinical information is recorded in the correct place on CRS RiO. If everything is recorded in the progress notes it will be difficult to locate.
If clinical information cannot be typed directly onto CRS RiO, the CRS RiO Business Continuity Forms should be used, for input into CRS RiO at a later time (in line with Service agreed timescales listed below). Any paper documents created for this purpose must subsequently be shredded and not kept on the secondary paper record. Assessments should be completed as soon as possible following contact with the client and, in line with Solent Healthcare standards. For entries to Inpatient services: All entries are to be completed before the end of shift or immediately where a significant/risk event is identified For entries to Community services: All entries to be completed by end of shift or within 24 hours of the contact or immediately where a significant/risk event is identified.
• Risk Assessment is an integral part of the overview assessment (risks arising):
o Free text fields must be completed for any identified risks and scored as appropriate.
The Overview Assessment Form (within the Single Assessment) is the chosen Core Assessment for Community Services and must be completed at the point of initial Service delivery and updated as appropriate. Jubilee House and Rembrandt must also complete the Admissions Assessment See appendix 7 “mandatory sections for Community Services”.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
26
25 Safeguarding
Safeguarding Children
RiO will not, at present, replace the current processes for recording information relating to children on the child protection plan. However, RiO should be used, in addition to the current processes:
Safeguarding Adults CRS RiO does not, at present, support the concept of vulnerable adults. Therefore those clients who have been accepted under Local Authority Safeguarding Adults should have their information recorded in CRS RiO using the table below:
Scenario What to do on RiO A client (or a child whose parent or carer is a client) has been identified as being the subject of a Child Protection Plan/child in need
Add an alert: select the relevant alert type for children, in the comments box enter a title of SAFEGUARDING CHILDREN, followed by the type of abuse and a contact number for more information.
When the child is removed from the Child Protection Plan
Remove Alert (this will remain in the historical record of the alert)
Scenario What to do on CRS RiO A client is suspected as being abused • Risk Assessment updated to include your concerns
• Complete progress note and set as a significant event
A client case has been accepted under Local Authority Safeguarding Adults. Data should be entered by:
• In the first instance the attending Clinician
• If there is no attending Clinician the Safeguarding Health representative
Add an alert: select alert type of “Vulnerable Adult”, in the comments box enter a title of SAFEGUARDING ADULTS, followed by the type of abuse and a contact number for more information.
• Client is closed to safeguarding team.
Remove Alert (this will remain in the historical record of the alert)

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
27
26 Care Planning, Treatment and Review
For All Clients Lead Health Care Professional
Key worker
Information Sharing and Consent
This must be recorded in the Overview Assessment (Single Assessment List) Record information about who the client does not wish to share information with. Record whether a signature has been collected on the information sharing and consent form. Current paper forms will be used (where appropriate) and input retrospectively onto the CRS RiO Form. For those clients who do not have the capacity to consent a progress note should be generated, indicating this and saved as a significant event.
Care Plan Care Plan Record problems/needs and interventions Care Plan contact Record office and out of hours contacts
Record client leaflet distribution Care Plan distribution Record dates that care plan has been distributed to involved parties. If a copy
of the care plan is not given to the client, record the reason why
27 Progress Notes Each individual HCP is responsible for making relevant entries into the progress notes. If clinical information cannot be typed directly into CRS RiO, the Business Continuity Form should be used for entering onto CRS RiO at a later time, according to locally agreed procedures. Any paper documents created for this purpose must subsequently be shredded and not kept in the secondary paper record, or anywhere else, as this would be a data protection risk for the HCP, the client and Solent Healthcare.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
28
Progress note entries The progress notes form an important part of the clinical record. Each HCP is responsible for keeping up-to-date progress notes for clients on their caseload. Progress notes must be entered into CRS RiO following contact with the client and the ‘validate this note’ box ticked when completed (this is the equivalent of signing an entry in the paper notes). The following table provides guidance on completing progress notes:
Item Guidance Team/ward of completing HCP Type the name of the team/ward, to enable other staff to see where
the information was generated.
Content The entry should be concise and an accurate reflection of the contact with the client.
Problem/Need types When adding a new note the option will be given to select a problem type from those selected when adding a problem/need to the Care Plan. This will help should it be necessary to filter information about a particular problem/ need type
Timeliness
Progress notes must be updated as soon as possible following contact with client. • In-patient services: all entries to be complete by handover of
shift/end of duty or immediately where a significant/risk event is identified
• Community services: all entries to be complete by end of shift or within one working day of community or outpatient contact or immediately where a significant/risk event is identified.
Significant events Please ensure the significant event box it ticked for all progress note
entries relating to significant events. Risk events Progress notes that have had the “Add to Risk History” Box ticked, are
also viewable via the Significant. Events hyperlink
Information that cannot be recorded in CRS RiO, e.g., reports/correspondence from outside agencies
Must be filed in the secondary care record and reference made to their existence in the CRS RiO progress notes. The reference must include:
• Title (what is it?) • Date (when it was received?) • Filing location (where is it filed within the secondary record, i.e.
which section (green notes Recording sensitive information Some information recorded in the clinical record is particularly
sensitive, e.g. Psychology progress notes. Such information should be recorded in the paper secondary record and a summary progress note entered on CRS RiO stating that further information is held in the secondary paper record and can be obtained from the team.
3rd party information
See “PCT Access to records guidance and procedures” Progress note entries containing 3rd party information, e.g.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
29
information supplied by or pertaining to a friend/relative or outside agency must be marked as such by ticking “this note contains third party information” box at the foot of the progress notes screen
Validation Access to progress notes on CRS RiO will be granted at one of four levels: Students, Health Care Support Workers
• Can view all note types • Can add notes but cannot validate
Therapy technicians • Can view all note types • Can add notes and validate their own
Registered Staff • Can view all note types • Can add notes and validate their own and others entries
(students) Clerical Staff
• Can view admin notes • Can add notes and validate their own notes
The validation of progress notes acts as a signature and prevents any further changes being made to the entry.
Notes cannot be deleted; if entered in error they can be “scored through”
Timescales for validation It is the responsibility of all HCP’s who are recording information on the client’s record, to ensure that all entries are validated as soon as possible after their entry onto CRS RiO. The expected timescales for validation are:
Entries made by the HCP – must be validated as soon as the entry is completed or known to be accurate. Entries made on behalf of the HCP - by end of shift or the next working day Validation of student/non registered entry should be as per current Trust Policy
Entries by administrators on behalf of HCP’s Administrators can only record information on progress notes and assessments/forms on behalf of a clinician if requested to do so by the HCP:
• Must be entered in a timely manner • State when and how the information was received • Include the name and designation of the dictating HCP • Be checked and validated by the HCP by end of shift or the next working day

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
30
28 Inpatient Admission The CRS RiO inpatient admission screen must be completed at the time of admission with any missing or updated information added as soon as it is known.
29 Death of Inpatient/Notification of Death If Services receive notification of the death of a client or a death of a client occurs during an inpatient stay, staff should contact the Back Office Team immediately; via an NHS email The Back Office Team will close down all open referrals and notify those teams to whom the referral relates. Cancellation of transport will remain with the individual teams. [email protected]
30 Community Contacts and Outpatient Clinic Recording
All community and outpatient client face-to-face and telephone contacts must be entered onto CRS RiO and an outcome recorded on CRS RiO to provide evidence of contract performance to Commissioners. The place to do this is the CRS RiO diary or clinic. It is the responsibility of each HCP to ensure their CRS RiO diary is kept up-to-date; administrators can book and cancel diary and clinic appointments on their behalf. All HCP’s will be expected to treat their CRS RiO diary as their primary source for recording contacts with clients. Other staff within a team can view/book appointments into the diaries of their colleagues; access is locally configured. In general, staff should not book into the diary of others without prior agreement. Retrospective contacts/appointments can be recorded/outcomed in the CRS RiO diary, by the end of the shift or the next working day.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
31
Recording Contacts/Appointments
The following table provides guidance for recording community contacts and outpatient clinic appointments on CRS RiO:
Item Guidance Where to record Client community face-to-face and telephone contacts in a non-clinic settings, including therapy contacts
CRS RiO diary
Home visits CRS RiO diary Group appointments CRS RiO diary or clinic
if this has been set up for the team
Client face-to-face and telephone contacts in a clinic setting
CRS RiO clinic
Inpatient contacts by community HCP’s
CRS RiO diary
Indirect client activity, e.g. supervision contacts, team discussion
Information about the contact should be recorded in the CRS RiO progress notes
Non-client activities e.g.:
• Administration • Leave Planned • Report Writing
As appropriate in CRS RiO diary
The following table provides guidance for recording inpatient contacts on CRS RiO:
Item Guidance Where to record Inpatient contacts by inpatient HCP’s
All contacts by inpatient HCP’s, e.g. Occupational Therapists Need to refer to Service Workflows – those OT’s and Physio,s who aren’t integrated will need to raise a referral to ensure their activities are captured.
CRS RiO Diary or Clinic if they have been set up. Additional Information about the contact should be recorded in the CRS RiO progress notes before the end of the shift if appropriate

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
32
All contacts recorded on CRS RiO are marked as “face to face” (default option) unless this box is unchecked. The following table provides guidance for selecting the appropriate appointment type in CRS RiO:
Appointment Type Guidance First Appointment To record a client or carer’s first face-to-face appointment or
clinically significant contact Follow-up appointment To record any further ongoing interventions; face-to-face
appointments / clinically significant contacts with a patient or carer Review To record reviews; updates/reassessments Telephone contact To record any telephone care contacts with a client or carer/s.
These must be judged to be clinically relevant. Telephone calls regarding making/changing/ confirming appointments with clients or carers should not be recorded. This information should be recorded in a progress note.
Unplanned contact To record any unplanned contacts Consultation As appropriate 48 hour follow up contact
To record the follow up contacts that must take place for clients discharged from inpatient units (where appropriate)
7 day follow up contact To be used to record 7 day follow up contacts (where appropriate) Recording an outcome from contacts/appointments
To ensure activities are captured for reporting an outcome must be recorded following each contact/appointment; See table below for guidance on outcoming appointments on CRS RiO:
Item Guidance When to record Activities The relevant activity(s) must be recorded
against each contact/appointment. See Appendix 10 for a breakdown of activities by Service
When recording an outcome following a diary/clinic contact/ appointment
Arrival time The ‘arrival time’ should be recorded correctly if known, or as the appointment time if not known
When recording an outcome following a clinic appointment
Seen time The ‘seen time’ should be recorded as the time the client was actually seen by the HCP, or as the appointment time if not known
When recording an outcome following a diary/clinic contact/ appointment
Outcome Select the relevant outcome type. When out coming a diary/clinic contact/ appointment

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
33
31 Editable Letters
CRS RiO will contain a range of pre configured letter templates; these can be edited and “sent to RiO” These letters will be stored against the patient record. An additional Blank letter template has been included; this will be pre populated with the patients/clients demographic details and may be used for cutting and pasting reports, assessment outcomes etc
These forms are not mandatory and can be used as required by Services.
32 Printing Clinical Information from CRS RiO
CRS RiO users should refrain from printing clinical data unless absolutely necessary and instead use data direct from the screen. Users should validate the identity of any printed material against the on-screen data and mark the sheet(s) accordingly, to ensure that the printing has completed correctly. Any information printed from CRS RIO should be clearly identifiable by services using a stamp which clearly indicated this is a copy of information held electronically. Any copies made should be destroyed under confidential conditions.
33 Access to RiO for bank staff and staff employed on a non-regular basis NHS Professional/agency registered staff employed regularly (a minimum of 1 shift a week or 4 per month) will be issued with smartcards and receive CRS RiO training. No other temporary staff will be given access to CRS RiO.
34 Logging on CRS RiO
Access to CRS RiO is controlled with smartcards. Staff are responsible for ensuring that they have their smartcards with them AT ALL TIMES and that they are not shared with anyone else. Anyone reporting to work without their smartcard should either be asked to go home and get it or should be redeployed to work not requiring access to the system. If the smartcard is locked (generally because the unique pin number has been wrongly entered 3 times) it can only be unlocked by an RA agent. Refer either to your manager or Health Records. If there is any concern that a pin number has been compromised, it must be changed immediately. If a smartcard is lost or stolen the relevant smartcard agent must be contacted and an incident form completed. Staff should be aware that smartcards are only valid for a period of two years, after which the certificates attached to their log in will need to be renewed they are responsible for completing this process. For more detailed information refer to the Registration Authority Guidance Documentation on the Solent Healthcare intranet.
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
34
35 Logging off from CRS RiO To log off from CRS RiO, click the ‘log off’ hyperlink and remove the smartcard. In an emergency it is acceptable to remove the smartcard without logging off from CRS RiO. This will close any open internet explorer windows any unsaved data will be lost e.g. if the progress note has not been saved prior to removing the card. The computer should still be locked (CTRL+ALT+DEL) as per Trust policy.
36 What to do when CRS RiO is not available
In the first instance, any problems should be reported to the local ICT Service Desk
Hours: 08:00 - 17:00 Monday to Friday (ex bank holidays) Tel: 023 9268 2680 Fax: 023 9268 3413 Email: [email protected]
37 Business continuity Planned Downtime There are likely to be times when CRS RiO is unavailable for short periods of time to enable upgrades and maintenance on the system. During periods of planned downtime, the CRS RiO Business Continuity Procedure must be followed (see appendix 2). Business Continuity Packs will be provided to all teams and Champion Users. These packs will include paper versions of specific forms within RiO.
Unplanned Downtime In the event of CRS RiO not being available, inform your local ICT Service Desk in the first instance; The CRS RiO Business Continuity Procedure must be followed.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
35
38 Appendix 1 The Secondary Care Record
CRS RiO is the designated electronic record for Solent Healthcare and must be used to record all clinical activity. However there will be some information that will not be able to be recorded on the system (e.g. medication charts; incoming correspondence, minutes and specialist assessment forms used by individual services that are not recordable on CRS RiO. Therefore it is necessary for the Primary CRS RiO Case Record to have a Secondary Paper Record. The purpose of this guidance is to ensure that the there is continuity on the management of the Secondary Paper Record throughout Solent Healthcare.
Existing patients may already have paper health records. Services should ensure that they have made a search of any legacy systems in order to note any previous health record numbers already issued. If a previous paper record exists for the service it should be utilised as the secondary paper record. A label is to be applied to the paper record to show that the client now has a record on the CRS RIO system and the following information will be recorded on a label to be applied to the front of the paper record folder. The date of first entry on CRS RIO is to be added to the label and a summary of any clinically relevant information transferred from the “old volumes” onto the CRS RiO Primary Care Record and marked as a significant event.
Process to implement a new Secondary Paper Record: If a client is not known to the service a new Secondary Paper Record will need to be made.
Section Contents A Demographics/Consent
• Identification Sheet – printed from RiO Consent to Share Information Form – Use current paper form and enter on RiO retrospectively indicating that the patient has signed
B Clinical Forms Those Clinical Forms that cannot be captured in RiO
C Correspondence
• External Referral Letters • Discharge Letter – to be cut and pasted into
RiO Progress Note and set as a significant event
• Faxes • Any other relevant correspondence
D Physical Section Summary to be cut and pasted into a progress note • Pathology and other results • X Ray and Scan results • ECT/ECG/EEG • Monitoring forms not contained within RiO • Pharmacy Charts •
E Legal Documents F Downtime Documentation Each service will be provided with a downtime
pack, to be used in the event of RiO not being available

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
36
Movement of the Secondary Care Record:
Some services are able to store their current secondary care paper record on site for the duration of the episode of care; however, some services return paper records to the Central Records Library at St James Hospital. The CRS RiO system does not have an electronic case note tracking system, therefore it is important that services are able to locate and track their secondary paper records. Services should ensure that they put in place a system for tracking their secondary paper records, using the paper tracer cards. This should be recorded on a progress note on RiO; Titled “Secondary Paper Record Created. Before creating a Secondary paper record the progress notes should be searched to ensure a Secondary record has not already been created
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
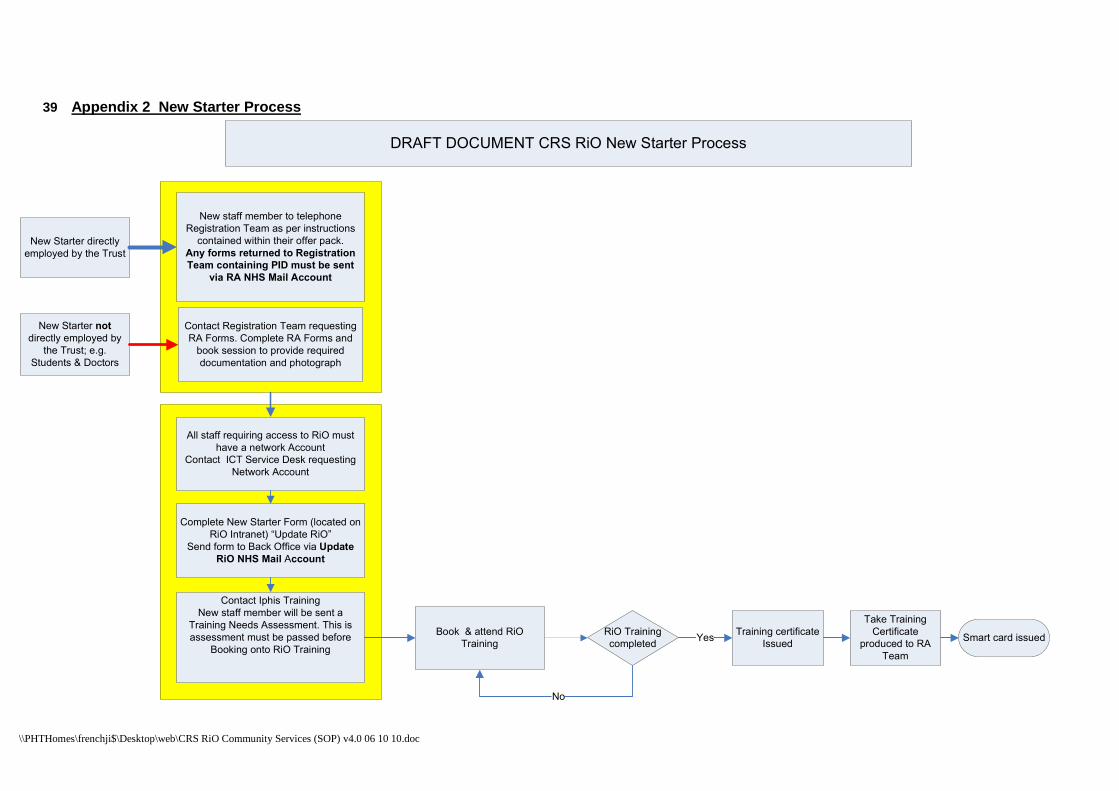
39 Appendix 2 New Starter Process
New Starter directly
employed by the Trust
Complete New Starter Form (located on
RiO Intranet) “Update RiO”
Send form to Back Office via Update
RiO NHS Mail Account
Contact Registration Team requesting
RA Forms. Complete RA Forms and
book session to provide required
documentation and photograph
Contact Iphis Training
New staff member will be sent a
Training Needs Assessment. This is
assessment must be passed before
Booking onto RiO Training
All staff requiring access to RiO must
have a network Account
Contact ICT Service Desk requesting
Network Account
New Starter not
directly employed by
the Trust; e.g.
Students & Doctors
New staff member to telephone
Registration Team as per instructions
contained within their offer pack.
Any forms returned to Registration
Team containing PID must be sent
via RA NHS Mail Account
Book & attend RiO
Training
RiO Training
completed
No
Training certificate
IssuedYes Smart card issued
Take Training
Certificate
produced to RA
Team
DRAFT DOCUMENT CRS RiO New Starter Process

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
40 Appendix 3 leaver process
Complete Staff Leaver Form (located on
RiO Intranet) “Update RiO”
Send form to Back Office via Update
RiO NHS Mail Account
Inform Registration Team of the date
staff member is leaving, via RA NHS
Mail Account
Contact ICT Service Desk requesting
Network Account is deleted/disabled
leaverSmart Card is disabled
Network Account
deleted/ disabled
Deleted from RiO
DRAFT DOCUMENT - CRS RiO Leaver Process

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
41 Appendix 4 Business Continuity Process
Confirmation of RiO not
being available must be
confirmed by Help Desk
before the Downtime
Process is implemented.
OOH’s the On Call
Manager will be contacted
Additional Business
Continuity Forms are
available on the RiO intranet
site
Downtime Procedure
All teams will have a “Downtime Pack”. These will include paper versions of specific forms within RiO. These
paper forms must be completed once the Business Continuity Procedure has been implemented. These
paper records must be filed in the Clients/patients Secondary Record. All information captured on these
forms must be retrospectively entered onto RiO. Each service will locally agree who will be responsible for
this retrospective entry of data.
RiO on line?
No
Helpdesk confirm
RiO is unavailable
Locally agreed person
responsible
Retrospectively enter all
information from the
paper forms into RiO
Yes
Ensure all fields on the data
validation frontsheet are
completed and signed
Complete paper forms
as appropriate and file
in the Secondary
Record
Progress note is entered
identifying Business
Continuity forms have
been entered onto RiO.
Mark the progress note
as a Significant Event
Once information has been
validated by the originator the
paper form should be destroyed as
confidential waste or shredded
Contact Help desk and
register problem
RiO Business Continuity Procedure

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
42 Appendix 5 Generic Flow
The OVERVIEW ASSESSMENT FORM within the SINGLE
ASSESSMENT is the chosen Core Assessment for Community
Services; Complete the relevant sections of this form (this includes
“Consent to Share Information”)
Case Record>Core Single Assessment Process> Overview Assessment
Referral received –
Admin/HCP
(external source)
If referral source is
internal the referral
will already be on
RiO - Go to step 3
Patient found on
Local RiO?
NoPatient found on
National Spine
1. Complete details on Business Continuity
Form
2. Contact Back Office Team for New
Registration on RiO
No
1. Update Demographic Details – Admin/HCP
Client record Icon>Registration>Search for Client>Edit this
Client
2.. Create a new referral to the Team - Admin/HCP
Client details Icon>>Entry/Exit> Create New referral
Synchronise (Import
data from spine)
STEP 1
yes
Yes
STEP 2
Is the Referral
Appropriate?
STEP 3
1. Discharge Referral as inappropriate – Admin/HCP
Client details Icon>Entry/Exit>Discharge
Inform Patient/GP/Referrer – As appropriate for your Service/Team –
Admin/HCP
NoSTEP 4a
1. Record referral Accepted date – Admin/HCP
Client Details Icon>Entry/Exit> Click on referral>enter
accepted date
2. Allocate to a HCP – lead HCP
New referrals will sit in the Lead HCP’s Caseload until
allocated to an HCP. The local team workflows will
identify whether or not your team allocates at this point.
3.Allocate a referral:
Client record Icon>Caseload>Select Lead HCP from drop
down>Click on blue icon (right hand side of case load
screen)>Allocate
Letters sent to client (if appropriate)
STEP 4
Appointment Booking - Admin/HCP:
Diary or Clinic as relevant
Diary – Appointment icon>Diary>Appointment date/time
Clinic – Appointment Icon>Clinic Appts>Clinic ID>Go>Clinic
date>Go
STEP 5
DNA: Admin/HCP
If patient DNA’s Outcome as such and either re-book or
discharge (dependant on your DNA Policy)
STEP 6
Continue
with Care?
NO
NO
Follow Up Appointments – Admin/HCP:
Diary – Appointments Icon>Diary>Go to HCP Diary>Appt Date and Time
Clinic – Clinic Appt>Clinic ID>Go>Clinic Date
Progress Notes Admin/HCP/Medics/Med Secs
Case Record>Progress Notes>Add New Note
STEP 7b
Outcome Appt HCP
Diary – Appointments Icon> HCP Diary>Appt Date and Time
Clinic – Appointments Icon>Clinic Appts>Clinic ID>Go>Clinic Date
If local team process denotes a transfer from one caseload to another after the initial
assessment; this must be done before booking any follow up appts. Client Record Icon>Entry/
Exit>Transfer
Yes
Community Services Generic Workflow
Yes
1. Discharge Referral with accurate, appropriate outcome – If
Discharge reason is DEATH, contact Back Office team
Case Record>Client referrals>Entry/Exit>Discharge
Letter to Referrer/GP/Patient – As appropriate for your Service/Team
2. If appropriate - refer to other Service for additional treatment
Case Record>Client referrals>Entry/Exit>Add new
STEP 7a
yes
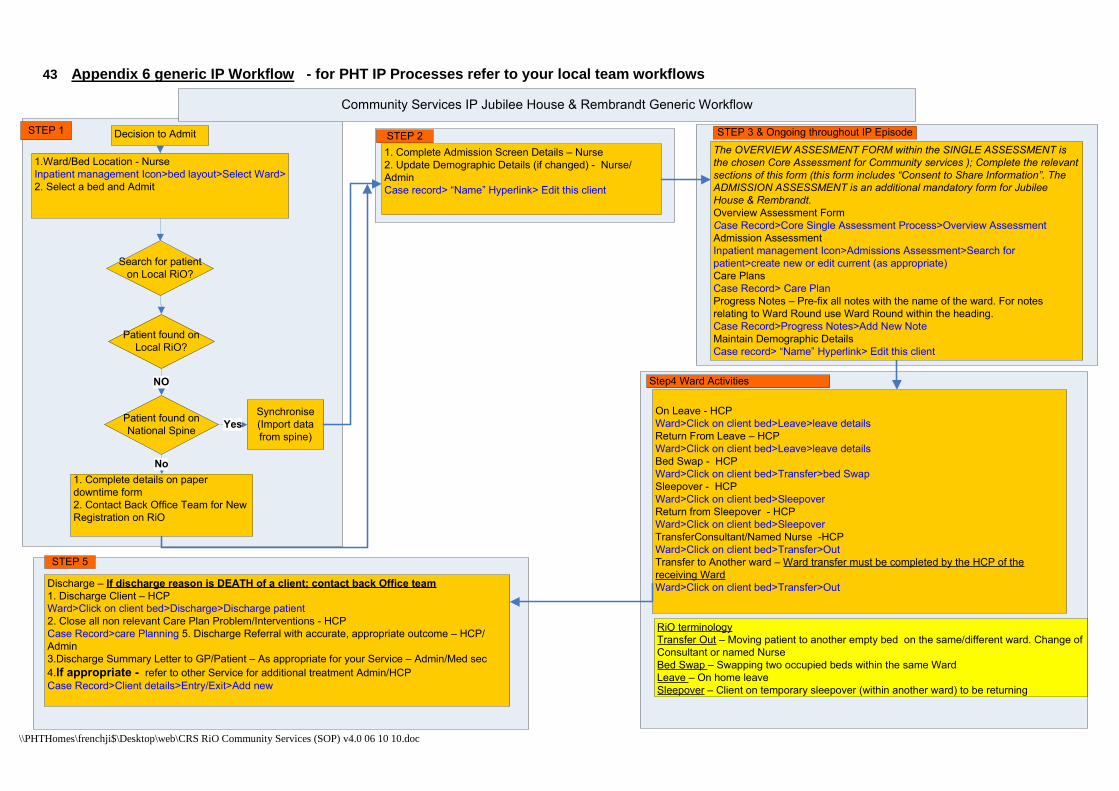
\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
43 Appendix 6 generic IP Workflow - for PHT IP Processes refer to your local team workf lows
1. Complete Admission Screen Details – Nurse
2. Update Demographic Details (if changed) - Nurse/
Admin
Case record> “Name” Hyperlink> Edit this client
STEP 2
Discharge – If discharge reason is DEATH of a client; contact back Office team
1. Discharge Client – HCP
Ward>Click on client bed>Discharge>Discharge patient
2. Close all non relevant Care Plan Problem/Interventions - HCP
Case Record>care Planning 5. Discharge Referral with accurate, appropriate outcome – HCP/
Admin
3.Discharge Summary Letter to GP/Patient – As appropriate for your Service – Admin/Med sec
4.If appropriate - refer to other Service for additional treatment Admin/HCP
Case Record>Client details>Entry/Exit>Add new
STEP 5
The OVERVIEW ASSESMENT FORM within the SINGLE ASSESSMENT is
the chosen Core Assessment for Community services ); Complete the relevant
sections of this form (this form includes “Consent to Share Information”. The
ADMISSION ASSESSMENT is an additional mandatory form for Jubilee
House & Rembrandt.
Overview Assessment Form
Case Record>Core Single Assessment Process>Overview Assessment
Admission Assessment
Inpatient management Icon>Admissions Assessment>Search for
patient>create new or edit current (as appropriate)
Care Plans
Case Record> Care Plan
Progress Notes – Pre-fix all notes with the name of the ward. For notes
relating to Ward Round use Ward Round within the heading.
Case Record>Progress Notes>Add New Note
Maintain Demographic Details
Case record> “Name” Hyperlink> Edit this client
Patient found on
Local RiO?
Patient found on
National Spine
1. Complete details on paper
downtime form
2. Contact Back Office Team for New
Registration on RiO
Synchronise
(Import data
from spine)
NO
STEP 1
1.Ward/Bed Location - Nurse
Inpatient management Icon>bed layout>Select Ward>
2. Select a bed and Admit
Decision to Admit
Search for patient
on Local RiO?
Yes
No
STEP 3 & Ongoing throughout IP Episode
On Leave - HCP
Ward>Click on client bed>Leave>leave details
Return From Leave – HCP
Ward>Click on client bed>Leave>leave details
Bed Swap - HCP
Ward>Click on client bed>Transfer>bed Swap
Sleepover - HCP
Ward>Click on client bed>Sleepover
Return from Sleepover - HCP
Ward>Click on client bed>Sleepover
TransferConsultant/Named Nurse -HCP
Ward>Click on client bed>Transfer>Out
Transfer to Another ward – Ward transfer must be completed by the HCP of the
receiving Ward
Ward>Click on client bed>Transfer>Out
Step4 Ward Activities
RiO terminology
Transfer Out – Moving patient to another empty bed on the same/different ward. Change of
Consultant or named Nurse
Bed Swap – Swapping two occupied beds within the same Ward
Leave – On home leave
Sleepover – Client on temporary sleepover (within another ward) to be returning
Community Services IP Jubilee House & Rembrandt Generic Workflow

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
44 Appendix 7 Community Nursing - First Initial Overvi ew Assessment Minimum Data Set recording requiremen ts
Overview Assessment - MANDATORY SECTIONS (to be completed when carrying out First Initial Assessmen t)
Overview Assessment - Complete these sections WHER E APPLICABLE
Client Details Health Screening Communication Psychological Wellbeing Medical History Mobility Inside Home Physical Wellbeing Mobility Outside Home Medication Assistance Equipment Activities of Daily Living Interpersonal Relationships Self Care Social Circumstances Everyday Tasks Housing Situation Assessment Summary Home Environment Record of Completion Employment Consent and Information Sharing Finances Health and Social Care Needs Nature of Caring Roles Risk Arising Carers Needs Other Assessment or Observation Assessment Circulation Family and Carers

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
45 Appendix 8 Occupational Therapy Overview Assessment (SAP) Minimum Data Set recording requirements
Overview Assessment - MANDATORY SECTIONS (to be completed when carrying out First Initial Assessmen t)
Overview Assessment - Complete these sections WHER E APPLICABLE
Client Details Physical Wellbeing Formal Care/Support currently received Health Screening Communication Medication Medical History Interpersonal Relationships Psychological Wellbeing Activities & Employment Activities of Daily Living Finances Self Care Family & Carers Everyday Tasks Nature of Caring Roles Mobility Inside Home Carers Needs & Concerns Mobility Outside Home Health and Social Care Needs Assistance Equipment Assessment Circulation Social Circumstances/Housing Situation Other Assessment or Observation Home Environment Assessment Summary Risk Arising Consent and Information Sharing Record of Completion

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
46 Appendix 9 Physiotherapy Overview Assessment (SAP) Minimum Data Set recording requirements – THIS APPL IES TO COMMUNITY PHYSIO TEAMS COMPLETING THE SAP. IN-PATIENT & OUTPA TIENT TEAMS MUST CONTINUE USING THE PAPER ASSESSMEN T TEMPLATES IN ACCORDANCE WITH THE PHYSIOTHERAPY RECO RD KEEPING STANDARDS.
Overview Assessment - MANDATORY SECTIONS (to be completed when carrying out First Initial Assessmen t)
Overview Assessment - Complete these sections WHER E APPLICABLE
Client Details Health Screening Formal Care/Support currently received Housing Situation Mobility Inside Home Home Environment Mobility Outside Home Psychological Wellbeing Medication Physical Wellbeing Communication Social Circumstances Medical History Assistance Equipment Activities of Daily Living Interpersonal Relationships Self Care Health and Social Care Needs Everyday Tasks Employment Assessment Summary Finances Record of Completion Nature of Caring Roles Consent and Information Sharing Carers Needs Risk Arising Other Assessment or Observation Assessment Circulation Family & Carers

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
47 Appendix 10 Appointment Outcome Activities by Servi ce District Nursing
District Nursing Intermediate Care – Appointment Outcome Activities Adult Protection Assessment for Equipment Blood Glucose Monitoring Blood Pressure Management Bladder care Bowel care Care Support/Training Case Conference Continuing Care Assessment Discharge Planning Exercise Health Promotion Advice Home Assesment Intervention Joint Visit Medication – Intravenous Route Mental Health Wellbeing Nerve Conduction Observations Oral Medication Personal Care Phlebotomy Planning Meeting Planning Meeting (Client) Pressure Ulcer Care 1 Pressure Ulcer Care 2 Pressure Ulcer Care 3 Pressure Ulcer Care 4 Review Triage/Pre Assessment Wheelchair Assessment
District Nursing Specialist Palliative Care Adult Protection Bereavement Support Attend Strategy Meeting Child Protection Case Conference Consultant Domiciliary Visit Chronic Disease Management Educator Discharge Planning Funeral Attendance Emotional & Psychological Support Group Education Gait Re-education Therapy Home Visit Health Promotion Advice Liaison Initial Assessment Medication-Injection Lymphodema Neurological Therapy Medication-Prescription Pain Management Nutritional Advice Patient Rehabilitation Palliative Care-Symptom Control Prevention of Admission to Hospital or Institutional
Care Pre-admission Assessment Referral with this Service Provision of Aids Review Respiratory Management Review of Equipment Review of Medication Treatment Risk Assessment Venepuncture

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
District Nursing Clusters
Adult Protection Accident Prevention Advice Assessment for Equipment Assessment for free Nursing Care Assessment for free nursing home care Attend Strategy Meeting Bandaging Bereavement Support Bowel care Carer Support/Training Case Conference Catheter Management Central Line care Child Protection Chronic Disease Management Clinic Preparation Complex Assessment (SAP) Continence Advice Continence Assessment Continuing Care Assessment Diabetes Care Discharge Planning Ear Syringing Educator Support/Training Emotional & Psychological Support Equipment Demonstration Equipment Review Follow Up of Emergency Department Attendance Health Promotion Influenza/Pneumococcal Immunisation Initial Assessment Liaison Lymphodema Management of Leg Ulcer Management of Pressure areas Medication – Ear Drops Medication – Eye drops Medication - Injection Medication - Intravenous Route Medication – Rectally Medication - Syringe Driver Medication via NG Tube Medication via PEG Network Meeting Nutritional Assessment Nutritional Monitoring Observations Oral Medication Pain Management Palliative Care- Symptom Control Personal Care Planning meeting Prevention of Admission to Hospital or Institutional
Care Pressure Ulcer Care 1 Pressure Ulcer Care 2 Pressure Ulcer Care 3 Pressure Ulcer Care 4 Reassessment Respiratory Management Review Review Medication Review of Equipment Risk Assessment Sample taking non Venepuncture Smoking Cessation Suture/Clip Removal Venepuncture Wound Care Writing Case Records/Reports

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
District Nursing Community Matrons
Adult Protection Advice Re-Sexual Dysfunction Advice Assessment for Equipment Assessment for Continuing Care Bereavement Support Bowel Care Carer Support/Training Case Conference Catheter Management Central Line Care Chronic Disease Management Clinic Preparation Complex Assessment (SAP) Consultancy Domiciliary Visit Continence Advice Continuing Care Assessment Counselling Diabetes Care Discharge Planning Educator Support/Training Emotional & Psychological Support Equipment Demonstration Equipment Review External Review First Appointment/Treatment First Appointment Triage/Pre Assessment Follow Up of Emergency Department Attendance Group Attendance Health Promotion Influenza/Pneumococcal Immunisation Initial Assessment Joint Visit Liaison Lymphodema Management of Leg Ulcer Medication – Ear Drops Medication – Eye drops Medication - Injection Medication - Intravenous Route Medication – Rectally Medication - Syringe Driver Medication Prescription Mental Health Wellbeing Medication via NG Tube Medication via PEG Nutritional Assessment Nutritional Monitoring Oral Medication Pain Management Palliative Care- Symptom Control Planning Meeting Pressure Ulcer Care 1 Pressure Ulcer Care 2 Pressure Ulcer Care 3 Pressure Ulcer Care 4 Prevention of Admission to Hospital or Institutional Care
Reassessment
Respiratory Management Review Review Medication Smoking Cessation Strategy Meeting Suture/Clip Removal Urine Analysis Wound Care

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
District Nursing Bladder & Bowel Adult Protection Attend Strategy Meeting Bladder care Bowel Care Carer Support/Training Case Conference Catheter Management Continence Advice Continence Assessment Continence Clinic Initial Assessment Continence Clinic Review Educator Support/Training Enuresis Assessment Enuresis Review Group Education Gynaecological treatment – other Health Promotion Home Visit Influenza/Pneumococcal Immunisation Initial Assesment Liaison Management of Pressure Areas Menopause Advice Nutrition Assessment Nutritional Monitoring Observations Other Client Related Meeting Pain Management Pressure Ulcer Care 1 Pressure Ulcer Care 2 Pressure Ulcer Care 3 Pressure Ulcer Care 4 Provision of Aids Reassessment Review Risk Assesment Setting up Clinics Stoma Care Suture/Clip removal Training with Carer Treatment Triage/Pre assessment Ultrasound Urethral Swab Urine Analysis Venepuncture
District Nursing Tissue Viability
Adult Protection Advice Attend Strategy meeting Bandaging Carer Support/Training Case Conference Compression Bandaging Doppler Assessment Equipment Assessment Equipment Demonstration Equipment Review Group Education Health Promotion Home Visit Influenza/Pneumococcal Immunisation Initial Assessment Leg Ulcer Prevention Liaison Lymphodema Management of leg ulcer Management of pressure areas Medication Prescription Nutritional Assessment Nutritional Monitoring Observations Other Client Related Meeting Pain Management Pressure Ulcer Care 1 Pressure Ulcer Care 2 Pressure Ulcer Care 3 Pressure Ulcer Care 4 Reassessment Review Risk Assessment Setting up Clinics Skin – Leg Ulcer Care Stoma Care Strategy Meeting Suture/Clip Removal Triage/Pre Assessment Ultrasound Vascular Assessment Venepuncture Wound Care Wound Care –fungating Wound Care – post operative Wound Care – post trauma Writing Case Records/Reports

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
District Nursing Out of Hours
Accident Prevention Adult Protection Advice Assessment for Equipment Attend strategy meeting Bereavement Support Bowel Care Carer Support/Training Case Conference Catheter Management Central Line Care Child Protection Chronic Disease Management Clinic Preparation Continence Advice Diabetes Care Discharge Planning Equipment Demonstration Equipment Review Follow up of Emergency Department Attendance Health promotion Influenza/Pnuemococcal immunisation Initial Assessment Liaison Lymphodema Management of leg ulcer Management of pressure areas Medication – Ear Drops Medication – Eye Drops Medication – Injection Medication – Rectally Medication – Syringe Driver Medication via NG tube Medication via PEG Network Meeting Nutritional Assessment Obesity Advice Observations Oral Medication Pain Management Palliative Care – Symptom Control Personal care Planning Meeting Pressure Ulcer Care 1 Pressure Ulcer Care 2 Pressure Ulcer Care 3 Pressure Ulcer Care 4 Prevention of Admission to Hospital or Institutional
Care Reassessment Respiratory Management Review Risk Assessment Sample Taking – Non Venepuncture Smoking Cessation Suture/Clip Removal Wound Care Writing Case Record/Reports

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
48 Appendix 11 Appointment Outcome Activities by Servi ce Therapists
Musculoskeletal OP Physio’s Advice Advice Re-Gynaecological Problem Balance Therapy Continence Assessment Exercise Gait Re-Education Therapy Hydrotherapy Initial Assessment Mobility Therapy Manual Therapy – Joint Manual Therapy – Soft Tissue Postural Management Provision of Aids Patient Rehabilitation Review Bursa – Injection into Triage/Pre Assessment Technical – Acupuncture Treatment Technical – Ultrasound Ultrasound Back Class Continence Advice Electrotherapy Hand Therapy Interferential Therapy Knee Class Obesity Advice Risk Assessment Shoulder Class Splinting of Hand Musculoskeletal Intervention Antenatal Assessment Pain Management First Appointment, Triage/Pre-Assessment Gait Analysis Group Session Strengthening Stretching Injection of Therapeutic substance into joint
Physiotherapy IP Carer Support/Training Exercise Health Promotion Advice Hydrotherapy Initial Assessment Intervention Mobility Therapy Respiratory Management Adult Protection Assessment – Respiratory Multidisciplinary intervention Attend review child protection conference Assessment for Equipment CAF Case Conference Discharge Planning Home Assessment Visit Nerve Conduction Studies

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
Community Rehab Physio’s
Carer Support / Training Equipment Assessment Exercise Therapy Exercise Group Education Gait Re – Education therapy Health Promotion Advice Health Review Hydrotherapy Initial Assessment Intervention Joint Visit Mobility Therapy Neurological Therapy Orthotics Postural Management Respiratory Management Therapy / Treatment Adult Protection Assessment – respiratory Equipment Demonstration Falls Group Neuro- developmental Therapy Prevention of admission to hospital or institutional
care Promotion of Mobility Pulmonary Rehabilitation Respiratory – Treatment Risk Assessment Musculoskeletal Intervention Child Assessment Working with teacher Multi-disciplinary assessment Multi-disciplinary review with child Multi-disciplinary review without child Prematurity at risk follow up Assessment for equipment CAF Case Conference Children’s Development Team Meeting Discharge Planning Equipment Check Equipment Review First Appointment, Treatment First Appointment, Triage/Pre-Assessment Group Session Home Assessment Visit Home Visit Nerve Conduction Studies Nursery/Playgroup Visit Planning Meeting School Appointment Splinting Teach a Programme Wheelchair Assessment
Chronic Fatigue Advice Equipment Assessment Full Assessment Joint Visit Liaison Review Therapy/Treatment Equipment Demonstration Environment Adaptations Case Conference Equipment Check Equipment Review First Appointment Treatment Group Session Home Assessment Visit Other Client Related Meeting Writing Case Record/Reports

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
Occupational Therapy
Activities of Daily Living Advice Carer Support/ Training Equipment Assessment Full Assessment Home Assessment Initial Assessment Intervention Joint Visit Mental Health Wellbeing Neurological Therapy Postural Management Review RTT – First definitive treatment Triage / Pre Assessment Continuing Care Assessment Falls Group Pulmonary Rehabilitation Risk Assessment Transfer Practice Environment Adaptations Mobilising Overview Assessment (SAP) Discharge Planning Equipment Review Group Session Home Assessment Visit Link Assessment Planning Meeting Wheelchair Assessment
Speech and Language Advice Carer Support/Training Liaison Review Therapy/Treatment Alternative and Augmentative Communication
Intervention Multi-disciplinary assessment Assessment Communication Assessment Swallow Case Conference Group Session Initial Assessment Communication Initial Assessment Swallow Writing Case Record/Reports
Neuro Psychology Advice Admission Assessment Carer Support /Training Full Assessment Initial Assessment Intervention Liaison Observations Patient Rehabilitation Review Therapy / Treatment Adult Protection Parenting Advice Risk Assessment Multidisciplinary Intervention Parent / Child Interaction Reassessment Emotional and Psychological Support Training with carer Multi – Disciplinary assessment Obtaining further history Case Conference Group session Home visit Other Client Related Meeting Writing Case Record/Reports

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
Pain Management
Advice Advice Re – Gynaecological Problem Balance Therapy Continence Assessment Exercise Gait Re – Education Therapy Hydrotherapy Initial Assessment Mobility Therapy Manual Therapy – Joint Manual Therapy – Soft Tissue Postural Management Provision of Aids Patient Rehabilitation Review Bursa – injection into Triage / Pre Assessment Technical – Acupuncture Treatment Technical – TENS Technical– Ultrasound Ultrasound Back Class Continence Advice Electrotherapy Hand Therapy Interferential Therapy Knee Class Obesity Advice Risk Assessment Shoulder Class Splinting of Hand Hand Function Assessment Musculoskeletal Intervention Antenatal Assessment Pain Management Injectable Consultation First Appointment, Triage/Pre Assessment Gait Analysis Group Session Strengthening Stretching Writing Case Records/Reports Injection of therapeutic substance into joint.

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
Podiatry Excision of lesion of peripheral nerve Activities of Daily Living Advice Biomechanics Carer Support/ Training Chemical Therapy Domiciliary Foot Care Nutritional Counselling Diabetic Foot Screen Exercise Therapy Foot Care Full Assessment Group Education Gait Re-Education therapy Home Assessment Health Education preparation Health Promotion Health Promotion Advice Health Review Initial Assessment Intervention Joint Visit Manual Therapy – Joint Manual Therapy – soft Tissue Nutritional Assessment Nutritional Advice Nutritional Monitoring Non Pathological Nail Care Nail surgery Orthotic Casting Orthotic Manufacture Orthotic Fitting Orthotics Padding Therapy Patient Rehabilitation Patient Support Curettage and cauterisation of lesion of skin ned Chemical peeling of lesion of skin Drainage of lesion of skin nec Incision of lesion of skin nec Incision of skin nec Insertion of steroid into subcutaneous tissue Insertion of therapeutic substance into subcutaneous tissue
Nail re-dressing
Bilateral partial nail avulsion Plantar fasciectomy Excision of lesion of fascia Freeing of adhesions of fascia Ganglion excision Bursa – total excision Bursa – aspiration Bursa – injection into Lengthening of tendon Accident Prevention Child Protection Chronic Disease Management Diabetes Care Equipment Demonstration Falls Group Hygiene Injection Therapy Management of pressure areas Obesity Advice Obesity Prevention Patient Training Personal care Prevention of Admission to Hospital or Institutional Care
Educator Support /Training
Multidisciplinary Intervention Musculoskeletal Intervention Pressure Ulcer Care 1 Pressure Ulcer Care 3 Post Operative Care Child assessment Complex Assessment (SAP) Post operative complication Pressure Ulcer Care 2 Doppler Assessment Immunisation Advice Multi – disciplinary assessment Multi- disciplinary review with child Multi-disciplinary review without child External referral Implant check Implant consultation Implant fitting Implant removal Injectable administration –other Assessment for Equipment Bio Feedback Case Conference Children’s development team meeting Core group Meeting Discharge Home Visit Discharge Planning Equipment Check Equipment Review First Appointment, Treatment First Appointment, Triage/Pre assessment Gait Analysis Group Session Home Assessment Visit Home Visit Initial Assessment Communication

\\PHTHomes\frenchji$\Desktop\web\CRS RiO Community Services (SOP) v4.0 06 10 10.doc
Leg Ulcer Prevention Multi Disciplinary Special Needs Meeting Pressure Ulcer Care 4 Multiple metatarsal head excisions Multiple metatarsal excisions Claw toe – total correction Excision of natural protuberance of bone nec. Excision of overgrowth of bone Excision of excrescence of bone Excision of fragment of bone Open osteoclasis and angular correction and internal fixation hfq
Open osteoclasis and angular correction and external fixation hfq
Open osteoclasis and angular correction nec Open osteoclasis and internal fixation nec Closed osteoclasis Displacement osteotomy Osteotomy of neck of 1st metatarsal bone Osteotomy of base of 1st meatatarsal bone Osteotomy of 1st metatarsal bone Osteotomy of head of metatarsal bone Osteotomy of midfoot tarsal bone Multiple osteotomies & internal fixation Multiple osteotomies & external fixation Ostoeotomy multiple nec Adjustment to external fixation of bone nec Primary excision arthroplasty of 1st MTPJ Primary excision arthroplasty of joint nec Fusion of 1st Metatarsophalangeal joint nec Fusion of ipj hallux Fusion of ipj lesser toe Fusion revision – of joint of toe Conversion to fusion of other joint Excision of bunion nec Injection of therapeutic substance into joint Injection onto joint nec Amputation of great toe Amputation of phalanx of toe Amputation revision (reamputation at higher level) Curly 5th toe correction Crossed toe Injection of steroid into subcutaneous tissue Injection of therapeutic substance into subcutaneous
tissue