Embed Size (px)
Citation preview
1
Slide 1JSOMTC, SWMG(A)
SOCMOverview: Physical Exam
and History Taking PFN: SOMPYL11
Hours: 3.0
Slide 2JSOMTC, SWMG(A)
Terminal Learning Objective Action: Communicate knowledge of “Overview: Physical Exam and History Taking"
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% IAW course standards on the formative quizzes and the Physical Exam Practical Test grade sheet
Slide 3JSOMTC, SWMG(A)
References
Bates’ Guide to Physical Examination And History Taking (11th edition; 2013; Lynn S. Bickley)
Evidence‐Based Physical Diagnosis (3rd
edition; 2012; Steven McGee)

2
Slide 4JSOMTC, SWMG(A)
Reason
As a SOF medic, you may find yourself in austere environments that will limit your medical resources and test your diagnostic capabilities. Your ability to obtain patient history, perform a thorough physical exam and come to a correct diagnosis may save your patient's life.
Slide 5JSOMTC, SWMG(A)
Agenda
Identify the components of a Comprehensive Physical Exam
Communicate the Techniques of a Patient interview and Head‐to‐Toe Exam
Identify the basic concepts of evidence‐based medicine and clinical reasoning
Identify the components of a clear and accurate SOAP note
Slide 6JSOMTC, SWMG(A)
The Components of a Comprehensive Physical Exam

3
Slide 7JSOMTC, SWMG(A)
Comprehensive Physical Exam
Determining the scope of your assessment
Comprehensive
• appropriate for new patients (provides baseline)
• can be time‐intensive
• suitable for enlistment screening (e.g., UW, FID, etc.) and special schools (e.g., MFF, scuba, Ranger, etc.)
Focused
• problem‐oriented assessment
• generally restricted to a specific body system
• applies same techniques as comprehensive exam
Slide 8JSOMTC, SWMG(A)
Comprehensive Physical Exam
SOAP Format
Subjective
• interview (history) – all the patient tells you
• often under‐stressed!
Objective
• physical exam – your detections
•methodical approach to reduce omissions
Assessment – diagnosis (include differentials)
Plan – treatment (include follow‐up tests/visits)
Slide 9JSOMTC, SWMG(A)
Comprehensive Physical Exam
Prepare for Success
Follow personalized sequence of exam
Check all equipment
Remain professional
Document everything
• this includes negative findings as well as positive
• assure modesty, privacy, and accountability

4
Slide 10JSOMTC, SWMG(A)
Comprehensive Exam
Identification
Chief complaint(s)
History of present illness
Past medical history
Family history
Social history
Review of systems
Slide 11JSOMTC, SWMG(A)
Comprehensive Exam
Identification (ID)
Data
• age, gender, occupation, marital status
• primary physician and/or guardian if applicable
Source
• usually the patient
• can be family member, friend, medical records, etc.
Reliability – varies according to the patient's memory, trust, and mood
Slide 12JSOMTC, SWMG(A)
Comprehensive Exam
Chief Complaint (CC)
Reason for visit
• could be one or many
• could be simply for check‐up or screening
Should be brief

5
Slide 13JSOMTC, SWMG(A)
Comprehensive Exam
History of Present Illness (HOPI/HPI)
Further develops CC
OPQRST
•Onset – general duration? (e.g., acute, chronic, etc.)
• Provocation/palliation – what makes it worse/better?
•Quality – “feels like…” (e.g., sharp, nauseating, etc.)
• Radiation – does it extend to other areas?
• Severity – 0 to 10 (for future reference)
• Time – how long? (possible intervals)
Slide 14JSOMTC, SWMG(A)
Comprehensive Exam
HOPI (cont.)
SAMPLE
• Signs/symptoms – associated with the CC
• Allergies – drug, food, environmental, etc.
•Medications – prescribed, OTC, supplements, etc.
• Past pertinent history – detailed history of CC
• Last oral intake – food & drink (include ETOH/H2O)
• Events leading up to illness/injury
Slide 15JSOMTC, SWMG(A)
Comprehensive Exam
Past Medical History (PMHx)
Past relevant illnesses/injuries
Past major illnesses
Childhood illnesses
Past surgeries
Immunizations
Current ongoing illnesses (e.g., DM, HIV, etc.)

6
Slide 16JSOMTC, SWMG(A)
Comprehensive Exam
Family History (FHx)
Age/health or age/cause‐of‐death
• blood siblings
• parents
• grandparents
Presence/absence of specific illnesses
• could point to cause of CC
• examples: HTN, CAD, type 2 DM
Slide 17JSOMTC, SWMG(A)
Comprehensive Exam
Social History (SHx)
Living arrangements
Number of children (female: GPA)
Drug use
• includes tobacco, ETOH, recreational drugs, etc.
• includes quantity and frequency
Foreign travel
Recent activities/exposures
Sleep
Slide 18JSOMTC, SWMG(A)
ROS
Review of Systems (ROS)
Constitutional
• generally non‐specific
• weight loss, malaise, fever, fatigue, etc.
HEENT
• changes in vision can be a key indicator
• epistaxis, sinus pn, tinnitus, sore throat, etc.
CV
• heart – chest pn, orthopnea, palpitations, etc.
• peripheral – claudication, edema, etc.

7
Slide 19JSOMTC, SWMG(A)
ROS
Resp
• association with CV could be unknown to pt
• coughing, wheezing, SOB, exercise intolerance, etc.
GI
• common: diarrhea, constipation, abd pn, anorexia, etc.
• red flags: hematemesis, hematochezia, melena, etc.
GU
•male: testicular pn, decreased force of stream, etc.
• female: LMP, dysmenorrhea, contraception, etc.
• both: incontinence, dysuria, hematuria, etc.
Slide 20JSOMTC, SWMG(A)
ROS
MSK
• symptoms often change over time
• pn, decreased ROM, stiffness, joint swelling
Integ
• should include recent minor abrasions/lesions
• pruritus, rashes, eczema, excessive dryness, etc.
Neuro
• symptoms may appear in other systems
• HA, seizures, disequilibrium, higher mental functions, numbness/weakness/paresthesia, etc.
Slide 21JSOMTC, SWMG(A)
ROS
Psych – depression, anxiety, sleep patterns, etc,
Endocrine
• thyroid – sweating, cachexia, skin/hair, etc.
• diabetes – polydipsia, polyuria, polyphagia, etc.
• adrenal – orthostatic symptoms, etc.
Blood/lymph – prolonged/excessive bleeding, petechia, etc.
Allergic/immune – unusual sneezing, swollen lymph nodes, rhinorrhea, etc.

8
Slide 22JSOMTC, SWMG(A)
The Techniques of a Patient Interview and Head‐to‐Toe Exam
Slide 23JSOMTC, SWMG(A)
Interviewing Techniques
Approaching an Interview
Review medical records
• this may require leg‐work
• have medical records translated if necessary
• ensure you properly continue patient records
Slide 24JSOMTC, SWMG(A)
Interviewing Techniques
Approach (cont.)
Prepare clinical setting
• safe setting for yourself/patient is priority
• ensure proper lighting
• prepare any privacy requirements
• procure an interpreter if necessary (medical knowledge is preferred)
• procure a chaperone if necessary

9
Slide 25JSOMTC, SWMG(A)
Interviewing Techniques
Difficult Patients
Different levels of education/capacity
• include low literacy, vision/hearing impaired, etc.
• explain in simple terms, but avoid being perceived as condescending
• pts with medical knowledge can be a challenge
Altered compliances
• can range from silent pts to angry pts
• informed consent is ethical, not just U.S. law
Slide 26JSOMTC, SWMG(A)
Interviewing Techniques
Difficult Topics
Remain objective and non‐judgmental
Sexual history
• especially sensitive in women (but not exclusively)
• attempt to isolate pt if guardian is present
Mental health history
• can be perceived as a stigma
• emphasize confidentiality (esp. in teammates)
• in poor countries, this frequently presents as a Hxof “communicating with the spirit world”
Slide 27JSOMTC, SWMG(A)
Interviewing Techniques
Difficult Topics (cont.)
Alcohol and illicit drug use
Family violence
•maintain cultural awareness
• be perceptive of key indicators
injuries that are unexplained, recurring, inconsistent with Hx, etc.
these do not always indicate abuse!
Death and the dying patient (5 stages)

10
Slide 28JSOMTC, SWMG(A)
Interviewing Techniques
Cultural Differences
Imperative: maintain self & cultural awareness!
• local culture dictates acceptable behavior
•mistakes can quickly lead to lost rapport
Can differ greatly amongst people & areas
• area studies should include differences in culture
•many differences can occur within a small area
Slide 29JSOMTC, SWMG(A)
Interviewing Techniques
Cultural Differences (cont.)
Culture – the total of inherited ideas, beliefs, values, and knowledge, which constitute the shared bases in a society
Ethics – the rules of conduct recognized in respect to a particular culture
Morals – the personal and variable principles of right and wrong
Slide 30JSOMTC, SWMG(A)
The Techniques of a Head‐to‐Toe Exam

11
Slide 31JSOMTC, SWMG(A)
Head‐to‐Toe Exam Techniques
Inspection
Auscultation
Palpation
Percussion
Slide 32JSOMTC, SWMG(A)
Head‐to‐Toe Exam Techniques
Inspection (appearance, behavior, mvmt)
Physique, posture, contours, clothing
Symmetry, deficits, patterns, color
Facial expression, mood, eye movements
Manner of speaking & potential guarding
Gait & off‐setting movements
Respiratory variations
Tremors, tics, spasms
Slide 33JSOMTC, SWMG(A)
Head‐to‐Toe Exam Techniques
Auscultation
Not restricted to the lungs and heart!
Stethoscope
• diaphragm
primarily transmits high‐pitched frequencies
generally ideal in almost all situations
• bell – primarily transmits low‐pitched frequencies
• highly dependent on the model of stethoscope and operator expertise

12
Slide 34JSOMTC, SWMG(A)
Head‐to‐Toe Exam Techniques
Palpation
Elevation/depression/deformities
Temperature
Tenderness
Lymph nodes
Pulses
Crepitus in the joints
Contours & sizes of organs/masses
Slide 35JSOMTC, SWMG(A)
Head‐to‐Toe Exam Techniques
Percussion
Results vary greatly by patient and expertise
Technique
• use of a plexor to tap/strike the pleximeter
• evokes a subtle sound wave (e.g., resonance, dullness, etc.)
Only appropriate in quiet, controlled settings
Slide 36JSOMTC, SWMG(A)
Head‐to‐Toe Exam Techniques
Notes on IAPP/IPA/etc.
Generally follow the rule “least invasive to most invasive”
Order of progression differs depending on the system being examined
• lungs – inspection, auscultation, palpation, palpation
• abd – inspection, auscultation, light palpation, deep palpation, percussion of liver span
•msk – inspection, palpation, active ROM, passive ROM, against resistance

13
Slide 37JSOMTC, SWMG(A)
Head‐to‐Toe Exam
General Survey / Vital Signs
Skin, Hair, & Nails
Musculoskeletal
Neurological
Head, Ears, Eyes, Nose, & Throat (HEENT)
Thorax and Abdomen
Reproductive
Slide 38JSOMTC, SWMG(A)
Head‐to‐Toe Exam
General Survey / Vital Signs
General appearance
• begins the moment you encounter the pt
• note level of consciousness
Apparent state of health
• skin color
• build
• body symmetry
• dressing, grooming, and hygiene
Slide 39JSOMTC, SWMG(A)
Head‐to‐Toe Exam
General Survey / Vital Signs (cont.)
Apparent state of health (cont.)
• facial expressions
• body odors
• posture, gate, motor capability
• signs of distress
Vital signs
• P/R/BP at a minimum! (don’t forget about qualities)
• consider SpO2, Temp, orthostatics, cap refill, and pain scale (if appropriate)

14
Slide 40JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Skin, Hair, and Nails
Skin
• correct lighting can be paramount!
consider amount and position
different types (i.e., natural vs. artificial)
• thorough inspection required
any little thing missed can be huge
check color, moisture, temp, texture, mobility/turgor, moles/lesions
• ensure patient modesty when appropriate
Slide 41JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Hair
• include head and body
• note amount, pattern, distribution, texture, etc.
Nails
• include fingers and toes
• findings can be genetically, pathologically, and/or habitually related
Slide 42JSOMTC, SWMG(A)
Head‐to‐Toe Exam
HEENT
Head and face should be checked for general abnormalities and trauma
Eyes (including fundoscopy)
• visual acuity (OU, OD, and OS)
• shape and reactivity of pupils (before & after PERRL)
• extraoccular movements (EOM: LR6, SO4, R3)
• color and clarity of sclera
• fundus and microcirculation
15
Slide 43JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Ears, to include the tympanic membrane (TM), should checked for impaction and inflammation
Nose should be checked for patency and deviation
Throat should be examined for abnormalities
Also included mouth, teeth, and neck!
Slide 44JSOMTC, SWMG(A)
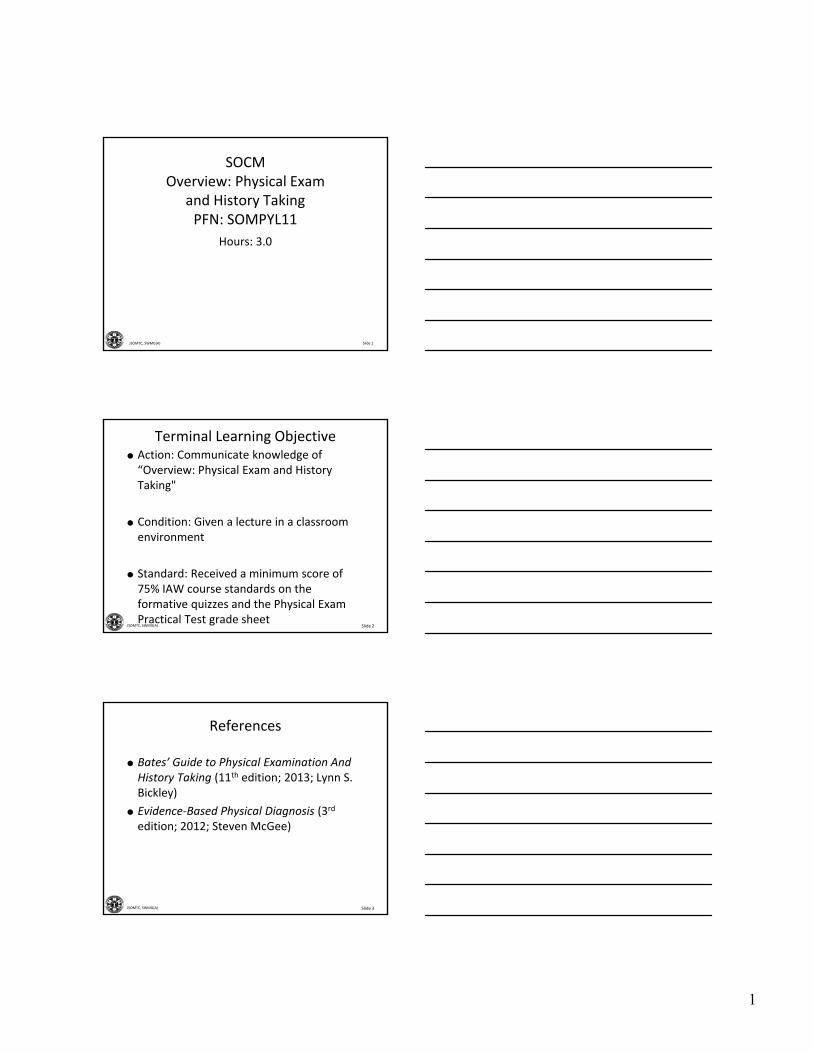
PMH Matters
Patient reports a history of going SCUBA diving 3 days prior. Patient states he completed one dive in salt water which was to 55 feet for 30 minutes.
Slide 45JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Thorax and Abdomen
Chest and Lungs
• symmetry, work of breathing, and tenderness
• auscultation and percussion of multiple fields
Heart (CV)
• auscultation of rate, rhythm, and heart sounds
•manual blood pressure
• peripheral circulation and pulses
16
Slide 46JSOMTC, SWMG(A)
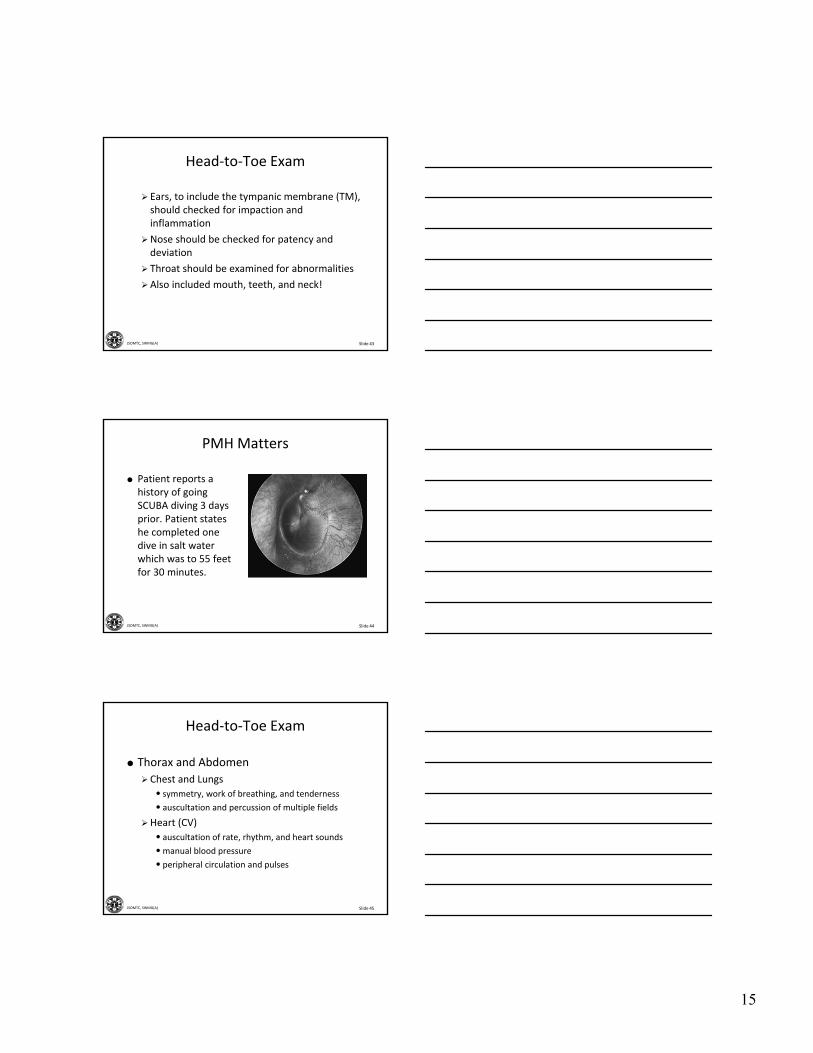
Head‐to‐Toe Exam Techniques
Slide 47JSOMTC, SWMG(A)
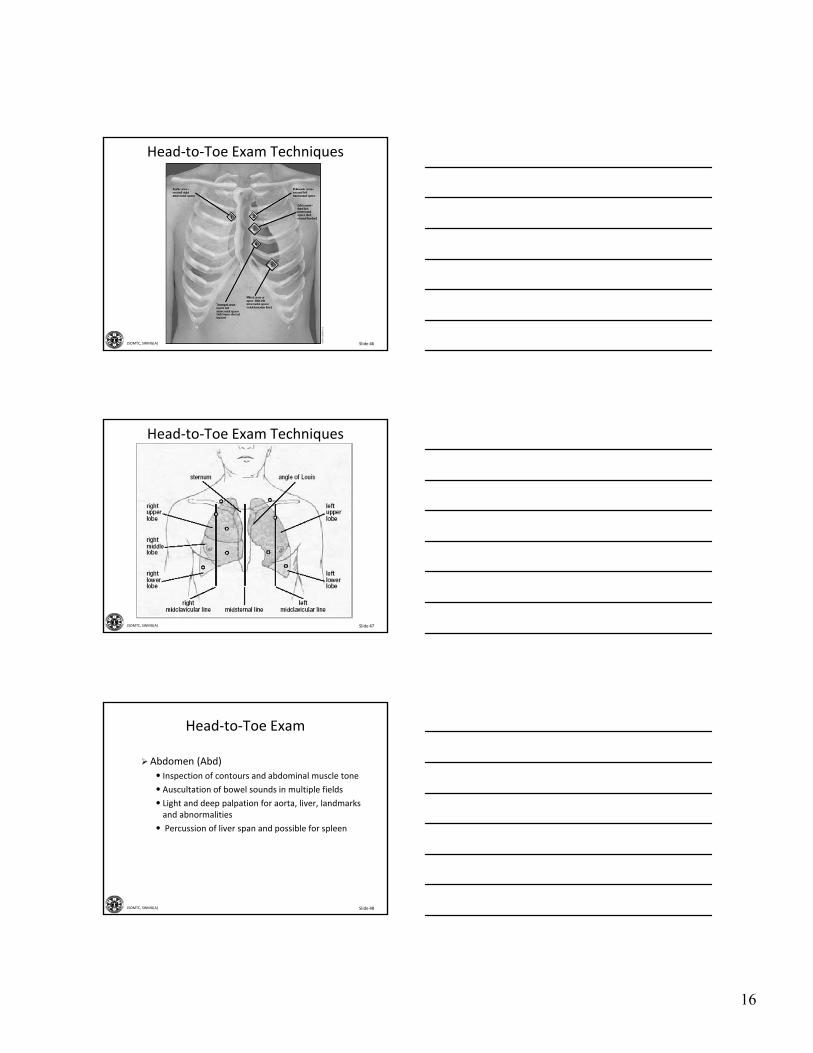
Head‐to‐Toe Exam Techniques
Slide 48JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Abdomen (Abd)
• Inspection of contours and abdominal muscle tone
• Auscultation of bowel sounds in multiple fields
• Light and deep palpation for aorta, liver, landmarks and abnormalities
• Percussion of liver span and possible for spleen

17
Slide 49JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Musculoskeletal (MSK)
Inspection and palpation of joints and landmarks
Active range of movement (ROM) & strength for all extremities/spine
Passive ROM & special tests
Slide 50JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Neurological
Mental status – more than just A&Ox3!
Cranial nerves (CN I – XII)
Cerebellar function
Muscle tone and strength
Sensory perception
Applicable reflexes (e.g., DTRs, Babinski, etc.)
Slide 51JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Reproductive
Breast – always have chaperone present
Female genitalia (see above)
• inspect and palpate external genitalia
• inspect internal genitalia with speculum and perform bimanual exam (don’t forget the anus)
Male genitalia
• inspect and palpate the dangling participles
• perform digital rectal exam (DRE)

18
Slide 52JSOMTC, SWMG(A)
Head‐to‐Toe Exam
Key Points
Generally, focused PE will not require an examination of most of the organ systems
The ability to recognize “normal” helps to catch the “abnormal”
Findings may present differently in healthy patients (i.e., “normal” is only relative to each individual)
Slide 53JSOMTC, SWMG(A)
The Basic Concepts of Evidence‐Based Medicine and
Clinical Reasoning
Patient History
Physical ExamDia
g.
Patient History
Physical ExamDiagnostics
"Normal" U.S. Healthcare Provider SOCM
Slide 54JSOMTC, SWMG(A)
Evidence‐Based Medicine
Evaluating Clinical Evidence
Patient history, physical exam findings, & diagnostic results are inherently imperfect
Gold standard
• the most accurate and precise test possible
• usually MRIs, arthroscopy, endoscopy, etc.
Alloyed gold standard
• best available test under constrained conditions
• SOCM often must rely on these tests/combinations

19
Slide 55JSOMTC, SWMG(A)
Evidence‐Based Medicine
Understanding the Evidence
Reliability
• indicates how well repeated measurements yield the same result
• often associated with the precision of a test
• intra‐observer reliability vs. inter‐observer reliability
Validity
• indicates how closely a given observation agrees with “the true state of affairs”
• often associated with the accuracy of a test
Slide 56JSOMTC, SWMG(A)
Evidence‐Based Medicine
Validity (cont.)
• Sensitivity
identifies the proportion of people who test positive in a group of people known to have the disease or condition
“SnNout” – when sensitivity is high, a negative result rules out a disease/disorder
positive results may mean very little
Slide 57JSOMTC, SWMG(A)
Evidence‐Based Medicine
Validity (cont.)
• Specificity
identifies the proportion of people who test negative in a group of people known to be without a given disease or condition
“SpPin” – when specificity is high, a positive result rules in a disease/disorder
negative results may mean very little

20
Slide 58JSOMTC, SWMG(A)
Evidence‐Based Medicine
Test Findings
True positive – correctly identified (sick people correctly diagnosed as sick)
False positive – incorrectly identified (healthy people incorrectly diagnosed as sick)
True negative – correctly rejected (healthy people correctly identified as healthy)
False negative – incorrectly rejected (sick people incorrectly identified as healthy)
Slide 59JSOMTC, SWMG(A)
Evidence‐Based Medicine
Predictive values
• based on the prevalence of a disorder in a defined population (i.e., can change in different AOs)
• “positive” predictive value – probability that a positive result reflects the condition being tested
• “negative” predictive value – probability that a negative result reflects a health individual
Slide 60JSOMTC, SWMG(A)
The Process of Clinical Reasoning in

21
Slide 61JSOMTC, SWMG(A)
Clinical Reasoning
Identify the Problem
Develop a Hypothesis
Test the Hypothesis
Establish a Diagnosis (Dx and DDx)
Develop a Plan
Slide 62JSOMTC, SWMG(A)
Clinical Reasoning
Identify the Problem
Identify abnormal findings
Localize the findings anatomically
Interpret findings in terms of a probable process
Make hypotheses about the nature of the problem
Slide 63JSOMTC, SWMG(A)
Clinical Reasoning
Develop a Hypothesis
Select the most specific and critical findings
• e.g., "sudden pain in my right shoulder while throwing a football".
•match the findings against any conditions that could produce them
• e.g., pain could be caused by a muscle strain, early osteoarthritis, was there trauma involved, prior injuries, over use / repetitive use injury. Asking the right questions will help.

22
Slide 64JSOMTC, SWMG(A)
Clinical Reasoning
Develop a Hypothesis (cont.)
Eliminate the diagnostic possibilities that fail to explain the findings
• e.g., which special tests will identify AC injury, torn labrum or rotator cuff injury? Patient has a positive O'Brian's test, relieved with 2nd test
• weigh competing possibilities
• statistical probability of a given disease by:
age, sex, ethnicity, habits, lifestyle, and locality
Slide 65JSOMTC, SWMG(A)
Clinical Reasoning
Develop a Hypothesis (cont.)
Weigh competing possibilities (cont.)
•initial onset of Injury / illnesse.g., patient had a shoulder injury at age 16. At age 21 while wrestling in college, experienced sudden sharp shoulder pain with a loud popping noise. Pain subsided after several weeks of rest and rehab. (Always, get a good history)
Slide 66JSOMTC, SWMG(A)
Clinical Reasoning
Give special attention to potentially life‐threatening and treatable conditions
minimize the risk of missing the “zebra”
rule of thumb for differential diagnoses
always include “worst case scenario"
Test the Hypothesis
Gather additional information through:
• history
• physical examination
• laboratory results
• radiology

23
Slide 67JSOMTC, SWMG(A)
Clinical Reasoning
Establish a Diagnosis
Use highest level of explicitness and certainty that the data allows
• symptoms may be broad or limited
e.g., “repetitive use injury, cause unknown”
• explicit problems
e.g., “bicipital tendonitis, and torn labrum”
Include multiple differential diagnoses (DDX)
Slide 68JSOMTC, SWMG(A)
Clinical Reasoning
Develop a Plan
Must be logical management from the diagnosis
Specify further necessary steps
• ancillary testing
• consultation
• additions, deletions, or changes to medication
Slide 69JSOMTC, SWMG(A)
Clinical Reasoning
Develop a Plan (cont.)
Note any education that was provided
Remember to consult with the patient to ensure comprehension and compliance
The plan should always be within your scope of practice!

24
Slide 70JSOMTC, SWMG(A)
The Components of Clear and Accurate Records
Slide 71JSOMTC, SWMG(A)
Clear and Accurate Records
Recording your Findings
An important adjunct to patient care
Will evolve with increased knowledge
Organization is essential
• order and readability for future providers
• include all details during the exam
builds your examining skills
extremely time consuming and often compromised due to workload
Slide 72JSOMTC, SWMG(A)
Clear and Accurate Records
Checklist
Is the order clear?
•make the headings clear
• accent your organization with indentations and spacing
• arrange the “present illness” in chronologic order
start with the current episode
then fill in relevant background information

25
Slide 73JSOMTC, SWMG(A)
Clear and Accurate Records
Checklist (cont.)
Does the data included contribute directly to the assessment?
Are pertinent negatives specifically described?
Are there overgeneralizations or omissions of important data?
Is there too much detail?
Are phrases and short words used appropriately and is there unnecessary repetition of data?
Slide 74JSOMTC, SWMG(A)
Clear and Accurate Records
Checklist (cont.)
Is the written style succinct? Are there excessive abbreviations? Are the abbreviations well known or customary for your “clinic?”
Are diagrams and precise measurements included where appropriate?
Is the tone of the write‐up neutral and professional?
Slide 75JSOMTC, SWMG(A)
The SOAP Note

26
Slide 76JSOMTC, SWMG(A)
Slide 77JSOMTC, SWMG(A)
Slide 78JSOMTC, SWMG(A)
SOAP Note

27
Slide 79JSOMTC, SWMG(A)
Questions?
Don't you wish everything in medicine was this obvious?
Slide 80JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of “Overview: Physical Exam and History Taking"
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 81JSOMTC, SWMG(A)
Agenda
Identify the components of a comprehensive physical exam
Identify the Techniques of a Patient interview and Head‐to‐Toe Exam
Identify the basic concepts of evidence‐based medicine and clinical reasoning
Identify the components of a clear and accurate SOAP note

28
Slide 82JSOMTC, SWMG(A)
Reason
As a SOF medic, you may find yourself in austere environments that will limit your medical resources and test your diagnostic capabilities. Your ability to obtain quality patient history, perform a systematic physical exam and come to a correct diagnosis may save your patient's life.
Slide 83JSOMTC, SWMG(A)
Break





























