Embed Size (px)
Citation preview

12/10/2014
1
Slide 1JSOMTC, SWMG(A)
Special Operations Combat MedicPFN: SOMTCL02
Hours: 2.0
Instructor:
Slide 2JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of the Special Operations Combat Medic
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 3JSOMTC, SWMG(A)
Reason
The SOCM must program their reactions and learn from their responses

12/10/2014
2
Slide 4JSOMTC, SWMG(A)
Agenda
Define the Special Operations Combat Medic
Outline SOCM trauma training
Identify Combat Medic variables
Describe environment based thinking
Identify Combat Medic equipment
Identify SOCM packing principles
Determine death and resuscitation termination
Identify SOCM Pearls of Wisdom
Slide 5JSOMTC, SWMG(A)
Special Operations Combat Medic
Slide 6JSOMTC, SWMG(A)
“ Special Operations Combat Medics (SOCMs) may often find themselves in austere tactical environments where evacuation of a teammate to a medical treatment facility may not be possible or may be severely delayed. They must be prepared for any injury within any environment.”
SOCM

12/10/2014
3
Slide 7JSOMTC, SWMG(A)
SOCM Abilities
Capability to treat numerous different types of traumatic wounds
Aptitude to increase team survivability
Comprehension of multisystem trauma patients
Dexterity to operate in all types of environments tactically and medically
Competence to self adjust shortfalls
Slide 8JSOMTC, SWMG(A)
Core Attributes
Integrity
Courage
Perseverance
Personal Responsibility
Professionalism
Adaptability
Team Player
Capability
Slide 9JSOMTC, SWMG(A)
SOCM Trauma Training

12/10/2014
4
Slide 10JSOMTC, SWMG(A)
Trauma 1
ACLS
PEPP
Military Medicine
Lecture / PMST II
Slide 11JSOMTC, SWMG(A)
Trauma 2
Trauma Patient Assessment (TPA)
Trauma Surgical Skills (TSS)
Combat Trauma Management (CTM)
Slide 12JSOMTC, SWMG(A)
Trauma 3
K9 Instruction
Tactical Combat Casualty Care
Military Triage
MASCAL
Advanced Trauma Management (ATM)
Field Training Exercise (FTX)
12/10/2014
5
Slide 13JSOMTC, SWMG(A)
Summation
Each training block is built to add onto the next section
Skills are introduced and reinforced
The medical information will always be changing and the SOCM needs to be informed and integrating the new knowledge
Slide 14JSOMTC, SWMG(A)
Combat Medic Variables
Slide 15JSOMTC, SWMG(A)
Two Types Of Variables
Controllable
Uncontrollable
12/10/2014
6
Slide 16JSOMTC, SWMG(A)
Controllable Variables
What are the variables we can control?
1. Preparation/ Training/ Contingency Plans
2. Mental Capacity/ Composure/ Emotion
3. Education/ Medical Updates
Slide 17JSOMTC, SWMG(A)
Mental Capacity
Developed securely through experience
The ability to filter out what is important in relation to all stimuli
Maturity to distinguish threat from non‐threat medically and tactically
Maturity of reaction
Slide 18JSOMTC, SWMG(A)
Preparation
Preparation entails:
1. Team training
2. Medic training
3. Augmentee training in medical skills
4. Indigenous integration
5. Equipment placement (individual vs. aid bag)
6. PCI checks for mission

12/10/2014
7
Slide 19JSOMTC, SWMG(A)
Training
Medical skills are perishable
Team Medical SOP’s (must be enforced)
Medical training should not be a separate event from other training
Focus on the basics when training teammates (BLS, bandaging and splinting)
Slide 20JSOMTC, SWMG(A)
Numerous Concerns
Slide 21JSOMTC, SWMG(A)
Beyond Medical Concerns
Mini‐gun
Feed mechanism for the Mini‐gun
Load plan for rounds(mini‐gun)
Round box maintenance
Pindle configuration for Mini‐gun
Power Layout
Feed tube immediate action
Trigger operation
Trigger maintenance
M240 operation (butterfly trigger)
M249 operation
M4 operation
M9 operation
DAMA
MERC Chat
MBTIR fill
MBTIR zero
MBTIR operation
Winch operation (GMV)
Compressor
Power converter
AT‐4 safety
AT‐4 operation
Carl Gustav safety
Carl Gustav operation
60mm mortar
Trigger fire operation
Mortar round settings
102 SAT
Team internal chat

12/10/2014
8
Slide 22JSOMTC, SWMG(A)
Preparation is Controllable
There are many, many competing considerations besides medical proficiency and training (weapons maintenance)
As a medical operator, stressing medical training will be a non‐stop job requirement
Training and preparation is a controllable variable that needs to be stressed in terms of the medical component
Slide 23JSOMTC, SWMG(A)
Uncontrolled Variables
Slide 24JSOMTC, SWMG(A)
Uncontrollable Aspects
Weather
Follow‐on missions
Enemy activity
Unavoidable equipment malfunction
Changing environment
Number of casualties
Evacuation response time
12/10/2014
9
Slide 25JSOMTC, SWMG(A)
Variables Continued
Resupply response time
Time of day
Augmentee additions to mission
Force strength (teammates leaving or entering theatre)
Loyalties of Indigenous forces
Slide 26JSOMTC, SWMG(A)
Key points
Categorizing variables helps the operator define the battlefield
“How can I deflate this variable which is uncontrollable?”
Each mission requires a different thought process for the SOCM
The mission may be constant but the execution will change (multi‐use items)
Slide 27JSOMTC, SWMG(A)
Key points Continued
“The operator cannot wait for information to come to them, they must first establish what information they need and then seek it out until they find a required answer”
Developing initiative for preparation will save more lives than any other skill

12/10/2014
10
Slide 28JSOMTC, SWMG(A)
Environment Based Thinking
Slide 29JSOMTC, SWMG(A)
All Actions Depend on Environment
Slide 30JSOMTC, SWMG(A)
Casualty Movement
12/10/2014
11
Slide 31JSOMTC, SWMG(A)
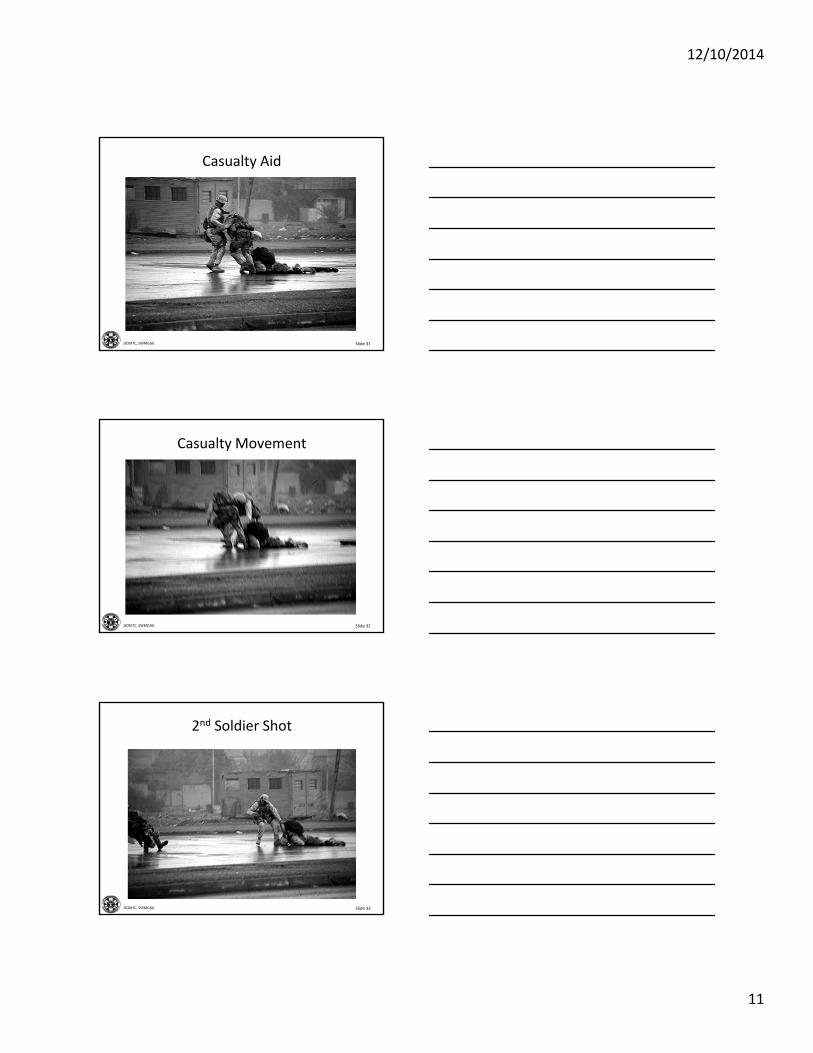
Casualty Aid
Slide 32JSOMTC, SWMG(A)
Casualty Movement
Slide 33JSOMTC, SWMG(A)
2nd Soldier Shot

12/10/2014
12
Slide 34JSOMTC, SWMG(A)
What is the Environment?
Slide 35JSOMTC, SWMG(A)
Review of Reaction
Casualty appears in open area
Rescuer responds by running to casualty (unknown suppressive fire extent)
Casualty weight is overwhelming limiting speed of exit to solid cover
2nd rescuer responds in same manner
One rescuer becomes casualty
Rescuer retreats from open area to regroup
Slide 36JSOMTC, SWMG(A)
Schematic
Road
Road
Wood Building
Enemy fire
Enemy fire
Rescuer direction of travel

12/10/2014
13
Slide 37JSOMTC, SWMG(A)
Environmental Factors
Enemy position unknown or well covered
Large open area, little solid cover
Casualty is unresponsive, no help with extraction
Casualties equipment adds weight
Daylight, full visibility
Distance to solid cover extensive
Slide 38JSOMTC, SWMG(A)
Keys to Rescue/ SOCM Thought Process
Enemy position located (fire superiority)
Location for casualty located (solid cover)
Method of extraction (casualty carry)
Aided rescue tactics (smoke, vehicle cover)
Factors of speed (equipment necessity)
Factors of speed (# of rescuers, pros, cons)
Coordination/ Orchestration (effective fire)
Communication
Slide 39JSOMTC, SWMG(A)
Schematic
Road
Road
Wood Building
Enemy fire
Enemy fire
Rescuer direction of travel
Vehicle
Which way to bring casualty?

12/10/2014
14
Slide 40JSOMTC, SWMG(A)
Tactical Principles
3 F’s of Combat
Find
Fix
Finish
Finding the enemy is easier said than done
Fixing the enemy requires accurate suppression
Finishing may require any number of possibilities
Slide 41JSOMTC, SWMG(A)
Medic Considerations
The thought process and communication requirements for the Medic revolves around the 3 F’s.
Care Under Fire phrase is misleading
Limited medical care should be given to the casualty until SOLID cover is between you and the enemy
SOLID cover will be different for every environment
Slide 42JSOMTC, SWMG(A)
Considerations Continued
SOLID cover examples

12/10/2014
15
Slide 43JSOMTC, SWMG(A)
Environment Scenario
Slide 44JSOMTC, SWMG(A)
Suicide Bomber
Your clinic has been targeted by suicide bombers
As the only medic involved in the clinic you need to make the clinic safe due to this threat
Slide 45JSOMTC, SWMG(A)
Schematic
Two way road
10 meter mud wall
Door Entrance
Female Clinic
Male Clinic
Door Entrances
50 meter distance
Suicide Bomber Threat is imminent from cross checked intelligence reports and HUMINT resources.
SafeArea to the West

12/10/2014
16
Slide 46JSOMTC, SWMG(A)
Resources available 2inX4inX8ft wood planks (unlimited)
Nails unlimited
5 Camp workers with necessary tools (shovels, hammers, etc)
1 loader
3ftX3ft Hesco containers
(unlimited amount)
30 man Afghan Infantry Co
All the mud you want
Slide 47JSOMTC, SWMG(A)
Exercise
With the schematic and the resources given you must make the clinic safe for your patients, the host nation doctors working for you, your teammates, and any other guests which may visit the clinic at any time
You now have 10 minutes to think about and draw out a strategy for safety
Questions?
Slide 48JSOMTC, SWMG(A)
Schematic Review
Two way road
10 meter mud wall
Door Entrance
Female Clinic
Male Clinic
Door Entrances
50 meter distance
Suicide Bomber Threat is imminent from cross checked intelligence reports and HUMINT resources.
SafeArea to the West
12/10/2014
17
Slide 49JSOMTC, SWMG(A)
Answer Considerations
The Threat: suicide bomber
Characteristics : On foot?
More than one individual?
Armed with one bomb, weapon and bomb, just grenades, RPG’s
Male, female, child?
Channelize threat
Increase time to react
Address cultural concerns
Use Host Nation Soldiers whenever possible
Slide 50JSOMTC, SWMG(A)
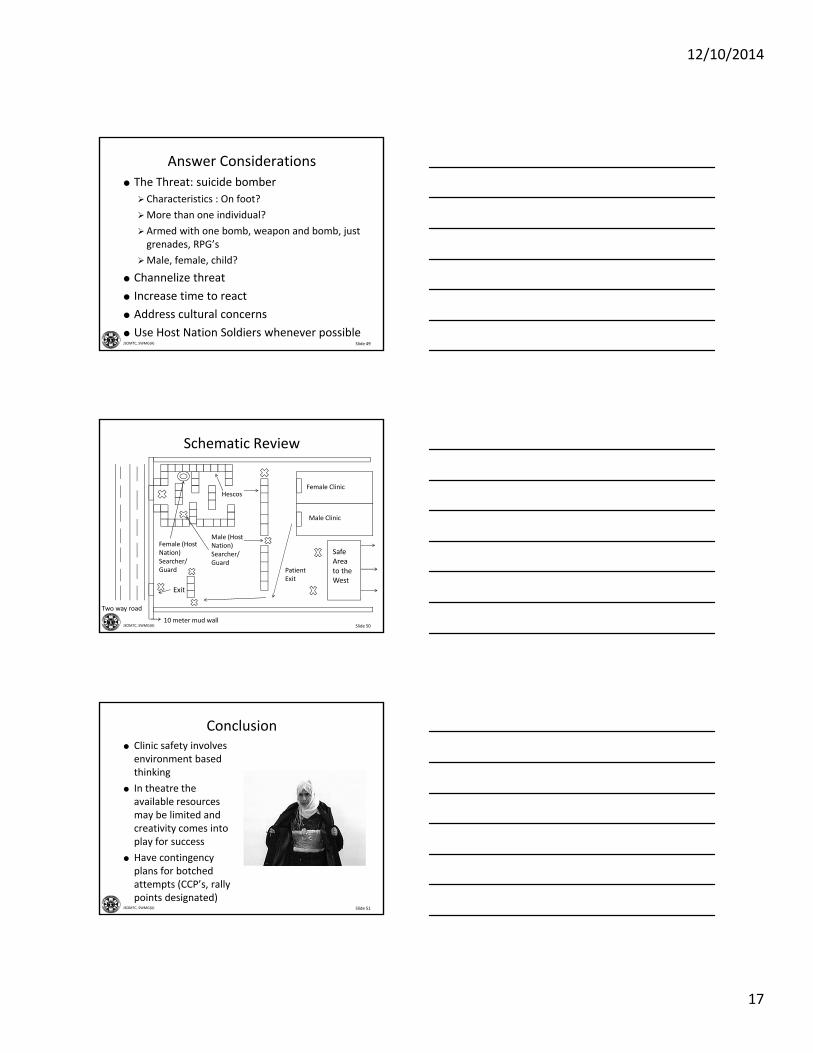
Schematic Review
Two way road
10 meter mud wall
Female Clinic
Male Clinic
SafeArea to the West
Hescos
Female (Host Nation) Searcher/ Guard
Male (Host Nation) Searcher/Guard
Exit
PatientExit
Slide 51JSOMTC, SWMG(A)
Conclusion Clinic safety involves environment based thinking
In theatre the available resources may be limited and creativity comes into play for success
Have contingency plans for botched attempts (CCP’s, rally points designated)

12/10/2014
18
Slide 52JSOMTC, SWMG(A)
Key Operational Points
If Hescos are scarce, digging trenches for VBIED protection is an alternative (remember channelization)
Static site security is executed in layers
Outer layer is made up of host nation
Inner layermay be U.S. regular army or more host nation Team layer for all
team members
Slide 53JSOMTC, SWMG(A)
Changing Environments
Slide 54JSOMTC, SWMG(A)
Firebase Clinic
Medicine in this environment requires a different approach than the situation we just critiqued

12/10/2014
19
Slide 55JSOMTC, SWMG(A)
Rural Vehicle Combat
* Courtesy SFC Elwood (1SFG)
Slide 56JSOMTC, SWMG(A)
Urban Foot Combat
Slide 57JSOMTC, SWMG(A)
7000 Feet Logar Province, Afghanistan

12/10/2014
20
Slide 58JSOMTC, SWMG(A)
Jungle Combat
Slide 59JSOMTC, SWMG(A)
Operating in Rotary Wing Aircraft
Slide 60JSOMTC, SWMG(A)
Darkness Considerations

12/10/2014
21
Slide 61JSOMTC, SWMG(A)
Combat Medic Equipment
Slide 62JSOMTC, SWMG(A)
Soldier Load
Soldier load given the terrain
Mobility requirements given combat action
Mission dependent variables for equipment considerations
Slide 63JSOMTC, SWMG(A)
Soldier Kit Issues
Very bulky on the anterior
The posterior camelback makes movement difficult
The prone shooting position is almost impossible

12/10/2014
22
Slide 64JSOMTC, SWMG(A)
Principles for Equipment Selection
Mission specific (don’t forget contingencies)
Multi‐use items
Contents should be mission tested
Packaging should be water resistant/durable
Equipment should be team‐member specific in certain cases
Chosen articles need to address possible injuries seen at each level of the mission
Slide 65JSOMTC, SWMG(A)
Mission Dependent/ Operator Dependent Medical Gear Matrix
Designated by GradesIFAK/Blowout Kit AID BAG EVAC Ground/ AIR FireBase/FAST/CASHGrade 1 MED gear Grade 2 MED gear Grade 3 MED gear Grade 4 MED Gear
NPA Cric kit Extra fluids UltrasoundTourniquet IV (2) IV supplies ECG/MonitorsChest Seal Drugs Israeli Litter VentilatorACE Wrap Airway Kit Blankets/Hypothermia kit OxygenKerlex Chest Tube Kit Thermal Angel Field Blood Supply
14ga (ND) Kerlex/Ace Wrap Traction Devices Extra/Additional DrugsAlcohol/Betadine Sam Splint C‐collar Foley/NG
CravatsExtra‐Bandages/ Ace
wraps SuctionABD dressing Tourniquets PleurovacTourniquets Skedco
BVM with maskStethescopeHemostats
Bandage ScissorsOPA
Slide 66JSOMTC, SWMG(A)
Grade I
Operator equipment is stream line
IFAK worn on left side‐rear
Pros and Cons for IFAK position
Mobility needs to be considered when placing Grade I gear

12/10/2014
23
Slide 67JSOMTC, SWMG(A)
Grade II
M9 Medic Bag
Low profile
Used mainly for assaults or short term missions
May be used for long range patrol; weight and equipment decisions become potential issues
Slide 68JSOMTC, SWMG(A)
Grade II Continued
Larger medical bag
Used for vehicle operations
May be used as “drop and go bag” when assaulting
Medical bag for range operations
More room more possibilities
Slide 69JSOMTC, SWMG(A)
Grade III
GMV, ATV, or any alternate place where follow on medical gear may be stored for use on the battlefield
This Grade is open to places of experience or creativity of the operator and the team
12/10/2014
24
Slide 70JSOMTC, SWMG(A)
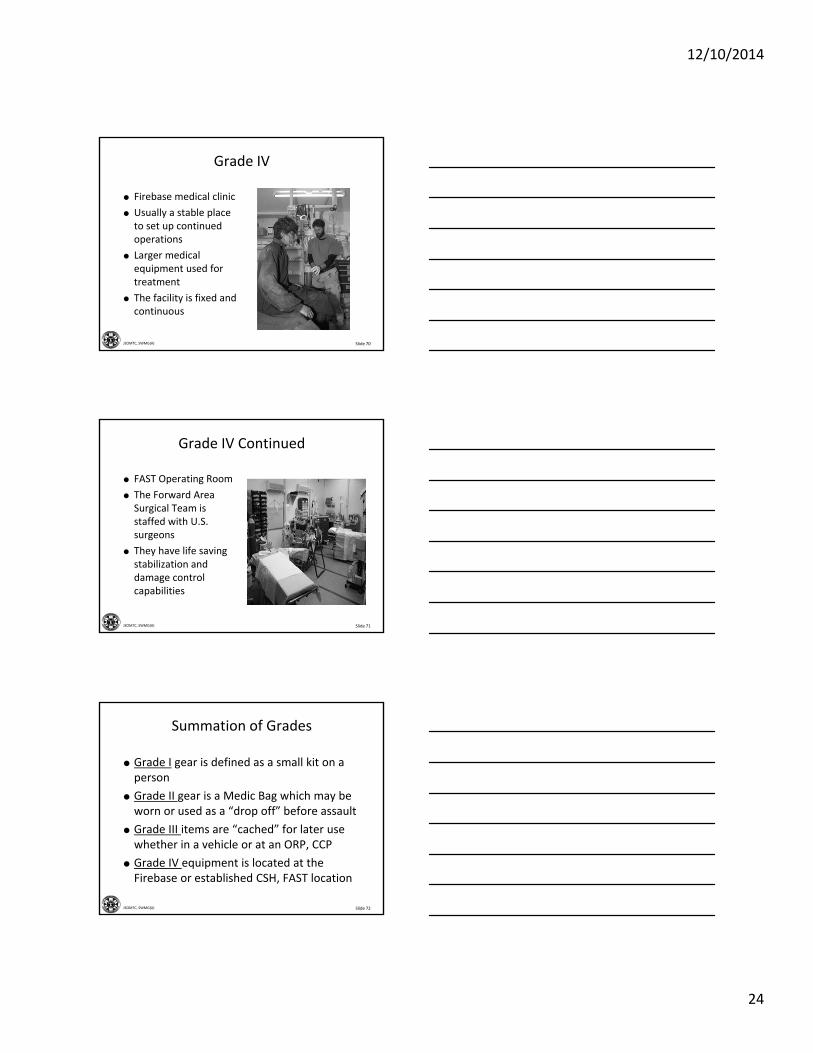
Grade IV
Firebase medical clinic
Usually a stable place to set up continued operations
Larger medical equipment used for treatment
The facility is fixed and continuous
Slide 71JSOMTC, SWMG(A)
Grade IV Continued
FAST Operating Room
The Forward Area Surgical Team is staffed with U.S. surgeons
They have life saving stabilization and damage control capabilities
Slide 72JSOMTC, SWMG(A)
Summation of Grades
Grade I gear is defined as a small kit on a person
Grade II gear is a Medic Bag which may be worn or used as a “drop off” before assault
Grade III items are “cached” for later use whether in a vehicle or at an ORP, CCP
Grade IV equipment is located at the Firebase or established CSH, FAST location

12/10/2014
25
Slide 73JSOMTC, SWMG(A)
SOCM Packing Principles
Slide 74JSOMTC, SWMG(A)
Packing Gear Principles
Waterproof and preferably CBRNE proof
Compact
Easy to locate within the bag
Contents ordered in terms of use
Slide 75JSOMTC, SWMG(A)
Gear Principles Continued
Extra items available
Sterility kept with products
Kits made for procedures
Items are tested and familiar to operator

12/10/2014
26
Slide 76JSOMTC, SWMG(A)
Waterproof Contents
Slide 77JSOMTC, SWMG(A)
Vacuum Sealing Pros
Excess air is evacuated decreasing size of medical components or kits
All contents are sealed and dry
Gives the operator the ability to package kits for a team member to carry
Gives the Medic freedom to include what contents are deemed personally necessary
Slide 78JSOMTC, SWMG(A)
Vacuum Sealing Cons
Time consuming
Resource intensive (vacuum sealer and vacuum bags)
May not have the ability to perform in austere conditions
Some products don’t seal well

12/10/2014
27
Slide 79JSOMTC, SWMG(A)
Compact
Cricothyroidotomy Kit Repackaged 6” Ace
Slide 80JSOMTC, SWMG(A)
Easy to Locate Inside Medic Bag
Slide 81JSOMTC, SWMG(A)
Contents Ordered in Terms of Use
Tape on tape
Trash stays with cravat
Contents may be placed in order of use

12/10/2014
28
Slide 82JSOMTC, SWMG(A)
Retrieving Contents
Slide 83JSOMTC, SWMG(A)
Extra Items Available
Slide 84JSOMTC, SWMG(A)
Sterility Kept with Products
* Courtesy Mr. Resurreccion
12/10/2014
29
Slide 85JSOMTC, SWMG(A)
Drug Box Design
Slide 86JSOMTC, SWMG(A)
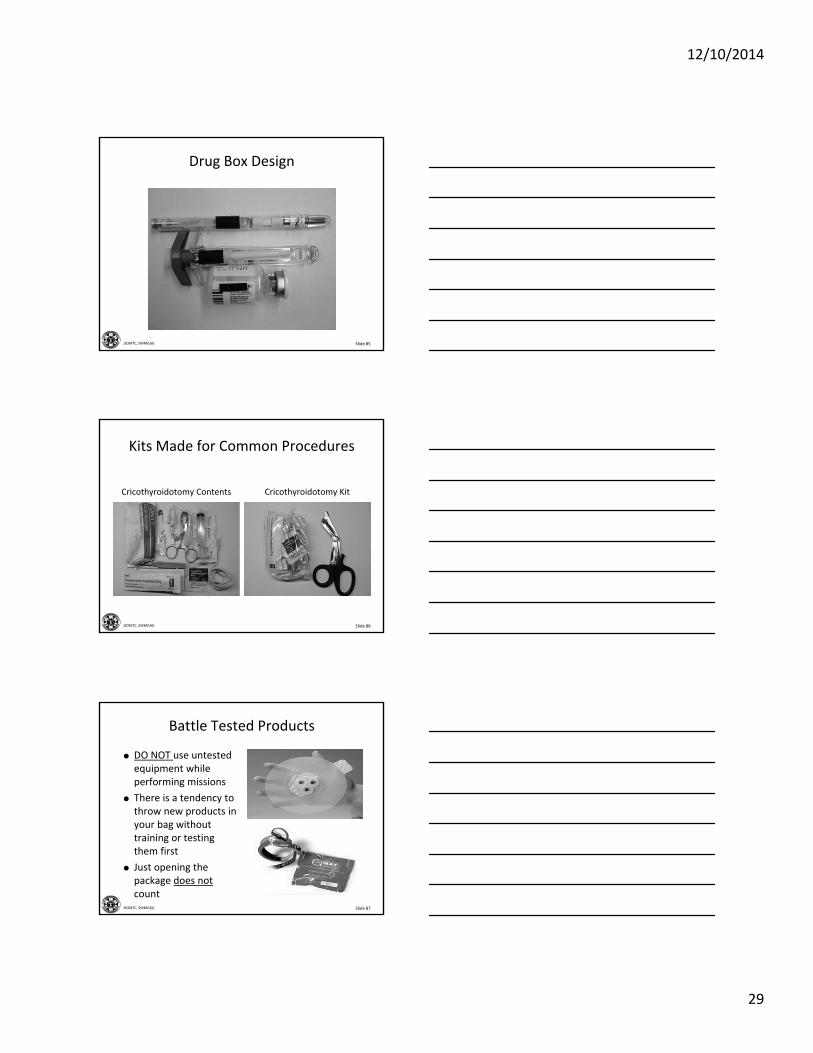
Kits Made for Common Procedures
Cricothyroidotomy Contents Cricothyroidotomy Kit
Slide 87JSOMTC, SWMG(A)
Battle Tested Products
DO NOT use untested equipment while performing missions
There is a tendency to throw new products in your bag without training or testing them first
Just opening the package does not count

12/10/2014
30
Slide 88JSOMTC, SWMG(A)
Discussion
This is the modified ET tube for the Cricothyroidotomy Kit
Why is there a STYLETplaced inside the tube?
* RAISE your hand with the answer
Slide 89JSOMTC, SWMG(A)
Answer
The stylet is used only to keep the tube open while it is stored inside the kit
Without the stylet the tube will be flattened and during use may be altered, decreasing the flow of air through the tube
Slide 90JSOMTC, SWMG(A)
Determine Death and Resuscitation Termination
12/10/2014
31
Slide 91JSOMTC, SWMG(A)
Determine Death and Resuscitation Termination
Obvious death
Decapitation
Massive crush injury and or penetrating trauma with evisceration of heart, lung or brain
Incineration
Decomposition of body tissues
Rigor Mortis or post mortem lividity
Slide 92JSOMTC, SWMG(A)
Determine Death and Resuscitation Termination
Termination of resuscitation efforts
After 15 minutes if MOI is unknown or due to trauma, PLUS
After 30 minutes if MOI is hypothermia, lightning strike, electrical injury, cold water drowning PLUS
Persistent absent pulse and respirations when adequate ventilation, fluids and medications have been administered
Slide 93JSOMTC, SWMG(A)
Determine Death and Resuscitation Termination
Termination of resuscitation efforts
Persistent absent pulse and respirations
Pupils are fixed and dilated
No deep pain response
Absence of end tidal CO2 from a correctly placed ET tube or alternate airway device

12/10/2014
32
Slide 94JSOMTC, SWMG(A)
SOCM Pearls of Wisdom
Slide 95JSOMTC, SWMG(A)
Tourniquet Requirements
Operators coming home have stated the need for 3 tourniquets on each Soldier
The need for 2 tourniquets on some leg wounds has driven the change
Remember in harsh environments check tourniquet serviceability regularly
Slide 96JSOMTC, SWMG(A)
Products Seen Downrange
Combat Gauze
S‐Rolled Kerlex
Saline Lock Kit
Altered Cric Tube
Altered Scalpel for Cric

12/10/2014
33
Slide 97JSOMTC, SWMG(A)
Tourniquet Placement
Tourniquets may be placed anywhere for easy access
Inside this GMV there are numerous tourniquets accessible at any time
They were secured to many different non‐removable features of the GMV by electrical tape
The idea used was for breakaway capability of use
Slide 98JSOMTC, SWMG(A)
Low Visibility Operations
Low Visibility Operations create issues for medical requirements
Prior planning and medical kit component choices are the keys
What do you bring for this mission?
Slide 99JSOMTC, SWMG(A)
Firebase Clinic Safety
Patients screened prior to entrance to clinic (Indigenous then U.S.)
Holding area established
No vehicles allowed to deliver patients to clinic (VBIED concerns)
12/10/2014
34
Slide 100JSOMTC, SWMG(A)
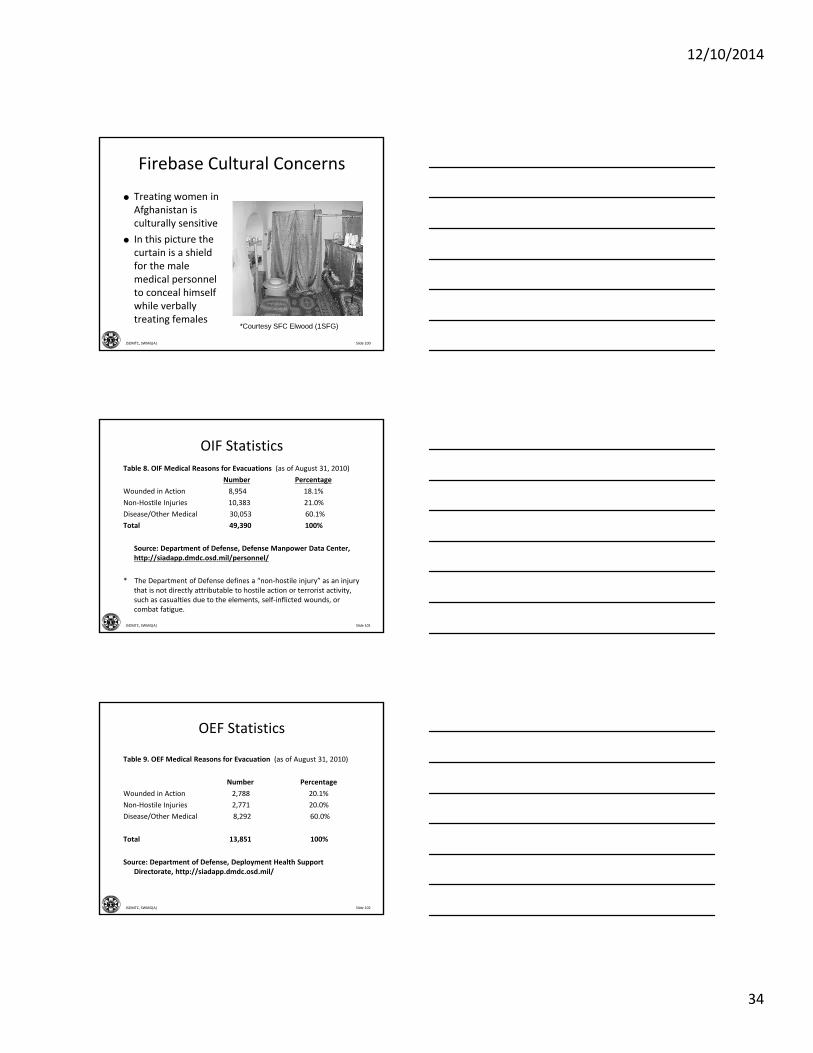
Firebase Cultural Concerns
Treating women in Afghanistan is culturally sensitive
In this picture the curtain is a shield for the male medical personnel to conceal himself while verbally treating females
*Courtesy SFC Elwood (1SFG)
Slide 101JSOMTC, SWMG(A)
Table 8. OIF Medical Reasons for Evacuations (as of August 31, 2010)
Number Percentage
Wounded in Action 8,954 18.1%
Non‐Hostile Injuries 10,383 21.0%
Disease/Other Medical 30,053 60.1%
Total 49,390 100%
Source: Department of Defense, Defense Manpower Data Center, http://siadapp.dmdc.osd.mil/personnel/
* The Department of Defense defines a “non‐hostile injury” as an injury that is not directly attributable to hostile action or terrorist activity, such as casualties due to the elements, self‐inflicted wounds, or combat fatigue.
OIF Statistics
Slide 102JSOMTC, SWMG(A)
OEF Statistics
Table 9. OEF Medical Reasons for Evacuation (as of August 31, 2010)
Number Percentage
Wounded in Action 2,788 20.1%
Non‐Hostile Injuries 2,771 20.0%
Disease/Other Medical 8,292 60.0%
Total 13,851 100%
Source: Department of Defense, Deployment Health Support Directorate, http://siadapp.dmdc.osd.mil/

12/10/2014
35
Slide 103JSOMTC, SWMG(A)
Statistical Meaning for the SOCM
81.1% of Injuries were non‐action issues (OIF)
80% of Injuries were non‐action issues (OEF)
Wounded in Action results in approximately 20% of the injuries seen
That 20% will be the most serious injuries the SOCM will see while deployed
Do not become complacent with preparation and skills given the make‐up of injuries
Slide 104JSOMTC, SWMG(A)
Amputations for OIF,OEF, EtcTable 3. Count of Individuals with Amputations by Service for OIF, OEF, and Unaffiliated Conflicts, 2001 to
September 1, 2010
Theater Type of Amputation Army Marine Navy Air Force Foreign Other Total
OIF Major Limb 620 158 18 8 4 8 816
Partial(Hand/Foot,Toes/Fingers) 272 49 7 11 0 3 342
OEF Major Limb 145 53 5 6 4 4 217
Partial(Hand/Foot,Toes/Fingers) 24 6 0 2 0 0 32
Unaffiliated Major Limb 94 12 25 31 1 26 189
Conflicts Partial(Hand/Foot,Toes/Fingers) 20 1 2 1 0 1 25
Total 1,621
Source: Personal correspondence with Dr. Michael J. Carino, Army Office of the Surgeon General, September 21, 2010.
Slide 105JSOMTC, SWMG(A)
TBI Incidence
Table 2. Traumatic Brain Injuries in the U.S. Military (2000 to 2010 Q1)
Year 2003 2004 2005 2006 2007 2008 2009 2010 Total
Incident 12,886 13,271 12,025 16,873 23,002 28,557 27,862 7,604 178,876
Source: The Defense and Veterans Brain Injury Center, http://www.dvbic.org/TBI‐Numbers.aspx, last updated on May 20, 2010.

12/10/2014
36
Slide 106JSOMTC, SWMG(A)
Lessons
Be aware and prepared for the TBI patient
Have systems in place to deal with TBI suspected casualties
Extremity injury is very common
Focus on courses of action for extremity trauma (teach your teammates)
Slide 107JSOMTC, SWMG(A)
Discussion
You are the Senior medic without a Junior medic tasked with a vehicle mounted direct hit on a small collection of buildings 20km East of Bagram, Afghanistan. Provide a medical load out plan for all 9 personnel and the 3 GMV’s in your team. All answers will be written. All materials will be collected with your name attached.
Slide 108JSOMTC, SWMG(A)
Your Target Landscape

12/10/2014
37
Slide 109JSOMTC, SWMG(A)
Carrying Load for Personnel
NPA (1)
Tourniquet X 3
Cric Kit
2 inch Ace with 1 Kerlex
1 pack Combat Gauze
Needle Decompression Kit (2:14ga Needles)
2 Asherman chest seals
Slide 110JSOMTC, SWMG(A)
Possible Outload Plan
Driver
TC
Gunner
Large MED Bag
Marks the
position of break away tourniquets attached to the vehicle. The front 2 are attached to the sun visors and the rear 2 to the frame cross bar.
Slide 111JSOMTC, SWMG(A)
GMV Med Bag Contents
Tourniquet (4)
Compressed Kerlex (8)
6in Ace Wraps (8)
Abdominal Bandage w/cravat (2)
Chest tube Kit (1)
IV kits with 500ml Hextend (2)
FAST 1 IO (1)
SAM Splints (3)
Cravats (8)
Sodium Chloride 100ml (2)
Airway Kit with Laryngoscope (1)
Field Dressings (5)
Cricothyroidotomy kit (1)
Hypothermia Kit (1)
Nine Line Casevac Card (2)
BVM w/mask
KTD Traction device (1)
Combat Gauze (2)
Penlight (2)
Stethescope (1)
BP cuff (1)
C‐Collar (1)
Trauma Shears (1)
Sharpies pens (3)
Head lamp (1) Extra Batteries
Drugs: Invanz (3 vials)
Moxifloxacin (2 vials)
Fentanyl Lollipops
Morphine (3 Vials)
Snivel Drugs
Indigenous Drugs
Any Extra contents

12/10/2014
38
Slide 112JSOMTC, SWMG(A)
Contingencies
The mission starts as vehicle mounted, remember concerns for dismounted operations
Your proposed CASEVAC time is just proposed and will probably be longer
Mass casualty events are always a concern
Pre‐hit and Post‐hit travel
Nail down CASEVAC plan with the pilots if possible
Slide 113JSOMTC, SWMG(A)
Questions?
Slide 114JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of the Special Operations Combat Medic
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
12/10/2014
39
Slide 115JSOMTC, SWMG(A)
Agenda
Define the Special Operations Combat Medic
Outline SOCM trauma training
Identify Combat Medic variables
Describe environment based thinking
Identify Combat Medic equipment
Identify SOCM packing principles
Determine death and resuscitation termination
Identify SOCM Pearls of Wisdom
Slide 116JSOMTC, SWMG(A)
Reason





























