-
Simulation of Pulmonary Pathophysiology During
SpontaneousBreathing
Y. C. Zhao, S. E. Rees, S. Kjrgaard, S. Andreassen
Center for Model-based Medical Decision Support, Alborg
University, DenmarkDepartment of Anaesthesiology, Alborg Hospital,
Denmark
Abstract This paper presents a functional model of lungmechanics
including a non-linear alveolar pressure volumecurve and
representation of the work of respiratory musclesduring breathing.
The model is used to simulate the responseto forced inspiration and
expiration, and these simulationscompared to the standard results
of lung function tests routinelyperformed in departments of lung
medicine. The model cansimulate the characteristics of inspiratory
and expiratory flowprofiles seen in normal subjects, and in
patients with obstructiveor restrictive diseases.
I. INTRODUCTIONIn clinical practice linear models of respiratory
mechanics
can be used to estimate resistance and elastance parametersof
the respiratory system. These may provide an under-standing of the
pathogenesis of lung disease, and may beused to optimize ventilator
settings or adjust pharmacologicaltherapy. Whilst the parameters of
these linear models canbe estimated in the clinical settings, the
complexity of themodels is insufficient, meaning that these models
oftenprovide a poor fit to measurements of flow and pressure,
andgive parameter values which are physiologically implausible[1].
To overcome these limitations, models have been builtusing the so
called functional approach [2][3][4][5][6]. Thesemodels divide the
airways into three sections: upper airwaysdescribed as a flow
dependent resistance; central airwaysdescribed as a transmural
pressure dependent resistance; andlower airways described as a
volume dependent resistance. Inthis approach, alveoli are lumped
into single a compartmentwith a constant compliance. Models built
using the functionalapproach have been used to simulate flows and
pressuresduring mechanical ventilation. However, these models
havenot been used to simulate spontaneous ventilation. In
par-ticular they have not been used to simulate the flow andvolume
profile that occurs during forced breathing, wherethese profiles
are often used in the diagnosis of respiratorydisease.
This paper presents a modified version of the modelpreviously
proposed by Barbini et al [6]. This model includesa sigmoid [7]
function to represent the nonlinear properties ofboth airways and
the alveoli space, and a pressure generatorto describe the work of
the respiratory muscles. In doing so,it will be tested whether this
model can simulate spontaneousbreathing, including forced breathing
patterns in normalsubjects and patients with lung diseases.
This work was supported by the IT committee under the Danish
TechnicalResearch Council.
II. MODEL OF RESPIRATORY MECHANICSMechanical and electrical
analogues of respiratory me-
chanics are illustrated in figure 1. The derivation of
amathematical description of these models and its
detailedphysiological interpretation follows.
A. Alveoli and Thoracic CageFigure 1(a) illustrates the
physiology included in the
model. Alveoli are surrounded the pleural space which
isconnected with the thoracic cage. The pressure inside thealveoli
and pleural space are called alveolar gas pressure (Pa)and the
pleural pressure (Ppl) respectively. During breathingthe work
performed by the muscles of the chest wall anddiaphragm generate
pressure (Pm) in the pleural space,whilst chest wall elasticity
(Ecw) exerts recoiling pressure(Pcw) against it. Ppl is therefore
given by
Ppl = Pm + Pcw (1)The elastic recoil pressure of the chest wall
is consideredhaving a linear relationship with the thoracic cage
volume(Vtc) and describes as
Pcw = EcwVtc Pcw0 (2)where Pcw0 is a parameter representing the
outward pullingpressure generated by chest wall at the relaxed
state, atwhich the opposite pull of the alveoli and the chest
wallreaches the equilibrium. Vtc is approximated equal to thesum of
alveolar volume (Va) and central airway volume (Vc),assuming
negligible pleural volume, i.e.
Vtc = Va + Vc (3)The pressure difference between Ppl and body
surface
pressure (Pbs) is termed as trans-chestwall pressure (Ptc),which
drives Vtc and is described as
Ptc = Ppl Pbs (4)The pressure difference between the alveoli and
the pleural
space is called transpulmonary pressure (Ptp), which drivesVa
change in a nonlinear relationship [8][9][10], and isdescribed
as
Ptp = Pa Ppl (5)In this paper, the relationship between Ptp and
Va is repre-sented by a sigmoid equation (6) proposed by Venegas et
al[7]
Va = a + [b/
(1 + e(d/(Ptpc)))] (6)
Proceedings of the 2005 IEEEEngineering in Medicine and Biology
27th Annual ConferenceShanghai, China, September 1-4, 2005
0-7803-8740-6/05/$20.00 2005 IEEE. 6128
-
Thoracic Cage (Vtc)
Alveoli
Va
RcRlRu
PaPmPcw
Pv
av
Pbs
Ppl
Pc Vc
Chest Wall
Diaphragm
Ptp
Ptc
Ptm
Ecwc
v
Pleural Space
u c l
(a)
Ru Rl
Va
Pc
PPl
v PaRc
+
-
Pm Pcw
Vtc Ecw
Vc
av
cv
Ptm PtpP
Pbs
1 2
+
+-
-
+
-
(b)
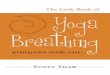
Fig. 1. (a) A mechanical analogue representing physiological
interpretation of respiratory mechanics. Airways are lumped into
three sections, i.e. upper(u), central (c), and lower airways (l).
The thoracic cage is represented as a solid and dashed line, which
indicates its compression due to pressure appliedby the chest wall
and muscle work. (b) Respiratory mechanics is modeled and
calculated in an electric analogue. Body surface pressure is
referred asground in circuit analysis. The direction of inflation
flow v is assumed as the positive direction.
where a corresponds to the lower asymptote of the lungvolume; b
corresponds to the difference between the upperand the lower
asymptote of the lung volume; c is the pressureat the inflection
point between the upper and the lowerasymptote of the sigmoid
curve; d indicates a pressure range,in which the most constant
compliance occurs, i.e. the range(c 2d) to (c + 2d).B. Airways
The respiratory airways are divided into three sections,upper,
central and lower airways, according to their func-tional
importance. Upper airways are assumed to consist ofairways from
mouth to extrathoracic trachea; Central airwaysare assumed from
intrathoracic trachea to small bronchi(11th generation of Weibel
model [11]); Lower airways areassumed to consist of bronchioles
extending to the alveoli,i.e. generations (12th-23th) [11].
a) Upper Airways: Upper airways are represented asrigid pipes
with considerable structural resistance to collapse,and can be
modeled as flow dependent resistance (Ru)according to Rohrer
[12]
Ru = k1 + k2 |v| (7)where k1 represents resistance due to
laminar flow, and k2represents resistance due to turbulent
flow.
b) Central Airways: Central airways can be com-pressed and
correspondingly cause expiratory flow limitation(EFL) during forced
expirations or during normal ventila-tion in patients with chronic
obstructive pulmonary disease(COPD) [13]. Modeling this compression
is therefore neces-sary to represent EFL. Compression due to high
transmuralpressure (Ptm) can be represented as the difference
betweenintraluminal pressure (Pc) and pleural pressure (Ppl)
Ptm = Pc Ppl (8)Golden et al [3] modeled resistance due to
collapsibleairways as a compressible cylinder with a fixed
lengthand variable volume Vc, whose resistance Rc is
assumedproportional to 1/V 2c , and represented as
Rc = k3
(Vcmax
Vc
)2(9)
where Vcmax stands for the maximal volume of collapsibleairways
when the airways are fully distended. Under fullydistended
conditions, k3 represent a small viscose airwayresistance.
Previously the relationship between Vc and Ptm has beenmodeled
as a nonlinear sigmoid function [6], the slope ofwhich is the
airway compliance.
Ptm = a b ln
(Vcmax
Vc 1
)(10)
where a stands for the point of the maximal airway com-pliance;
b is the parameter standing for a range in whichthe most constant
airway compliance occurs, i.e. the range(a 2b) to (a + 2b).
c) Lower Airways: Lower airways have no rigid struc-ture and are
embedded in the lung parenchyma. Due totraction arising from
parenchyma on the airway walls the air-ways dilate with lung volume
expansion [14], and thereforeminimize the airway resistance. The
lower airway resistance(Rl) is inversely proportional to alveolar
volume (Va) [15],thereby giving
Rl =k4Va
(11)where k4 is a model parameter describing different
patho-physiological states of the lower airways.
C. Model DynamicsTo describe the dynamics of the respiratory
system re-
quires representation of the volumes of lung compartmentsand
dynamics of gas flow between these. State variables areselected
describing the volume of gas in each compartment(Va1, Vc, Vtc), and
differential equations formulated as:
dVadt
= va (12)dVtcdt
= v (13)dVcdt
= vc (14)va describes the net air flow into the alveoli, which
can becalculated from the pressure drop over the lower airways
1where lower airway volume is lumped into the alveolar
compartment
6129
-
(Pc Pa) divided by the lower airway resistance (Rl)
asillustrated in figure 1(b), i.e.
va =Pc Pa
Rl(15)
v describes airflow into the respiratory system, which can
becalculated from pressure gradient over the upper and
centralairways (P Pc) divided by the sum of airway resistancein the
upper (Ru) and central (Rc) airways as illustrated infigure 1(b),
i.e.
v =P PcRu + Rc
(16)
vc describes flow bypass due to collapsible airways, whichcan be
calculated from the flow entering the respiratorysystem minus the
flow entering the alveolar compartment(v va) as illustrated in
figure 1(b), i.e.
vc = v va (17)III. MODEL SIMULATIONS
This model includes seventeen equations with three dif-ferential
equations (12-14) describing changes in state vari-ables (Va, Vtc,
Vc), three equations describing flows betweencompartments (15-17)
and the remaining (1-11) describingthe relationship between
pressures, volumes and resistances.All equations can be solved to
simulate a dynamic responseof the respiratory system to changes in
ventilation, andthe resultant steady state, given values of model
parame-ters {k1, k2, k3, a, b, Vcmax, k4, a, b, c, d, Ecw}, initial
con-ditions of state variables (Va(0), Vtc(0), Vc(0)), and
modelinputs (Pm, P , v). For spontaneous respiration
inspiratoryflow (v) is not required as an input to the model, and
thepressure at mouth P equals the body surface pressure Pbs.
The model is used here to simulate forced inspiration
andexpiration in three cases: normal patients, obstructive
lungdisease (OLD) and restrictive lung disease (RLD). OLD
ischaracterized by an increase in airway resistance, because
ofthickening, partial blockage and narrowing of the airways,as is
commonly seen in COPD. RLD is characterized by areduction on vital
capacity (VC), because of alternations inthe lung parenchyma,
disease of the pleura or the chest wall,or neuromuscular
apparatus.
To perform these simulations, initial values of state vari-ables
are set as in Table I according to reported values offunctional
residual capacity (FRC) in normal, obstructive andrestrictive lung
disease [16]. Values of model parameters arefixed to represent the
three conditions (Table II). OLD isassumed to be an isolated airway
disease, so that modelparameters of the alveolar space are assumed
to be normal.RLD is assumed to be an isolated alveolar disease, so
that themodel parameters of the airways are assumed to be
normal.Values of k1, k2, k3, a, b, Vcmax, k4 for airway model
pa-rameters are taken from the reference [6]. Values of a, b, c,
dfor normal subjects and OLD patients are set or estimatedfrom
textbook values [16] using an average elastance ofalveolar space,
i.e. 5 cmH2O/L [16]. For patients with RLDthese values are obtained
from the work of Pereira et al [17].
Chest wall elastance (Ecw) is assumed to be normal in allcases,
i.e. 5 cmH2O/L [16].
TABLE IINITIAL VALUES FOR STATE VARIABLES.
Va(0)(L) Vtc(0)(L) Vc(0)(L)Normal 3.0000 3.0748 0.0748OLD 3.5000
3.5689 0.0689RLD 1.5000 1.5735 0.0735
For each case (normal, OLD, and RLD) the model is usedto
simulate flow and volume curves during forced respiration.Four
simulations are performed for each case, inspiratorymuscle pressure
is fixed at -25 cmH2O and expiratory musclepressure is set to 0,
30, 40, and 50 cmH2O, respectively. Toverify the model, these
simulations can be compared to theresults of standard lung function
tests.
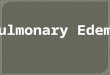
Figure 2 illustrates model simulated flow volume curvesduring
forced inspiration and expiration. Forced inspirationstarts at the
FRC (point A), and ends at total lung capacity(TLC) (point B).
Relaxed expiration returns to point A, andforced expiration ends at
the RC (point C). The volumebetween point B and C is the forced
vital capacity (FVC),and the forced expired volume in the first
second is labeledFEV1. In clinical practice, two measurements are
often usedto characterize obstructive and restrictive lung disease.
Theseare a relative FEV1 (FEV1,r) calculated as FEV1 divided byFVC;
and a relative FVC (FVCr) calculated as FVC dividedby the normal
value of FVC. Model simulated values ofFEV1,r and FVCr are given in
table III. The value of FVCin normal conditions used in calculating
FVCr is assumed tobe that obtained from model simulation of forced
expirationin normal subject with expiratory muscle pressure (Pm)
equalto 50 cmH2O.
TABLE IIIRELATIVE FEV1 AND FVC AS FRACTION OF NORMAL
Pm = 30cmH2O Pm = 40cmH2O Pm = 50cmH2OFEV1,r FVCr FEV1,r FVCr
FEV1,r FVCr
Normal 0.82 0.98 0.83 0.99 0.84 1.00OLD 0.35 0.79 0.35 0.80 0.35
0.81RLD 0.96 0.48 0.96 0.48 0.97 0.48
Figure 2(a) illustrates a flow-volume curve of forcedventilation
in a normal subject. The maximal expiratory flow(MEF) is about 8
L/s, and is only achieved during forcedexpiration. The peak
expiratory flow obtained in each forcedexpiration varies only
slightly when increasing expiratoryeffort, i.e. when increasing Pm
from 30 to 50 cmH2O, astandard result of lung function tests on
normal subjects.The values of FEV1,r (Table III), 0.82-0.84, for
the normalsubject are consistent with reported values [16]. Figure
2(b)illustrates forced ventilation in a patient with OLD. The
sim-ulated value of MEF is about 1.8 L/s, substantially lower
thannormal. MEF is almost achieved during passive expiration(Pm =
0) simulating flow limitation in relaxed expiration,a simulation
which is consistent with clinical findings insevere COPD patients
[13]. The calculated value of FEV1,r
6130
-
TABLE IIMODEL PARAMETER VALUES FOR NORMAL, OLD AND RLD.
k1 k2 k3 a b Vcmax k4 a b c d Ecw
cmH2O s/L cmH2O s2/L2 cmH2O s/L cmH2O cmH2O L cmH2O s L L cmH2O
cmH2O cmH2O/L
Normal 0.5 0.2 0.2 0.35 2.0 0.1 9.5 1.3 5.2 8.0 4.0 5.0OLD 0.5
0.2 0.2 1.05 6.0 0.1 47.5 1.3 5.2 8.0 4.0 5.0RLD 0.5 0.2 0.2 0.35
2.0 0.1 9.5 1.0 2.6 13.3 5.84 5.0
1 1.5 2 2.5 3 3.5 4 4.5 5 5.5 66
4
2
0
2
4
6
8
Flow
(L/s)
Lung volume (L)
AC B
Pm=50
Pm=40
Pm=30
Pm=0
MEF
Pm=25
Normal
(a)
2.5 3 3.5 4 4.5 5 5.5 6 6.52
1.5
1
0.5
0
0.5
1
1.5
2
Lung volume (L)
Pm=50Pm=40
Pm=30
MEF
Pm=0A B C
Pm=25
OLD
(b)
1 1.5 2 2.5 34
3
2
1
0
1
2
3
4
5
6
Lung volume (L)
MEFPm=50
Pm=40
Pm=30
Pm=0A BC
Pm=25
RLD
(c)Fig. 2. Model simulated flow-volume profiles during forced
inspiration and expiration. Inspiratory and expiratory flow are
represented using negative andpositive values respectively. FEV1
for an expiratory muscle pressure of 40 cmH20 is indicated by a
circle. Solid lines represent forced inspiration at Pm= -25 cmH20
and forced expiration at Pm = 50 cmH2O. Dotted lines represent
forced expiration at Pm = 40 cmH2O. Dashed lines represent
forcedexpiration at Pm= 30 cmH2O. Dashed-dotted lines represent
passive expiration. Subplots illustrate flow-volume curves for (a)
a normal subject; (b) anOLD patient; and (c) a RLD patient.
and FVCr (Table III) are around 0.35 and 0.80
respectively,typical of OLD patients [16]. Figure 2(c) illustrates
forcedventilation in a patient with RLD. MEF is close to
normal,FEV1,r is higher than normal and FVCr is reduced to
0.48(Table III), typical of OLD patients [16].
IV. CONCLUSIONThis paper has described a model of respiratory
mechanics
modified from previous models built using the
functionalapproach. By including representation of nonlinear
pressure-volume curve of alveolar space and muscle pressure,
themodel can be used to simulate forced respiration. The resultsof
these simulations are consistent with the usual results oflung
function test in normal subjects and in patients withOLD and RLD,
illustrating that quite complex pathologiescan be simulated with
relatively simple models. Furtherwork is required to determine
whether unique values canbe obtained for all model parameters in
the clinical setting,enabling tuning of the model to the individual
patient.
REFERENCES[1] J. Rousselot, R. Peslin, and C. Duvivier,
Evaluation of the multiple
linear regression method to monitor respiratory mechanics in
ventilatedneonates and young children, Pediatr Pulmonol, vol. 13,
no. 3, pp.1618, 1992.
[2] B. Feinberg and E. Chester, A dynamic model of pulmonary
mechan-ics to simulate a panting maneuver, Bull Physiopathol
Respir, vol. 8,no. 2, pp. 30522, 1972.
[3] J. Golden, J. J. Clark, and P. Stevens, Mathematical
modeling ofpulmonary airway dynamics, IEEE Trans. Biomed. Eng.,
vol. 20,no. 6, pp. 397404, 1973.
[4] A. Verbraak, J. Bogaard, J. Beneken, and E. H. A.
Versprille, Seriallung model for simulation and parameter
estimation in body plethys-mography, Med Biol Eng Comput, vol. 29,
no. 3, pp. 30917, 1991.
[5] G. Avanzolini, P. Barbini, F. Bernardi, G. Cevenini, and G.
Gnudi,Role of the mechanical properties of tracheobronchial airways
indetermining the respiratory resistance time course, Ann Biomed
Eng,vol. 29, no. 7, pp. 57586, 2001.
[6] P. Barbini, G. Cevenini, and G. Avanzolni, Nonlinear
mechanismsdetermining expiratory flow limitation in mechanical
ventilation: amodel-based interpretation, Ann Biomed Eng, vol. 31,
no. 8, pp. 90816, 2003.
[7] J. Venegas, R. Harris, and B. Simon, A comprehensive
equation forthe pulmonary pressure-volume curve, J. Appl. Physiol.,
vol. 84, no. 1,pp. 38995, 1998.
[8] L. Pengelly, Curve-fitting analysis of pressure-volume
characteristicsof the lungs, J Appl Physiol, vol. 42, no. 1, pp.
111116, 1977.
[9] E. Salazar and J. Knowles, An analysis of pressure-volume
charac-teristics of the lungs, J Appl Physiol, vol. 19, pp. 97104,
1964.
[10] B. Murphy and L. Engel, Models of the pressure-volume
relationshipof the human lung, Respir Physiol, vol. 32, pp. 183194,
1978.
[11] E. Weibel, Morphometry of the Human Lung. Berlin:
Springer-Verlag,1963.
[12] F. Rohrer, Der stromungswiderstand in den menschlichen
atemwegenund der einfluss der unregelmassigen verzweigung des
bronchial-systems auf der atmungsverlauf in verschiedenen
lungenbezirken,Pflugers Arch. Gesamte Physiol Menschen Tiere, vol.
162, pp. 225299, 1915.
[13] J. Aerts, B. van den Berg, and J. Bogaard, Controlled
expiration inmechanically-ventilated patients with chronic
obstructive pulmonarydisease (copd), Eur Respir J, vol. 10, no. 3,
pp. 5506, 1978.
[14] T. Sera, H. Fujioka, H. Yokota, A. Makinouchi, R. Himeno,R.
Schroter, and K. Tanishita, Localized compliance of small airwaysin
excised rat lungs using microfocal x-ray computed tomography, JAppl
Physiol, vol. 96, no. 5, pp. 166573, 2004.
[15] A. Lumb, Nunns Applied Respiratory Physiology. U.K:
Butterworth& Co., 1997.
[16] A. Despopoulos and S. Silbernagl, Color Atlas of
Physiology. Ger-many: Thieme, 2003.
[17] C. Pereira, B. Julien, S. Rosselli, E. Combourieu, C.
Pommier,J. Perdrix, J. Richard, M. Badet, S. Gaillard, F. Philit,
and C. Guerin,Sigmoidal equation for lung and chest wall
volume-pressure curves inacute respiratory failure, J Appl Physiol,
vol. 95, no. 5, pp. 206471,2003.
6131
/ColorImageDict > /JPEG2000ColorACSImageDict >
/JPEG2000ColorImageDict > /AntiAliasGrayImages false
/DownsampleGrayImages true /GrayImageDownsampleType /Bicubic
/GrayImageResolution 300 /GrayImageDepth -1
/GrayImageDownsampleThreshold 2.00333 /EncodeGrayImages true
/GrayImageFilter /DCTEncode /AutoFilterGrayImages false
/GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict >
/GrayImageDict > /JPEG2000GrayACSImageDict >
/JPEG2000GrayImageDict > /AntiAliasMonoImages false
/DownsampleMonoImages true /MonoImageDownsampleType /Bicubic
/MonoImageResolution 600 /MonoImageDepth -1
/MonoImageDownsampleThreshold 1.00167 /EncodeMonoImages true
/MonoImageFilter /CCITTFaxEncode /MonoImageDict >
/AllowPSXObjects false /PDFX1aCheck false /PDFX3Check false
/PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true
/PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ]
/PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [
0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (None)
/PDFXOutputCondition () /PDFXRegistryName (http://www.color.org)
/PDFXTrapped /False
/Description >>> setdistillerparams>
setpagedevice