Embed Size (px)
DESCRIPTION
ILMU ANESTESI
Citation preview

RESEARCH Open Access
The Simple Triage Scoring System (STSS)successfully predicts mortality and critical careresource utilization in H1N1 pandemic flu: aretrospective analysisKayode A Adeniji*, Rebecca Cusack
Abstract
Introduction: Triage protocols are only initiated when it is apparent that resource deficits will occur across a broadgeographical area despite efforts to expand or acquire additional capacity. Prior to the pandemic the UKDepartment of Health (DOH) recommended the use of a staged triage plan incorporating Sepsis-related OrganFailure Assessment (SOFA) developed by the Ontario Ministry of Health to assist in the triage of critical careadmissions and discharges during an influenza outbreak in the UK. There are data to suggest that had it beenused in the recent H1N1 pandemic it may have led to inappropriate limitation of therapy if surge capacity hadbeen overwhelmed.
Methods: We retrospectively reviewed the performance of the Simple Triage Scoring System (STSS) as an indicatorof the utilization of hospital resources in adult patients with confirmed H1N1 admitted to a university teachinghospital. Our aim was to compare it against the staged initial SOFA score process with regards to mortality, needfor intensive care admission and requirement for mechanical ventilation and assess its validity.
Results: Over an 8 month period, 62 patients with confirmed H1N1 were admitted. Forty (65%) had documentedcomorbidities and 27 (44%) had pneumonic changes on their admission CXR. Nineteen (31%) were admitted tothe intensive care unit where 5 (26%) required mechanical ventilation (MV). There were 3 deaths. The STSS groupcategorization demonstrated a better discriminating accuracy in predicting critical care resource usage with areceiver operating characteristic area under the curve (95% confidence interval) for ICU admission of 0.88 (0.78-0.98) and need for MV of 0.91 (0.83-0.99). This compared to the staged SOFA score of 0.77 (0.65-0.89) and 0.87(0.72-1.00) respectively. Low mortality rates limited analysis on survival predictions.
Conclusions: The STSS accurately risk stratified patients in this cohort according to their risk of death andpredicted the likelihood of admission to critical care and the requirement for MV. Its single point in time, accuracyand easily collected component variables commend it as an alternative reproducible system to facilitate the triageand treatment of patients in any future influenza pandemic.
IntroductionThe word ‘triage’ originates from the French ‘trier’ (tochoose from among several) and was originally appliedaround 1792 by Baron Dominique Jean Larrey, surgeonin chief to Napoleon’s Imperial Guard, as a process ofsorting wounded soldiers. Its aim was to optimize the
use of available medical resources to maximize efficacy[1]. Patients with the greatest chance of survival withthe least resource use are treated first [2]. In disastersituations, the focus of medical care is directed towardthe needs of the community. In this approach, it is clearthat the standard of care for all patients, including thosenot directly related to the incident, may need to beadjusted and reduced. While this may infringe on indivi-dual rights, the higher ethical principle of ‘wellness of
* Correspondence: [email protected] Care Research Unit, SUHT, Southampton General Hospital, TremonaRoad, Southampton, SO16 6YD, UK
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
© 2011 Adeniji et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative CommonsAttribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction inany medium, provided the original work is properly cited.

society as a whole’ calls for the direction of resources tothose for whom it is felt to be the most effective.An influenza pandemic had been expected for a num-
ber of years. The resulting preparations led to the needto examine how different health-care systems aroundthe world could respond to such an event, which mayrequire a large surge in the need for critical care capa-city. On 11 June 2009, the World Health Organizationdeclared the first influenza pandemic since 1968. Emer-ging from a triple-reasortant virus circulating in NorthAmerican swine [3], the new influenza A virus variant,H1N1, has affected more than 213 countries and terri-tories worldwide [4]. Epidemiological models assumedthat the peak demand for critical care resources wouldsignificantly outstrip supply [5]. The pandemic declara-tion brought into sharp focus the strategic planning thatthe international community had been developing sincethe outbreak of avian flu H5N1 in 2005 [6]. Surge capa-city planning identified the need for a consistent andobjective triage system that was based on physiologicalscores and that was valid, reproducible, and transparentgiven the likelihood of a need to ration critical careresources [4].The UK Department of Health (DOH) recommended
a system devised by a panel of experts commissioned bythe Ontario Ministry of Health. This system was pro-posed to guide ‘critical care resource allocation issues’during the initial days and weeks of an overwhelminginfluenza pandemic and to prioritize admission to criti-cal care beds. After an exhaustive literature search, theSepsis-related Organ Failure Assessment (SOFA) score[7] was suggested as part of a staged triage and treat-ment prioritization tool to be used in association with anumber of inclusion and exclusion criteria based uponcomorbidities and estimated prognosis [8,9].The SOFA score has been shown to reliably evaluate
and quantify the degree of organ dysfunction present onadmission to the intensive care unit (ICU) (initial score)or developing during ICU stay (delta score equals subse-quent total maximum SOFA scores minus admissiontotal SOFA). The maximum SOFA score reflects cumu-lative organ dysfunction that develops and correlateswith mortality, whereas the mean score is a good prog-nostic indicator predicting outcome throughout an ICUstay [10,11].The Ontario Working Group’s proposal to aid mass
triage had no information on the epidemiology or patho-physiology of the virus that would cause the pandemic.The clinical course of H1N1 pandemic influenza has notoccurred as expected. As data has become accessible,reports suggest that SOFA score may not be a good dis-criminator of outcome in this cohort of patients [12,13].Thus, its suitability as a means to assist in the triage ofH1N1 patients has been called into question.
The Simple Triage Scoring System (STSS) (Table 1),which uses only those vital signs and patient characteris-tics that are readily available at initial presentation, wasproposed in 2007 by Talmor and colleagues [14] as apotential alternative tool in predicting death and the uti-lization of critical care resources during epidemics. Itscomponents are age, shock index (heart rate > bloodpressure), respiratory rate, oxygen saturation, andaltered mental state. In a multicenter retrospective ana-lysis of prospectively collected data, the STSS score vari-ables were validated in two cohorts of patients (n =1,927) presenting with sepsis to one of two emergencydepartments (EDs). The score was found to be predic-tive of the need for admission to the ICU and therequirement for mechanical ventilation (MV) and of theprimary outcome of mortality. Our objective was toreview the performance of the admission STSS andSOFA scoring systems as indicators of the utilization ofhospital resources and of mortality in H1N1 infectionpatients admitted to a UK university teaching hospital.
Materials and methodsIn a service evaluation assessment, we retrospectivelyreviewed the records of all adult patients who wereadmitted to the hospital and who were subsequentlyconfirmed to have contracted H1N1 between July 2009and February 2010. The study was conducted under theauspices of the Critical Care Department Research Unitof the Southampton University Hospital Trust. Pertinentdemographic data, comorbidity, initial chest x-ray (CXR)findings, mode of ventilatory support, level of care, beddays, mortality, and the physiological and laboratorycomponents required to calculate the STSS and SOFAscores at the point of hospital admission were collected.Where an arterial blood gas result was not available tocalculate the respiratory component of the SOFA score,the validated oxygen saturation as measured by pulseoximetry/fraction of inspired oxygen (SpO2/FiO2) ratiocorrelations derived by Pandharipande and colleagues[15] were used. Our institution’s pandemic flu protocolcalled for the involvement of critical care in any patientwhose FiO2 requirements exceeded 60% to maintain anarterial partial pressure of oxygen (PaO2) of greater than8 kPa. The discriminatory power of the individual scoregroupings was calculated and analyzed to assess theirperformance in the initial triage of the H1N1 patientwith reference to mortality (primary outcome) and theneed for ICU and need for MV (secondary outcomes).
StatisticsThe accuracy of each score in predicting outcome wasassessed by plotting the receiver operating characteristic(ROC) curve and calculating the area under the ROCcurve (AUC) with 95% confidence intervals [16].
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 2 of 9

The AUC values were ‘ranked’ as excellent (AUC of 0.90and above), good (AUC of from 0.80 to less than 0.90),fair (AUC of from 0.70 to less than 0.80), and poor(AUC of less than 0.70) (SPSS Statistics 19 Inc., Chi-cago, IL, USA, and IBM, Armonk, NY, USA).
ResultsSixty-two adult patients (35 males) were admitted to ourhospital from either the medical assessment unit or EDwith a polymerase chain reaction-confirmed diagnosis ofH1N1. Their mean age (range) was 41 (18 to 71) years(Table 2). Forty (65%) had either one (32) or two (8)comorbidities documented (25 respiratory), three weremorbidly obese, and three were pregnant. Twenty-seven(44%) had either a secondary bronchopneumonia orlobar pneumonia reported and formally confirmed by aconsultant radiologist on the admission CXR. Nineteen
(31%) were admitted to the ICU, where three requiredonly supplementary oxygen, 11 (58%) were managedwith noninvasive ventilation (NIV), and five (26%)required intubation and MV.There were three deaths, all with pneumonic features
on their admission CXRs, and two were invasively venti-lated. Of the two male patients with an STSS score of 2,one had chronic obstructive pulmonary disease (COPD)and the other had COPD and biventricular failure. Thelatter patient had been treated for H1N1 a week pre-viously and discharged home and re-presented with asecondary bacterial chest infection and associated sepsis.He was still H1N1-positive at this time. He suffered amyocardial infarction and went into multiple organ fail-ure. The patient with an STSS score of at least 3 was an18-year-old female with no comorbidities, presentedafter being symptomatic for 5 days with bilateralbronchopneumonic changes on her CXR, and died fromcomplications of extracorporeal membrane oxygenation(ECMO) at the national ECMO center.The median time from presentation to admission to
the ICU for 16 out of 19 (84%) patients was less than 24hours (range of 0 to 2 days). Of the three remainingpatients, two were admitted to the ICU after 24 hoursas in-patients and had STSS scores of 2 and SOFAscores of 3 and 5, respectively. The third patient wasadmitted to the ICU 48 hours after hospital admissionand had an STSS score of 2 and a SOFA score of 1; thatpatient did not survive. The median (range) numbers oflevel 2 and level 3 critical care bed days used for H1N1patients over the study period were 4 (2 to 23) and 23(1 to 46) days, respectively.A comparison of the STSS and SOFA score categori-
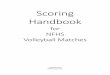
zation shows a reasonable agreement regarding theseverity of the patients’ illness (Figure 1). The admissionSTSS (Table 3) and initial SOFA (Table 4) scores werecalculated and compared against actual mortality, needfor ICU admission, and need for MV. The performanceof STSS and SOFA in our subset is compared with thefigures quoted in the original reports [9,13], in whichthe ROC AUC results were used to assess the perfor-mance of the individual score groupings.
Table 1 The Simple Triage Scoring System
Variable Odds ratio 95%confidenceinterval
Complex rule points Simplified (final) rule points
Respiratory rate >30 breaths per minute 3.9 2.5-6.3 4 1
Shock index >1 (HR > BP) 2.8 1.8-4.2 3 1
Low oxygen saturation 2.8 1.8-4.2 3 1
Altered mental status 1.9 1.3-2.8 2 1
Age of 65 to 74 years 3.0 1.7-5.5 3 1
Age of at least 75 years 4.4 2.7-7.2 4 1
BP, blood pressure; HR, heart rate. Reproduced with the kind permission of Wolters Kluwer Health [14].
Table 2 Clinical characteristics of H1N1 patients admittedto the hospital
Patient characteristics Ward-based ICU admissions
Number of patients 43 19
Age in years, median (range) 35 (19-71) 53 (18-71)
Sex
Male 26 9
Female 17 10
Comorbidity
1 20 12
2 3 5
≥3 0 0
Obese 0 3
Pregnant 3 0
Abnormal chest x-ray on admission
Bronchopneumonia 10 9
Lobar pneumonia 4 3
Pulmonary edema 0 1
Mode of ventilation: NIV/MV 0/0 11/5
Hospital outcomes
Bed days, median (range) 4 (0-13) 7 (1-46)
Mortality 0 3a
aOne patient was transferred from the intensive care unit (ICU) to the wardfor palliation. MV, mechanical ventilation; NIV, noninvasive ventilation.
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 3 of 9

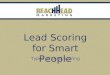
Owing to the low H1N1-related mortality rate in ourcohort, analysis of this outcome data was not possible.However, the trends suggest that a higher STSS scoreequates with higher mortality in comparison with a highSOFA score. The SOFA score performed well in pre-dicting the need for admission to the ICU (ROC AUC0.77; 0.65 to 0.89) and the requirement for MV (ROCAUC 0.87; 0.72 to 1.00). Nonetheless, the performanceof the STSS score was better at predicting need for ICUadmission (ROC AUC 0.88; 0.78 to 0.98) and need forMV (0.91; 0.83 to 0.99) (Figure 2).If the exclusion criteria within the staged triage proto-
col that incorporated SOFA (developed by Ontario andrecommended by the UK DOH) - that is, SOFA score
of greater than 11, chronic lymphocytic leukemia (afterallogenic transplant), lymphoma (after allogenic trans-plant), cervical cancer, and cystic fibrosis - had beenapplied, a total of five patients would have beenexcluded from ICU admission. All of these patients sur-vived this hospital admission to discharge.
DiscussionDuring a mass casualty event, the triage of patients todetermine those who may require, do require, and arereceiving definitive critical care interventions needs con-tinuous re-evaluation to impartially allocate the limitedresources. Once surge capacity has reached its limit, thedelivery of critical care moves to the ‘process of last
0
5
10
15
20
25
0 1 2 3
No. of Patients
STSS Scores
>11
10 11
8 9
6 7
4 5
2 3
0 1
SOFA Scores
Figure 1 Graph comparing the calculated Simple Triage Scoring System (STSS) with the Sepsis-related Organ Failure Assessment(SOFA) score patient categories.
Table 3 Discrimination of STSS score groupings in predicting death, ICU admission, and need for mechanicalventilation in our study population (n = 62) and the derivation population (n = 3,206)
STSSscore
Mortality,fraction (percentage)
Need for ICU Need for MV,fraction (percentage)
Derivationgroupa
n = 3,206
Study groupn = 62
Derivationgroupa, fraction(percentage)
Study group,fraction
(percentage)
Study bed days, median(range)
Derivationgroupa
Studygroup
0 5/1,144 (0.4) 0/19 (0) 61/1,144 (5.3) 1/19 (5.3) 4 18/1,144 (1.6) 0/19 (0)
1 45/1,257 (3.6) 0/21 (0) 124/1,257 (9.9) 2/21 (9.5) 3 (2-4) 37/1,257 (2.9) 0/21 (0)
2 54/617 (8.8) 2/13 (15.3) 140/617 (23) 7/13 (53.8) 9 (2-46) 43/617 (7) 1/13 (7.7)
≥ 3 47/188 (25) 1/9 (11.1) 68/188 (36) 8/9 (88.8) 8 (3-24) 25/188 (13) 4/9 (44.4)
ROCAUC(95% CI)
0.8 Sample toosmall
0.7 0.88(0.78-0.98)b
- 0.69 0.91(0.83-0.99)
b
aTalmor and colleagues [14]; bFigure 2: Receiver operating characteristic (ROC) curves for Simple Triage Scoring System (STSS) versus intensive care unit (ICU) andSTSS versus mechanical ventilation (MV). AUC, area under the curve; CI, confidence interval.
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 4 of 9

resort’ (that is, triage) [17]. Ideally, the selected prioriti-zation tool needs not only to be able to facilitate tertiarycritical care triage (the allocation of mechanical ventila-tors) [18] but also to be applied in the community,assisting general practitioners in deciding which patientsshould be referred to the hospital and assisting hospitalphysicians in deciding whether referral to the ICU isappropriate [19].Recently, there has been a great effort to define these
prerequisite basic concepts and assumptions to cope withcritical care resource allocation with many references tomilitary experience. Standard operating proceduresdescribing the rationale, components, implementation,and framework to guide and support the development oflocal and national protocols, particularly with regard tomass infection, have been published [20-22].A decision matrix in which the weight of objective
prognostic information supersedes any subjective orindividual patient factors may be an uncomfortableparadigm of deliberation for the physician. Therefore, toensure justice both to the physician and to the patient,there has to be institutional oversight and ‘guidelines’.A triage plan will equitably provide every person theopportunity to survive but cannot guarantee either treat-ment or survival [8]. However, such a plan cannotsupersede the judgment of a physician faced with thetriage situation as it is only upon retrospective analysis
of the true outcomes of individual patients comparedwith their predicted outcomes and triaged status that anevaluation of the appropriateness and justice of thetriage decision can be made [2].The SOFA score was originally designed to describe
the morbidity ensuing from organ dysfunction in criti-cally ill patients over the course of their ICU stay. Themaximum SOFA score and the delta SOFA have beenshown to be good instruments in the evaluation andquantification of the degree of organ dysfunction/failurepresent on admission to the ICU [11]. Ferreira and col-leagues [10] evaluated the initial, mean, highest, anddelta SOFA scores in a cohort of 352 patients admittedto their ICU in Belgium. Scores were then correlatedwith mortality. The authors showed that an initial SOFAscore of up to 9 predicted a mortality of less than 33%whereas a score of greater than 11 predicted a mortalityof 95%. When the initial score was 8 to 11, anunchanged or increasing score was associated with amortality rate of 60% (initial score of 2 to 7 and mortal-ity of 37%). Therefore, a positive delta SOFA score dur-ing the first 48 hours of an ICU admission predicted amortality of at least 50%.The Ontario protocol, as in the military, advocated the
application of a color-coded prioritization tool. Reassess-ment would occur at specified time periods (approxi-mately 48 and 120 hours) by a member of the triage
Table 4 Discrimination of initial SOFA score groupings in predicting mortality in our study population (n = 62) and inthe derivation population (n = 352)
InitialSOFAScore
Mortality,fraction (percentage)
Need for ICU Need for MV, fraction(percentage)
Derivationgroupa
n = 352
Study groupn = 62
Study group,fraction
(percentage)
Study bed days, median(range)
Study group
0-1 0/43(0)
1/21(4.8)
2/21(9.5)
10.5(4-17)
0/21(0)
2-3 5/77(6.5)
1/25(4)
9/25(36)
4(2-23)
2/25(8)
4-5 18/89(20.2)
0/10(0)
2/10(20)
15(8-22)
0/10(0)
6-7 14/65(21.5)
1/5(20)
5/5(100)
4(1-46)
2/5(40)
8-9 11/33(33.3)
0/0(0)
0/0(0)
0 0/0(0)
10-11 12/24(50)
0/0(0)
0/0(0)
0 0/0(0)
>11 20/21(95.2)
0/1(0)
1/1(100)
24 1/1(100)
ROC AUC (95%CI)
0.79 Sample toosmall
0.77 (0.65-0.89)b - 0.87 (0.72-1.00)b
>11 andexclusion criteria
20/21(95.2)
0/5(0)
3/5(60)
- 2/5(40)
These data were used to assess whether Sepsis-related Organ Failure Assessment (SOFA) score had some functionality in predicting need for intensive care unit(ICU) and need for mechanical ventilation (MV) in our study group. aFerreira and colleagues [10]; bFigure 2: Receiver operating characteristic (ROC) curves forSOFA versus ICU and SOFA versus MV. AUC, area under the curve; CI, confidence interval.
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 5 of 9

team. Patients not meeting the inclusion criteria at reas-sessment or deteriorating and not expected to survive aretransferred to the ward for ongoing care or palliation,respectively. This re-evaluation would also be applied toward-based patients who deteriorate or improve. The‘cutoff’ would be the presentation with or development ofa SOFA score of greater than 11 [2,8,19,20,22].Predictive validity considers the degree to which the
triage acuity level predicts true acuity. The primary pro-blem with predictive scoring systems is that they arepopulation-specific and are derived from and validatedon specific cohorts of patients and thus their ability to
predict the outcome of an individual is poor [23].Therefore, the decision to reassign a mechanical ventila-tor from one patient to another would be difficult tojustify unless a large difference (approximately 25%) [22]in the survival advantage predicted by the scoring sys-tem were demonstrated. Critical care scoring systemshave not been designed for this purpose.In this study, we assessed the performance of an alter-
native scoring system, the STSS, in H1N1 patientsadmitted to a UK teaching hospital. We compared thiswith the initial SOFA score as the organ dysfunctionmeasure within a triage prioritization tool. To our
Figure 2 Comparisons of the area under the receiver operating characteristic curves predicting admission to the intensive care unitand requirement for mechanical ventilation. (A) STSS scores ability to predict the H1N1 patients admission to the ICU. (B) SOFA scores abilityto predict the H1N1 patients admission to the ICU. (C) STSS scores ability to predict the H1N1 patients subsequent need for mechanicalventilation. (D) SOFA scores ability to predict the H1N1 patients subsequent need for mechanical ventilation. SOFA, Sepsis-related Organ FailureAssessment; STSS, Simple Triage Scoring System.
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 6 of 9

knowledge, the performance of STSS has not beentested on patients during a pandemic. Although theSTSS was developed in a cohort of individuals present-ing with a variety of infectious diseases to an ED, it wasrecommended for use during a pandemic. It is simpleand can be carried out by a wide range of health-carestaff in a variety of settings. Importantly, the STSS scoreexcludes both the patient’s history (which may not beavailable at the point of entrance into the medical sys-tem) and laboratory testing (which adds time delay totriage). SOFA incorporation of the latter would result ina delay in decision making and consumption ofstretched laboratory resources. Additionally, whereas thevariability in the subjective assessment of the GlasgowComa Scale component in the SOFA may affect itsinter-observer accuracy, the binary nature of the com-parison measure in the STSS of ‘altered mental state’may ameliorate this source of error. In our cohort ofpatients, STSS performed well, risk-stratifying patientswith this viral illness with regard to the need for admis-sion to the ICU and need for MV.The clinical nature of any pandemic becomes apparent
only as the event unfolds. Fortunately, the mortality ofH1N1 has been considerably less than that seen withH5N1. It is widely reported that the clinical attack rateand most severe disease have been highest in the young[24]. The Australasian and Canadian experiences of the2009 pandemic demonstrated how population differ-ences in different communities can confound the appli-cation of ‘evidence’ across these disparate populations.Kumar and colleagues [25] reported that 43/168 (25.6%)of critically ill flu patients in Canada over the perioddescribed were Inuit, who represent just 3.75% of thepopulation. Similarly, the ANZIC (Australian and NewZealand Intensive Care) investigators reported that theAboriginals (2.5% of the population) represented 9.7% ofthe ICU admissions in Australia and the Maoris (13.6%of the population) emerged as 25% of the critically ill inNew Zealand [25,26]. The pattern of illness was mark-edly different in our population. Without a native indi-genous population that may have lacked exposure toprevious H1N1 epidemics and in the context of freelyavailable antivirals and latterly a specific pandemic vac-cine, we were fortunate to suffer only three deaths inour study population. In addition, a large number of ouralmost entirely European Caucasian patients benefitedfrom the application of NIV - this was not seen in eitherCanada or Australasia. Our low mortality rate preventedassessment of the STSS scores’ discriminatory potentialwith regard to H1N1.Although the STSS scale has only 4 points (as
opposed to a maximum of 24 on the SOFA scale), theSTSS discriminated between outcomes equally well inthis study, and crude data analysis suggest that it may
be better. The ROC areas for the STSS score whichrelated to both secondary outcomes of ICU admissionand need for MV demonstrated both higher values andbetter fit than the SOFA score values, despite our smallsample size.Although the Ontario staged triage protocol has not
been evaluated as a predictor of health-care resourceusage, our study suggests that SOFA’s utility in thisrespect was fair for ICU admission (AUC 0.77) andgood for MV (AUC 0.87). Part of the Ontario’s recom-mended remit was to ‘identify at an early stage thosepatients not responding to treatment and thereforelikely to have a poor outcome ... once treatment andcare start ... by formal periodic assessments to determinewhether ... they are not responding to treatment or aredeteriorating despite treatment, and so further treatmentshould be withheld in favor of symptom relief’ [19]. Fer-reira and colleagues [10] note that length of stay (LOS)was not related to outcome prediction when usingSOFA and that the mean SOFA score had a better prog-nostic value than the other SOFA-derived variables; thatis, patients who presented with a limited degree oforgan dysfunction and had a long stay could still have ahigh likelihood of survival.An increase in SOFA score in the first 48 hours is
associated with 53% risk of death and a mean LOS 12.4days. However, Khan and colleagues [12] showed 63%survival in their SOFA defined poor prognosis groupwith H1N1 with a mean LOS of 11 (range of 3 to 17)days. This presents a problem if we assume that theDOH intended that the triage tool be applied to limitthose 12.4 days by early palliation. If we also considerthe published risk of death following delta SOFA reduc-tion (23%) to the risk of death with delta SOFA increase(37%) of Khan and colleagues, this significantly narrowsthe difference in risk between those who would possiblydie or possibly survive (14%). Hick and colleagues [22]suggest that this level of difference would not be enoughto confidently reallocate ventilator resources.The SOFA score was designed for ICU admission, and
the STSS system was designed for hospital admission.Their use as the organ dysfunction component within atriage prioritization tool designed for use at all levels ofhealth-care delivery from community to critical careobviates any concerns about the difference between sec-ondary and tertiary triage measures. Eighty-four percentof the patients were transferred to the ICU less than24 hours after their admission and we would thereforehave expected an equivalent or better performance fromthe SOFA score. The three patients who had theirscores calculated at a time distant from their admissionto the ICU had SOFA scores ranging from 1 to 5 andan STSS score of 2. The patient with the SOFA score of1 was admitted to the ICU after 2 days as an in-patient
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 7 of 9

but did not survive; he was readmitted to the hospitalwith pneumonia after being discharged home (but stillH1N1-positive) and died of multi-organ failure.We would submit that these factors suggest that the
STSS performs better in this population and overallwould be a more appropriate early-assessment triagerule. Given the heterogeneity of possible events causinga mass casualty episode, no single tool can be expectedto provide adequate decision-making power. Owing tothe potential uncertainty arising from each individualpatient’s physiological response to treatment, scoringsystems must be tempered by clinical decision makingand viewed as indicators to assist clinical assessmentsand not as definitive triaging values. Owing to theunpredictable nature of any new strain of a pandemicvirus, many authorities call for continuous revalidationand refinement of any triage model and its scoring sys-tems at the point of outbreak and throughout all of itsphases to thereby determine their suitability and discri-minating power for use as triage prioritization tools at amulticenter/national level [8,18,19].It is clear that, in the absence of a thoughtful
approach to triage, critical care resources would bedepleted within the first weeks of a pandemic. Suchtriage tools will also require a staged approach thatneeds to start with the patient in the community and totriage in a stepwise manner those who ultimately willrequire maximum care in a critical care unit. The STSSscore is designed to be used at the front door of thehospital and may be of value in indicating patients whowill require high resource utilization. In our smallcohort, it appeared to perform as well as, if not betterthan, the SOFA score in identifying those who neededICU care. The focus at the hospital level would be onestablishing the process that will be followed at thehealth-care facility. This is crucial because, regardless ofthe origin of the decision tool, the implementation ofthe tool occurs at the hospital level [22]. Therefore, ade-quate workforce knowledge and training regarding theunderlying principles of any prioritization tool arerequired to overcome the natural reluctance of medicalstaff to ‘ration’ their care delivery [27].Our study is limited by its retrospective nature, size,
and number of significant events. The performance ofSTSS scores in ‘all comers’ to the ED and specifically tothe ICU as well as over the time course of each indivi-dual admission was not assessed, raising concerns aboutthe validity of these scores in other critically ill patients.However, it should be remembered that the SOFA scorewas also initially developed, in 1996, as a sepsis-relatedscore [7]. What our study highlights is that mandating aparticular scoring system may not be the best approach.Perhaps considering different tools in the early phase,
including perhaps one employing a disease-specific scor-ing system, and quickly assessing their utility may bethe most pragmatic approach until the clinical courseand pathophysiology of the particular influenza variantbecome apparent.
ConclusionsIn summary, it would appear that the four groupings ofthe STSS score, despite being underpowered because ofa small sample size, number of deaths, and percentageof those mechanical ventilated, ‘accurately’ risk-stratifypatients in this cohort according to their risk of deathand predict the likelihood of admission to critical careand the requirement for mechanical ventilation in linewith the derivation population. The fact that the STSSscore is measured at a single point in time, its accuracy,and its easily collected component variables commend itas an alternative reproducible system to facilitate thetriage and treatment of patients in any future influenzapandemic. Further analysis should include a prospectiveevaluation of its validity as a staged protocol in a largercohort of unselected unwell patients presenting to theED and an assessment of its morbidity and mortalityprediction in different populations once those patientshave been admitted to the ICU.
Key messages• The Simple Triage Scoring System (STSS) score iseasier to calculate and accurately predicts criticalcare resource usage (admission to the intensive careunit and requirement for mechanical ventilation) inH1N1 with initial hospital presentation parameters.• Further analysis of the STSS score as a predictor ofmortality in this cohort of patients should beinvestigated.• The STSS score should be considered an alterna-tive triage tool in future epidemics.
AbbreviationsAUC: area under the curve; COPD: chronic obstructive pulmonary disease;CXR: chest x-ray; DOH: Department of Health; ECMO: extracorporealmembrane oxygenation; ED: emergency department; FiO2: fraction ofinspired oxygen; ICU: intensive care unit; LOS: length of stay; MV: mechanicalventilation; NIV: noninvasive ventilation; ROC: receiver operatingcharacteristic; SOFA: Sepsis-related Organ Failure Assessment; STSS: SimpleTriage Scoring System.
AcknowledgementsThe authors would like to acknowledge Kim de Courcy-Golder for hercollection of the data that informed the study and Bernard Higgins for hiscontribution to the statistical analysis of our findings.
Authors’ contributionsBoth authors participated in the formulation and design of this study,performed the literature search, and abstracted the data. KAA wrote the firstdraft of the manuscript, which was then revised by RC. Both authors readand approved the final manuscript.
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 8 of 9

Competing interestsThe authors declare that they have no competing interests.
Received: 28 May 2010 Revised: 26 November 2010Accepted: 26 January 2011 Published: 26 January 2011
References1. Robertson-Steel I: Evolution of triage systems. Emerg Med J 2006,
23:154-155.2. Repine TB, Lisagor P, Cohen DJ: The dynamics and ethics of triage:
rationing care in hard times. Mil Med 2005, 170:505-509.3. Smith GJ, Vijaykrishna D, Bahl J, Lycett SJ, Worobey M, Pybus OG, Ma SK,
Cheung CL, Raghwani J, Bhatt S, Peiris JS, Guan Y, Rambaut A: Origins andevolutionary genomics of the 2009 swine-origin H1N1 influenza Aepidemic. Nature 2009, 459:1122-1125.
4. World Health Organization: Pandemic (H1N1) 2009 - update 9. [http://www.who.int/csr/don/2010_03_12/en/index.html].
5. Ercole A, Taylor BL, Rhodes A, Menon DK: Modelling the impact of aninfluenza A/H1N1 pandemic on critical care demand from earlypathogenicity data: the case for sentinel reporting. Anaesthesia 2009,64:937-941.
6. Beigel JH, Farrar J, Han AM, Hayden FG, Hyer R, de Jong MD, Lochindarat S,Nguyen TK, Nguyen TH, Tran TH, Nicoll A, Touch S, Yuen KY, WritingCommittee of the World Health Organization (WHO) Consultation onHuman Influenza A/H5: Avian influenza A (H5N1) infection in humans. NEngl J Med 2005, 353:1374-1385.
7. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H,Reinhart CK, Suter PM, Thijs LG: The SOFA (Sepsis-related Organ FailureAssessment) score to describe organ dysfunction/failure. On behalf ofthe Working Group on Sepsis-Related Problems of the European Societyof Intensive Care Medicine. Intensive Care Med 1996, 22:707-710.
8. Christian MD, Hawryluck L, Wax RS, Cook T, Lazar NM, Herridge MS,Muller MP, Gowans DR, Fortier W, Burkle FM: Development of a triageprotocol for critical care during an influenza pandemic. CMAJ 2006,175:1377-1381.
9. Christian M, Hamielec C, Lazar N, Wax R, Griffith L, Herridge M, Lee D,Cook DJ: A retrospective cohort pilot study to evaluate a triage tool foruse in a pandemic. Crit Care 2009, 13:R170.
10. Ferreira FL, Bota DP, Bross A, Melot C, Vincent J: Serial evaluation of theSOFA score to predict outcome in critically ill patients. JAMA 2001,286:1754-1758.
11. Moreno R, Vincent JL, Matos R, Mendonça A, Cantraine F, Thijs L, Sprung C,Antonelli M, Bruining H, Willatts S: The use of maximum SOFA score toquantify organ dysfunction/failure in intensive care. Results of aprospective, multicentre study. Working Group on Sepsis relatedProblems of the ESICM. Intensive Care Med 1999, 25:686-696.
12. Khan Z, Hulme J, Sherwood N: An assessment of the validity of SOFAscore based triage in H1N1 critically ill patients during an influenzapandemic. Anaesthesia 2009, 64:1283-1288.
13. Guest T, Tantam G, Donlin N, Tantam K, McMillan H, Tillyard A: Anobservational cohort study of triage for critical care provision duringpandemic influenza: ‘clipboard physicians’ or ‘evidenced basedmedicine’? Anaesthesia 2009, 64:1199-1206.
14. Talmor D, Jones AE, Rubinson L, Howell MD, Shapiro NI: Simple triagescoring system predicting death and the need for critical care resourcesfor use during epidemics. Crit Care Med 2007, 35:1251-1256.
15. Pandharipande PP, Shintani AK, Hagerman HE, St Jacques PJ, Rice TW,Sanders NW, Ware LB, Bernard GR, Ely EW: Derivation and validation ofSpo2/Fio2 ratio to impute for Pao2/Fio2 ratio in the respiratorycomponent of the Sequential Organ Failure Assessment score. Crit CareMed 2009, 37:1317-1321.
16. Zweig MH, Campbell G: Receiver-operating characteristic (ROC) plots: afundamental evaluation tool in clinical medicine. Clin Chem 1993,39:561-577.
17. Tillyard A: Reorganising the pandemic triage processes to ethicallymaximise individuals’ best interests. Intensive Care Med 2010,36:1966-1971.
18. Challen K, Bentley A, Bright J, Walter D: Clinical review: mass casualtytriage - pandemic influenza and critical care. Crit Care 2007, 11:212-212.
19. Department of Health: Pandemic flu: managing demand and capacity inhealth care organisations (surge). [http://www.dh.gov.uk/en/
Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_098769].
20. Christian MD, Joynt GM, Hick JL, Colvin J, Danis M, Sprung CL: Chapter 7.Critical care triage. Recommendations and standard operatingprocedures for intensive care unit and hospital preparations for aninfluenza epidemic or mass disaster. Intensive Care Med 2010, 36(Suppl 1):S55-S64.
21. Sprung CL, Zimmerman JL, Christian MD, Joynt GM, Hick JL, Taylor B,Richards GA, Sandrock C, Cohen R, Adini B, European Society of IntensiveCare Medicine Task Force for Intensive Care Unit Triage during an InfluenzaEpidemic or Mass Disaster: Recommendations for intensive care unit andhospital preparations for an influenza epidemic or mass disaster:summary report of the European Society of Intensive Care Medicine’sTask Force for intensive care unit triage during an influenza epidemic ormass disaster. Intensive Care Med 2010, 36:428-443.
22. Hick J, Rubinson L, O’Laughlin D, Farmer JC: Clinical review: allocatingventilators during large-scale disasters - problems, planning, andprocess. Crit Care 2007, 11:217.
23. Zygun DA, Laupland KB, Fick GH, Sandham JD, Doig CJ: Limited ability ofSOFA and MOD scores to discriminate outcome: a prospectiveevaluation in 1,436 patients. Can J Anaesth 2005, 52:302-308.
24. Writing Committee of the WHO Consultation on Clinical Aspects ofPandemic (H1N1) 2009 Influenza, Bautista E, Chotpitayasunondh T, Gao Z,Harper SA, Shaw M, Uyeki TM, Zaki SR, Hayden FG, Hui DS, Kettner JD,Kumar A, Lim M, Shindo N, Penn C, Nicholson KG: Clinical aspects ofpandemic 2009 influenza A (H1N1) virus infection. N Engl J Med 2010,362:1708-1719.
25. Kumar A, Zarychanski R, Pinto R, Cook DJ, Marshall J, Lacroix J, Stelfox T,Bagshaw S, Choong K, Lamontagne F, Turgeon AF, Lapinsky S, Ahern SP,Smith O, Siddiqui F, Jouvet P, Khwaja K, McIntyre L, Menon K, Hutchison J,Hornstein D, Joffe A, Lauzier F, Singh J, Karachi T, Wiebe K, Olafson K,Ramsey C, Sharma S, Dodek P, Meade M, et al: Critically ill patients with2009 influenza A(H1N1) infection in Canada. JAMA 2009, 302:1872-1879.
26. ANZIC Influenza Investigators, Webb SA, Pettilä V, Seppelt I, Bellomo R,Bailey M, Cooper DJ, Cretikos M, Davies AR, Finfer S, Harrigan PW, Hart GK,Howe B, Iredell JR, McArthur C, Mitchell I, Morrison S, Nichol AD,Paterson DL, Peake S, Richards B, Stephens D, Turner A, Yung M: Criticalcare services and 2009 H1N1 influenza in Australia and New Zealand. NEngl J Med 2009, 361:1925-1934.
27. Tourtier J, Auroy Y: Triage tools errors. Crit Care Med 2010, 38:1500-1501.
doi:10.1186/cc10001Cite this article as: Adeniji and Cusack: The Simple Triage ScoringSystem (STSS) successfully predicts mortality and critical care resourceutilization in H1N1 pandemic flu: a retrospective analysis. Critical Care2011 15:R39.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Adeniji and Cusack Critical Care 2011, 15:R39http://ccforum.com/content/15/1/R39
Page 9 of 9