Embed Size (px)
Citation preview
Shoulder Injuries in the Shoulder Injuries in the Young Throwing AthleteYoung Throwing Athlete
Ken Ken KrogmanKrogman, PT/ATC, PT/ATCSports Medicine ConferenceSports Medicine Conference
ObjectivesObjectives
Describe epidemiology and presentation of Describe epidemiology and presentation of common adolescent shoulder injuriescommon adolescent shoulder injuriesDiscuss humeral head retroversionDiscuss humeral head retroversionDiscuss intrinsic and extrinsic factors of Discuss intrinsic and extrinsic factors of these injuriesthese injuriesDiscuss rehabilitation and prevention Discuss rehabilitation and prevention considerationsconsiderationsPromote a new throwing analysis program Promote a new throwing analysis program with indications for referralwith indications for referral
EpidemiologyEpidemiology
2.6 million athletes in Little League in 20072.6 million athletes in Little League in 2007Ages 9Ages 9--1414380K in Pop Warner in 2007380K in Pop Warner in 2007
~30% of pitchers self~30% of pitchers self--report shoulder pain per report shoulder pain per season; 9% of pitching outings produce painseason; 9% of pitching outings produce pain
20% ages 820% ages 8--12 report 12 report armarm pain, 45% ages 13pain, 45% ages 13--1414
Dx’sDx’s: Little Leaguer’s shoulder, fractures, : Little Leaguer’s shoulder, fractures, instability, RTC (instability, RTC (osos acromialeacromiale), SLAP), SLAP
Current DataCurrent Data--
UNC UNC (Marshall and Mueller)(Marshall and Mueller)
5 year study with annual questionnaires5 year study with annual questionnairesyear 1year 1-- 404 pitchers from ~50 Little Leagues 404 pitchers from ~50 Little Leagues across the US involved at Year 1 across the US involved at Year 1 year 2year 2-- f/uf/u LL and initial HSLL and initial HSyear 3year 3-- f/uf/u LL, LL, f/uf/u HS, initial collegeHS, initial collegeyear 4year 4-- f/uf/u all 3 groupsall 3 groupsyear 5year 5-- ??
Current DataCurrent Data--
UNCUNC
Major Year 1 findings:Major Year 1 findings:42% also pitched in another league42% also pitched in another league
24% pitched in LL and Travel League at same time24% pitched in LL and Travel League at same time
99% throw a fastball, 75% change99% throw a fastball, 75% change--up, 33% up, 33% curve, 19% knuckleball, 9% slidercurve, 19% knuckleball, 9% slider18.9% report elbow pain, 18.6% shoulder pain18.9% report elbow pain, 18.6% shoulder pain38.6% have pitched when arm was tired38.6% have pitched when arm was tired50% use ice as pain relief, 20% use 50% use ice as pain relief, 20% use NSAIDsNSAIDs
5% use 5% use NSAIDsNSAIDs to pitchto pitch
Pitching BiomechanicsPitching Biomechanics
Youth Pitching Data, 2008Youth Pitching Data, 200829 athletes 12.5 (+/29 athletes 12.5 (+/-- 1.7) 1.7) y.oy.o..Max GH ER= 178 (+/Max GH ER= 178 (+/-- 12)12)°°Shoulder IR Shoulder IR torqtorq= 35 (+/= 35 (+/-- 16) Nm16) NmElbow Elbow varusvarus torqtorq= 35 (+/= 35 (+/-- 15) Nm15) NmIR velocity= 7182 (+/IR velocity= 7182 (+/-- 1313)1313)°°/sec/secShoulder proximal force= 466 (+/Shoulder proximal force= 466 (+/-- 170) N170) N
Above data with fastballsAbove data with fastballs-- 58.8 (+/58.8 (+/-- 8.5) 8.5) mphmph
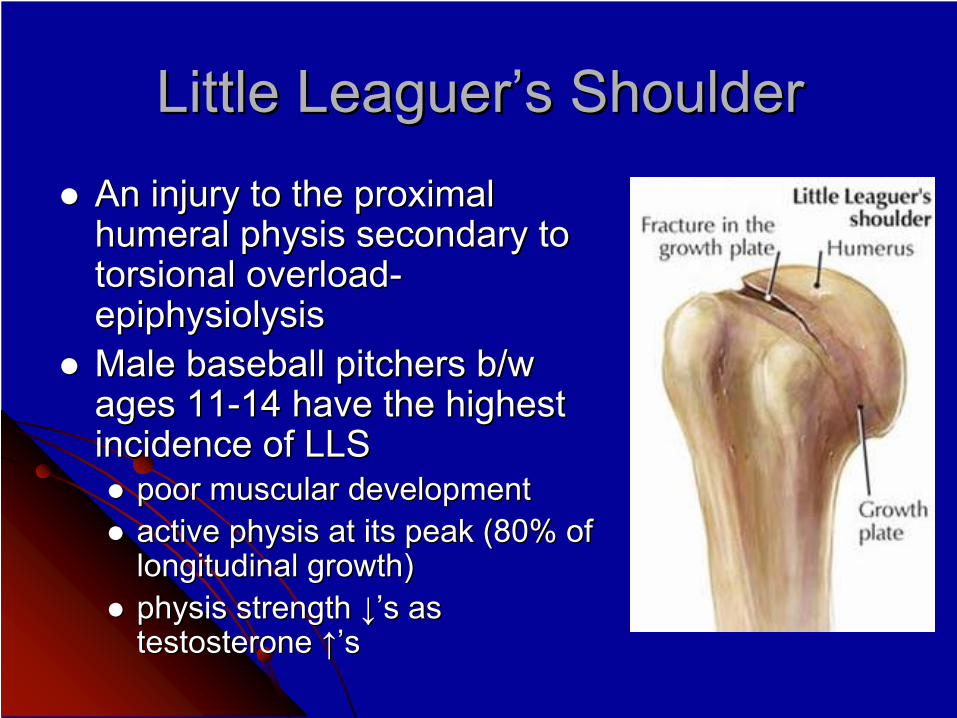
Little Leaguer’s ShoulderLittle Leaguer’s ShoulderAn injury to the proximal An injury to the proximal humeral humeral physisphysis secondary to secondary to torsionaltorsional overloadoverload--epiphysiolysisepiphysiolysisMale baseball pitchers b/w Male baseball pitchers b/w ages 11ages 11--14 have the highest 14 have the highest incidence of LLSincidence of LLS
poor muscular developmentpoor muscular developmentactive active physisphysis at its peak (80% of at its peak (80% of longitudinal growth)longitudinal growth)physisphysis strength strength ↓↓’’s s as as testosterone testosterone ↑↑’’ss
Little Leaguer’s ShoulderLittle Leaguer’s Shoulder
Signs and symptomsSigns and symptomsProximal humeral pain during (hard) throwing, Proximal humeral pain during (hard) throwing, typically asymptomatic otherwisetypically asymptomatic otherwiseCorrelation with throwing >12 monthsCorrelation with throwing >12 monthsVisual exam typically unremarkableVisual exam typically unremarkablePossible painful arc, typically no ROM lossPossible painful arc, typically no ROM lossTTP over TTP over proxprox humerushumerus in up to 80%in up to 80%
Little Leaguer’s ShoulderLittle Leaguer’s Shoulder
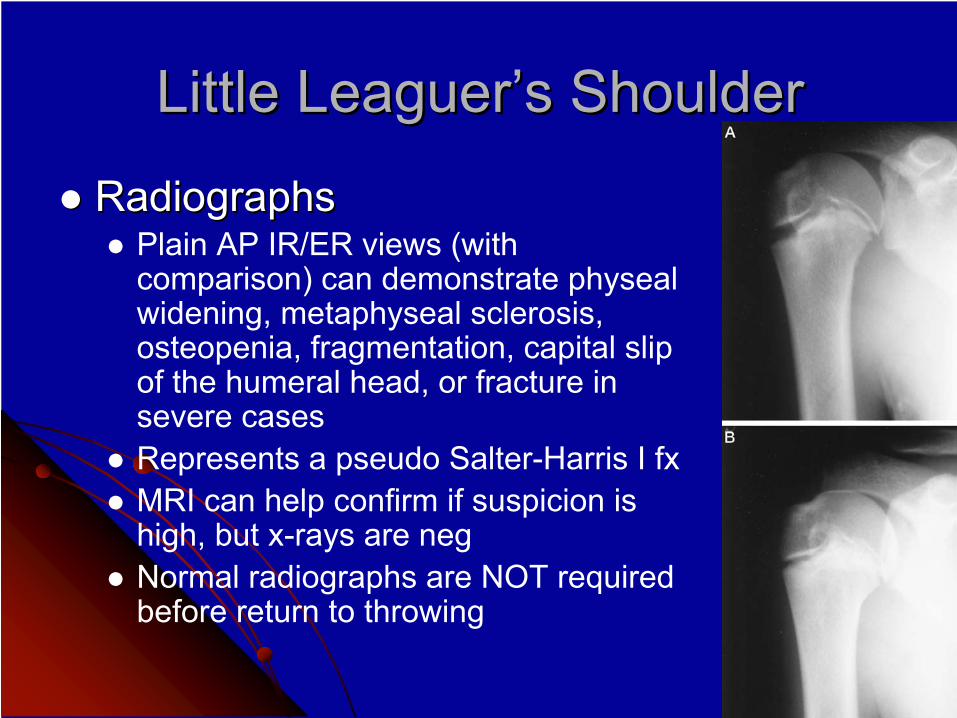
RadiographsRadiographsPlain AP IR/ER views (with comparison) can demonstrate physealwidening, metaphyseal sclerosis, osteopenia, fragmentation, capital slip of the humeral head, or fracture in severe casesRepresents a pseudo Salter-Harris I fxMRI can help confirm if suspicion is high, but x-rays are negNormal radiographs are NOT required before return to throwing
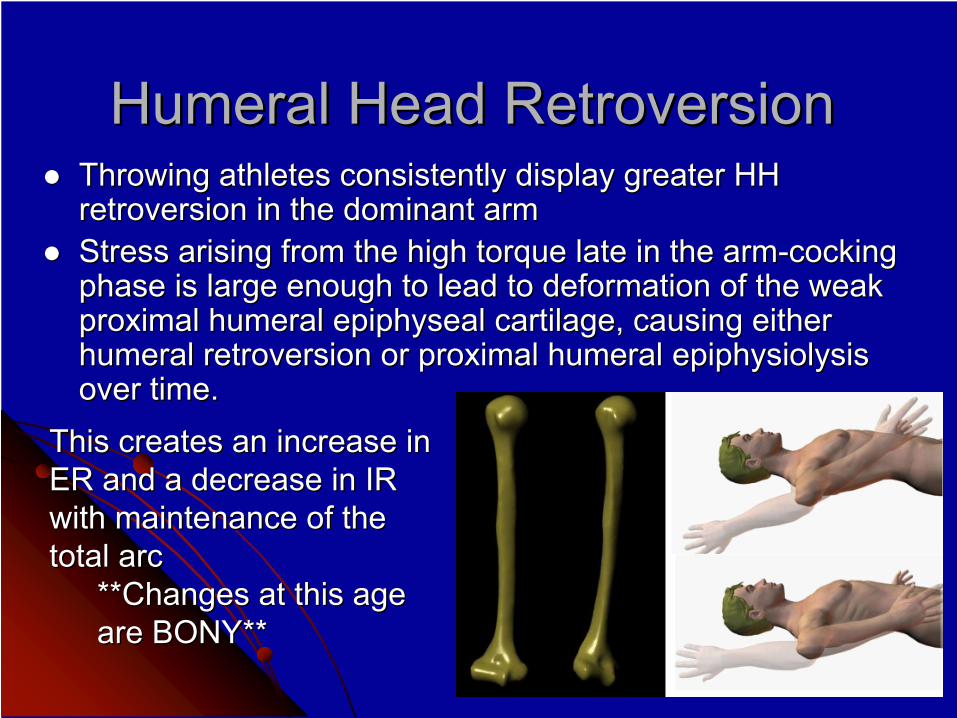
Humeral Head RetroversionHumeral Head RetroversionThrowing athletes consistently display greater HH Throwing athletes consistently display greater HH retroversion in the dominant armretroversion in the dominant armStress arising from the high torque late in the armStress arising from the high torque late in the arm--cocking cocking phase is large enough to lead to deformation of the weak phase is large enough to lead to deformation of the weak proximal humeral proximal humeral epiphysealepiphyseal cartilage, causing either cartilage, causing either humeral retroversion or proximal humeral humeral retroversion or proximal humeral epiphysiolysisepiphysiolysisover time.over time.
This creates an increase in This creates an increase in ER and a decrease in IR ER and a decrease in IR with maintenance of the with maintenance of the total arctotal arc
**Changes at this age **Changes at this age are BONY**are BONY**
Humeral Head RetroversionHumeral Head RetroversionAs the athlete matures, the As the athlete matures, the physisphysis closescloses
Decreased ability to plastically deform and Decreased ability to plastically deform and remodel through the growth plateremodel through the growth plate
Stress Stress fxfx and acute and acute fxfx can occur (13can occur (13--16 16 y.oy.o. males). males)Increased soft tissue adaptation into HS and collegeIncreased soft tissue adaptation into HS and college
WhiteleyWhiteley et al (JSAMS 6/09) found that less et al (JSAMS 6/09) found that less nonnon--dominant arm retroversion is a dominant arm retroversion is a significant predictor of dominant arm significant predictor of dominant arm throwing injurythrowing injury
Genetic Genetic vsvs acquired versionacquired version
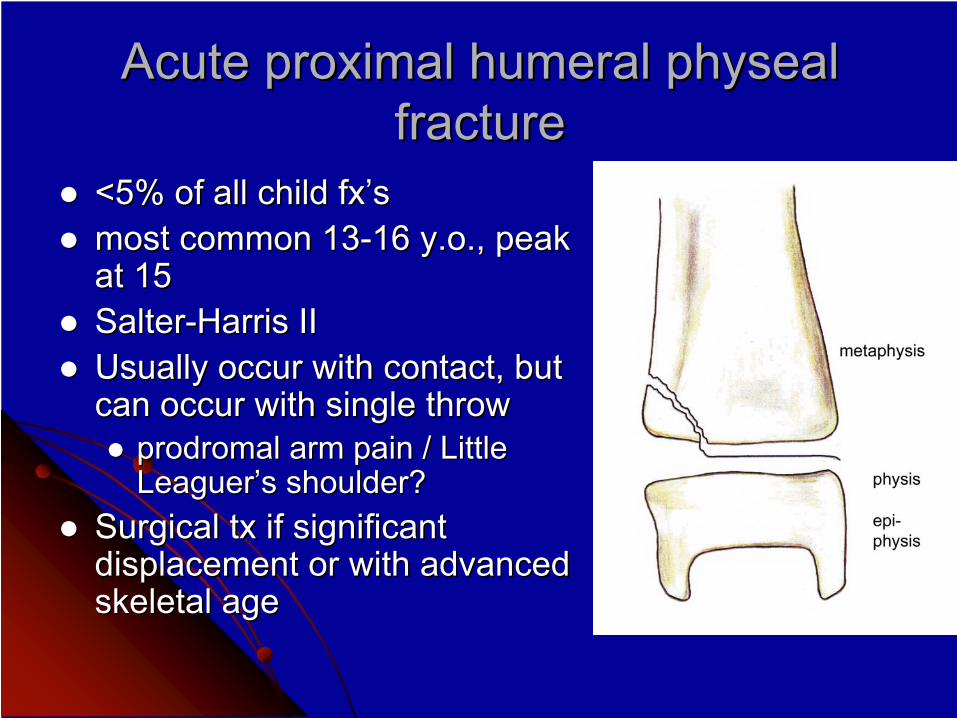
Acute proximal humeral Acute proximal humeral physealphyseal fracturefracture
<5% of all child <5% of all child fx’sfx’smost common 13most common 13--16 16 y.oy.o., peak ., peak at 15at 15SalterSalter--Harris IIHarris IIUsually occur with contact, but Usually occur with contact, but can occur with single throwcan occur with single throw
prodromalprodromal arm pain / Little arm pain / Little Leaguer’s shoulder?Leaguer’s shoulder?
Surgical Surgical txtx if significant if significant displacement or with advanced displacement or with advanced skeletal ageskeletal age
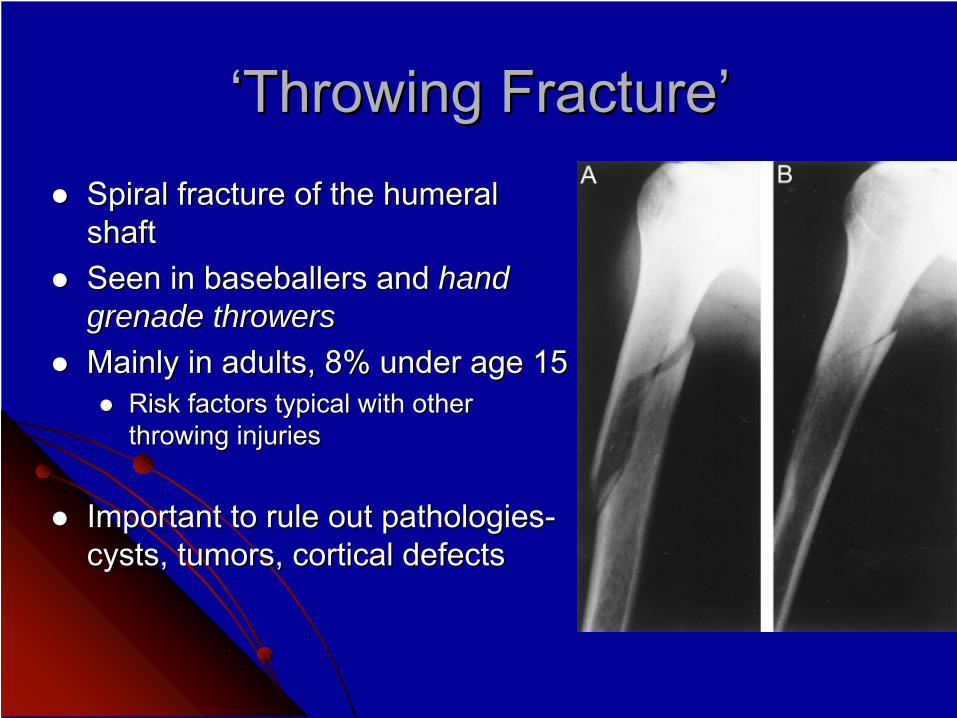
‘‘Throwing Fracture’Throwing Fracture’Spiral fracture of the humeral Spiral fracture of the humeral shaftshaftSeen in Seen in baseballersbaseballers and and hand hand grenade throwersgrenade throwersMainly in adults, 8% under age 15Mainly in adults, 8% under age 15
Risk factors typical with other Risk factors typical with other throwing injuriesthrowing injuries
Important to rule out pathologiesImportant to rule out pathologies--cysts, tumors, cortical defectscysts, tumors, cortical defects
InstabilityInstability
GH GH macroinstabilitymacroinstability uncommon in young uncommon in young throwersthrowers
2.52.5--4.7% of all GH dislocations <12 4.7% of all GH dislocations <12 y.oy.o..AtraumaticAtraumatic MDI more commonMDI more common
generalized generalized ligamentousligamentous laxity in this age laxity in this age group with recurrent group with recurrent microtraumamicrotrauma of throwingof throwing
Pathologic laxity Pathologic laxity vsvs normal generalized normal generalized hypermobilityhypermobility
Compare to other UE => translation and apprehension Compare to other UE => translation and apprehension testingtesting
InstabilityInstability
Signs and symptomsSigns and symptomsPain (max ER Pain (max ER vsvs follow through)follow through)Decreased velocity and/or controlDecreased velocity and/or controlCrepitusCrepitus / / subluxationsubluxation??
adolescents may not ID during throwadolescents may not ID during throw
Pain / weakness with RTC testingPain / weakness with RTC testing+/+/-- impingmentimpingment signssigns+ + SulcusSulcus sign, + load and shift, +/sign, + load and shift, +/-- apprehensionapprehensionNormal xNormal x--raysrays
Rotator Cuff InjuriesRotator Cuff Injuries
Adolescents => tendonitis and strains (<1% Adolescents => tendonitis and strains (<1% of tears)of tears)Rarely primary impingement, more likely Rarely primary impingement, more likely secondary to underlying instabilitysecondary to underlying instability
similar S&S to instabilitysimilar S&S to instabilitypain at or after release, loss of speed/controlpain at or after release, loss of speed/controlpain/weakness with RTC MMTpain/weakness with RTC MMT
OVERUSEOVERUSEexcessive throwing and/or poor preseason excessive throwing and/or poor preseason conditioningconditioning
Rotator Cuff InjuriesRotator Cuff Injuries
External External impingmentimpingment in this group more in this group more d/td/tanatomical variantsanatomical variants-- type III type III acromionacromion, , coracoidcoracoidor CA ligament hypertrophy, or…or CA ligament hypertrophy, or…Os Os AcromialeAcromiale
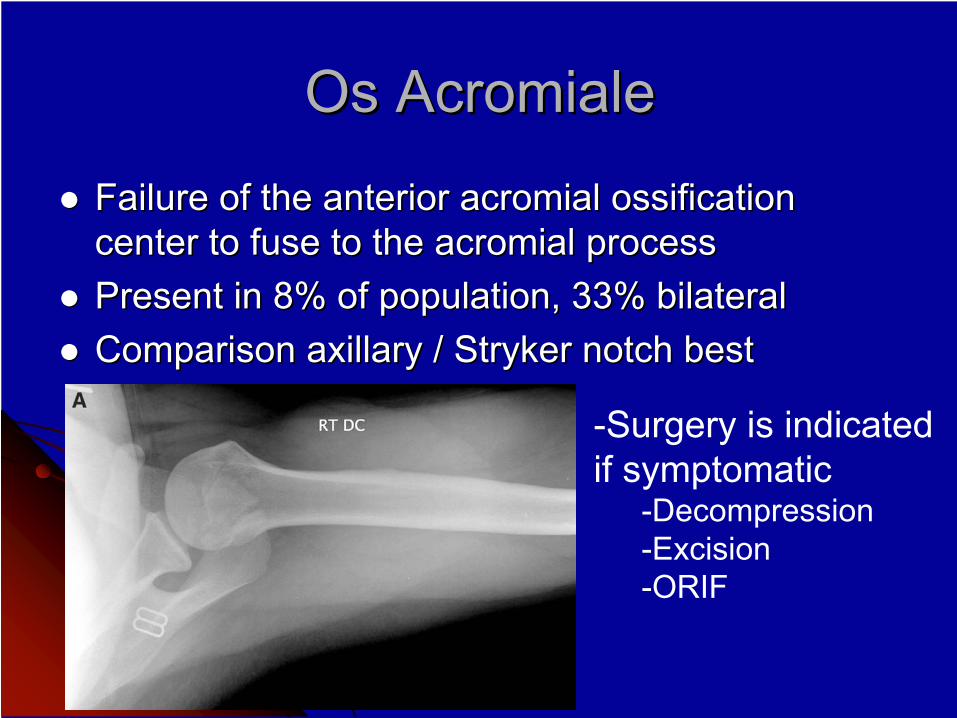
Os Os AcromialeAcromiale
Failure of the anterior Failure of the anterior acromialacromial ossification ossification center to fuse to the center to fuse to the acromialacromial processprocessPresent in 8% of population, 33% bilateralPresent in 8% of population, 33% bilateralComparison Comparison axillaryaxillary / Stryker notch best/ Stryker notch best
-Surgery is indicated if symptomatic
-Decompression-Excision-ORIF
SLAP InjuriesSLAP Injuries
Low SLAP incidence with skeletally immature Low SLAP incidence with skeletally immature throwersthrowers
2009 study2009 study-- 5% of all shoulder injuries in junior high, 5% of all shoulder injuries in junior high, 22% in HS, 26% in college22% in HS, 26% in college
Internal impingement is also rare at this age Internal impingement is also rare at this age Again, ROM changes are Again, ROM changes are d/td/t bony remodeling at the bony remodeling at the proximal humeral proximal humeral physisphysis (Wolff’s Law), not posterior (Wolff’s Law), not posterior soft tissuesoft tissuePosterior Posterior labrallabral fraying and fraying and articulararticular surface partial surface partial RTC tear incidence increases with ageRTC tear incidence increases with age
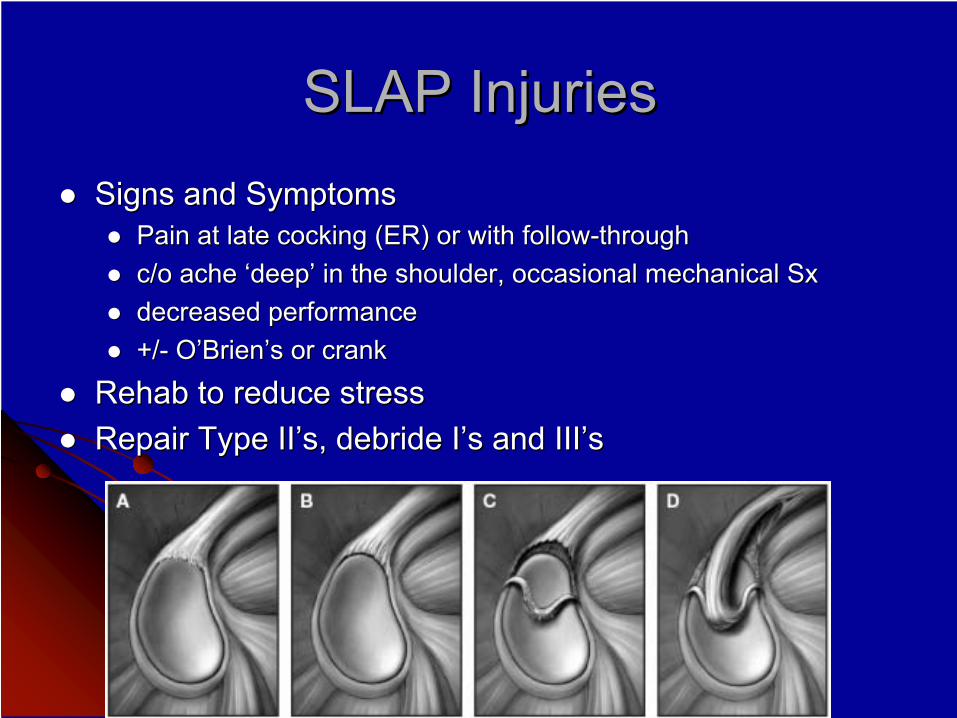
SLAP InjuriesSLAP InjuriesSigns and SymptomsSigns and Symptoms
Pain at late cocking (ER) or with followPain at late cocking (ER) or with follow--throughthroughc/o ache ‘deep’ in the shoulder, occasional mechanical c/o ache ‘deep’ in the shoulder, occasional mechanical SxSxdecreased performancedecreased performance+/+/-- O’Brien’s or crankO’Brien’s or crank
Rehab to reduce stress Rehab to reduce stress Repair Type Repair Type II’sII’s, , debridedebride I’sI’s and and III’sIII’s
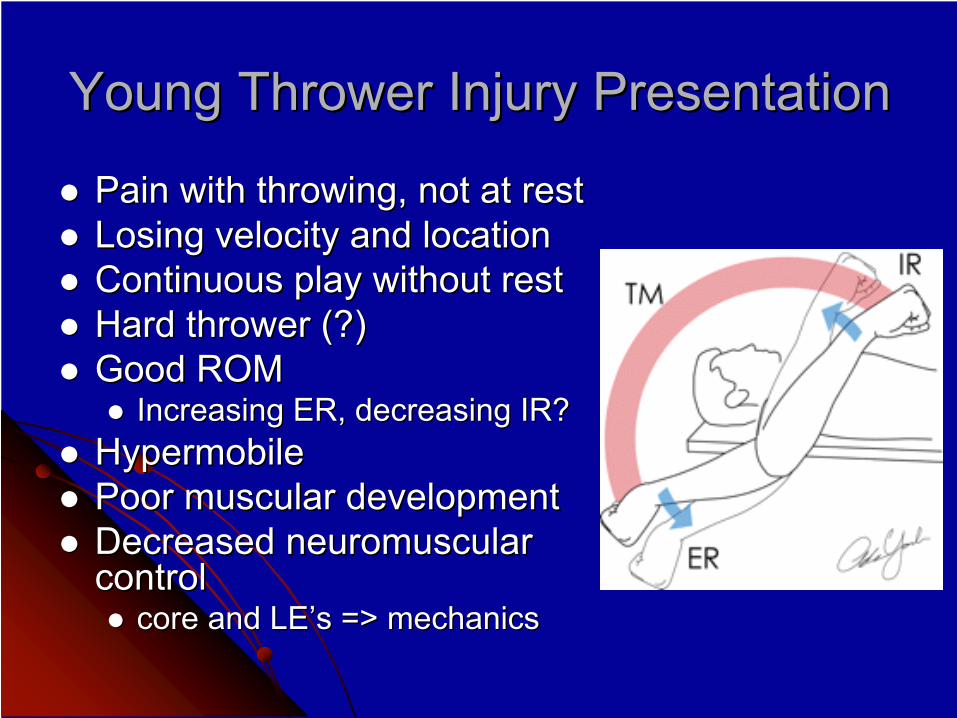
Young Thrower Injury PresentationYoung Thrower Injury Presentation
Pain with throwing, not at restPain with throwing, not at restLosing velocity and locationLosing velocity and locationContinuous play without restContinuous play without restHard thrower (?)Hard thrower (?)Good ROMGood ROM
Increasing ER, decreasing IR?Increasing ER, decreasing IR?HypermobileHypermobilePoor muscular developmentPoor muscular developmentDecreased neuromuscular Decreased neuromuscular controlcontrol
core and core and LE’sLE’s => mechanics=> mechanics
Intrinsic FactorsIntrinsic Factors
AnatomyAnatomy-- humeral head, AC joint, etc.humeral head, AC joint, etc.Skeletal AgeSkeletal AgeMass, size, heightMass, size, heightMuscular strength and developmentMuscular strength and developmentMechanicsMechanics
up to 85% of force is generated before the up to 85% of force is generated before the shouldershoulder
ConditioningConditioning
Ball velocityBall velocity
Extrinsic FactorsExtrinsic FactorsLevel of playLevel of play
moundmound--home distancehome distancegame length, amounts, frequencygame length, amounts, frequency
Sport demandsSport demandspitcher> catcher> IF> OF shoulder complaintspitcher> catcher> IF> OF shoulder complaints
Pitch countsPitch countsPitch type?Pitch type?
52% increased risk of shoulder pain with curveball52% increased risk of shoulder pain with curveballRecent data shows fastballs generally have higher Recent data shows fastballs generally have higher elbow and shoulder force momentselbow and shoulder force moments
RehabilitationRehabilitation
Must address intrinsic and extrinsic factorsMust address intrinsic and extrinsic factorsConsider physiologic ageConsider physiologic ageREST!!!REST!!!
LLS=> no throw for 12 wks (PT for 2LLS=> no throw for 12 wks (PT for 2ndnd 6 wks)6 wks)Post Post fxfx => no throw 6 months post => no throw 6 months post fxfxOthers=> variable and based on Others=> variable and based on SxSx
‘asymptomatic’ and normal RTC function‘asymptomatic’ and normal RTC function
Thrower’s ParadoxThrower’s Paradox-- mobility (excessive mobility (excessive ER), but functionally stable (no symptoms)ER), but functionally stable (no symptoms)
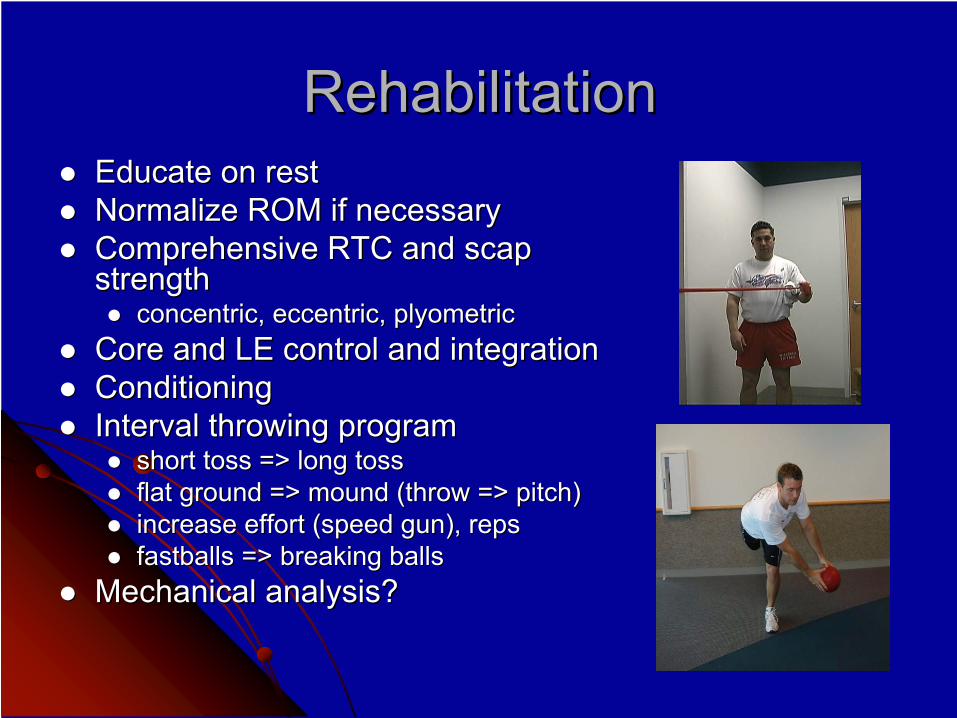
RehabilitationRehabilitationEducate on restEducate on restNormalize ROM if necessaryNormalize ROM if necessaryComprehensive RTC and Comprehensive RTC and scapscapstrengthstrength
concentric, eccentric, concentric, eccentric, plyometricplyometricCore and LE control and integrationCore and LE control and integrationConditioningConditioningInterval throwing programInterval throwing program
short toss => long tossshort toss => long tossflat ground => mound (throw => pitch)flat ground => mound (throw => pitch)increase effort (speed gun), repsincrease effort (speed gun), repsfastballs => breaking ballsfastballs => breaking balls
Mechanical analysis?Mechanical analysis?
PreventionPrevention
Education of players, parents, coaches, Education of players, parents, coaches, trainers, MD’s, etc.trainers, MD’s, etc.
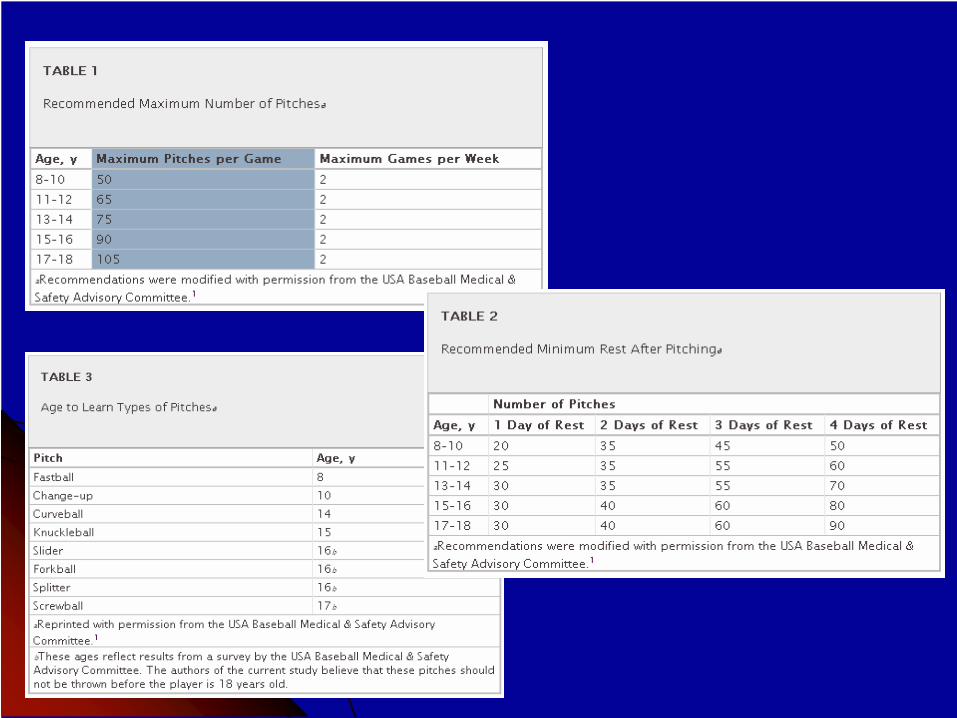
Pitch count and type Pitch count and type OffOff--season conditioningseason conditioningInterval throwingInterval throwing
ID hard throwersID hard throwersID mechanical flawsID mechanical flaws
ReferencesReferences1.1.
Taylor DC, Taylor DC, KrasinskiKrasinski
KL. Adolescent Shoulder Injuries: Consensus and Controversies. KL. Adolescent Shoulder Injuries: Consensus and Controversies. JBJS. 2009; 91:462JBJS. 2009; 91:462--
473.473.2.2.
WasserlaufWasserlauf
BL, BL, PalettaPaletta
GA. Shoulder Disorders in the Skeletally Immature Throwing AthlGA. Shoulder Disorders in the Skeletally Immature Throwing Athlete. ete. OrthopOrthop
ClinClin
N N Am. 2003; 34:427Am. 2003; 34:427--437.437.
3.3.
Parks ED, Ray TR. Prevention of Overuse Injuries in Young BasebaParks ED, Ray TR. Prevention of Overuse Injuries in Young Baseball Pitchers. Sports Health. 2009; Dec:514ll Pitchers. Sports Health. 2009; Dec:514--
517.517.4.4.
Meister K, Day T, Meister K, Day T, HorodyskiHorodyski
M, Kaminski TW, M, Kaminski TW, WasikWasik
MP, Tillman S. Rotational Motion Changes in the MP, Tillman S. Rotational Motion Changes in the GlenohumeralGlenohumeral
Joint of the Adolescent/Little League Baseball Player. AJSM. 20Joint of the Adolescent/Little League Baseball Player. AJSM. 2005;33:69305;33:693--698.698.5.5.
Dotter WE. Little Leaguer’s Shoulder: A Fracture of the ProximalDotter WE. Little Leaguer’s Shoulder: A Fracture of the Proximal
EpiphysealEpiphyseal
Cartilage of the Cartilage of the HumerusHumerus
due to due to Baseball Pitching. Guthrie Baseball Pitching. Guthrie ClinClin
Bull.1953; 23:68Bull.1953; 23:68--72.72.6.6.
WhiteleyWhiteley
RJ, Adams RD, Nicholson LL, RJ, Adams RD, Nicholson LL, GinnGinn
KA. Reduced Humeral Torsion Predicts ThrowingKA. Reduced Humeral Torsion Predicts Throwing--Related Injury Related Injury in Adolescent in Adolescent BaseballersBaseballers. J . J SciSci
Med Sport. 2009.06.001.Med Sport. 2009.06.001.7.7.
Lyman S, Lyman S, FleisigFleisig
GS, GS, WaterborWaterbor
JW, JW, FunkhouserFunkhouser
EM, Pulley L, Andrews JR, EM, Pulley L, Andrews JR, OsinskiOsinski
D, D, RosemanRoseman
JM. JM. Longitudinal Study of Elbow and Shoulder Pain in Youth Baseball Longitudinal Study of Elbow and Shoulder Pain in Youth Baseball Pitchers. Med Pitchers. Med SciSci
Sport Sport ExercExerc. . 2001;33:18032001;33:1803--1810.1810.
8.8.
Carson Carson JrJr
WG, Gasser SJ. Little Leaguer’s Shoulder: A Report of 23 Cases.WG, Gasser SJ. Little Leaguer’s Shoulder: A Report of 23 Cases.
AJSM. 1998;26:575AJSM. 1998;26:575--580.580.9.9.
Mueller F, Marshall, S. Epidemiologic Study of Pitching InjuriesMueller F, Marshall, S. Epidemiologic Study of Pitching Injuries
in Baseball. in Baseball. In Progress. In Progress. 2009. 2009. www.uncbaseballstudy.comwww.uncbaseballstudy.com..
10.10.
SciasciaSciascia
A, A, KiblerKibler
WB. The Pediatric Overhead Athlete: What is the Real Problem? WB. The Pediatric Overhead Athlete: What is the Real Problem? ClinClin
J Sport Med. J Sport Med. 2006;16:4712006;16:471--477.477.
11.11.
NissenNissen
CW, CW, WestwellWestwell
M, M, OunpuuOunpuu
S, Patel M, S, Patel M, SolomitoSolomito
M, Tate J. A Biomechanical comparison of the fastball M, Tate J. A Biomechanical comparison of the fastball and curveball in adolescent baseball pitchers. Am J Sport Med. 2and curveball in adolescent baseball pitchers. Am J Sport Med. 2009;37:1492009;37:1492--1498.1498.
12.12.
Lyman S, Lyman S, FleisigFleisig
GS. Baseball Injuries. Med Sport GS. Baseball Injuries. Med Sport SciSci. 2005; 49:9. 2005; 49:9--30.30.13.13.
Lyman S, Lyman S, FleisigFleisig
GS, Andrews JR, GS, Andrews JR, OsinskiOsinski
ED. Effect of pitch type, pitch count, and pitching mechanics oED. Effect of pitch type, pitch count, and pitching mechanics on n risk of elbow and shoulder pain in youth baseball pitchers. Am Jrisk of elbow and shoulder pain in youth baseball pitchers. Am J
Sports Med. 2002 JulSports Med. 2002 Jul--Aug;30(4):463Aug;30(4):463--8. 8. 14.14.
Andrews JR, Andrews JR, WilkWilk
KE. ASMI 27KE. ASMI 27thth
Annual Injuries in Baseball Course. Course Handout. 2009.Annual Injuries in Baseball Course. Course Handout. 2009.