Embed Size (px)
Citation preview

Session Title
Presenter namePresenter email
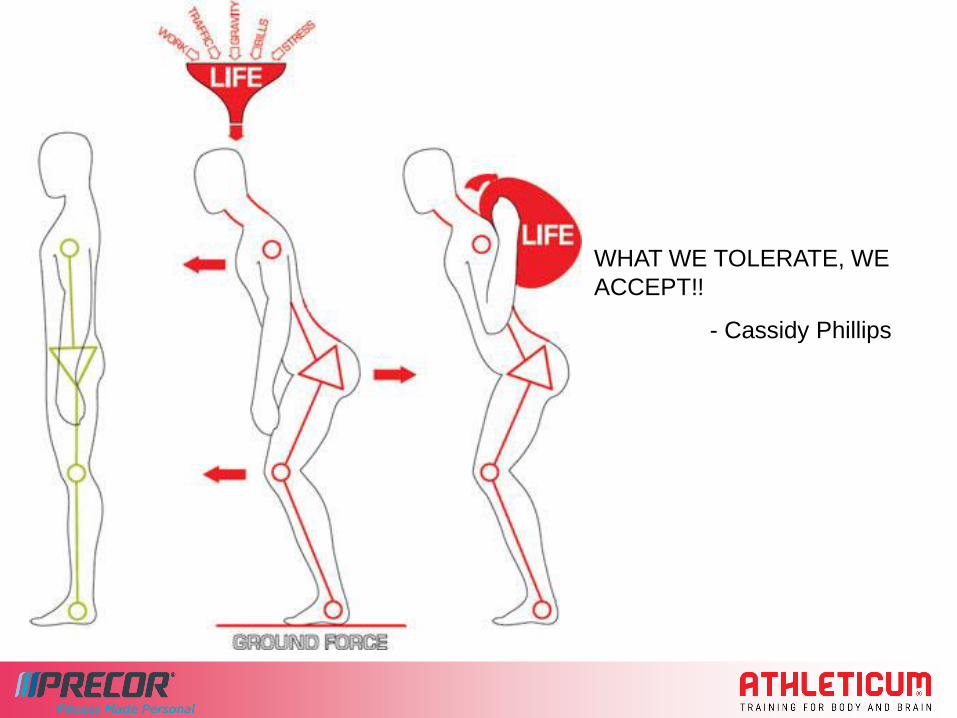
WHAT WE TOLERATE, WE
ACCEPT!!
- Cassidy Phillips
Some other factors that cause Triggerpoints..
Overuse - extrinsic factors.
Training errors
Inadequate preparation
Inadequate massage for sore and tired muscles
Overhard or soft surfaces
Inappropriate shoes/equipment;
Environmental conditions
Overuse- Intrinsic factors..
Poor biomechanics
Muscle fatigue
Muscle weakness
Joint instability/hypermobility
Lack of muscle flexibility.
The Physiology of Tightness
Joint ROM can be limited by the following factors (Hutton, 1992):
1. Joint constraints
2. Subcutaneous connective tissue.
3. Neurogenic constraints (voluntary and reflexive)
4. Myogenic constraints
Can you explain the word ‘Tight’?
Muscle Fibres (myogenic effect)
Can stretch to at least 50% greater length than when at rest (last cross bridges intact).
Magnesium deficiency can cause tightness (cramping) as magnesium facilitates actin-myosin release.
Muscle Spindles (neurogenic effect)
•Primary stretch receptors in the muscles.
•reflexive capabilities via alpha-motoneuron (the alpha-motoneuron is responsible for initiating muscular contraction)
•Strong phasic contraction upon detection of stretch, followed by controlled tonic contraction.
•Regular stretching may decrease sensitivity of muscle spindles
•This may explain acute performance decreases post-passive stretch

Fascia
Composed of collagen and elastin, providing tensile and elastic properties.
Continuous structure that surrounds and integrates tissues and structures
Can affect relationship amongst structures
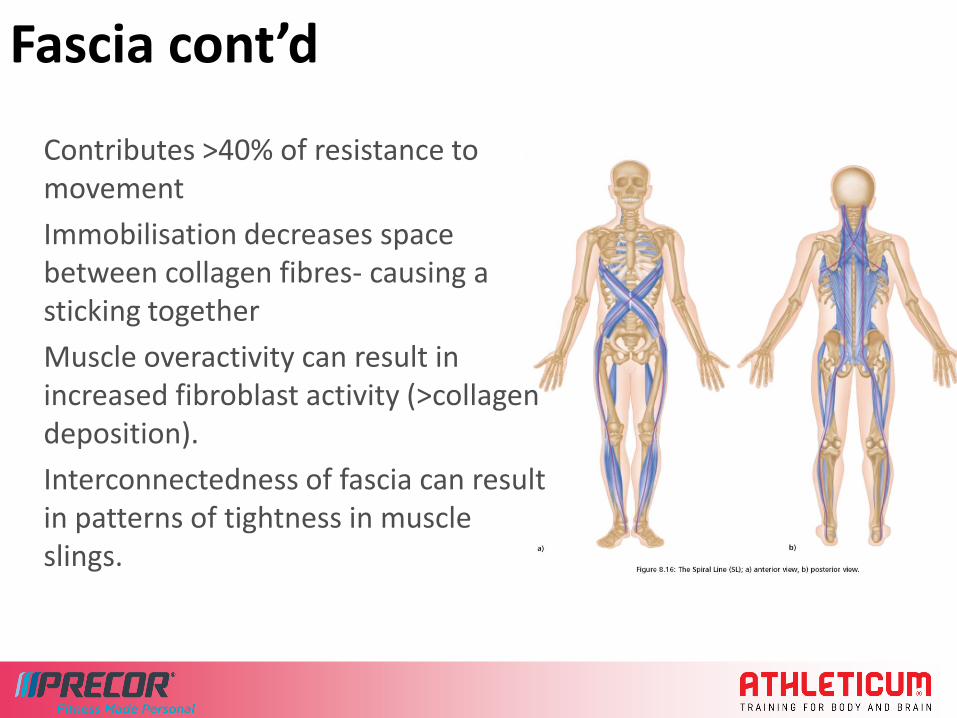
Fascia cont’d
Contributes >40% of resistance to movement
Immobilisation decreases space between collagen fibres- causing a sticking together
Muscle overactivity can result in increased fibroblast activity (>collagen deposition).
Interconnectedness of fascia can result in patterns of tightness in muscle slings.
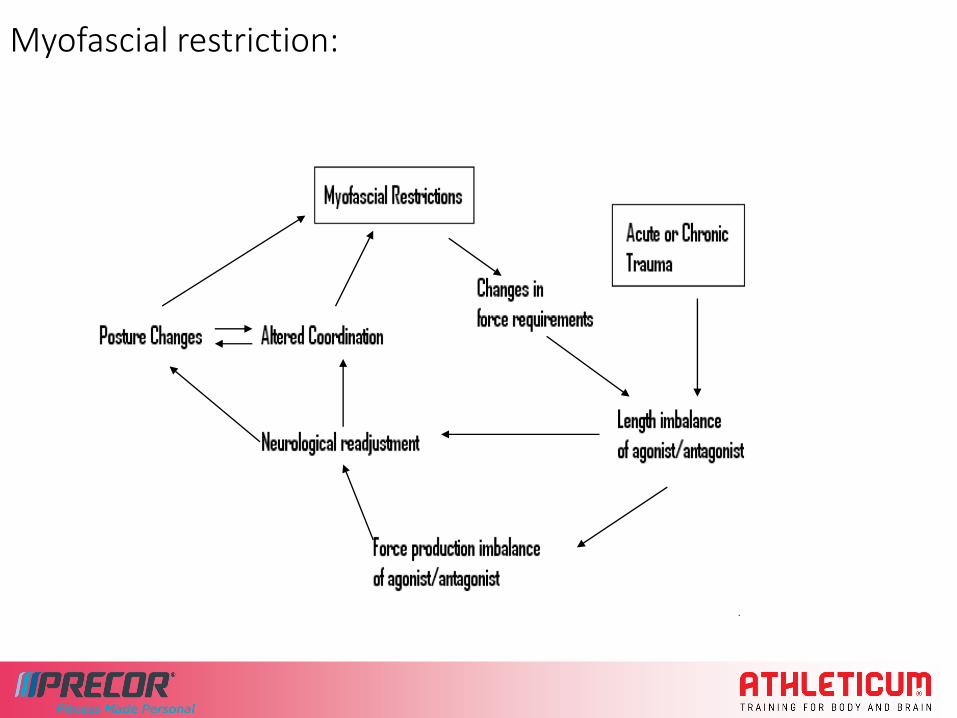
Myofascial restriction:

Trigger points
Discrete, focal, hyperirritable spot in taut band of muscle
Occurring in all patients with musculoskeletal pain
Can be active or latent
Symptoms:
Painful on compression
Referred pain/tenderness
Motor dysfunction
No evidence for development mechanism of Trigger Points
Acute and chronic trauma, chronic lengthening, sleep disturbance, anxiety

Some common Triggerpoints(Back)
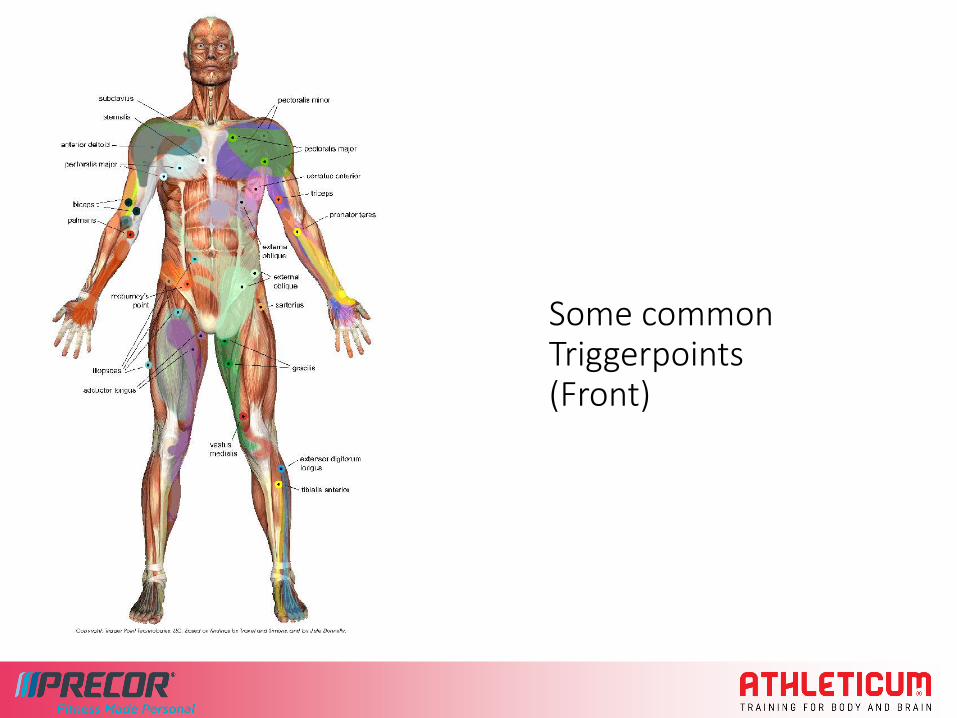
Some common Triggerpoints(Front)
Myofascial release – the alternative
Similar to massage
Uses palpation, pressure and tissue stretch to relieve tension and improve:
Muscle tone,
Length,
Timing,
Strength,
Endurance,
Control
Can be used on various soft tissue abnormalities:
Local increased muscle tone
Trigger points
Muscle shortness
Fascial tightness
Deficits in motor activity or control
Can result in pro-inflammatory effect and decreased fibroblast activity and collagen production (short-term)

Myofascial release- cont’d
• It is an important tool helping the body correct imbalances throughout the myofascial system.
• Applying gentle force to the adhesion; the elastic collagenous fibers are manipulated from the bundled position into an alignment that is straighter with the direction of the muscle and /or fascia. (Theory!)
• The gentle pressure applied with the roller will assist in releasing the tension by stimulating the GTO
Exercise and myofascial release
Exercise is vital for myofascial release treatment
Resets neurological programming (Theory)
Both needed for permanent change

Self Myo-Fascial and Trigger Point Release
Interactive soft tissue release requiring feedback from patient to determine correct position, amount of pressure and duration of stretch
Uses body weight on tool i.e. foam roller or tennis ball
Penetrates into muscle and or fascia
Easy and effective
Releases tightness and trigger points
Can be painful
Research to prove efficacy is poor and inherently
difficult to achieve.
Practical programming
Warm up:Self-myofascial release/ joint capsule workActivation exercisesDynamic warm up with progressive loading
(jog, add speed and direction change, dynamic stretch, agility, skill)
Cool DownDecrease metabolic load for waste product clearanceSlow dynamic stretching movementsSMFRStatic stretching later
Look at what is short/tight and facilitated (assess!!)
Address Right/left and front/back imbalances
Consider performance effect of chosen modality
So, how does it work?
Traditionally, we thought…
Rolf believed that applying manual pressure to fascia can change its density and arrangement, making it less dense and therefore more fluid. (Thixotrophy)
The Piezoelectric model (Schleip or Juhan)
‘Fuzz’ – Gil Hedley
But..
These two models appear to be effective over the long-term not short-term.
A modern approach..
The Golgi reflex arc…
GTO- Ruffini and Pacini Corpuscles
Motor unit not fibre activation??
DNIC (Diffuse Noxious Inhibitory Controls)
Important things to remember
• Cue the client to breathe & relax when a tender point is found.
• Muscles are three dimensional, don’t roll in one plane/direction!
• If unsure about the clients imbalances REFER them to a Professional!
FAQ…
• Which direction do I go?
• How long do I hold?
• I feel referral to other parts of my body, is this normal?
• I don’t feel anything, is this possible?
• Do I really need to do this?
• Which parts of the body can I use it on?

THANK YOU!
Enjoy the rest of your SPINNING® SHOWCASE 2017