Embed Size (px)
Citation preview
Teaching Prevention in the Flipped Classroom
Jim Medder, MD, MPH
I have no relevant
financial relationships with
any ‘commercial interests’.
At the conclusion of this presentation, the participants should be able to:
• List basic components and rationale for the theory of the flipped classroom model of instruction.
• Develop initial plans for flipped classroom instruction for preventive medicine presentations at their institution.
• List the pros and cons of using the flipped classroom model, especially within the framework of the traditional curriculum, and potential solutions to barriers.

Outline
Why I did it…
What I did…
Student feedback…
What do you think I should do?
What the literature says…

How many of you have “flipped”?

Why flip?
(The next best thing?)
Lecture shortcomings New technologies New generation of learners/different styles

How long does it take in the average 50 minute lecture…until you see this?

Bunce DM, Flens EA, Neiles KY. How long can students pay attention in class? A study of student attention decline using clickers. Journal of Chemical Education. 2010;87:1438-1443.
15-20 minutes?
“Instead, across all three courses, they observed a pattern in which the first “spike” in reported attention lapses occurred just 30 seconds into a lecture segment, reflecting the “settling-in” period; the next spike occurred at 4.5 to 5.5 minutes into the lecture; the next at 7 to 9 minutes; and the next at 9 to 10 minutes in.
This waxing-and-waning pattern continued throughout the lecture, with attention lapses occurring more frequently as the lecture progressed. By the end of the lecture, lapses occurred about every two minutes.”

What you want to see…

What we’ve been seeing… Where are the students?


Multi-tasking generation


It begins early…

Today’s (Millennial) learners prefer/want: • Group projects
• Immediate feedback
• Learning in their own time frame
• Innovative learning environments
• Interactive and engaging; learn through discovery
• Personal encouragement and feedback from
teachers
• Emphasis on self-motivation and responsibility
• Learning from friends and teaching friends within
context of multiple social media platforms

So what did we do?

UNMC Fall Semester M2 Year
Introduction to Disease Processes Core
(AM)
Cardiology/Endocrine Pulmonary/ENT Core
(AM)
Pharmacology Pharmacology
Integrated Clinical Experience (ICE) Core
(2 afternoons/week)

PM/PH Curriculum (M2 ICE)
• Fall Lectures:
• Introduction to Prevention/Public Health
• Clinical Preventive Medicine
• Douglas County Health Department
• COPC
• Immunizations
• Motivational Interviewing
• Tobacco Cessation
• Nutrition
• Pediatric HCM
• Small Groups:
• Adult H&P/HCM (2)
Spring:
• Epidemiology/Biostatistics Lectures/Small Groups
• Sensitivity/Specificity/Predictive Value

Two years’ experience… • In 2013, lectures on population/public health and
clinical preventive services were changed from two fifty-minute PowerPoint lectures into two asynchronous online sessions using the flipped classroom model.
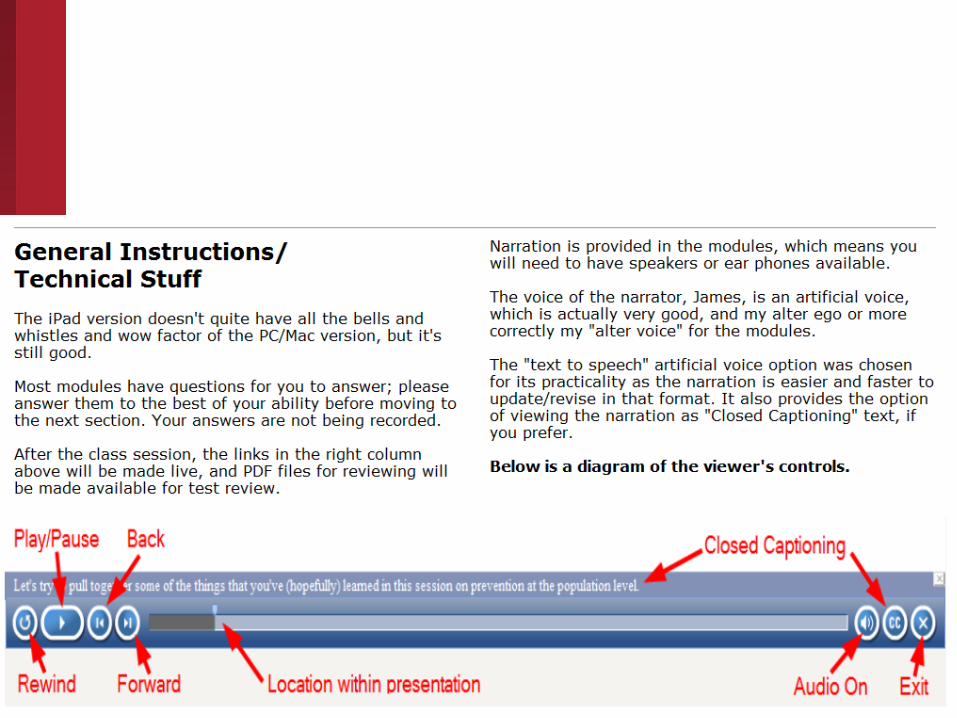
• Each lecture was divided into 4-5 short modules (total 20-25 minutes/session) by using Adobe Captivate software with its multimedia capabilities, closed captioning, and narration by artificial voices. (Captivate can directly import PowerPoint slides.)
• Students were instructed to review the “mini lectures” prior to class and to complete an assignment for each session.

Two years’ experience… • The first assignment was a community
action/implementation project on decreasing the rate of Chlamydia infections, a major STI in the local community.
• For the second session students were given a written patient case and had to determine what preventive services should be provided.
• The original class lecture time slots were modified to become Q&A or review sessions to discuss the online content/concepts and to review the online assignments that were designed for students to apply concepts learned in the modules.
• Also, a post-test of prevention terms/definitions was included to determine if students understood those concepts.




LINKS:
Population-Based Prevention
http://app1.unmc.edu/prevent/m2icepp/
Clinical Prevention
http://app1.unmc.edu/prevent/m2icecp/
Sometimes it can be painful to be an early adopter…
• My personal observations/feelings after the two sessions:
• Some students did not like listening to an artificial voice (fewer this year than last).
• While student participation and discussion in the first class session (Chlamydia) were very good, discussion in the second session (health care maintenance) was less spontaneous and more difficult to elicit. (I actually thought it would be the opposite)
• From the quality of discussion and review of the post-test, it appeared that many students had not even reviewed the online material for the second session.

Focus Group Feedback (from the course director)
• They felt unprepared for a flipped classroom model, as they had never experienced this before (which surprised me—I thought they did some of this in the M1 year).
• They felt that the classroom session associated with the first online module was very laid back, and that you spent more time completing it with them in class. That is why no one was well prepared for the second lecture, as they thought that they would go over it more in class together.
• They still do not love the electronic voice on the modules.

• They would like to see the online portion more interactive—questions scattered throughout, that they have to answer.
• Some commented that the modules were too long, but this was not a big complaint.
• The overriding comments about the flipped model in general, is that if the entire core goes to a flipped model, it makes it easier, rather than some lecturers doing it that way, and some lecturers not. Because then they are having to prepare for the next person and review all at the same time.
Focus Group Feedback (from the course director)

So, based on that feedback, what would you recommend?
Traditional classroom • Classroom lecture
• Followed by small group sessions or homework assignments (sometimes)
• Self study/review before test
Flipping the classroom: Content attainment phase “In this model, which uses the leverage of computer technology, students acquire basic knowledge and facts about a subject through a series of short videos hosted online. Young learners watch these videos on their own schedule and as many times as necessary to master the content. Students demonstrate mastery by providing a consecutive series of correct responses to a number of embedded questions.”
Flipping the classroom: Concept application phase “In subsequent classroom sessions,
students engage with their teacher in problem-
solving exercises.
There is a “flipping of the classroom”: Lessons
previously taught in class are learned at home, and
“homework” is performed in the classroom in
collaboration with peers and guided by teachers.
The pace of learning is guided by the individual
student, and the relevance of the material is
underscored through in-class problem solving.”

Short online videos… • 10 minutes
• Peak learning periods for adults
• Easily archived
• Easily searched
• Core content, scientifically validated (lower order cognitive skills)
• Easily updated with new knowledge
• Same material in different formats (meet different learning styles):
• Powerpoint (but not just videotaped lectures)
• Embedded quizzes
• Ability to alter speed of presentation
• Ability to view speaker/instructor

Dynamic interactive sessions • Apply knowledge with meaningful exercises with
peers and faculty
• Case-, problem-, and team-based learning exercises
• Simulations
• Patient encounters
• Role-playing
• Debates
• Videos/movie clips
• Multiple faculty with different expertise
• Faculty:Student ratio of 4:1 to 25:1 (face-to-face time with faculty; interact with colleagues/peers)

Deep dives • In-depth experiences fueled by students’ specific
learning objectives and passions
• Similar to scholarly/advanced tracks available at some medical schools


Flipped classroom negatives • Additional time and work to change lecture into
new format (not just adding narration to a PowerPoint presentation)
• Students must be self-motivated and take responsibility for their education
• Tendency to provide excessive content (ideally, time should be same or less than the time used previously for lecture and post-lecture homework in traditional classroom)
• Ideally provide more than one modality (besides video) to learn the material

Evidence for/against the flipped classroom model • Minimal/limited studies
• Mixed results with many compound variables

So what am I going to do? • Make sure the students have been formally
oriented to the process and philosophy of the flipped classroom (or remind them).
• Integrate summative quizzes into online modules.
• Shorten the modules (content)?
• Current modules are 5-7 minutes long (below 10 minute recommendation).
• For first in-class PH session (Chlamydia):
• Take current COPC lecture and use COPC as model;
• Introduce COPC and work through project in class;
• Co-facilitate with other COPH faculty and DCHD director.
So what am I going to do? • Second in-class CPM session (USPSTF/HCM):
• Drop; already have two small group sessions, which are ideal for follow-up and application of content (12 small groups with 12 different expert facilitators)
• Keep the artificial voice:
• It’s really pretty good.
• Makes editing really easy and students have option to review with closed captioning if they do not want to listen to voice.

Why flip?
(The next best thing?)

Captivate screen shot

Captivate screen shots
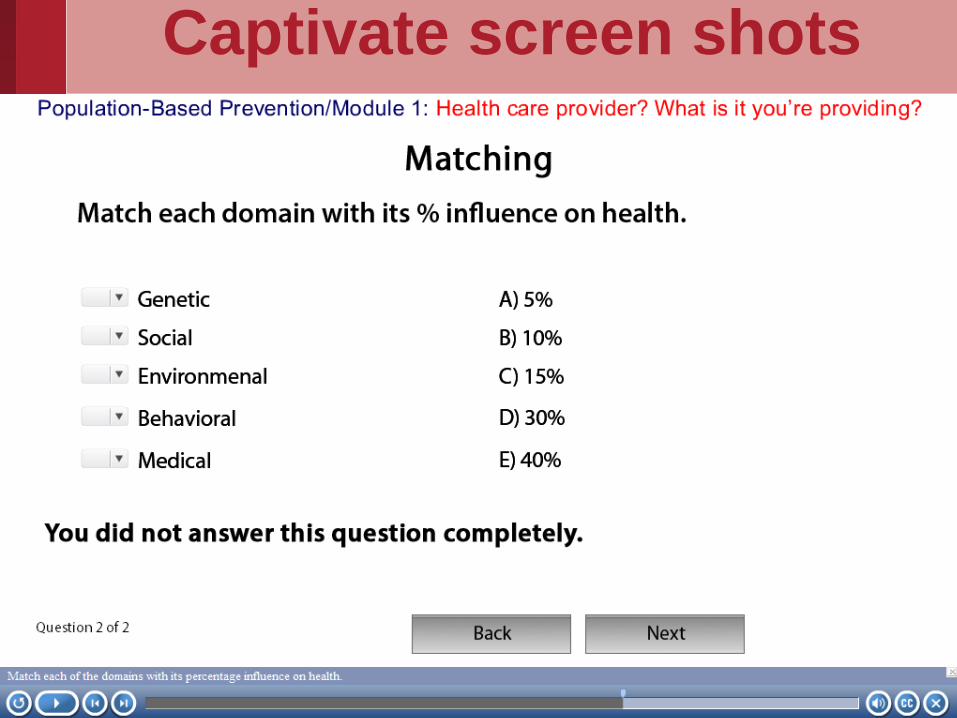
Captivate screen shots

Captivate screen shots

References
• Bunce DM, Flens EA, Neiles KY. How long can students pay attention in class? A study of student attention decline using clickers. Journal of Chemical Education. 2010;87:1438-1443.
• Jensen JL, Kummer TA, Gody PDM. Improvements from a flipped classroom may simply be the fruits of active learning. Life Sciences Education. 2015;14:1-12.
• Moffett J. Twelve tips for “flipping” the classroom. Medical Teacher. 2014;1-6.
• Prober CG, Heath C. Lecture halls without lectures-A proposal for medical education. The New England Journal of Medicine. May 3, 2012;366(18):1657-1659.
• Prober CG, Khan S. Medical education reimagined: A call to action. Academic Medicine. 2013;88:1407-1410.
• Simpson V, Richards E. Flipping the classroom to teach population health: Increasing the relevance. Nurse Education in Practice 2014:1-6 (In Press).




















![Cleaning Validation (2010[1].03.17) [호환 모드]](https://img.pdfslide.us/doc/110x75/61c459d34325ab4c8c1a09d5/cleaning-validation-201010317-.jpg)





![Sam jae portfolio [03.17].compressed](https://img.pdfslide.us/doc/110x75/58cf02131a28abab738b6947/sam-jae-portfolio-0317compressed.jpg)