Embed Size (px)
Citation preview

Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
Steven Q Simpson, MD, FCCP, FACP
Professor of Medicine
Division of Pulmonary and Critical Care
University of Kansas

Disclosures
No commercial interests to disclose
Founder of Midwest Critical Care
Collaborative
Founder of the Kansas Sepsis Project
Participant 2016 update, Surviving Sepsis
Campaign Guidelines
Dissenting opinion on Sepsis-3 in CHEST

Kansas: Exemplar of Rural America

Objectives
1. Discuss definitions of sepsis and what they
mean
2. Discuss the role of Early Goal Directed
Therapy in sepsis
3. Discuss CMS measures and their role in
improving sepsis care

21st Century Sepsis Teaching?
“as the physicians say it happens in hectic fever,
that in the beginning of the malady it is easy to
cure but difficult to detect, but in the course of
time, not having been either detected or treated in
the beginning, it becomes easy to detect but
difficult to cure”
Niccolò Machiavelli
The Prince – 1513 or 1532

What is Sepsis?
Life threatening organ dysfunction due
to a dysregulated host response to
infection

What is Sepsis?
Life threatening organ dysfunction due
to a dysregulated host response to
infection

Hospital Case
•72 y.o. man, 3 days post-op from ureteral stent
placement; Foley in place
• Nurse finds him with flank pain and fever,
mild confusion (previously oriented x 4)
•Hx of CAD, HTN
•Meds include terazosin, atorvastatin,
metoprolol
•BP 105/43, P 117, R 21, T 39.1o , SpO2 87%
•Exam: left CVA tenderness, BPH

ACCP/SCCM Consensus Definitions
• Infection - Inflammatory response to
microorganisms, or
- Invasion of normally sterile
tissues
• Systemic Inflammatory
Response Syndrome
(SIRS)
- Systemic response to a variety of
processes
- 2 or more SIRS criteria
•Sepsis – Infection plus
2 or more SIRS criteria
• Severe Sepsis – Sepsis
– Organ dysfunction
• Septic shock – Sepsis
– Hypotension despite fluid
resuscitation
Bone RC et al. Chest. 1992;101:1644-55.

SIRS:
Systemic Inflammatory Response Syndrome
• SIRS: nonspecific insult
≥ 2 of the following:
– Temperature
> 38o C or < 36o C
– HR > 90 beats/min
– Respirations > 20/min
– WBC > 12,000/µL,
< 4,000/µL, or >10%
immature neutrophils (bands)
Adapted from: Bone RC et al. Chest. 1992;101:1644-55.
Opal SM et al. Crit Care Med. 2000;28:S81-2.
SIRS

Acute Organ Dysfunction as the Hallmark of
Severe Sepsis
Hypotension SBP < 90 MAP < 65
Oliguria - < 20 mL/hr Anuria
Creatinine △ (>0.5 mg/dL)
↓Platelets (< 100k) ↑(INR>1.5, PTT>60 sec)
↑ D-dimer
Altered Consciousness
Confusion Psychosis
Tachypnea PaO2 <70 mm Hg
SaO2 <90% PaO2/FiO2 < 300
T. Bilirubin > 4 mg/dL
Lactic acidosis

Sepsis: What Are We Talking About?
Roger C. Bone, MD
•ICD-9: “septicemia”
•Positive blood cultures
•Multiple positive blood
cultures
•Positive blood cultures +
hypotension
•Syndrome: how shall we
define it?


The Third International Consensus Definitions
for Sepsis and Septic Shock (Sepsis-3)
Definition:
Sepsis is life threatening organ dysfunction
caused by a dysregulated host response to
infection
Drops the term “severe sepsis”
Drops the use of SIRS and infection + SIRS

Condition Sepsis-2 Sepsis-3
Sepsis Infection + SIRS Infection + ∆ SOFA ≥ 2
Severe Sepsis Infection + SIRS + organ dysfunction
NON-EXISTENT
Septic Shock Infection + Unresponsive Hypotension*
Infection + Unresponsive Hypotension* + Serum Lactate > 2 mmol/L
The Third International Consensus Definitions
for Sepsis and Septic Shock (Sepsis-3)
*Hypotension that does not respond to volume infusion and requires vasopressor administration

SOFA Score 1 2 3 4
Respiration PaO2/FiO2
< 400 < 300 < 200
With respiratory support
< 100 with respiratory
support
Cardiovascular Hypotension
MAP < 70 mm Hg
Dopamine ≤ 5 or dobutamine, any
dose
Dopamine > 5 or epinephrine or norepinephrine
≤ 0.1
Dopamine > 15 or epinephrine
or norepinephrine
> 0.1
Liver Bilirubin (mg/dL) 1.2 – 1.9 2.0 – 5.9 6.0 – 11.9 > 12.0
Renal Creatinine (mg/dL) or urine output
1.2 – 1.9 2.0 – 3.4 3.5 – 4.9 or
< 500 mL/24 hr ≥ 5.0 or
< 200 mL/24 hr
Coagulation Platelets x 103/mm3 < 150 < 100 < 50 < 25
CNS Glasgow Coma Scale 13 - 14 10 - 12 6 - 9 < 6


Quick SOFA
• Also known as qSOFA
• Any two of:
- Glasgow Coma Scale < 15
- Respiratory rate ≥ 22/min
- Systolic blood pressure ≤ 100 mm Hg

ROC Results

ROC Curves & Diagnostic
Accuracy Excellent
Fair-Good Worthless
1 – specificity (False Positive Rate)
Sen
siti
vity
(Tr
ue
Posi
tive
Rat
e)
This is NOT the probability of the OUTCOME, if the TEST is positive. It is the probability that the TEST is positive in someone who had
the OUTCOME and negative in someone without it.
i.e.
This is NOT the probability of death if qSOFA or SIRS is positive. It is the probability that qSOFA or SIRS was present in those who
died and not present in those who survived.

“SIRS is too non-specific”
“I make love to my wife and I get SIRS”
“Hopefully, more than once!”
Jean-Louis Vincent

Bayes’ Theorem
P(D|T) = P(T|D)P(D)
P(T|D)P(D) + P(T|D’)P(D’)
Psepsis | SIRS ≅ PSIRS | sepsis x Psepsis in group

Bayes’ Theorem
Psepsis | SIRS ≅ PSIRS | sepsis x Psepsis in group
PSIRS

Likelihood Ratio / Fagan Nomogram “The essence of the Bayesian approach is to provide a mathematical rule explaining
how you should change your existing beliefs in the light of new evidence.”
Post-test probability of a disease is dependent on:
1. the pre-test probability of disease
2. characteristics of the test (likelihood ratio)
LR + = sensitivity / (1 – specificity)
LR - = (1 – sensitivity) / specificity
Treatment threshold
Test threshold
Fagan TJ. N Engl J Med 1975;293:257.

Criticizing SIRS for being too
sensitive a test to diagnose sepsis
in all comers is like criticizing a
hammer for being the only tool in
your toolbox.

SIRS Infection Suspect
SEPSIS

qSOFA Infection Suspect
SEPSIS

Infection Syndromes
Pneumonia – cough, purulent sputum, pleuritic chest
pain, consolidation
Cellulitis – redness, tenderness, advancing margin
Pyelonephritis – flank pain, costophrenic angle
tenderness, urinary leukocytosis
Peritonitis – abdominal pain, ileus, rebound
tenderness, rigidity
Possible BSI from indwelling catheter

Hospital Case
•72 y.o. man, 3 days post-op from ureteral stent
placement; Foley in place
• Nurse finds him with flank pain and fever,
mild confusion (previously oriented x 4)
•Hx of CAD, HTN
•Meds include terazosin, atorvastatin,
metoprolol
•BP 105/43, P 117, R 21, T 39.1o , SpO2 87%
•Exam: left CVA tenderness, BPH

Early Goal Directed Therapy
Wanted Dead or Alive?

Rivers E, et al. N Engl J Med 345:1368 – 1377, 2001.
• Primary Endpoint: In hospital mortality; single center
• Secondary Endpoints:
- Resuscitation endpoints
- Organ dysfunctions
- Coagulation endpoints
- Healthcare resources

EGDT
NEJM 345:1368 – 77, 2001.
Lactate
> 4 mmol/L
or
Septic Shock

EGDT Initial Results
Rivers E, et al. N Engl J Med 345:1368 – 1377, 2001.

EGDT
NEJM 345:1368 – 77, 2001.


ARISE
ProCESS ProCESS
ARISE
ProMISE


HOWEVER – I2 = 57%
SUBSTANTIAL HETEROGENEITY

Cut and Dried?

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if hypotensive > 29 mL/kg > 30 mL/kg
> 1.95 L in 2.5
hours

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if hypotensive > 29 mL/kg > 30 mL/kg
> 1.95 L in 2.5
hours

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if hypotensive > 29 mL/kg > 30 mL/kg
> 1.95 L in 2.5
hours

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if hypotensive > 29 mL/kg > 30 mL/kg
> 1.95 L in 2.5
hours

Power of randomization
Properties of the normal distribution
Two Concepts to Remember

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if hypotensive > 29 mL/kg > 30 mL/kg
> 1.95 L in 2.5
hours

Intention to Treat Analysis
Inclusion of all randomized patients in each
group
Helps overcome
– Protocol non-compliance
– Missing data
Not intended for
– Patients who already meet endpoint at inclusion
Perspect Clin Res. 2011 Jul-Sep; 2(3): 109–112.

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if hypotensive > 29 mL/kg > 30 mL/kg
> 1.95 L in 2.5
hours

Rivers, et al. ProCESS ARISE ProMISe
# per group 130, 130 445, 448, 458 792, 796 625, 626
Standard Rx
Mortality 46.5% 18.9% 18.8% 29.2%
EGDT
Mortality 30.5% 21.0% 18.6% 29.5%
APACHE II 20.4 20.7 15.8 18.0
ScvO2 % 48.6 ± 11.2 71 ± 13 72.7 ± 10.5 70 ± 12
ScvO2 > 70% 3, 3 222, 224, 229 346, 348 312, 313
Antibiotic
Time
92.4% in 6
hours
75% in 72
minutes
median 91
minutes
100% in 2.5
hours
Fluids Before
Randomizing
20-30 mL/kg,
if
hypotensive
> 29 mL/kg > 30 mL/kg > 1.95 L in 2.5
hours

ProCESS, ARISE, ProMISe
• EGDT, as originally defined, applied to patients
who meet the original criteria, does not add
survival benefit in centers adept at sepsis
management when patients are identified early,
given antibiotics and fluid boluses early.

EGDT vs Control:
Benefit Depends on Control
Group Mortality
Benefit when
Control Mortality >35%
EGDT inferior to
Lactate/CVP directed
therapy

Remaining Scientific Questions
How important is low ScvO2 in determining
MORTALITY from septic shock?
Should all patients with septic shock be
assessed for low ScvO2? (this means central
access in all)
For patients who actually have low ScvO2, is
some form of systematic approach
desirable?
Time will tell!

CMS Measures
and
Quality Sepsis Care
“We’re from the Government
We’re here to help”

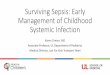
Surviving Sepsis Campaign Bundles
To be completed within 3 hours:
1. Measure serum lactate level
2. Obtain blood cultures prior to administration of
antibiotics (1C)
3. Administer broad spectrum antibiotics (1B, 1C)
4. Administer 30 mL/kg crystalloid for
hypotension or lactate ≥ 4 mmol/L

Surviving Sepsis Campaign Bundles
To be completed within 6 hours
1. Apply vasopressors (for hypotension that does not
respond to initial fluid resuscitation) to maintain a
mean arterial pressure (MAP) ≥ 65 mm Hg
2. In the event of persistent arterial hypotension despite
volume resuscitation (septic shock) or initial lactate ≥
4 mmol/L (36 mg/dL)
Measure central venous pressure (CVP)*
Measure central venous oxygen saturation (ScvO2)*
3. Re-measure lactate if initial lactate was elevated*
*Targets are: CVP 8 mm Hg, ScvO2 > 70%, lactate normal

CMS Core Measures: Simply Complicated
Within 3 hours of Presentation of
Severe Sepsis
1. Initial lactate level measurement
2. Broad spectrum antibiotics administered
3. Blood cultures drawn prior to antibiotics
4. Crystalloid fluid initiated
Within 3 hours of Presentation of
Septic Shock
1. Resuscitation with 30ml/kg crystalloid fluids
2. Evaluate the need for vasopressors
Did hypotension persist after fluid given?
NO
YES, continue on
Core Measure goals met, re-measure lactate within 6hrs
After fluid resuscitation, but within 6
hours of Presentation of Septic Shock
Re-assessment of volume status and tissue perfusion A focused exam including
• Vital signs
• Cardiopulmonary exam
• Capillary refill evaluation
• Peripheral pulse evaluation
• Skin examination
Must be performed and
documented by a Physician,
ARNP, or PA
2 out of 4 from the following:
CVP Bedside Cardio US ScvO2
Passive Leg Raise or Fluid Challenge

www.mwcritcare.org

www.kansassepsisproject.org

www.kansassepsisproject.org