Embed Size (px)
Citation preview

10/26/2015
1
Diagnosis and Management of Sepsis
David Shimabukuro, MDCMMedical Director, 13 ICU
Physician Lead, UCSF Sepsis Bundle Compliance and Mortality Reduction
Disclosures
• I have no disclosures

10/26/2015
2
The following feature has been edited for content and to run in
the allotted time
Agenda
• Epidemiology
• Definitions and Diagnosis
• Treatment
– Definitive
– End‐organ support

10/26/2015
3
Agenda
• Epidemiology
• Definitions and Diagnosis
• Treatment
– Definitive
– End‐organ support
Epidemiology

10/26/2015
4
Epidemiology
Epidemiology

10/26/2015
5
Death rate over time
0
50
100
150
200
250
300
2000 2002 2004 2006 2008 2010
Heart Disease
Malignant Neoplasms
Cerebrovascular Disease
Septicemia
National Vital Statistics Reports, vol 6, no 4, May 08, 2013
Epidemiology
38%
20%
8%
8%
14% 12%
Cause
Lung
Blood
Skin/Soft Tissue
Abdominal
Genitourinary
Other

10/26/2015
6
Agenda
• Epidemiology
• Definitions and Diagnosis
• Treatment
– Definitive
– End‐organ support
CASE
Mrs. M is an 82 year‐old woman with a past medical history significant for Alzheimer’s, hypothyroidism, and hypertension, was admitted to the floor from a skilled nursing facility with dysarthria from an acute CVA.

10/26/2015
7
CASE
On hospital day 2, she is quite somnolent but arouses with tactile stimulation. Her vitals are BP 120/76, HR 78, RR 30, Temp 38, and oxygen saturation 90% on 6LNC (she was on RA yesterday evening). Her WBC this morning has increased to 11.1 from 8.9.
CASE

10/26/2015
8
Does she have…
1. Systemic inflammatory response syndrome
2. Sepsis
3. Severe Sepsis
4. Septic shock
5. None of the above
I would order a lactate?
1. No
2. Yes

10/26/2015
9
CASE
Her lactate level returns at 4.4 mmol/L.
Does she have…
1. Systemic inflammatory response syndrome
2. Sepsis
3. Severe Sepsis
4. Septic shock
5. None of the above

10/26/2015
10
I would transfer her to the ICU
1. No
2. Yes
I would place a central venous catheter
1. No
2. Yes

10/26/2015
11
Sepsis Definitions
• SIRS
• Sepsis
• Severe Sepsis
• Septic Shock
Septic Shock
SEVERE SEPSIS plushypotension (Systolicblood pressure < 90 orMean Arterial Blood Pressure < 65) OR Lactate > 4
Severe Sepsis
SEPSIS plus evidenceof at least one alteration in organ perfusion
Sepsis
SIRS plus confirmed or suspected infection
Sepsis: ACCP/SCCM Definitions
SIRS
T > 38.3 C or < 36 CHR > 90 beats/minTachypneaWBC > 12K or < 4K
SIRS
T > 38.3 C or < 36 CHR > 90 beats/minTachypneaWBC > 12K or < 4K
SIRS
T > 38.3 C or < 36 CHR > 90 beats/minTachypneaWBC > 12K or < 4K

10/26/2015
12
Severe Sepsis Definition
Crit Care Med February 2013 Volume 41 Number 2 pp. 580‐637

10/26/2015
13
San Francisco Definition
Sepsis is defined as a life‐threatening organ dysfunction due to a dysregulated host response to infection.

10/26/2015
14
What is Sepsis??
• A variable condition that affects each of us differently and is initiated by a known or suspected infectious insult.
Is catching it earlier better??

10/26/2015
15
Sepsis Screening
Crit Care Med February 2013 Volume 41 Number 2 pp. 580‐637
Sepsis Screening
Crit Care Med February 2013 Volume 41 Number 2 pp. 580‐637
Great….but when should we do it and how should it be done!!!!

10/26/2015
16
Sepsis Screening
Sepsis Screening

10/26/2015
17
Sepsis Screening
• Important to have one that works for your hospital
• Should probably do once a shift (no clear data)
• Screening works as a reminder for continued awareness and vigilance
• (Determine time of presentation)
Agenda
• Epidemiology
• Definitions and Diagnosis
• Treatment
– Definitive
– End‐organ support

10/26/2015
18
Definitive Treatment
• Antibiotics
• Source Control
Management of Severe Sepsis and Septic Shock
Crit Care Med February 2013 Volume 41 Number 2 pp. 580‐637

10/26/2015
19
Management of Severe Sepsis and Septic Shock
1
Crit Care Med 2006 Vol. 34, No. 6

10/26/2015
20

10/26/2015
21
End‐organ support (by improving tissue perfusion)…
Management of Severe Sepsis and Septic Shock

10/26/2015
22
Management of Severe Sepsis and Septic Shock
• Fluid Therapy
– Crystalloids are first choice for the overwhelming majority of patients
– Albumin can be used to reduce volume from crystalloids
– Hydroxyethyl starches should not be used
Management of Severe Sepsis and Septic Shock
• Fluid Therapy
– WATCH OUT!!!!!
– Too much fluid is bad and not enough is bad…

10/26/2015
23
Management of Severe Sepsis and Septic Shock
Management of Severe Sepsis and Septic Shock

10/26/2015
24
Management of Severe Sepsis and Septic Shock
Beyond the 6‐hour resuscitation

10/26/2015
25
Management of Severe Sepsis and Septic Shock
• Lung Injury
– All patients at risk
– Low‐tidal volume ( 6cc/kg IBW)
– Plateau pressure < 30 cm H20
– Permissive hypercapnia
– FIO2:PEEP strategy
Management of Severe Sepsis and Septic Shock
• Corticosteroids
– For refractory hypotension despite fluids and vasopressors/inotropes
– Do not perform ACTH stimulation test
• Glucose
– Target level to less than 180 mg/dL

10/26/2015
26
Management of Severe Sepsis and Septic Shock
• Blood Products
– HGB level 7.0 – 9.0 g/dL after hypoperfusion has resolved
– FFP not to be used unless bleeding is present or for planned invasive procedure
– PLT to be given prophylactically when <10K in absence of bleeding
Management of Severe Sepsis and Septic Shock

10/26/2015
27
EGDT
Management of Severe Sepsis and Septic Shock
Does this bundle actually work??

10/26/2015
28
Management of Severe Sepsis and Septic Shock
yes…
no…
Crit Care Med 2010 Vol 38 No 2 pp 367‐374
Management of Severe Sepsis and Septic Shock

10/26/2015
29
Management of Severe Sepsis and Septic Shock
Management of Severe Sepsis and Septic Shock

10/26/2015
30
Management of Severe Sepsis and Septic Shock
Management of Severe Sepsis and Septic Shock

10/26/2015
31
Original Article
A Randomized Trial of Protocol-Based Care for Early Septic Shock
The ProCESS Investigators
N Engl J MedVolume 370(18):1683-1693
May 1, 2014
Cumulative Mortality.
The ProCESS Investigators. N Engl J Med 2014;370:1683-1693

10/26/2015
32
Conclusions
• In a multicenter trial conducted in the tertiary care setting, protocol-based resuscitation of patients in whom septic shock was diagnosed in the emergency department did not improve outcomes.
Original Article
Goal-Directed Resuscitation for Patients with Early Septic Shock
The ARISE Investigators and the ANZICS Clinical Trials Group
N Engl J MedVolume 371(16):1496-1506
October 16, 2014

10/26/2015
33
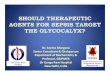
Probability of Survival and Subgroup Analyses of the Risk of Death at 90 Days.
The ARISE Investigators and the ANZICS Clinical Trials Group. N Engl J Med 2014;371:1496-1506
Conclusions
• In critically ill patients presenting to the emergency department with early septic shock, EGDT did not reduce all-cause mortality at 90 days.

10/26/2015
34
Original Article
Trial of Early, Goal-Directed Resuscitation for Septic Shock
Paul R. Mouncey, M.Sc., Tiffany M. Osborn, M.D., G. Sarah Power, M.Sc., David A. Harrison, Ph.D., M. Zia Sadique, Ph.D., Richard D. Grieve, Ph.D., Rahi Jahan, B.A.,
Sheila E. Harvey, Ph.D., Derek Bell, M.D., Julian F. Bion, M.D., Timothy J. Coats, M.D., Mervyn Singer, M.D., J. Duncan Young, D.M., Kathryn M. Rowan, Ph.D.,
for the ProMISe Trial Investigators
N Engl J MedVolume 372(14):1301-1311
April 2, 2015
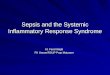
Kaplan–Meier Survival Estimates.
Mouncey PR et al. N Engl J Med 2015;372:1301-1311

10/26/2015
35
Conclusions
• In patients with septic shock who were identified early and received intravenous antibiotics and adequate fluid resuscitation, hemodynamic management according to a strict EGDT protocol did not lead to an improvement in outcome.
Changes…

10/26/2015
36
Surviving Sepsis Campaign Bundle Revision 2015
Surviving Sepsis Campaign Bundle Revision 2015

10/26/2015
37
Summary
• A very heterogeneous disease that is difficult to diagnose in its early stages and difficult to treat in its later stages.
• Routine screening can allow for earlier identification
• Early intervention can attenuate its course
Summary
• Definitive treatment involves rapid appropriate antibiotic administration and source control
• Supportive care for end‐organ dysfunction is the mainstay of treatment
• Management bundle continues to evolve

10/26/2015
38
UCSF Experience
Leveraging data in the EMR
• Vital signs/assessments
• Laboratory values
• Problem list
• Medication list

10/26/2015
39
Leveraging data in the EMR
• 6 different algorithms based on patient location
– ED
– Medical/Surgical ward
– Medical/Surgical ICU
– Hematology/Oncology
– CVT ward
– CVT ICU

10/26/2015
40
• Code Sepsis
• UCSF Sepsis Bundle
10/26/2015
Sepsis Updates80
UHC Sepsis Mortality Index

10/26/2015
41