Embed Size (px)
Citation preview

Seminar Research in actionRemoving the gap between research and practical prevention
European ParliamentBrussels
25 november 2010
Proceedings

Research in action. Removing the gap between research and practical preventionSeminar proceedings
Brussels, European Parliament, 25 November 2010
Copyright: PEROSH 2011
Partnership for European Research in Occupational Safety and Health PEROSH Secretariatc/o PreventRue Gachard 88/4B - 1050 Brussels
e-mail: [email protected]
Photos: Freddy Willems

Introduction On 25 November 2010, European researchers and policymakers came to-gether to reflect on how to improve the transfer of evidence-based research with regard to the working environment and the practical implementation at the workplace.
The seminar was organised by PEROSH and part of ‘The Quality of Working Life’ Event, prepared by Prevent (Belgian Institute for Occupational Safety and Health) within the framework of the Belgian EU Presidency. It concerned a series of seminars, network events and a closing colloquium, organised from 24-26 November 2010 at the European Parliament in Brussels.
The theme of the seminar was inspired by an earlier seminar organized by the Danish working environment authority and PEROSH in September 2009 in Copenhagen with regard to the Working Environment Challenges of the Future. During this seminar the participating researchers concluded that more attention should be paid to action and implementation of research to test the effectiveness of preventive solutions. More collaboration between researchers at the international level could improve the consideration of these topics .
The seminar ‘Research in Action’ was introduced by Marc De Greef, member of the Executive committee of PEROSH and chaired by Chairman Dr. Palle Ørbæk and Vice-chairman Dr. Didier Baptiste.
The seminar opened with two keynote speakers setting the frame of the seminar by focusing on the drivers for applied research on the one hand and on the other hand elaborating on how the link between corporate competi-tiveness and occupational health and safety can be enhanced. A number of strong case examples proved that the implementation of re-search driven results on the work floor is possible. To conclude, the PEROSH seminar sought the visions and expectations of the European social partners and government with regard to the transfer between research and practice and on how the interaction between research and policy could be improved.
The proceedings contain a summary of the presentations at the seminar as well as a number of papers drafted by the speakers. The presentations, papers and proceedings can be accessed via the PEROSH website, www.perosh.eu
We wish to thank all speakers for their inspiring presentations and best practices to remove the gaps between research and practical prevention.
Introduction �


Contents
Introduction ............................................................................................................................................................................................ 1
Programme ............................................................................................................................................................................................... 4
Summary of presentations ......................................................................................................................................................... 5
1. Research in action�� Importance�� driversResearch in action�� Importance�� drivers ................................................................................................................... 5 1.1 Drivers for applied OSH-research – Dr. Dietmar Reinert, Scientific Chairman of PEROSH, Institute for Occupational Safety and Health (IFA – DGUV) ................................................. 5 1.2 Competitiveness in a global context – Dr. Guy Ahonen, Research professor, Finnish Institute of Occupational Health (FIOH) ............................................................................................... 6
2. Case examples of research in action .......................................................................................................................... 8 2.1 Return to work intervention on a national scale in Denmark - Research and action – Mr. Glen Winzor, Senior Consultant, National Research Centre for the Working Environment (NRCWE) ....................................................................................................................................................... 8 2.2 Improving productivity and working conditions to reduce Musculosketal Disorders (MSD) – Ms. Gu van Rhijn, Senior project leader, TNO Work and Employment ............................................. 9 2.3 Flexible working time and mental health – Dr. Dorota Zolnierczyk-Zreda, Department of Ergonomics, Laboratory of Work Psychology and Sociology, Central Institute for Labour Protection (CIOP – PIB) ..................................................................................... 11 2.4 Measuring and preventing noise – Dr. Séverine Brunet, Head of the Work Equipment Engineering division, Institut National de Recherche et de Sécurité (INRS) ................................. 12
3. Vision and expectations of the social partners and government ............................................ ......... 13 3.1 European Public Health Research into Policy – Mr. Kevin Mc Carthy, Head of sector , Public Health Research, DG Research ................................................................................................. 13 3.2 Vision and expectations for research in action from the employers side – Mr. Kris De Meester, Chair Health and Safety working group, Business Europe .................................................. 15 3.3 Reflections on research in action from the employees side - Dr Stefano Boy, Senior Researcher, European Trade Union Institute .................................................................................. 16 3.4 Governmental vision and expectations on (OSH) research and development activities – Dr. Erkki Yrjänheikki, Governmental group of the Advisory Committee on Health and Safety, Director Ministry of Social Affairs and Health, Finland .................................... 18
4. PEROSH and the transfer between research and practice ...................................................................... 19 – Dr. Didier Baptiste, Vice-Chairman, Chairman-elect PEROSH
Papers ..................................................................................................................................................................................................... 21Science meets Practice – driving forces behind applied OSH research – Dr. Dietmar Reinert (IFA-DGUV) ................................................................................................................................................................................................ 21OSH and corporate competitiveness in a global context – Dr. Guy Ahonen (FIOH) ................................. 28The Danish National Return to Work Project – Glen Winzor (NRCWE) .............................................................. 31Improving performance and working conditions in Industry – Gu Van Rhijn, Tim Bosch (TNO) ... 33 Enhancing mental health of employees working long hours through flexible time arrangements – Dr. Dorota Zolnierczyk-Zreda (CIOP-PIB) ....................................................................................... 42
Contents �

� Seminar Research in action 25/11/2010
Programme November 25, 2010
13:30 – 13:40 Welcome Mr. Marc De Greef, Steering Committee PEROSH
13:40 – 14:35 I. Research in action: Importance, drivers and practical examples Chair: Dr. Palle Ørbæk, chairman of PEROSH
13:40 – 13:45 Introduction
Keynotes
13:45 – 14:10 Keynote �: Science meets Practice - Drivers for applied OSH-research.
Dr. Dietmar Reinert, Scientific Chairman of PEROSH, Institute for Occupational Safety and Health (IFA – DGUV)
14:10 – 14:35 Keynote 2: OSH and Corporate Competitiveness in a Global Context. Dr. Guy Ahonen, Research professor, Finnish Institute of Occupational Health (FIOH)
14:35 – 15:35 PEROSH cases
Return-to-work intervention on a national scale in Denmark - Research and action. Mr. Glen Winzor, Senior Consultant, National Research Centre for the Working Environment (NRCWE)
Improvement of both productivity and working conditions, with special focus on MSD. Ms. Gu van Rhijn, Senior project leader, TNO Work and Employment
Enhancing mental health of employees working long hours through flexible time arrangements. Dr. Dorota Zolnierczyk-Zreda, Department of Ergonomics, Laboratory of Work Psychology and Sociology, Central Institute for Labour Protection, (CIOP – PIB)
Noise at work: ISIT, a tool from research to practical intervention. Dr. Séverine Brunet, Head of the Work Equipment Engineering division, Institut National de Recherche et de Sécurité (INRS)
15:35 – 16:00 Break
16:00 – 17:20 II. Vision and expectations of the social partners and government from research in action Chair: Dr. Didier Baptiste, Vice-chairman of PEROSH
16:00 – 16:05 Introduction
16:05 – 17:20 - Mr. Kevin Mc Carthy, Director Public Health Research, DG Research - Mr. Kris De Meester, Chair Health and Safety working group, Business Europe - Dr. Stefano Boy, Health and Safety Department, ETUI - Dr. Erkki Yrjanheikki, Governmental group, Advisory Committee on Safety and Health
17:20 – 17:35 III. Vision of PEROSH on Research in action Dr. Didier Baptiste, Vice-chairman of PEROSH
17:35 – 17:45 IV. Conclusions Mr. Marc De Greef, Steering Committee PEROSH

Summary of presentationsNew developments in the field of working life and occupational safety and health should be sup-ported by scientific evidence and results coming from workplace research. However, new insights in workplace research do often not find their way to the workplace. Several barriers can slow down the effective transfer of research knowledge to the work floor. This summary provides an overview of the main points raised by the presentations.
�. Research in action: importance, drivers
1.1 Drivers for applied OSH-research Dr. Dietmar Reinert, Scientific Chairman of PEROSH, Institute for Occupational Safety and Health (IFA – DGUV)
A project of the German Statutory Accident Insu-rance (DGUV) investigated the mutual influences between the different prevention services and found that the knowledge that drives real innovation in pre-vention services is found in the expert committees and the research institutes.
One of the weaknesses of the transfer process is however that new research conclusions are rarely
directly read by the people who will implement new occupational health and safety solutions on the company floor.
From their projects, the IFA identified a number of drivers and quality indicators that are needed to enhance the likelihood of transfer between research and practice. It was concluded that besides the use of good academic practice and good time management, involvement of the company management and of the target group in an early stage of the project as well as tuning the research to the needs of the companies are crucial for the success of the project. Other than that, the timely translation of the research and development findings into a practical solution is needed to ensure the continuation and real use of the results. It was also found that external funding often has a beneficial impact on the management standards of a project. The implementation strategy – if needed with an external partner - as well as the dis-semination strategy should be included into the stage of the project design and clearly adapted to the company floor. Adequate transfer points should be carefully chosen to pass on the knowledge to the company.
Projects that take on an innovative, holistic, interdisciplinary and even international approach tend to be more successful than others. Dr. Reinert also made an appeal not to duplicate research and use of research findings as a basis for other projects and to develop a methodology.
Summary of presentations �

� Seminar Research in action 25/11/2010
1.2 Competitiveness in a global context Dr. Guy Ahonen, Research professor, Finnish Institute of Occupational Health (FIOH)
Dr. Ahonen stated that new ways of thinking and value creation models are emerging globally and have an effect on global competitiveness and strate-gies for co-operations.
The models and strategies that are currently adopted by firms are focused on- Cost leadership, where the focus is on the cost level and reduction of costs
- Product differentiations, where a business tries to establish small areas of monopolies- Knowledge and skills (intangible assets)
It is often thought by enterprises that the cost leadership strategy is the only suitable strategy avail-able. From this point of view occupational safety and health investment is considered an extra cost that the company cannot afford.
For that reason, investments in occupational safety and health in general and in applying OSH research results on the company floor are seldom considered as a way of reducing costs. The cost reducing effects of occupational safety and health are well documented in scientific literature.Critical reviews show that workplace health promotion leads to an increase in productivity, a reduc-tion in sickness leave, in health care costs and in pension costs.Moreover, studies investigating the issue carry a coherent message: well-planned and systematically carried out OSH measures create economic returns, which are 3-10 times the monetary investment. A project in more than 200 small and medium sized enterprises in Finland showed that promotion of workability had an important effect on profitability and productivity. It is possible even with a major investment to reach a profit.
European statistics show that there is a lot to gain from reducing the costs of sickness and espe-cially from early retirement. According to OECD figures, the cost of early retirement amounts to an average of 6,3% of the potential Gross Domestic Product (GDP). The cost of illness adds up to 3,8% of the GDP. This implies that here is a huge potential for cost reductions. Health related research shows also that indirect costs are not measured, which leads to a serious distortion of the real costs. Besides that, there is proof that the lower the workability, the higher the early retirement of the workforce will be.
From Finnish research, it becomes clear that the costs of early retirement, sickness leave, presentee-ism and occupational accidents do not measure up to the financial investments made to tackle these costs (via e.g. investments in training, OSH, promotion of workability, corporate fitness and communication). It was concluded that the costs of poor safety and health are approximately 15 times higher than the investments.

What can be done? Dr. Ahonen presented the triple bottom line approach which includes an expanded series of values and criteria, and measures the total performance by including not only the financial performance but also the environmental and social performance. OSH is included in the social aspects. This is closely linked to the concept of Corporate Social Responsibility. This concept stimulates companies on a voluntary basis to integrate social and environmental concerns in their business operations and in their interaction with their stakeholders. Human resource management is at the heart of CSR.
It was concluded that inadequate health and safety is an enormous cost for the industrial countries and can harm the competitiveness of businesses. While we are moving towards a more knowledge based production and consumption, the focus shifts towards three forms of intangible assets which are all related to OSH: human capital (knowledge and skills of employees), structural capital (work community and production processes), relational capital (stakeholders, such as clients, suppliers and competitors).
Summary of presentations �

2. Case examples of research in actionThe themes of the cases present four main challenges of the occupational health issues of today: sickness absence and return to work, musculoskeletal disorders (MSD), stress and mental health, and noise.
2.1 Return to work intervention on a national scale in Denmark - Research and action Mr. Glen Winzor, Senior Consultant, National Research Centre for the Working Environ-ment (NRCWE)
Glen Winzor presented one of the biggest research projects on return to work in the world. The project started from the need of Danish municipalities across Denmark to improve the return to work of people on long-term sickness absence, which dramatically rose between 2004 and 2008. The project is part of an action plan concluded between the government and social partners and includes people with all kinds of diagnoses such as
MSD and mental disorders. The aim of the project is to determine whether the developed model will reduce sickness leave and will improve the return to work. It should lead to concrete and practi-cal measures to reduce the duration of sickness absence and improve the return-to-work status, work ability and health related quality of life and psychosocial well-being.
Evidence – based recommendationsThe project was based on previous knowledge and emerging evidence from a range of smaller Danish and international studies on return to work interventions and on two comprehensive reviews on MSD and mental health of the scientific literature from the Danish National Research Centre for the Working Environment, which had a strong influence on the project.
Both white papers resulted in a number of recommendations for the project, including the need - for improvement of coordination and communications between all stakeholders- to early detect and treat health problems - to involve the sickness benefit offices and workplaces- for interdisciplinary intervention and early identification of the potential barriers for return to work- to adapt the work tasks to the reduced levels of functioning- to facilitate the social integration at work- to assess the individual level of functioning and evaluate how this influences work ability
� Seminar Research in action 25/11/2010

Project set-up The project made a distinction between interventions at organizational and individual level. For the organizational inventions a multidisciplinary team was created in the offices consisting of a case manager/return to work co-ordinator, psychologist, physiotherapist/occupational therapist, occupational physician, psychiatrist. Due to different backgrounds and visions of the experts on people that are on sickness leave, clear case-flow descriptions, tools and guides were necessary. At the individual level, persons on sickness leave received a multidisciplinary assessment leading to an individualised intervention, including education and counselling.
Crossing the action bridge between researchers and research usersThe project has identified several prerequisites to transfer the scientific research results into a large-scale action. The project needs a clear “burning platform” and support from all stakeholders - not least the social partners and politicians - involved. This implies that participants need to be convinced about the relevance of the project itself, but also have to understand and adhere to the vision of the project and the underlying research. Empowerment must be stimulated so that part-ners feel ownership of the project. There has to be room for flexibility and adjustments throughout the project but it is important that these changes are coordinated by the project management. The project management and researchers involved should have specific qualifications and experience to be able to implement and support a comprehensive organizational change.
2.2 Improving productivity and working conditions to reduce Musculosketal Disorders (MSD) Ms. Gu van Rhijn, Senior project leader, TNO Work and Employment
European manufacturers nowadays are confronted with a number of challenges that are directly linked to the market demands. Customers require a larger variety of products at a shorter delivery time, at low costs and with high quality. Companies are required to flexibly deal with demands for smaller batches of products but also with fluctuations in volumes throughout the year. The pressure under which companies are operating may lead to increased
physical and mental stress upon workers.
In the EU, a considerable challenge of tomorrow will be to keep the ageing workforce healthy. Be-sides that, musculoskeletal Disorders (MSDs) are the biggest cause of absence from work in practi-cally all member states. In some countries, 40% of the costs of workers’ compensation are caused by work related MSDs and up to 3% of the gross domestic product of the country itself; reducing the productivity and adding to the social costs of government.
Summary of presentations �

�0 Seminar Research in action 25/11/2010
In the manufacturing companies the question was how to immediately increase the output volume if the demand increases, without compromising efficiency, quality, costs and workload on employees.The projects implemented use a participatory and integrative approach to analyse and study the situation at the company. A priority in participatory ergonomic processes includes the reduction of MSDs by eliminating the physical and psychosocial risk factors that are associated with the disorders. Many of the physical risk factors associated with MSD are often the result of inefficient and poorly designed work prac-tices. Other risk factors that need attention are related to the temporal pattern of the load during the day. Aspects of this time pattern or ‘rhythm’, like work rest schedules, task variation, cycle time, and work pace may clearly affect the worker, both mentally and physically.
Integrated innovations lead to improvement of productivity and working conditionsOne of the case examples presented, concerned the change from a batch production to a mixed flow assembly system including ergonomically designed workstations. A second example focused on alternatives in work rest schemes to increase productivity and flexibility and to reduce fatigue. In both cases, the effects in terms of productivity, flexibility, and physical and mental loads on the workers were studied.
The results in the first case pointed to an increase of productivity of 44%. At the same time a reduc-tion of hazards of lifting and improved job satisfaction were observed. There was no increased risk of frequency and postures and the experience of mental workload did not change. A remaining point of discussion concerned however the increased time percentage of direct work or work intensification, which may increase the risk of MSD. In case of higher amounts of direct work, the need for variation interrupting the assembly work increases.
In the second case, the researchers studied this variation and interruption in a project on alternative pause systems. In this case the volume flexibility was attained by adding two workers and by apply-ing alternative work rest schemes. These modifications resulted in a 12-16% higher product output. It was noticed that the physical neck and shoulder load was reduced especially in the alternating scheme with a high number of breaks and total break time. However, due to social aspects, this scheme is only recommended during time periods of peak demand (up to 2 months). In this alter-nating work rest scheme the workers have a break in couples instead of a team break.
ConclusionsThe cases led to integrated improvements of both productivity and working conditions by innova-tions in production systems, workstation and organisation. Traditionally, most companies focus either on technological innovations or on the organizational structures or on enhancing human re-sources. It was found however that the best performance will be realized when all three factors are involved. Managers usually associate ergonomics with occupational health and not with business performance. The focus of human factors should be linked to business strategies and the manage-ment world. It is recommended that human factor specialists are involved at an early stage in the design process and accustom their arguments to make them understandable for management and engineers.

2.3 Flexible working time and mental health Dr. Dorota Zolnierczyk-Zreda, Department of Ergonomics, Laboratory of Work Psycho-logy and Sociology, Central Institute for Labour Protection, (CIOP – PIB)
Long working hours are being observed throughout Europe nowadays. Flexible working time has obtai-ned a growing interest because of, or partly due to, work intensification and is considered one of most prevalent emerging psychosocial risks today.
Dr. Zolnierczyk-Zreda presented a new study on Polish employees performing clerical work for more than 8 hours daily. The study investigated the poten-
tial role of flexible working time on different health dimensions such as somatic complaints, anxiety, social dysfunction and depression. The study also aimed at determining which age and gender group working long hours, benefits most from flexible work time. Flexibility was defined as the possibility to decide when to start and finish work.
The study was based on longitudinal data and found a significant effect of flexibility as a predictor of positive change in somatic complaints and social functioning. No significant effect was noticed with regard to anxiety and depression. There was however a significant effect of flexibility as predic-tor of a positive change in overall health complaints.
All in all, it can be said that increased working time flexibility is associated with: decreased overall health complaints, decreased somatic complaints and decreased social dysfunction.
Conclusions The study showed that working time flexibility has a significant influence on decreased depression in the youngest group of female workers aged 18-29 comparing to females not having flexible working hours. Even in the presence of objectively existing psychosocial risks, such as long working hours, pro-grams that promote work time flexibility may have a beneficial effect on workers’ mental health. Thus, providing employees with work time control may promote health in strenuous work life. In addition, men and women are not homogenous groups on matters related to workplace flexibi-lity. Female workers, especially in the youngest age group, seem to need and benefit from flexible time arrangements even more than male workers in terms of preserving their mental health in the long run and maintain it until a delayed retirement age.
Summary of presentations��
�2 Seminar Research in action 25/11/2010
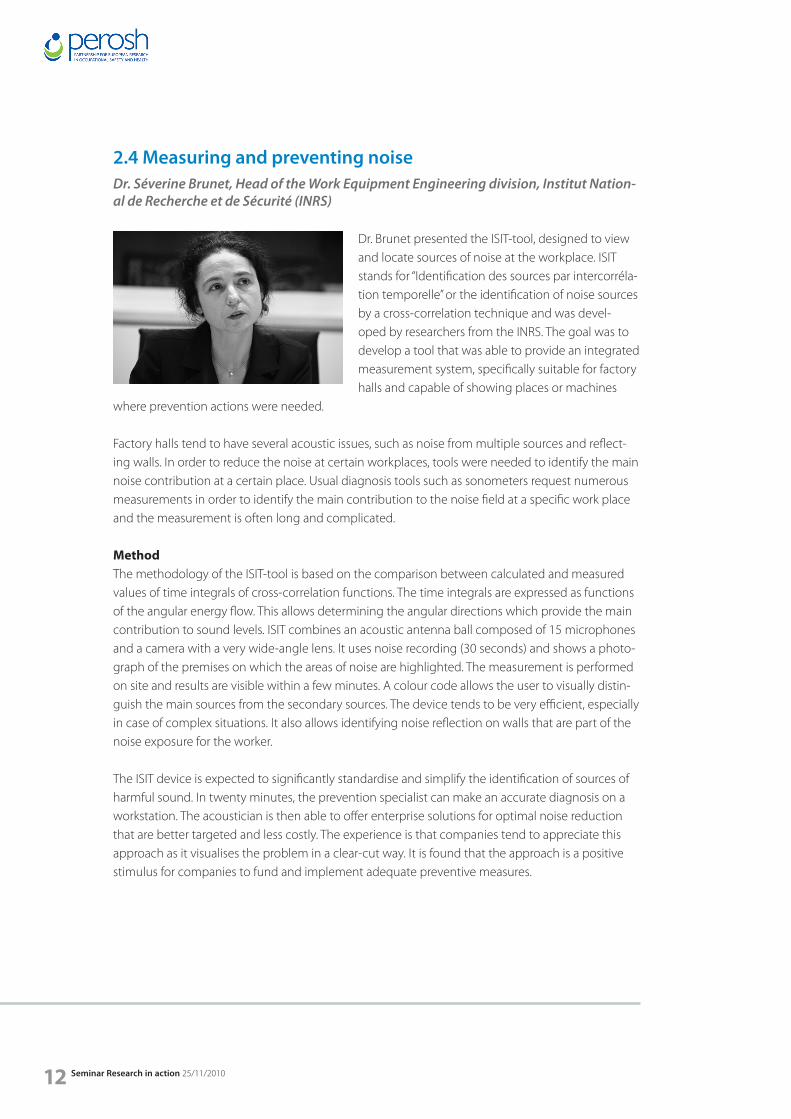
2.4 Measuring and preventing noise Dr. Séverine Brunet, Head of the Work Equipment Engineering division, Institut Nation-al de Recherche et de Sécurité (INRS)
Dr. Brunet presented the ISIT-tool, designed to view and locate sources of noise at the workplace. ISIT stands for “Identification des sources par intercorréla-tion temporelle” or the identification of noise sources by a cross-correlation technique and was devel-oped by researchers from the INRS. The goal was to develop a tool that was able to provide an integrated measurement system, specifically suitable for factory halls and capable of showing places or machines
where prevention actions were needed.
Factory halls tend to have several acoustic issues, such as noise from multiple sources and reflect-ing walls. In order to reduce the noise at certain workplaces, tools were needed to identify the main noise contribution at a certain place. Usual diagnosis tools such as sonometers request numerous measurements in order to identify the main contribution to the noise field at a specific work place and the measurement is often long and complicated.
MethodThe methodology of the ISIT-tool is based on the comparison between calculated and measured values of time integrals of cross-correlation functions. The time integrals are expressed as functions of the angular energy flow. This allows determining the angular directions which provide the main contribution to sound levels. ISIT combines an acoustic antenna ball composed of 15 microphones and a camera with a very wide-angle lens. It uses noise recording (30 seconds) and shows a photo-graph of the premises on which the areas of noise are highlighted. The measurement is performed on site and results are visible within a few minutes. A colour code allows the user to visually distin-guish the main sources from the secondary sources. The device tends to be very efficient, especially in case of complex situations. It also allows identifying noise reflection on walls that are part of the noise exposure for the worker.
The ISIT device is expected to significantly standardise and simplify the identification of sources of harmful sound. In twenty minutes, the prevention specialist can make an accurate diagnosis on a workstation. The acoustician is then able to offer enterprise solutions for optimal noise reduction that are better targeted and less costly. The experience is that companies tend to appreciate this approach as it visualises the problem in a clear-cut way. It is found that the approach is a positive stimulus for companies to fund and implement adequate preventive measures.

�. Visions and expectations of the social partners and governmentThe support of European social partners and decision makers is essential in anchoring initiatives for the transfer and interaction between research and practice in a wider and long-term European framework. In the following presentations the social partners gave their vision and expectations of research in action.
3.1 European Public Health Research into Policy Mr. Kevin Mc Carthy - Head of sector - Public Health Research
Mr. Mc Carthy, Head of the Public Health and Health services research department at the Health director-ate presented a number of relevant elements under the EU programme for research and more in specific with regard to the “delivery of care” and the transla-tion of research into policy; and described the frame in which his unit is active. Previously, the EU research concentrated more on a bottom-up approach. From the 5th Framework Pro-
gramme (FP), a more societal approach (such as a focus on ageing) including occupational safety and health was followed.
Mr. Mc Carthy presented the mandate and framework in which research is funded for the health theme. Delivery of care has a broad mandate within this programme. There is no formal mandate on occupational safety and health but the directorate adopts a holistic and horizontal approach on health and well-being.
There are three pillars in the structure. The public health research unit’s mandate concerns the specific activity of “Optimising the delivery of health care to citizens” (Activity n°3) which aims at providing the necessary basis both for informed policy decisions on health systems and for more effective and efficient evidence-based strategies of health promotion, disease prevention, diagnosis and therapy.
The specific activity is broken down into three subareas: 3.1 to translate clinical research into clini-cal practice, 3.2 to carry out health care systems research, 3.3 to stimulate health promotion and disease prevention. Mr. Mc Carthy described the projects running under these three subareas and pointed at openings for integrating OSH into the programmes. Each area has a particular mandate. The projects were mapped in a matrix demonstrating the spread of the project.
Subarea 3.3 on stimulating health promotion and disease prevention is aiming at providing evi-dence for the best public health measures in terms of life styles, work and living circumstances and
Summary of presentations ��

�� Seminar Research in action 25/11/2010
interventions at different levels and in different contexts. Focus will be on the wider determinants of health and how they interact at both the individual and community level (e.g. diet, stress, tobacco, alcohol and other substances, physical activity, cultural context, socio-economic and environmental factors). In particular mental health will be addressed in a life-course perspective.
Bridging the gap – translating research into policyMr Mc Carthy mentioned that it is important to choose the right kind of bridge to effectively trans-late research knowledge into policy and described a number of projects that are related to OSH. One of the mandates of public health research is to provide informed policy, based on research, and to realize knowledge transfer and brokering. Public health has a number of projects that specifically address the challenge of translating research into practice and building the bridge between the two. Besides that, a number of projects related to OSH were set up, especially on OSH and economics (ECOSH, ROWER), data collection on accidents and disabilities (INTEGRIS), etc. A call on health promotion and disease prevention has been closed recently. Due to time con-straints it is not possible for the Commission services to extract the knowledge from the projects for EU consumption. The project that will be funded under this call should use European projects to expand the horizon regarding new relevant areas on a national or even regional level.
Formulating what is scientific advice Scientific advice was defined by the European Science Advisory Network for Health (EuSANH) as ‘recommendations for policy, based on scientific knowledge, considering also expert judgement, ethical, cultural and societal aspects, and ‘experience expertise’.
It is crucial that the advice from the researchers is presented in an appropriate way, since in the end the policy makers will take the decisions. The network EuSANH established a joint working programme on Improving Science Advice for Health - EuSANH-ISA, supported by FP7, with the general objective to improve the quality, effective-ness and efficiency of science advice for health across Europe.Their work is complementary to the work that will be done by the awarded project within the Call on health promotion and disease prevention.
Innovation union and EU 2020Innovation will be at the core of the EU2020 strategy. It will use a challenge-driven approach focussed on key challenges. The aim will be to balance upstream research and activities closer to the market so as to achieve short and medium term impact. More attention will be given to the exploitation phase, the demonstration, technology transfer, dissemination & uptake of results,… There will be support to implement European Innovation Partnerships such as a partnership on Ac-tive and Healthy Ageing which will be a centre of attention during the next years. A strategic plan is underway and will be up and running by next year. It was concluded by Mr. Mc Carthy that the topics that were presented during the PEROSH seminar should serve the DG Public Health to assess what are the needs.

3.2 Vision and expectations for research in action from the employers sideMr. Kris De Meester - Chair Health and Safety working group, Business Europe
Mr. De Meester started by introducing Business Eu-rope, which is an umbrella organisation of confedera-tions, which in turn have branch federations as their members. This implies that there is a gap between Business Europe and the actual companies.
Businesses nowadays face a multitude of challenges: Amongst others:
• Globalisation of the economy, economic crisis• Restructuring • An ageing population and labour force• Greening of the economy• A more conscious working population and the need for balance between working and private life • Demand for more flexibility from employers as well as employees. • Work relations are under pressure due to external strains on workers (restructuring, pace of work, multitude of tasks,…) • Workplace health promotion, which needs a holistic approach of workers• Skilled labour force and the education system, the shortage of people
Expectations for the research communityIn general, it is crucial to bridge the gap with businesses and business needs. The efforts should not only be targeted towards the end user such as the companies and employees but also towards people that are under the sphere of influence of companies such as the education sector, labour and social inspections, the bank and finance sector, policymakers, etc. It is crucial to make them aware of the new trends, needs and possibilities in prevention. If this does not happen, there will never be a multiplicator that is big enough to reach out for all the businesses.
Challenges for the employersMr De Meester also formulated some opportunities for improvement by the employer organisa-tions. Employer organisations should raise awareness of businesses about the opportunities for improvement, and the innovations in the field. A knowledge gap with the end users remains. The presentations of the seminar show great examples but most probably companies are not aware of the existence of these methods and tools to reduce costs, and improve the prevention strategy. Moreover, some companies do not know that certain directives are of importance for their business.
Networks and network meetings are important to share information and to increase the exchange of information. Cross-over meetings between OSH practitioners and the research community should be stimulated in order for research findings to find their way to the floor more easily.
Summary of presentations ��

�� Seminar Research in action 25/11/2010
This should also include transfer between sectors and networks that might not directly be inter-linked (e.g. research developments at NASA could be extremely useful on the work floor).It was pointed out that walls between structures need to be broken down. Trade unions and em-ployers too often discuss about the past, while they should be discussing about innovations and greening the economy to prepare businesses and workers for the challenges that lie ahead of us.
3.3 Reflections on research in action from the employees sideDr. Stefano Boy – Senior Researcher - European Trade Union Institute
Dr. Boy presented some reflections on the topic and started by mentioning the importance of immate-rial factors of prevention next to the material factors, reminding of the strong message of the Framework Directive, which advocates a broad vision on preven-tion.
Missing bridges between policy and researchThe importance of acknowledging immaterial
factors of health and safety was also shown in the 5th European Working Conditions survey that was recently launched by the European Foundation for the Improvement of Living and Working Conditions (Eurofound, http://www.eurofound.europa.eu). Key words in the survey are: high work intensity, an increase in services, an increasing proportion of workers with temporal contracts or contingent workers and job (in)security.
SubcontractingAlthough research on OSH often focuses on contingent workers and the vulnerability of these workers in terms of OSH, research should also consider the vulnerability of subcontracting of people with permanent contracts. This is for example the case in production lines with a subcon-tracting chain in a global project (e.g. engineering project). Subcontracting can lead to a lack of control between the major contractor and the different small and medium sized enterprises (SMEs) working in this chain of an overall project.
Therefore, research on OSH should take into consideration the reality of subcontracting and should aim at a critical assessment of the connection between existing employment policies and OSH. In many industries, such as the petrochemical and construction industry, an enormous amount of companies is operating under the same main contractor. A coherent approach in terms of risk as-sessment is crucial in this respect, but is all too often lacking.
Work-related mortality The European Union counts more or less 150.000 work-related deaths per year. Only 5% of these fatalities are connected to accidents at work. The majority is linked to long-term diseases. If policy intervention and research priorities focus too much on short and medium term impact, the pos-sibility to cover long-term diseases can be lost.
Musculoskeletal disorders (MSD)It was mentioned by Dr. Boy that plenty of evidence on the connection between MSD and the working environment exists. He considers that what is needed now, is an adequate transfer of research data and knowledge to policy advice. The social partners are collaborating and negotiating to include an agreement on a draft directive. There is a need for binding obligations.
Research in terms of success of the internal marketWork is changing rapidly and there is a need to take care of this evolution. More collaboration between the different dimensions, on the one hand the factory with the employers, the workers and the prevention services and on the other hand outside the factory, the authorities and experts, should be envisaged.
Companies are obliged to carry out a risk assessment, but if there is no regulation and control of the market by the authorities, the risk assessment of the companies cannot be efficient. A discon-nection between the producers and the users is often noticed. More cooperation and research on how to tackle this disconnection between the two should be done, starting from the obligation of the risk assessment of the producer and the user. Here is also a role for policymakers such as DG Employment and DG Research and for Employers and Employee organisations.
Connection between productivity and OSHProductivity can be defined in different ways and can have an impact on OSH in different ways. According to the trade unions, cost-benefit should not be linked to occupational safety and health. It is questionable to quantify the suffering of people in monetary terms. The trade unions would be happy however to discuss about cost-benefit, but on the condition that calculations are transpar-ent, all assumptions are clear and also take into account the broader assumptions such as societal assumptions etc.
Valorising the experience of the workplaceDr. Boy also stressed the importance of the valorisation of the daily experience of the workplace. Adequate tools are needed to extract knowledge from the workplace and to make sure that the workplace knowledge and voices of OSH experts within the factories are diffused beyond the factory walls. Coherent approaches to the same problems in different countries should be found. Therefore, communication skills of the preventive services are important. Data on MSD and the impact on different workers and in different countries is readily available. Nevertheless, we are at the moment not able to collate this information and to ensure we can make a link with policy intervention.ETUI is open to any discussion on non-binding measures for OSH. The possibility to move forward on some directives e.g. the MSD Directive should however not be missed. The MSD directive is an example of an holistic and long term approach instead of the short-term action on the reduction of accidents at work.
Summary of presentations ��

3.4 Governmental vision and expectations on (OSH) research and development activitiesDr. Erkki Yrjänheikki – Governmental group of the Advisory Committee on Health and Safety – Director Ministry of Social Affairs and Health, Finland
Dr. Yrjänheikki started by explaining the Finnish understanding and approach, where the term well being at work is broadly used instead of OSH. This terminology will also prevail in the new strategy for health and social affairs that is being finalised. Mea-sures to improve well being at work are discussed.
Well being at work is understood as “safe, healthy and productive work, in a well-led/managed organiza-
tion and in a good work community by competent workers who find their work meaningful and rewarding and supporting for their own life planning”.
In this view, well being leads to better safety and health for individuals, high work motivation and commitment to work, better quality of products and services, better customer satisfaction, higher productivity, better competitiveness, lower costs in losses and damages, higher savings in pay-ments and a higher national economy and social well-being.
Expectations from researchA number of basic demands and requirements apply when carrying out any kind of research. It is important to have a national research policy on OSH that can be the basis and states what are the main goals, challenges and needs for the coming periods, the emerging risks and research areas. The existence of a sector organisation on OSH research can be important to make sure that data are reliable.
Research units should be multi-professional. This entails that the units must have cross-disciplinary expertise. It goes without saying that high quality and reliability of research results are crucial.
An open collaboration between government and social partners, research organisation and the workplace is needed for relevance of results. There should be a compensation system to keep the costs of research reasonable to the workplace.
The OSH research organisations have a role in expertise support and service to the government so the latter can make elaborated decisions. This means for example support for the national strategy planning and other governmental programmes, input for new legislation and decision-making, the tools that have to be developed and the good practices available on implementation at the workplace.
�� Seminar Research in action 25/11/2010

To conclude, Dr Yrjänheikki summarised a number of focus areas that need attention in the com-ing periods such as occupational accidents and diseases, psychosocial risks and mental health, risks related to new technologies and new types of work, new kinds of exposure, scenarios on the future challenges and the cost-benefit ratio.
4. PEROSH and the transfer between research and practice Dr. Didier Baptiste – Vice-chairman, Chairman-elect PEROSH
Dr. Baptiste focused on a number of challenges for the translation of research into practice from the view of a research network.
One of the important challenges is the accessibility to the companies, depending on the size and type. Secondly, the exact identification of the problems at the workplace as well as the translation into a scien-tific question can pose a problem.
Conflicting dynamics of a company and research project should be taken into account. Where a company needs quick and practical answers, it can sometimes take two or more years for a research project to formulate a concrete solution to the workplace.
If the results are available, they should be translated into applicable and practical answers for the management and workers. This is most of the time not carried out by the same people. Besides this, other parameters, such as the political, social and economical context can influence the decision for one or the other solution. This is an iterative process.
Dr. Baptiste concluded his presentation by linking PEROSH to the topic of research in action. The PEROSH network stays in touch with what is happening in today’s workplaces. To this end the part-nership systematically shares information and builds new knowledge, for example via its 9 research projects that were developed on selected priority topics for workplaces today and in the future. Besides that, PEROSH also envisages to contribute to the next Framework Programme. A PEROSH working group on priorities for the future has recently been launched to monitor and discuss the future scenarios and challenges for the working life.
Summary of presentations ��

20 Seminar Research in action 25/11/2010

PapersScience meets Practice – driving forces behind applied OSH researchBy Dr. Dietmar Reinert, Institute for Occupational Safety and Health of the German Social Accident Insurance
1. Why does the German Social Accident Insurance conduct OSH research?
The German Social Accident Insurance is a part of Germany’s social insurance network. With a budget of €11.1 billion, it is one of the smaller branches of the social insurance system (see Fig. 1). In 2009, prevention activity accounted for 9% of expenditure, rehabilitation for 33.7%, and compensa-tion for 54.7% (1). For over a century, a small part of the prevention and rehabilitation expenditure has been invested in research into OSH and rehabilitation. Nine accident and two occupational disease clinics are maintained. These not only employ modern diagnostic and therapeutic tech-niques to international standards, but also conduct medical research. The German Social Accident Insurance conducts OSH research through three larger prevention research institutes. In addition, some €4 million is spent each year on the funding of external research projects. The accident insur-ance institutions’ research mandate is now set out in German acts and ordinances, particularly the German Social Code VII.
Research conducted by the German Social Accident Insurance is geared to practical needs in the field. It exploits findings from occupational and commuting accidents, occupational diseases and trends in work-related exposure. It is closely linked to other instruments such as regulation, train-ing, testing and certification, preventive health monitoring, curative treatment and rehabilitation, and makes use of these instruments in order to ensure that the findings are transferred swiftly and efficiently in the field (2).
In a large-scale project conducted between 2004 and 2008, the prevention services of the German Social Accident Insurance were studied with regard to their mutual influence and quality assurance. OSH research was found to be the driving force behind prevention services.
2. Research as a driving force behind the prevention services of the German Social Accident Insurance
In the research projects mentioned above, which studied the efficacy and cost-effectiveness of the industrial statutory accident insurance institutions’ prevention services, Sub-project 2 of a total of 14 sub-projects examined the mutual influences between the various prevention services. The aim was to identify not merely the different mutual influences, but also the services exerting or subject
Science meets practice - driving forces behind applied OSH research 2�

to the greatest influence upon or from other services. The mutual influences were analysed in detail with reference to three examples (noise prevention, the prevention of latex-induced allergies, and trends concerning the accident insurance of private care workers). From among the ten prevention services in total, 45 pairs of services were identified with a potential mutual influence. For each pair, the active and passive mutual influences were studied, resulting in ninety relationships in total. Esti-mates of the mutual influences for each service were made in workshops, with the involvement of all sub-project managers. In the course of these estimates, it was found that the mutual influences could be systemized both qualitatively and quantitatively. The result of the qualitative estimates is shown in Fig. 2.
Correlation analyses revealed significant correlation between the services in which people are involved. The services in question are the personal prevention services. Additional interviews with experts confirmed the correlations between the personal prevention services. They also identi-fied the reason behind these correlations, namely: the personal prevention services are generally conducted by persons with multiple functions. This group of persons is also that with the high-est number of staff in the prevention departments of the accident insurance institutions, i.e. the prevention department. In the technical prevention services, a crucial role is played by the «expert committees», which are organized on sectoral lines. Within the expert committees, which draw heavily upon the services of the accident insurance institutions’ research institutes, the technical services, encompassing certificates, accident prevention regulations, and the results of research and development, are also performed by staff with multiple functions. Analyses of the influences identi-fied the services driving innovation within the prevention network. These were generally found to originate not in the services delivered by the prevention service to companies, but in the services performed by the members of the expert committees and at the research institutes. For example, research activity conducted by the accident insurance institutions is a major driving force behind the other prevention services. The actual research results however do not find their way directly into the OSH activity conducted within companies, since the reports on the results and the scientific publications are rarely read directly by the individuals responsible for in-company OSH activity. For this to happen, transfer points are required. This function is performed primarily by consultancy, information, communication and training. Subject-matter from other services is incorporated into these services and adapted for user-friendly implementation directly within companies. The ser-vices in question are generally conducted by the prevention department of the accident insurance institutions. The function of Sub-project 12 of the research project described above was that of channelling the influential services, such as the results of research and development, more concert-edly into the transfer points.
3. Quality indicators for OSH research
A literature analysis was conducted in which the following quality criteria were identified for re-search and development projects: scientific reputation/implementation of project targets in a suit-able concept (expertise); flexible organization and completion/scope for influence by the project initiator upon its progress (co-operation); value for money/satisfaction with handling of the project (overall satisfaction); prior sectoral experience/benefit of the project in consideration of its targets
22 Seminar Research in action 25/11/2010

(relevance to the field); adherence to deadlines/appropriate time to project completion (time man-agement); and visibility in Germany and abroad/dissemination of the project results in the sector at national level (publication). The terms in brackets constitute important indicators for research projects. In order for these general quality criteria to be examined in consideration of the results of OSH research, 161 projects completed between 1999 and 2001 for the industrial statutory accident insurance institutions were analysed. The interval of several years since completion of the research projects was chosen deliberately, in order to permit evaluation of their success and effectiveness.
The analysis essentially confirmed the quality indicators found in the literature. The indicators of time management and relevance to the field were extended by the following aspects: clarity of the schedule and remit of a research project; incorporation of the results into other prevention services, in association with services and products of relevance in the field; and swift leverage of the research and development results. The indicator of expertise was extended by specific quality criteria which cannot necessarily be applied to all research projects: the adoption of new scientific approaches and topics, and holistic interdisciplinary and international management of research and develop-ment projects. For the indicator of publication, the benefit of the research and development results as a basis for other projects, for example in relation to the development of methods, was identified as a particular criterion. For the indicator of co-operation, it was found that the third-party funding of research projects generally led to more stringent project execution and clearer documentation of the results (3).
As the analysis shows, the identified quality indicators attach particular importance to the dissemi-nation and practical relevance of the OSH research. This will be illustrated below by three examples.
4. Examples of successful applied research
4.1 Working conditions in call centres
Between 2000 and 2002, a large project aimed at improving working conditions in call centres was conducted jointly by a total of 10 partners, including four universities. The project was funded by the German Federal Ministry of Labour and Social Affairs (BMA). Based upon the working conditions in call centres observed by the study, characteristic stresses and strains were examined and model measures developed for human-centric design of these new types and forms of workplace. The focus of the work lay upon the work equipment (software and hardware ergonomics) and general furnishings, the working environment (light, climate, area and acoustics), the work organization (tasks, procedures, structures), and personnel (resources, training, qualifications) (4). In over 100 call centres, characteristic strains were analysed, model concept solutions for improvements to daily working practices were implemented, and the identification of concrete design measures was evaluated. The work was supported by a targeted public information campaign whilst the project was still in progress. A website was set up at www.ccall.de and the results were published in the form of clearly structured and readable guides, reports and tools. The project was geared to sustain-ability from the outset. Eight years after the project’s completion, the site still receives some 5,000
Science meets practice - driving forces behind applied OSH research 23

visitors and a little under 2,000 document download requests each month. The hotline that was set up is still manned by three people who are able to answer enquiries.
If this successful project is considered with reference to the quality criteria stated above, the follow-ing characteristics can be demonstrated: the project initiator was involved in project management from the outset, and by the inclusion of the employees in call centres, the actual intended target group was also involved. The project design was sustainable and interdisciplinary from the outset and was used to address the topic of call centres holistically. The results of the project were trans-ferred to the field by a number of prevention services. Worthy of particular mention are consultan-cy, training, information and communication, and also surveillance. External funding necessitated strict project management and completion of the individual tasks to schedule. The results were implemented during the project or immediately following its completion. Via the website, which is still being maintained, the results are being made available both sustainably and in the long term to the affected parties and thus for application in the field.
4.2 Safe communications systems for machine guarding
Information technology entered the realm of machine guarding in the 1990s. Whereas up until that point, electronic and computer controls had to be excluded from safety-related applications, numerous research and development projects and ultimately worldwide standardization work resulted in electronics and information technology becoming established within safety engineer-ing. Demand therefore grew towards the late 1990s for communication systems to be used for safe interconnection of the individual safety-related units, particularly in more complex manufacturing systems such as those in the chemical or automotive industries. For this reason, the German Social Accident Insurance launched a project for the development of measures for safe communications systems. A survey within this area very quickly revealed that preliminary concepts were already in use in railway signalling. These concepts were transferred to the area of machine safety engineering in close consultation with the industry concerned. The idea was pursued of exploiting the standard communications systems (field buses) and their protocols for safety transmission purposes (5). A «safety layer» programmed in safe technology at the transmitter and receiver enabled safe com-munication to be achieved even over unsafe hardware. For this purpose, the standard protocols were used for transmission of the additional signals in the safety layer. Should communication be disrupted, this solution enables both the receiver and the transmitter to bring about the safe state. The underlying concept was published early at the beginning of 2000 and formulated in a standard, initially at national level. Certification procedures conducted in conjunction with all leading field bus manufacturers have resulted in this principle now being used throughout the world and in a safety function being added to all standard field bus systems.
With this project, too, it was a valuable advantage for the target group to be involved from the out-set. Implementation of the ideas in commercial products lay at the heart of the activities from the very beginning. Sustainable transfer in the field thus became the task of the product manufacturers. Once again, numerous prevention services were involved in transfer during this project: in this par-ticular case, consultancy with manufacturers, the certification of products, standardization, informa-
2� Seminar Research in action 25/11/2010

tion and communication. International co-operation was regarded as a given from the outset. Once again, the perseverance of the initiators was rewarded in this project by thorough implementation in products. Major reservations voiced at the beginning of the project had to be overcome; this was achieved by numerous workshops, conferences and publications, which generated the necessary market pressure.
4.3 Improvements to ergonomics at sewing workplaces
Industrial sewing activity may give rise to disorders of the musculoskeletal system. Possible causes are highly repetitive and in some cases one-sided stresses upon the muscular systems of the hand, arm and shoulder, and a posture with excessive forward inclination. The consequence of these stresses is a relatively high rate of unfitness for work. A number of insurers therefore approached the IFA in 2002 with the request to analyse and systematically improve the ergonomic design of sewing workplaces. A research project involving a workplace analysis was first conducted. In a holistic approach encompassing six sub-phases, prototypes of improved sewing workplaces were subsequently developed in conjunction with an engineering consultancy, an ergonomic actual/target comparison was conducted, and the results obtained from this were adapted for practical application. Analysis of the stresses was conducted in eight companies and focussed upon posture analysis by means of an adaptation of the CUELA system for hand-arm stresses, measurement of muscle activity, physical forces and the working environment (e.g. noise and lighting), and subjec-tive assessment of the stresses. The new sewing workplace designs were evaluated in four compa-nies by means of pre/post measurements. Over the six years since completion of the project, the engineering consultancy has completed an ergonomic redesign of forty workplaces. The costs are around €1,500 per workplace. Days lost owing to unfitness for work were reduced by 16% with an accompanying 15% increase in productivity. These figures result in a 100% return on investment within only a few months. The project won the 2007 European Best Practice Award in MSD Preven-tion from the European Agency for Safety and Health at Work in Bilbao (6).
This project also involved the project initiator (several accident insurance institutions) in project management from the outset. The target group was likewise involved from the outset. An inter-disciplinary and holistic project design promoted implementation in the form of the new sewing workplace. Transfer to the field was assisted by various prevention services including consultancy, training, investigation, and also information and communication. Implementation was assisted by involvement of the engineering consultancy during the project phase, and highly sustainably by the conversion of numerous sewing workplaces.
5. Summary
In this paper, three very successful examples have shown that criteria exist for the successful design of OSH projects. Facility for practical application, adherence to deadlines and also support for companies beyond the project’s completion are among the key characteristics of the successful transfer of OSH research results on the ground. Not all research projects satisfy these criteria, even at the German Social Accident Insurance. Systematic improvement of this situation was the objective
Science meets practice - driving forces behind applied OSH research 2�

of the research project referred to above. The criteria have been made part of the research manage-ment of the institutes of the German Social Accident Insurance, and have been monitored regularly since 2009.
Figure �: Direct social benefits in Germany in 200�
Figure 2: Research as a driving force behind other services
1 – Consulting, 2 – Investigation, 3 – Company medical support and guidance on safety technology,
4 – Inspection, 5 – Training, 6 – Information and communication, 7 – Accident prevention regulations,
8 – Certification, 9 – Research and development outcomes, 10 – Incentive schemes, 11 – External factors
2� Seminar Research in action 25/11/2010

6. References(1) DGUV 2008: DGUV statistics 2008. Figures and long-term trends. http://www.dguv.de/inhalt/zahlen/documents/dguvstatistiken2008e.pdf on 24.09.2010
(2) Kohstall, Thomas: Final Report. Quality in Prevention – Effectiveness and Efficiency of the Preven-tion Services of the Social Accident Insurance in Germany. http://www.dguv.de/iag/de/forschung/forschungsprojekte_archiv/qdp/qdp_abschluss/_dokumente/qdp_komplett_en.pdf on 24.09.2010
(3) Reinert, Dietmar; Eva Flaspöler: Project: «Qualität in der Prävention». Sub-project 12: «Forschun-gs- und Entwicklungsergebnisse» http://www.dguv.de/iag/de/forschung/forschungsprojekte_ar-chiv/qdp/qdp_abschluss/_dokumente/qdp_ab12.pdf on 24.09.2010
(4) Benninghoven, A.; Bindzius, F.; Cramer, J.; Ellegast, R.P.; Flowerday, U.; Genz, A.; von der Heyden, T.; Pfeiffer, W.; Schittly, D.; Schweer, R.; Stamm, R.: CCall - Healthy and Successful Work in Call-Centres. In: International Journal of Occupational Safety and Ergonomics (JOSE) 11 (2005) No. 4, pp. 409-421
(5) Reinert, D.; Schaefer, M.: Sichere Bussysteme für die Automation. Hüthig, Heidelberg 2001. ISBN: 3-7785-2797-5
(6) Ellegast, R.P.: Redesign of a sewing workplace. Work-related musculoskeletal disorders: Preven-tion report. p 45-49, Ed.: European Agency for Safety and Health at Work. European Communities
Science meets practice - driving forces behind applied OSH research 2�

2� Seminar Research in action 25/11/2010
OSH and corporate competitiveness in a global context By Dr. Guy Ahonen, Research Professor, FIOH, Finland
As the world is getting increasingly globalized, the competition among companies increases. As a result of increased global competition companies search for new means for reducing costs. It is widely assumed that competitive advantage can be gained by reducing safety and health levels of production. In a fierce competition situation also companies in highly industrialized countries tend to adopt this kind of policy. There are, however, a number of reasons for why reducing occupational safety and health levels is not a wise competition strategy.
The major corporate competition strategies are (Porter 1980, Sveiby 2001) • cost leadership• product differentiation and• knowledge (intangible assets)
From an occupational safety and health (OSH) perspective all three strategies are relevant. By reduc-ing the number of accidents and improving work well being, companies can strengthen their com-petitive position. OSH is relevant for planning the service and product portfolio of the firm. Finally, all aspects of the knowledge assets of the firm have OSH dimensions.
The cost reducing effects of OSH are well documented (Johanson et.al. 2007, Pelletier 2005, Aldana 2001, Chapman 2005, Baicker 2010). Taken together, they have a consistent message: well planned and systematically carried out OSH measures create economic returns which are 3-10 times the monetary investment. This is so, despite the difficulties to measure exactly the positive productivity effects of work. Systematic literature reviews indicate that both small-scale measures and compre-hensive OSH programs can be profitable for organisations. Finnish intervention studies show that there can be positive profitability effects even without immediate measurable productivity effects, which indicates that the economic benefit-mechanisms of OSH are more subtle than what is often assumed (Lindström et.al. 2000).
In Finland, it has for a long time been realized that multi-dimensional, comprehensive programs to simultaneously promote all aspects of work-ability and well being are most efficient. The Druvan-project is a recent example of such a program (Näsman & Ahonen 2009). The project demonstrated that even a 20-fold increase of the well being expenditure can lead to a positive return of invest-ment (see TTK 2008).
The basic economic logic of OSH measures starts from the facts that health and safety strongly af-fects the amount of productive work. Several studies show that early retirement reduces significant-ly the productive potential of highly developed countries. The OECD average is 6,3 % of GDP (Her-bertsson et.al. 2001). Recent calculations in Finland show that the annual loss of early retirement is 13% of the GDP. Some estimates are even higher (Herbertsson et.al.2001). The productive loss caused by sickness absenteeism is smaller (about 4 %) but much more observed (European founda-tion 2007). Also the hidden costs of occupational accidents are many times bigger than their direct
cost (Johanson 2007). Altogether the total cost burden of poor health and safety is enormous, and those costs will one way or the other affect the competitiveness of individual companies.Considering the economic relevance of health and safety it should be of interest to look at the in-vestments in OSH. On a macro-level the economic return of investing in health has been estimated to vary between 47% and 252% (Suhrcke et.al 2005). Attempts to estimate the total investments in work-ability and well being are scarce. In 2009 the first national estimate of magnitude of the direct investments in work well being was made in Finland (Aura et.al. 2010). It was found to be 1,9 Bill Euro. The figure becomes interesting when you consider that the total costs of non-optimal work-ing conditions are estimated to be close to 30 billion (Ibid.). It is obvious that there is under-invest-ment in work well-being.
In the industrial era the cost reducing strategy was dominating. Moving towards more knowledge intensive production and consumption (Sveiby 1997) the basis of competition has changed. Knowledge as the basis of business puts the main focus on the three main forms of intangible assets: Human Capital, including the knowledge and skills of the employees, Structural Capital, including the work community and the production processes, and Relational Capital, including the perceptions of the company held by the its relevant stakeholders, including those of the customers, suppliers and competitors (Ahonen 2008). All aspects of intangible assets are related to OSH. Safety affects directly the amount of available Human Capital. All forms of OSH activity affect the quantity, quality and effectiveness of Human Capital. Education improves skills; occupational health services increases available amounts of work, increased commitment to work increases productivity of work. Measures taken to improve corporate culture and leadership improve the productivity of work and innovation activity. Finally, all measures promoting employee satisfaction improve the employer and consumer image of the company, and therefore its economic performance.
Putting intangible assets at the heart of competition strategy has important implications for oc-cupational safety and health. The increasingly intangible nature of business and consumption emphasize responsible action. As consumers want to behave ethically, companies are compelled to demonstrate responsible conduct. The increasing role of Corporate Social Responsibility (CSR) is an expression of this (www.globalreporting.org). It is not often realized that OSH is a significant part of CSR.
To conclude: Inadequate health and safety causes enormous cost annually for the industrial coun-tries. All these costs are eventually transformed to production cost and therefore harm the com-petitiveness of companies. In the globalised, knowledge-intensive economy the role of intangible assets becomes crucial. As a consequence occupational safety and health gets a completely new meaning from an economic point of view. To promote the competitive position of highly industri-alised countries the awareness of policy- and decision-makers of all the economic aspects of OSH need to be raised.
OSH and corporate competitiveness in a global context 2�
�0 Seminar Research in action 25/11/2010
References
Ahonen, G. (2008): Inspired by Knowledge in organisations. Publications of the Swedish School of Economics and Business Administration. Nr 182. Helsinki.
Aldana, S. (2001): Financial Impact of Health Promotion Programs: A Comprehensive Review of the Literature. Am J. health Promotion, 15 (5), 296.320.
Aura, O., Ahonen, G., Ilmarinen, J. (2010): «Strategic Wellness Management in Finland - the first national survey of the management of employee well-being» Journal of Occupational and Environmental Medicine (Forthcoming).
Baicker, K., Cultler, D., Song, Z. (2010): Workplace Wellness Programs Can Generate Saving. Health Affairs, 29, no. 2 (2010): 304-311.
Chapman, L. (2005): Meta-Evaluation of Worksite Health Promotion Economic Return Studies. Art of Health Promotion Newsletter, Update.
European Foundation for the Improvement of Living and Working Conditions: Absence from work, Dublin, 2007.
Herbertsson, T., Orszag, J. (2001): The Costs of Early Retirement in the OECD. Institute of Economic Studies. Working Papers Series, WO1:2.
Johanson, U., Ahonen, G., Roslender, R (eds.) (2007): Work Health and Management Control. Thomson, Sweet & Max-well, Stockholm.
Lindström, K., Schrey, K., Ahonen, G., Kaleva,S (2000): The Effects of Promoting Organizational Health and Worker Well- Being and Organizational Effectiveness in Small and Medium-Sized Entreprises. In Murphy, R and Cooper, C: Healthy and productive Work. Taylor and Francis. London.
Näsman, O., Ahonen,G.: The DRUVAN-project: A major increase in Occupational health Services based on the Metal Age method in a Finnish municipality improved the work ability and gave significant financial return. In Kumashiro, M. (Ed): Promotion of Work Ability towards Productive Aging. Taylor & Francis, London 2009, 183-189.
Pelletier (2005): A Review and Analysis of the Clinical and Cost-Effectiveness Studies of Comprehensive Health Promotion and Disease Management Programs at the Worksite: Update VI 2000-2004. Journal of Occupational & Environmental Medicine: October 2005 - Volume 47 - Issue 10 - pp 1051-1058.
Porter, M. (1980): Competitive Strategy. Free Press. New York, NY.
Sveiby, K.E. (2001): A knowledge-base theory of the firm to guide in strategy formulation. Journal of Intellectual Capital, 2, 4, 344-358.
Sveiby, K.E. (1997): The New Organizational Wealth: Managing & Measuring Knowledge-Based Assets, Berrett-Koehler Publishers, San Francisco, CA.
Suhrcke, M. et.al. (2005): The contribution of health to the economy in the European Union. Health & Consumer Protection. Directorate- General. EU.

The Danish National Return to Work ProjectBy Glen Winzor, Head of RTW Project Division, The National Research Centre for the Working Environment, Denmark, [email protected]
The project in briefThe Danish National Return-To-Work (RTW) project is a large-scale research driven implementation project conducted in 22 Danish municipalities covering all regions in Denmark. The project builds on emerging evidence from previous published smaller Danish and international studies of RWT interventions.Particularly two comprehensive reviews of the scientific literature from The National Research Cen-tre for the Working Environment had a strong influence on the project (White paper on MSD and return to work, (NRCWE, 2008) and White paper on mental health, sickness absence and return to work (NRCWE, 2010))The study population is working-age adults, who are sick-listed for a period of at least 4 weeks. The study period is from April 1st 2010 to March 31st, 2012. The population includes employed, self-em-ployed and unemployed persons. Approximately 10,000 persons are expected to be included in the project.In agreement with the government and the social partners, the Danish Prevention Fund has granted 32.2 million EURO (240 million DKK) to the project. The grant covers the costs associated with the implementation of the project within the participating municipalities. In addition, the Dan-ish Ministry of Employment has granted 4,4 million EURO (32,5 million DKK) to finance the develop-ment, planning, administration, coordination and evaluation of the project.The main outcomes of the Danish National Return to Work Project are measures for duration of sick-ness absence, RTW-status, work ability, health related quality of life, and psychological well-being. In addition cost-benefit analyses will be conducted to assess the economic burdens and benefits of the RTW-intervention.
The interventionAt an organisational level, the intervention consists of the following elements
• Establishment of multidisciplinary RTW-organizations in sickness benefit offices• Preparatory RTW-courses for all RTW-actors• Case flow descriptions, tools and guides• Process facilitation and follow-up sessions
At an individual level, the intervention consists of the following elements• Case management /RTW-coordination• Multidisciplinary assessment• Individualized, co-ordinated and graded intervention• Education and counseling (self care, coping strategies)• Ergonomic and psychological workplace assessments and modifications
The Danish National Return to Work Project ��

�2 Seminar Research in action 25/11/2010
From research to actionTransferring the scientific research results into large-scale action has required a multi level imple-mentation effort. A prerequisite has been the backing from politicians and the social partners. Subsequently, the main implementation effort has been the comprehensive organisational change in the participating municipalities.It is argued that an intervention of this scale requires qualifications and experience among the group of researchers/project managers on at least the following areas:
• Credible knowledge about the intervention themes• Communication skills / knowledge brokering skills• Political flair• Press handling• Networking skills• Programme, portfolio and project management expertise• Strong and clear leadership• Change management• Process consultancy• Quantitative and qualitative research methodology
It is also argued that an intervention of this size requires at least the following implementation focus areas:
• Clearly communicated burning platforms• Clearly communicated visions/carrots/incentives• Dissemination of research knowledge• Removal of obstacles• Empowerment of the RTW-actors• Well-defined and clearly communicated intervention structure with point of departure in the existing structures in the municipalities• A balanced control regime• A well-planned and administrable data collection regime• Some facultative elements for the municipalities in the implementation process• Controlled room for adjustments and learning during the project period• Besides the above-mentioned elements, timing is crucial.
Future research and action resultsThe National Research Centre for the Working Environment will publish a comprehensive evalua-tion report by December 2012. Presumably the Danish government will use the results as an offset for the planning of the future RTW facilitation for sick listed persons in Denmark. It is also expected that a large number of peer-reviewed publications eventually will be published on the basis of the profound amount of data.

Improving performance and working conditions in Industrywith a focus on reduction of exposure to risk factors concerning musculoskeletal disorders
By Gu van Rhijn, Tim Bosch, TNO, The Netherlands, [email protected]
IntroductionIn various parts of the world the manufacturing companies are under a lot of pressure. Generally, customers demand a larger variety of products to be delivered at shorter time intervals than before, which may certainly not be at the cost of a lower quality or a higher price. In addition, the recent financial and economic crises put extra pressure on manufacturing industry. This all force manufacturers of (complex) products to improve the flow of production orders to-gether with a more efficient employment. The pressure on the organization is likely to increase the mental and physical stresses on the individual workers. At the same time, it is increasingly important to keep the workforce healthy and well, as there will be fewer people in the workforce due to the ageing population (e.g. de Beer and van Wissen, 1999).
In addition to the need for more efficiency, there is a need for flexibility. Automation can reduce manufacturing costs (Stahre and Vink, 2006). However, automation is most suitable for moderate or large batch sizes, and may have negative consequences for the remaining tasks. Jobs will show fewer opportunities for variation and recovery through discretionary breaks, and a larger occur-rence of short-cycle, repeated operations (Mathiassen, 2006). This might cause absenteeism but moreover presenteeism (i.e. productivity loss due to employees actually showing up for work while having disorders or experience discomfort). One aspect of flexibility concerns the growing level of customization and a shorter product lifecycle resulting in smaller batch sizes and more variety in products. In order to produce small batch sizes of varying products, production systems must be both flexible and efficient. There is no machine as flexible as a human being, which is the reason that manual handling will continue to exist (Rosecrance, et al., 2005).
Another aspect of flexibility deals with fluctuations in volume demand throughout the year. Many companies are exposed to relatively short periods of times (about one or two months), where the volume demands are significantly higher compared to the rest of the year. In some companies these periods are predictable, in other these are not. Companies have the impression that these fluctuations become more and more unpredictable. To improve flexibility there is - again - an increasing awareness of the role of the human workers. The adaptability of human workers makes them the most flexible part of the production system (Paquet and Lin, 2003).
In all these manufacturing companies it is the question how to immediately increase the output volume if the demand increases without compromising efficiency, quality, costs and workload on employees.
With regard to the workers, musculoskeletal disorders (MSD) are a major issue in terms of the economic and health burdens. In the EU, MSDs are the biggest cause of absence from work in practically all member states. In some, 40% of the costs of workers’ compensation are caused by
Improving performance and working conditions in industry ��

�� Seminar Research in action 25/11/2010
work related MSDs and up to 3% of the gross domestic product of the country itself; reducing the productivity and adding to the social costs of government (EU OSHA, 2007). Work-Related Upper Extremity Disorders (WRUED) are one of the most serious work-related health complaints in Europe (Eurostat 2010). One fifth of the work-related health problems were associated with upper extremity problems. A review of the literature by Buckle and Devereux (2002) showed 12-month prevalence among various EU countries ranging from 15 to 40%. In the Netherlands, the costs of WRUED were estimated 2.1 billion Euros per year (Blatter et al. 2006). In Europe, almost two-third of the people with WRUED experienced some or considerable limitations in normal daily activities either at work or outside of work (Eurostat 2010). These limitations are an important concern not just for worker but also for employers. Presenteeism might have catastrophic effects on a company’s performance and complementary to absenteeism lead to substantial costs. Although studies focusing on presen-teeism and musculoskeletal problems are sparse, productivity losses as a consequence of working with WRUED were considered as a main cost driver and estimated to be 808 million Euros per year in the Netherlands (Blatter et al., 2006).
One of the primary goals in participatory ergonomic processes involves the reduction of musculo-skeletal disorders by eliminating the physical and psychosocial risk factors that are associated with the disorders (e.g. Kilbom 1994; Bernard 1997; Bongers et al. 2006). Many of the physical risk factors associated with MSD are often the result of inefficient and poorly designed work practices. Other risk factors that needs attention have to do with the temporal pattern of the load during the day. Aspects of this time pattern or ‘rhythm’, like work rest schedules, task variation, cycle time, and work pace may clearly affect the worker, both mentally and physically (e.g. Bosch et al 2007). These risk factors can be evaluated and rated in occupational settings with a variety of risk assessment meth-ods as described in a recent systematical review (Takala et al. 2010). These risk assessment methods usually combine awkward postures with external loads, frequency of movement and duration of the task (e.g. CEN, 2002; ISO, 2005; De Kraker et al. 2008).
When a participatory ergonomics and a lean manufacturing process are integrated, it may be pos-sible to improve productivity and prevent injuries and illnesses to a greater extent possible than if either one is performed in isolation (Rosecrance, et al., 2005, Vink et al., 2008).In this paper two examples of integrated production improvements are described. One example concerns the change from a batch production to a mixed flow assembly system including er-gonomically designed work stations. The second example focuses on alternatives in work rest schemes to increase productivity and flexibility and to reduce fatigue. In both cases the effects in terms of both productivity, flexibility, and physical and mental loads on the workers were studied.

Case � Changing from batch to flow assembly in the production of emergency lighting devices
An (ergonomic) process innovation project was performed at a company that produces emergency lights. This company experienced a steep increase in the market demand. Due to lack of space, plans were already made for a new production facility, but the management decided to have the production systems first critically analyzed. Therefore we applied a participatory and integrative approach. Crucial elements in this are the involvement of company representatives and the integra-tion of the disciplines of ergonomics and assembly engineering. The approach includes seven steps.The first step is the initialization of a multidisciplinary working group consisting of a mixture of internal professionals (operators, middle management, process engineers, planners, line and company management) and external specialists: one assembly engineer and one ergonomist. The second and third steps involve the analysis of the assembly process and the analysis of issues (bottlenecks) with regard to the material flow and ergonomics. To give input to the working group sessions, direct observations and interviews took place addressing items like factory layout, delivery of components, availability of tools and equipment, time required to walk and search for tools and components, and physical and mental loads in assembly or transport. In the fourth step, potential alternative production systems including transportation systems are identified and subsequently evaluated in the working group on criteria like: the flow of materials, the logistics, the balancing of activities, the work content per individual, the time to learn (for new employees), the flexibility to cope with volume and product variances, and the required space and the investments. Finally, one production system is selected. In the fifth step, the selected system is designed in detail. This includes the definition of tasks, and ergonomical work station and equipment design. In the sixth step, mock-ups of workstations are built and tested. On the basis of the test results the assembly line and workstations are actually built and the new process is implemented. The final step con-cerns the evaluation of the new situation. The detailed results of each step were described by Van Rhijn et al. (Van Rhijn 2005). In this paper, we summarize the main system changes. In final assem-bly, we changed the production system from a batch-wise type of production into one-piece flow production. We integrated ergonomics in the workstation design during the process engineer-ing design. We replaced the large tables by two parallel workstations, where the large part of the required assembly steps are performed by two operators, and a third station in series, where the products are finished and packed by one operator. Inclined roller conveyors make the products glide from the first two workstations to the final one. All three work stations were ergonomically well-designed.
Measurements case �In the effect evaluation six workers, who were familiarized with the traditional and the new concept (for a period of six months at least) participated. Their general experience in assembly work ranged from 1.5 to 12.5 years. The average age of this subject group was 30.7 years (range 21 to 41 years). As both assembly concepts, the traditional and the new one, were simultaneously operative, we were able to test the subjects in both conditions and thus, to apply a within-subject design wherein the work condition (traditional vs. new) was the independent variable and the various production and human factors variables were the dependent ones.
In both conditions we measured the productivity in terms of the number of products per person
Improving performance and working conditions in industry ��

�� Seminar Research in action 25/11/2010
per day. Furthermore, we calculated the order lead-time, i.e. the duration of stay of product in the line. The required floor surface was measured including the workbench, the walking space at the work place and the material storage space at the work place. From video recordings in both condi-tions, we divided the activities into added value (assembling, mounting) and non-added value (walking, sorting, searching) activities and we calculated the time of added value activities as a percentage of the total working time. With respect to the physical load on the workers, we determined the time of occurrence of awk-ward body postures (CEN 2002, ISO 2005), the occurrence of high risk lifting situations (Waters et al., 1993) and the perceived physical load and fatigue. To measure the locally perceived discomfort (LPD) in the various body regions we used the validated LPD-method (van der Grinten 1991), where levels of discomfort are rated on a BorgCR-10 scale, ranging from 0 to 10, where 0 = no discomfort and 10 = extreme discomfort (almost maximum) and the other numbers points are also verbally anchored. In addition, we used a standardized questionnaire to evaluate the old and new situa-tion. This questionnaire addresses the following items: physical load, the mental load, the worker’s satisfaction, the health risks and the experienced fatigue.
Results case �An increase of 44% in productivity and a reduction of the order lead-time of 46% was obtained. The time that workers spent to added value activities significantly increased from 74% to 92%, without any increase in postural and experienced loads. The NIOSH equations for lifting boxes in the old and new situation showed an improved and safe way of lifting in the new situation. In the traditional situation the lifting situation was unacceptable due to the low placement (the vertical factor) of the pallets on the floor (30 cm) and the reaching (horizontal factor) before placing. In the new situation the boxes were placed on a pallet at adjustable height (70-80 cm) on a lifting table and reaching was less far. The workers experienced significantly less overall fatigue at the end of the day in the new situation.
Figure �. The work/rest schemes applied in the three conditions: traditional situation (T), the first alternative situation (A1), and the second alternative situation (A2). In A1 and A2, all breaks (except for the lunch break) were taken alternately in pairs of two operators. Also indicated are the total pause time and the total running time of the production line per shift.

Case 2 Alternative pause schemes in shaver assembly
In this case the question was of how to temporarily (in times of peak demand) increase the out-put of a line in a shaver assembly plant at Philips, which is already optimized to attain the “normal” output rate. Instead of a costly reconfiguration of the line creating extra workstations for more operators, we applied an approach of keeping the line intact, adding two extra operators, and ap-plying a scheme wherein the operators took their breaks alternately while the line kept running. For two different alternating break schemes, we compared the productivity rates, the physical load on operators, and the operators’ experiences to those of the traditional situation. 14 operators at Philips DAP took part as a subject in the experiment. They worked in a line of twelve work stations. Their task, which was repetitive and monotonous, comprised of assembling activities and technical and visual control (cycle times 12-45s).The operators were tested in three conditions. In the traditional condition (T), 12 operators were present: one for each work station. The pause scheme comprised a lunch break of 30 minutes and 4 short breaks over the day (figure 1). The operators took all breaks group-wise. In the first alternative condition (A1), 14 operators were present in the same line of 12 work stations. They took their lunch break all together, but the short breaks were taken alternately in couples of two. During the time periods that none of the fourteen workers had a break, the two extra opera-tors did some cleaning, supplying or giving some help elsewhere. The second alternative (A2) was similar to the first, except for an extra (fifth) break in the second half of the shift. The total pause time per day for each operator was 70, 80 and 85 minutes in T, A1 and A2, respec-tively. The total time that the line was not running was 70 minutes in T and only 30 minutes in A1 and A2 (Figure 1). All operators were exposed to each condition during two weeks. In the second week the measurements took place.
Figure 2 The average level (across participants) of discomfort in the neck and shoulder region during the day in the various conditions. Each point in the graph reflects a measuring point; all these measuring points took place just before or directly after each break.
Improving performance and working conditions in industry ��

�� Seminar Research in action 25/11/2010
Measurements case 2The productivity of the line was expressed as the number of products per day. In addition, the mean productivity of the operators in the first evaluation was determined by dividing the line out-put by the number of operators. In the second evaluation, the productivity was monitored for each individual worker.The physical load on workers was expressed as the level of locally perceived discomfort (LPD) using a Borg CR-10 rating scale in the various body regions (e.g. hands, lower arms, upper arms, neck, the high, middle and low region of the back, the buttocks, upper legs, lower legs and feet) indicated on a body map (van der Grinten, 1991). Other individual experiences were addressed in a question-naire at the end of the tests.
Results case 2The detailed results were described by de Looze and co-authors (de Looze et al., 2010a). For the alternating pause schemes the line productivity was significantly higher as compared to the tradi-tional pause scheme: A1 and A2 resulted in a 12 and 16% higher output, respectively. There were no significant differences in line output between A1 and A2. The productivity per operator per shift was not significantly different across conditions, despite the longer total pause times in A1 and A2. The local levels of discomfort were found to increase significantly during the day only in the neck and shoulder region. This increase, which was most pronounced in condition T and A1, is shown in Figure 2. The discomfort level at the end of the shift in scheme A2 was significantly lower compared to A1, whereas the time integral of discomfort over the shift in scheme A2 was significantly lower compared to the traditional condition T.A majority of the operators entitled this alternating break scheme as ‘pleasant’ (90%), but wanted the scheme to be applied only during the periods of peak demand because of social aspects (80%).
Conclusions and discussionIn case 1 the change of the production concept in combination with some ergonomic work place modifications resulted in some clear effects. There appeared to be no need for the company to invest in factory expansion. On the same factory area, it appeared to be possible to produce about twice as much when applying the new assembly concept. In addition, we observed a significant reduction in order lead time (46%) and a significant gain with respect to productivity (44%). The detailed costs and benefits of these interventions are described in de Looze et al. (2010b). This gain in productivity is partly based on an increase in the percentage of time that is spent on added-value activities.
This shift towards more added value assembly work did not lead to a clear increase in the physical or mental loads on the workers. Instead, we observed a decrease in the occurrence of stressful lift-ing activities and a decreased overall fatigue at the end of the day.One remaining point to discuss concerns the increased time percentage of direct work. Some argue that such development (also addressed as work intensification) may well increase the risk for musculoskeletal injury (Winkel et al. 2002). Also, monotonous work in the production industry has been associated with more health problems in the upper extremities and elevated sick leave rates (Johansson et al 1994, Olafsdottir et al. 1998, Parenmark et al. 1993). The theory behind this is that the long periods of time of monotonous assembling activities without interruption of other kinds of

(indirect) activity, give body structures not enough opportunities to recover during the day (Winkel et al. 2002). At higher percentages of direct work, the need for some kind of variation interrupting the assembly work so now and then, thus increases.
This variation and interruption was studied in case 2, the alternative pause schemes. It appeared that an increase in volume flexibility can be achieved by adding two extra workers and applying an alternating work rest scheme, and thus, without a costly reconfiguration of the line. Two extra workers and the implementation of an alternating work/rest scheme resulted in a 12–16% higher line output. Simultaneously, the operators experienced less physical load on their neck and shoulders, particularly in the alternating scheme with the highest number of breaks and highest total break time;
This alternating work/rest scheme is recommended only during time periods of peak demand (up to 2 months) because of social aspects. In this alternating work rest scheme the workers have a break in couples while in the traditional rest schemes they have a break together with the whole team. The Hawthorne effect, a form of reactivity whereby participants improve an aspect of their behaviour being experimentally measured simply in response to the fact that they are being stud-ied (Landsberger, 1958), might have influenced the results in the current study. However, produc-tivity results were collected over a two week period without being known by the operators. Other measures were compared in a within subject design at the end of each condition so if any effect existed it might be small and probably occurred in all conditions.
Finally, we would like to discuss two issues with regard to these two cases.Firstly, these two cases are examples of improvements of both productivity and working conditions by innovations in production systems, workstation and organisation. Traditionally, most companies focus either on technological innovations or on the organizational structures or on enhancing hu-man resources. The best performance however, will be realized when all three factors are involved. Corporate success can be enhanced by balancing technological, organizational and human factors in the production process (Vink et al, 1996). A recent paper by Dul and Neumann (2009) confirmed the importance of health and performance measurements. Managers usually associate ergonomics with occupational health and not with business performance. The focus of human factors should be linked to business strategies and the management world. Secondly, these two cases are examples of experimental studies in which effects were determined in short periods of time and with small sample sizes. We acknowledge that the described Haw-thorne could occur. From these studies focus on risk factors of MSD. However no direct link to MSD could be determined.
With regard to the musculoskeletal disorders (MSD) a recent overview of longitudinal studies by Bongers and colleagues (Bongers et al 2006) indicated that perceived stress and high demands in combination with low control at work are often related to neck and upper limb symptoms. Further-more, several factors like individual characteristics (age, gender etc.), motivation, work experience and skills might affect the relationships between exposure, responses and disorders. To reduce the risk of MSD requires an integrated approach consisting of a combination of interventions on organi-sational, workstation and individual level. Further research is needed to assess the effects of these interventions on both productivity and MSD reduction.
Improving performance and working conditions in industry ��

�0 Seminar Research in action 25/11/2010
References
Beer, de J. and van Wissen, L., (1999). Europe: One Continent, Different Worlds. Population Scenarios for the 21st Century. Kluwer Academic Publishers (Dordrecht 1999).
Bernard, P. (1997). Musculoskeletal Disorders and Workplace Factors: A Critical Review of Epidemiologic Evi-dence for Work-related Musculoskeletal Disorders of the Neck, Upper Extremity and Low Back (Cincinnati, Ohio: NIOSH).
Blatter, B., Houtman I., Van den Bossche S, Kraan K and Van den Heuvel, S.; Gezondheidsschade en kosten ten gevolge van RSI en psychosociale arbeidsbelasting in Nederland, The Hague, 2006.
Bongers, P.M., IJmker, S., van den Heuvel, S. and Blatter, B.M. (2006). Epidemiology of work related neck and upper limb problems: Psychosocial and personal risk factors (Part I) and effective interventions from a bio behavioural perspective (Part II). Journal of Occupational Rehabilitation, 16 (3), 272-295.
Bosch T., Looze, M.P. de, Dieën, J.H. van. Development of fatigue and discomfort in the upper trapezius muscle during light manual work. Ergonomics 2007;50(2):161-177.
CEN (2002). CEN, EN 1005-3. Safety of Machinery—Human Physical Performance—Part 3: Recommended Force Limits for Machinery Operation (2002).
Das, B. (1999). Development of a comprehensive industrial work design model. Human Factors and Ergono-mics in Manufacturing, 9(4), 393– 411.
Dul, J. and Neumann, P.W.. Ergonomics contributions to company strategies. Applied Ergonomics, 40 (4), 745-752
Eurostat (2010). Health and safety at work in Europe (1999-2007): A statistical portret. Luxembourg: Publications Office of the European Union
ISO (2005). ISO, ISO/DIS 11228-3. Safety of Machinery—Human Physical Performance—Part 5: Risk Assessment for Repetitive Handling at High Frequency (2005).
Johansson, J.Å. and Nonås, K., 1994, Psychosocial and physical working conditions ans associated musculos-keletal symptoms among operators in five plants using arc welding in robot stations. International Journal of Human Factors in Manufactoring, 4(2) 191-204.
Kilbom, Ǻ ., (1994). Repetitive work of the upper extremity Part II: the scientific basis (knowledge base) for the guide. International Journal of Industrial Ergonomics, 14, 59–86.
Kraker de H. and Douwes M. (2008). The development of a practical tool for risk assessment of manual work - the ‘HAT-tool’. In: Helgadóttir B, Ed. NES 2008 Abstracts: Ergonomics is a lifestyle. Reykjavik: Gutenberg, 190.
Landsberger, HA. Hawthorne Revisited. Ithaca: Cornell University Press; 1958
Looze, M.P. de, Bosch,T., Rhijn, J.W. van. Increasing short-term output in assembly work. Human Factors and Ergonomics in Manufacturing & Service Industries 20 (5) 470–477
Looze, M.P. de, Vink, P., Koningsveld, E.A. P., Kuijt-Evers, L., & Van Rhijn, J. W. (2010). Cost-effectiveness of ergono-
mic interventions in production. Human Factors and Ergonomics in Manufacturing&Service Industries, 20(4), 316–323.
Mathiassen, S.E. (2006). Diversity and variation in biomechanical exposure: what is it, and why would we like to know? Applied Ergonomics, 37, 419–427
Ólafsdóttir, H. & Rafnsson, V., 1998, Increase in musculoskeletal symptoms of upper limbs among women after introduction of the flow-line in fish-fillet plants. International Journal of Industrial Ergonomics , 21, 69-77.
Paquet, V. and Lin, L. (2003). An Integrated Methodology for Manufacturing Systems Design Using Manual and Computer Simulation, Human Factors and Ergonomics in Manufacturing, 13(1), 19–40.
Parenmark, G., Malmkvist, A.K. & Örtengren, R. ,1993, Ergonomic moves in an engineering industry: Effects on sick leave frequency, labor turnover and productivity. International Journal of Industrial Ergonomics , 11, 291-300.
Rosecrance, J., Douphrate, D. and Cross, S. (2005). Integration of Participatory Ergonomics and Lean Manufac-turing: A Model and Case Study. Human Factors in Organizational Design and Management - VIII, Edited by P. Carayon, M. Robertson, B. Kleiner and P.L.T. Hoonakker. IEA Press, Santa Monica, California, USA, 437 - 442.
Stahre J., Vink P. (2006). The future of intelligent manufacturing systems and human factors. In: Pikaar RN, Koningsveld EAP, Settels PJM, Eds. Meeting Diversity in Ergonomics. Proceedings IEA2006 Congress. Oxford: Elsevier. CD-rom: art0526.
Takala E.P., Pehkonen I, Forsman M., Hansson G.A., Mathiassen S.E, Neumann WP, Sjøgaard G, Veiersted KB, Westgaard RH, Winkel J., 2010. Systematic evaluation of observational methods assessing biomechanical expo-sures at work. Scand J Work Environ Health. 36 (1), 3-24.
Van Der Grinten, M.P., 1991, Test-retest reliability of a practical method for measuring body part discomfort. In Designing for Everyone, volume 1, Y. Que´innec and F. Daniellou (Eds.), London: Taylor and Francis, 54–57.
Van Rhijn, J.W., de Looze, M.P., Tuinzaad, G.H., Groenesteijn, L. , de Groot, M.S. and Vink, P. (2005). Changing from batch to flow assembly in the production of emergency lighting devices. International Journal for Production Research, 43, 3687-3701.
Vink, P. Rhijn, G. van, Dhondt, S. and J. Dul (1996): Ten times better: improving technological, organisational and human factors in companies. In O. Brown, H.W. Hendrick (Eds): Human Factors in Organisational Design and Management-V. Elsevier, A’dam.
Vink, P, van Rhijn, G. and Krassi, B. (2008) Collaborative design using mixed reality: suggestions from INTUITION partners In: Karwowski W, Salvendy G, Eds. Conference Proceedings, 2nd International Conference on Applied Human Factors and Ergonomics, AHFE 2008, 14-17 July 2008, Las Vegas, USA. Louisville: AHFE International, CD Rom.
Waters, TR, Putz-Anderson, V, Garg, A, Fine, LJ., 1993. Revised NIOSH equation for the design and evaluation of manual lifting tasks. Ergonomics, 36 (7) 749-776.
Winkel, J., Forsman, M., Kazmierczak, K., Kjellberg, A., Mathiassen, S.E., Neumann, P.W., and Wells, R.P., 2002, Ergonomic intervention for occuspational musculoskeletal health in manufacturing industry – trends, tools and processes. In:. Humans in a Complex Environment., Proc. 34th Congress of NES, pp 833-835, Linkopings University, Sweden.
Improving performance and working conditions in industry ��

�2 Seminar Research in action 25/11/2010
Enhancing mental health of employees working long hours through flexible time arrangementsBy Dr. Dorota Zolnierczyk-Zreda, PhD, Central Institute for Labour Protection-National Research Institute
One of the most consistent findings of the four EWCS’ over the last 15 years is the relative intensifi-cation of the pace of work (Burchell, et al., 2009). According to same resource, since 1991 there has been a clear trend in Europe towards a reduction in paid working hours. However this trend slowed down in 2005 when the New Member States working longer hours joined the EU in 2004. The return of the long hours culture is now being observed in many European countries, e.g. in the Netherlands, the number of reported overtime hours has increased substantially (from 4 hours to 6 hours) over the period from 2003 to 2007 (Bakhuys Roozenboom, et al. 2008). As the Trade Union in the United Kingdom announced in June 2008, the incidence of long working hours had increased among UK workers from 2007 to 2008 and “after a decade of progress, the battle against the long hours culture has stalled” (http://www.tuc.org.uk/extras/longhoursreturn.pdf ). Poland is the second top country of the EU-25, where weekly working time exceeds 48 hours (ESWC, 2007). The existing research clearly shows that the outcomes of long working hours are deterioration in both physical and mental health (Sparks et al., 1996; van der Hulst, 2003; Taris & all., 2007; for reviews). Long work hours and overtime have been found to be associated with adverse physical health problems, such as cardiovascular and musculoskeletal problems, immunological impair-ments, depression and anxiety. It has also been shown that overtime has an adverse effect on worker lifestyle, lack of physical activity and enough sleep or improper diet (van der Hulst, 2003). Working long hours impose a threat for ability to fulfill familiar duties and other personal goals. Work-life balance problems are widely recognized as connected to long working hours, and the amount of time that is occupied by the job is one of the most obvious antecedents of Work-Family Imbalance (Geurts & Demerouti, 2003; Harma, 2006).Flextime arrangements or worktime control is commonly regarded as an organisational practice to enhance worker’s health. Flextime arrangements can generally be divided into two schedules. Ac-cording to one schedule employees are allowed to decide when to start and end time of work on a day-to-day basis, and when to take a brake but not allowed for variations in the length of the daily work schedule (Costa et al., 2001). The second type of flextime allow for a much broader variability of working time, even in the length of the working day or working week. High worktime control has been found to be related to a lower cholesterol level (Thomas & Gangs-ter, 1995), fewer physical symptoms as well as lower levels of distress and burnout, (Galinsky, Bond & Friedman, 1996; Jansen & Nachreiner, 2004). On the other hand, low worktime control has been shown to increase the risks of subjective ill-health and sickness absence, especially among women. Ala-Marsula et al. (2005) in their prospective study on 16 139 public sector employees who had no medically certified sickness absence in the year proceeding the survey, have found that control over working time moderates the effects of work strain and effort-reward imbalance. However, longitudinal studies exploring the link between worktime control and health are still very rare, particularly in workers working long hours. Despite substantial practical interest, the evidence base linking flexibility to health-related outcomes is still relatively weak. The aim of the present study was to examine the potential role of flexible working time on different health dimensions such as: somatic complaints, anxiety, social dysfunction and depression. It has

been also attempted in the study to answer the question which age and gender group of em-ployees working long hours do benefit form flexible worktime the most.The data for this study came from 309 Polish employees performing clerical work for more than 8 hours daily with longitudinal data resulting from having completed the questionnaires in both 2008 and 2009. The sample was composed of 159 men and 150 women. The average age was 41,3 (SD=5,7).Perceived flexibility was measured as the ability to decide when a worker starts and finishes his/her work and whether he/she can decide when to make a break during his/her work. Mental health was diagnosed with the Polish version of The General Health Questionnaire-28 (Goldberg & Williams, 1991) Both the total indicator of the scale and the indicators of the four subscales were taken into account. These were: somatic complaints, anxiety and insomnia, social functioning and depression. The longitudinal effects of changes in flexibility on health-related outcomes were investigated by fitting a series of linear regression models. Each change score outcome (health dimensions) was regressed on variables reflecting change in perceived flexibility and covariates (age and gender). In order to compare the influence of flexibility on different age and gender groups a series of ANO-VA’ were performed, where age, gender, flexibility and their interaction were independent variables, and changes in health dimensions were dependent variables. The three following age categories were analyzed: 1- age 18-29, 2 – age 30-39, 3 – age 40-60.The results have shown that increased worktime flexibility was associated with decreased overall indicator of health complaints, in particular with decreased somatic complaints and social dys-function. Moreover, it has also been found that worktime flexibility had a significant influence on decreased depression in the youngest group of female workers aged 18-29. The results of this prospective study indicate that individuals whose flexibility increased showed favorable improvements in two health-related outcomes: less somatic complaints, and less social dysfunction. The result related to decreased somatic complaints as a consequence of flexibility is consistent with studies showing that long, rigid working hours are associated with less time for re-covery and difficulties to unwind after work and may result in serious health consequences (Geurts & Sonnentag, 2006, for review). The result showing decreased social dysfunction as a consequence of flexibility is in line with stu-dies showing that long weekly work hours are associated with higher levels of work-family imbalan-ce across time (Geurts & Sonnentag, 2006; Jansen & Nechreiner, 2004) and with difficulties to fulfill social commitments (Costa et all., 2006). In the present study, it has also been shown that flexibility was the most beneficial for mental health of the youngest woman working long hours. This outcome corroborate and extend the Ala-Mursula and colleagues’ findings showing that control over worktime reduces the adverse effect of work stress on sickness absence especially among female employees (Ala-Mursula et all., 2005).
ConclusionsEven in the presence of objectively existing psychosocial risks, such as long working hours, pro-grams that promote worktime flexibility may have beneficial effect for workers’ mental health. Thus, providing employees with worktime control may promote health in strenuous work life. Men and woman are not homogenous groups on matters related to workplace flexibility. Female workers, especially in the youngest age group, seem to need flexible time arrangements even more than men in terms of preserving their mental health in the long run and maintain it until a delayed retirement age.
Enhancing mental health of employees working long hours through flexible time arrangements ��

�� Seminar Research in action 25/11/2010
ReferencesAla-Marsula, L., Vahtera, J., Linna, A.., Pentti, J., & Kivimaki, M. (2005). Employee worktime control moderates the effects of work strain and effort-reward imbalance on sickness absence: The 10-town study. Journal of Epide-miology and Community Health, 59(10), 851-857.
Bakhuys Roozenboom, M , Gouw, P., Hooftman, W., Houtman, I. and Klein Hesselink, D.J. Arbobalans 2007-2008, Hoofddorp, TNO Kwaliteit van Leven, 2008
Burchell, B., Cartron, D., Csizmadia, P., Delcampe, S., Gollac, M., Illéssy, M., Lorenz, E., Makó, C., O’Brien, C., Valeyre, A. (2009). Working conditions in the European Union: Working time and work intensity, Luxembourg: Office for Official Publications of the European Communities
Costa, G.T., Akerstedt, F., Nachreiner, F., Baltieri, S., Folkard, Frings-Dresen, et al., (2001). Flexible Work Hours, Health and Well-Being in the European Union: Preliminary Data from a Saltsa Project
Costa, G., Sartori, S., Akerstedt, F., (2006). Influence of flexibility and variability of working hours on health and well-being. Chronobiology International,23(6). 1125-1137.
Third European Survey on Working Conditions, (2007). Dublin: European Foundation for the Improvement of Living and Working Conditions
Fifteen years of working conditions in the EU: charting the trends, Dublin: European Foundation for the Impro-vement of Living and Working Conditions
Galinsky, E., Bond, J.T. & Friedman, D.E. (1996). The role of employers in addressing the needs of employed parents. Journal of Social Issues, 52, 111-136.
Geurts, S.A.E. & Demerouti, E. (2003). Work/nonwork interference: A review of Theories and Findings, in M. Scha-bracq, J. Winnubst and C.I. Cooper (eds), Handbook of Work and Health Psychology. Wiley & Sons, Chichester, pp. 279-312.
Geurts, S.A.E. and Sonnentag, S. (2006). Recovery as an explanatory mechanism in the chronic health impair-ment. Scandinavian Journal of Work, Environment & Health, 32, 482-492.
Goldberg, D.P. & Williams, P. (1991). A user guide to the General Health Questionnaire. Berkshire: NFER-NELSON, 28(4), 915-21.
Harma, M. (2006). Workhours in relation to work stress, recovery and health. Scandinavian Journal of Work, Environment & Health, 32, 502-514.
Jansen, D. & Nachreiner, F. (2004). Health and psychosocial effects of flexible working hours. Revista de Saude Publica, 38(Suppl.), 11-18.
Sparks, K. Cooper, C., Fried, Y. i Shirom, A. (1997). The effects of hours of work on health: A meta-analytic review. Journal of Occupational and Organizational Psychology, 70, 391-408.
Taris, T., W., Beckers, D., G., J.,, Dahlgren, A., Geurts, S.A.E. & Tucker, P. (2007). Overtime work and well-being: Preva-lence, conceptualization and effects of working overtime. In S. McIntyre & J. Houdmont (Eds.), Occupational health psychology: European perspective on research, education and practice: Vol.2. Maia (POR): ISMAI.
Thomas, L.T. & Gangster, D.C. (1995). Impact of family-supportive work variables on work-family conflict and strain: A control perspective. Journal of Applied Psychology, 80, 6-15.
Van der Hulst, M. (2003). Long hours and health. Scandinavian Journal of Work, Environment