Embed Size (px)
Citation preview

Sedation, Analgesia and Paralysis in ICU
Mazen Kherallah, MD, FCCP

ICU Sedation
• ICU sedation is a complex clinical problem
• Current therapeutic approaches all have potential adverse side effects
• Agitated patients are often hypertensive, increase stress hormones, and require more intensive nursing care

The Need for Sedation
• Anxiety
• Pain
• Acute confusional status
• Mechanical ventilation
• Treatment or diagnostic procedures
• Psychological response to stress

• Patient comfort and • Control of pain• Anxiolysis and amnesia• Blunting adverse autonomic and
hemodynamic responses• Facilitate nursing management• Facilitate mechanical ventilation• Avoid self-extubation• Reduce oxygen consumption
Goals of sedation in the ICU

Characteristics of an ideal sedation agents for the ICU
• Lack of respiratory depression• Analgesia, especially for surgical patients• Rapid onset, titratable, with a short
elimination half-time• Sedation with ease of orientation and
arousability• Anxiolytic• Hemodynamic stability

The Challenges of ICU Sedation
• Assessment of sedation
• Altered pharmacology
• Tolerance
• Delayed emergence
• Withdrawal
• Drug interaction

Sedation
SedativesCauses for Agitation

Undersedation
Sedatives
Causes for AgitationAgitation & anxietyPain and discomfortCatheter displacementInadequate ventilationHypertensionTachycardiaArrhythmiasMyocardial ischemiaWound disruptionPatient injury

Oversedation
Sedatives
Causes for Agitation
Prolonged sedationDelayed emergenceRespiratory depressionHypotensionBradycardiaIncreased protein breakdownMuscle atrophyVenous stasisPressure injuryLoss of patient-staff interactionIncreased cost

Correctable Causes of Agitation
• Full bladder• Uncomfortable bed position• Inadequate ventilator flow rates• Mental illness• Uremia• Drug side effects• Disorientation• Sleep deprivation• Noise• Inability to communicate

Causes of Agitation Not to be Overlooked
• Hypoxia• Hypercarbia• Hypoglycemia• Endotracheal tube malposition• Pneumothorax• Myocardial ischemia• Abdominal pain• Drug and alcohol withdrawal

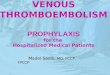
Altered PharmacologyMidazolam and Age
00.5
11.5
22.5
33.5
44.5
5
10 20 30 40 50 60 70 80
Age (y)
T 1 / 2
hou
rs
Harper et al. Br J Anesth, 1985;57:866-871

Delayed Emergence
• Overdose (prolonged infusion)– pK derived from healthy patients– Drug interaction– Individual variation
• Delayed elimination– Liver (Cp450)– Kidney dysfunction– Active metabolites

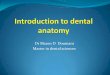
Morphine Metobolism
M orp h in e -3 -GA n tian a lg es ic
N orm orp h in eN eu ro toxic ity
M orp h in e -6 -GA n a lg es ic (4 0 X )
M orp h in eTyp e t it le h e re
80% 10%

Withdrawal
• Withdrawal from preoperative drugs
• Sudden cessation of sedation– Return of underlying agitation
• Hyperadrenergic syndrome– Hypertension, tachycardia,sweating
• Opioid withdrawal– Salivation, yawning, diarrhea

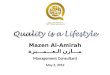
Drug InteractionsDiazepam-Morphine Interaction
Synergism
Antagonism
Morphine
Diazepam
ED50 isobologramRighting reflexIn rats
Kissin et al. Anesthesiology. 1989, 70:689-694

Strategies for Patient Comfort
• Set treatment goal
• Quantitate sedation and pain
• Choose the right medication
• Use combined infusion
• Reevaluate need
• Treat withdrawal

Set Treatment Goal
Sedation Analgesia
Amnesia AnxiolysisHypnosis
Patient Comfort

Quantitate Sedation & Analgesia
• Subjective measure
• Objective measures

Sedation Scoring Scales
• Ramsay Sedation Scale (RSS)
• Sedation-agitation Scale (SAS)
• Observers Assessment of Alertness/Sedation Scale (OAASS)
• Motor Activity Assessment Scale (MAAS)
BMJ 1974;2:656-659Crit Care Med 1999;27:1325-1329J Clin Psychopharmacol 1990;10:244-251Crit Care Med 1999;27:1271-1275

The Ramsay Scale
Scale Description
1 Anxious and agitated or restless, or both
2 Cooperative, oriented, and tranquil
3 Response to commands only
4 Brisk response to light glabellar tap or loud auditory stimulus
5 Sluggish response to light glabellar tap or loud auditory stimulus
6 No response to light glabellar tap or loud auditory stimulus

The Riker Sedation-Agitation ScaleScore Description Definition
7 Dangerous agitation Pulling at endotracheal tube, trying to strike at staff, thrashing side to side
6 Very agitated Does not calm despite frequent verbal commands, biting ETT
5 Agitated Anxious or mildly agitated, attempting to sit
4 Calm and cooperative
Calm, awakens easily, follows commands
3 Sedated Difficult to arouse, awakens to verbal stimuli, follows simple commands
2 Very sedated Arouse to physical stimuli, but does not communicate spontaneously
1 Unarousable Minimal or no response to noxious stimuli

The Motor Activity Assessment Scale
Score Description Definition
6 Dangerous agitation Pulling at endotracheal tube, trying to strike at staff, thrashing side to side
5 Agitated Does not calm despite frequent verbal commands, biting ETT
4 Restless and cooperative
Anxious or mildly agitated, attempting to sit
3 Calm and cooperative
Calm, awakens easily, follows commands
2 Responsive to touch or name
Opens eyes or raises eyebrows or turns head when touched or name is loudly spoken
1 Responsive only to noxious stimuli
Opens eyes or raises eyebrows or turns head with noxious stimuli
0 Unresponsive Does not move with noxious stimuli

What Sedation Scales Do
• Provide a semiquantitative “score”
• Standardize treatment endpoints
• Allow review of efficacy of sedation
• Facilitate sedation studies
• Help to avoid oversedation

What Sedation Scales Don’t Do
• Assess anxiety
• Assess pain
• Assess sedation in paralyzed patients
• Predict outcome
• Agree with each other

BIS Monitoring

BIS Monitoring

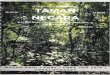
BIS Range Guidelines
Awake
Responds to loud commands or mild prodding/shaking
Low probability to explicit recallsUnresponsive to verbal stimuli
Burst suppression
Flat line EEG
Responds to normal voice Axiolysis
Moderatesedation
Deep Sedation
100
80
60
40
20
0
BIS

Pain
Assess Pain Separately

Visual Pain Scales
0 1 2 3 4 5 6 7 8 9 10
No pain Worst possible pain

Signs of Pain
• Hypertension
• Tachycardia
• Lacrimation
• Sweating
• Pupillary dilation

Principles of Pain Management• Anticipate pain• Recognize pain
– Ask the patient– Look for signs– Find the source
• Quantify pain • Treat:
– Quantify the patient’s perception of pain– Correct the cause where possible– Give appropriate analgesics regularly as required
• Remember, most sedative agents do not provide analgesia• Reassess

Nonpharmacologic Interventions
• Proper position of the patient
• Stabilization of fractures
• Elimination of irritating stimulation
• Proper positioning of the ventilator tubing to avoid traction on endotracheal tube

Choose the Right Drug
• Benzodiazepines
• Propofol
• Opioids-2 agonists

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
Benzodiazepines

Benzodiazepines
Onset Peaks Duration
Diazepam 2-5 min 5-30 min >20 hr
Midazolam 2-3 min 5-10 min 30-120 min
Lorazepam 5-20 min 30 min 10-20 hr

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
Propofol

Propofol
Onset Peaks Duration
Propofol 30-60 sec 2-5 min short

Propofol Dosing
• 3-5 g/kg/min antiemetic
• 5-20 g/kg/min anxiolytic
• 20-50 g/kg/min sedative hypnotic
• >100 g/kg/min anesthetic

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
Opioids

Pharmacology of Selected Analgesics
Agent Dose (iv) Half-life Metabolic pathway Active metabolites
Fentanyl 200 g 1.5-6 hr Oxidation None
Hydromorphone 1.5 mg 2-3 hr Glucuronidation None
Morphine 10 mg 3-7 hr Glucuronidation Yes (Sedation in RF)
Meperidine 75-100 mg
3-4 hr Demethylation & hydroxylation
Yes (neuroexcitation in RF)
Codeine 120 mg 3 hr Demethylation & Glucuronidation
Yes ( analgesia, sedation)
Remifentanil 3-10 min Plasma esterase None
Keterolac 2.4-8.6 hr Renal None

Opioids
Lipid Solubility
Histamine Release
Potency
Morphine +/- +++ 1
Hydromorphone + + 5
Fentanyl +++ - 50

Opioids
Onset Peaks Duration
Morphine 2 min 20 min 2-7 hr
Fentanyl 30 sec 5-15 min 30-60 min

Problems with Current Sedative Agents
Midazolam Propofol Opioids
Prolonged weaning X - X
Respiratory depression X - X
Severe hypotension X X -
Tolerance X - X
Hyperlipidemia - X -
Increased infection - X -
Constipation - - X
Lack of orientation and cooperation
X X X

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
-2 agonists

Alpha-2 Receptors
Brain(locus ceruleus)
Spinal Cord
Peripheral vasculature
SedationAnxiolysis
Sympatholysis
Analgesia
Vasoconstriction

DEX: Dosing
Loading infusion0.25-1 g/kg(10-20 min)
Maintenance infusion0.2-0.7 g/kg/hr

Use Continuous and Combined Infusion
Plasma Level
Load
Maintenance

Repeated Bolus
Plasma levels

Opioid + Hypnotic Infusion
Fentanyl + Midazolam or Propofol
Analgesia AmnesiaAnxiolysisHypnosis

Continuous Infusion Regimens
Fentanyl 25-250 g/h
Midazolam 0.5-5 mg/hr
Propofol 15-50 g/kg/min

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
-2 agonistsPrimary
Adjunct sedation Propofol

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
-2 agonistsPrimary
Adjunct sedation Midazolam

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
-2 agonistsPrimary
Adjunct analgesia Morphine

Choose the Right Drug
Sedation Analgesia
Amnesia AnxiolysisHypnosis
-2 agonistsPrimary
Adjunct analgesia Fentanyl

Reassess Need
• Use sedation score as endpoint
• Initiate sedation incrementally to desired level
• Periodically (q day) titrate infusion rate down until the patient begins to emerge
• Gradually increase infusion rate again to desired level of sedation
Barr, Donner. Crit Care Clin. 1995;11827

Treat Withdrawal
• Acute management– Resume sedation– Beta-blockade, dexmedetomidine
• Prolonged management– Methadone 5-10 mg VT bid– Clonidine 0.1-0.2 mg VT q8h– Lorazepam 1-2 mg IV q8h