Embed Size (px)
Citation preview
Approach of Infected patient Approach of Infected patient in Critical Care Unitin Critical Care Unit
Mazen Kherallah, MD, FCCPMazen Kherallah, MD, FCCP
Consultant, Infectious Disease & Critical Consultant, Infectious Disease & Critical Care Care Chairman, Critical Care Chairman, Critical Care
DepartmentDepartmentKing Faisal Specialist Hospital & Research King Faisal Specialist Hospital & Research
CenterCenter

1. What Sepsis Syndrome are we 1. What Sepsis Syndrome are we
Dealing with?Dealing with?
InfectionInfection SepsisSepsis Severe sepsisSevere sepsis Septic shockSeptic shock Multi-organ system failureMulti-organ system failure
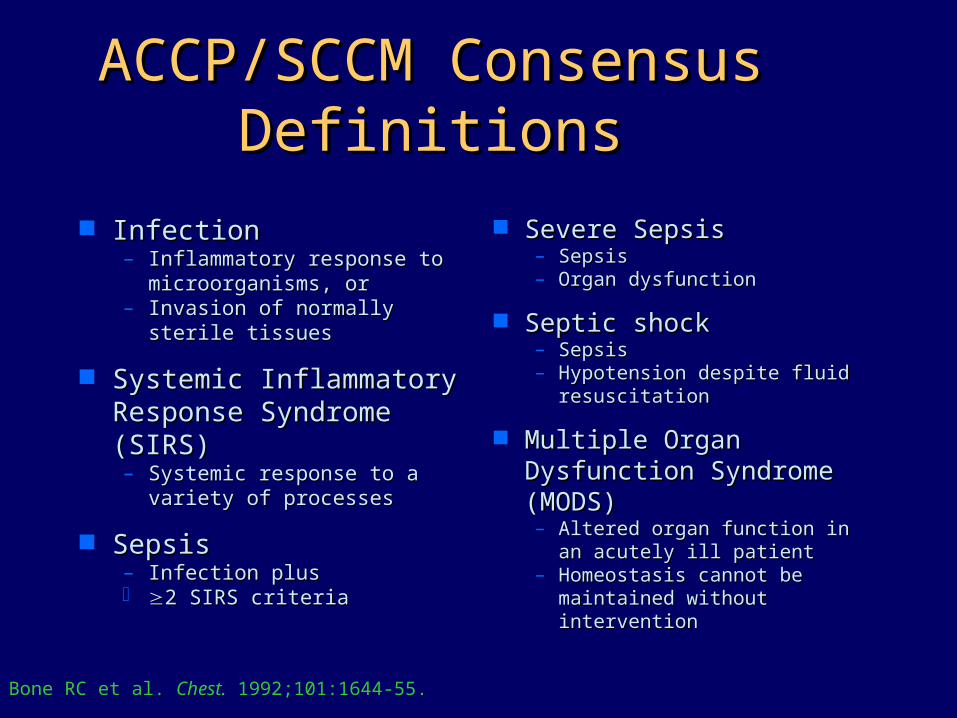
ACCP/SCCM Consensus ACCP/SCCM Consensus DefinitionsDefinitions
InfectionInfection– Inflammatory response to Inflammatory response to
microorganisms, ormicroorganisms, or– Invasion of normally sterile Invasion of normally sterile
tissuestissues
Systemic Inflammatory Systemic Inflammatory Response Syndrome Response Syndrome (SIRS)(SIRS)– Systemic response to a Systemic response to a
variety of processesvariety of processes
SepsisSepsis– Infection plusInfection plus 2 SIRS criteria2 SIRS criteria
Severe SepsisSevere Sepsis– SepsisSepsis– Organ dysfunctionOrgan dysfunction
Septic shockSeptic shock– SepsisSepsis– Hypotension despite fluid Hypotension despite fluid
resuscitationresuscitation
Multiple Organ Multiple Organ Dysfunction Syndrome Dysfunction Syndrome (MODS)(MODS)– Altered organ function in an Altered organ function in an
acutely ill patientacutely ill patient– Homeostasis cannot be Homeostasis cannot be
maintained without maintained without interventionintervention
Bone RC et al. Chest. 1992;101:1644-55.
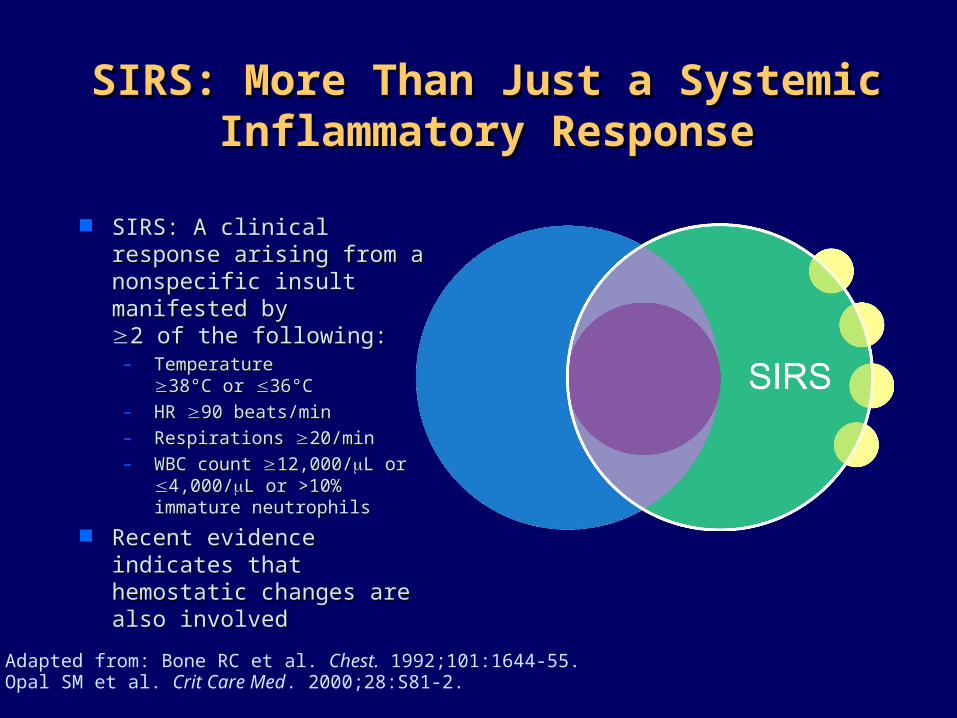
SIRS: More Than Just a Systemic SIRS: More Than Just a Systemic Inflammatory ResponseInflammatory Response
SIRS: A clinical response SIRS: A clinical response arising from a nonspecific arising from a nonspecific insult manifested by insult manifested by 2 of the following:2 of the following:– Temperature Temperature
38°C or 38°C or 36°C36°C– HR HR 90 beats/min90 beats/min– Respirations Respirations 20/min20/min– WBC count WBC count 12,000/12,000/L or L or
4,000/4,000/L or >10% L or >10% immature neutrophilsimmature neutrophils
Recent evidence Recent evidence indicates that hemostatic indicates that hemostatic changes are also changes are also involvedinvolved
Adapted from: Bone RC et al. Chest. 1992;101:1644-55.Opal SM et al. Crit Care Med. 2000;28:S81-2.

Severe Sepsis: Acute Organ Severe Sepsis: Acute Organ Dysfunction and Disordered Dysfunction and Disordered
HemostasisHemostasis
Severe Sepsis: Severe Sepsis: Sepsis with signs of Sepsis with signs of organ dysfunction in organ dysfunction in 1 of the following 1 of the following systems: systems: – CardiovascularCardiovascular– RenalRenal– RespiratoryRespiratory– HepaticHepatic– HemostasisHemostasis– CNSCNS– Unexplained metabolic Unexplained metabolic
acidosisacidosis
Adapted from: Bone RC et al. Chest. 1992;101:1644-55.
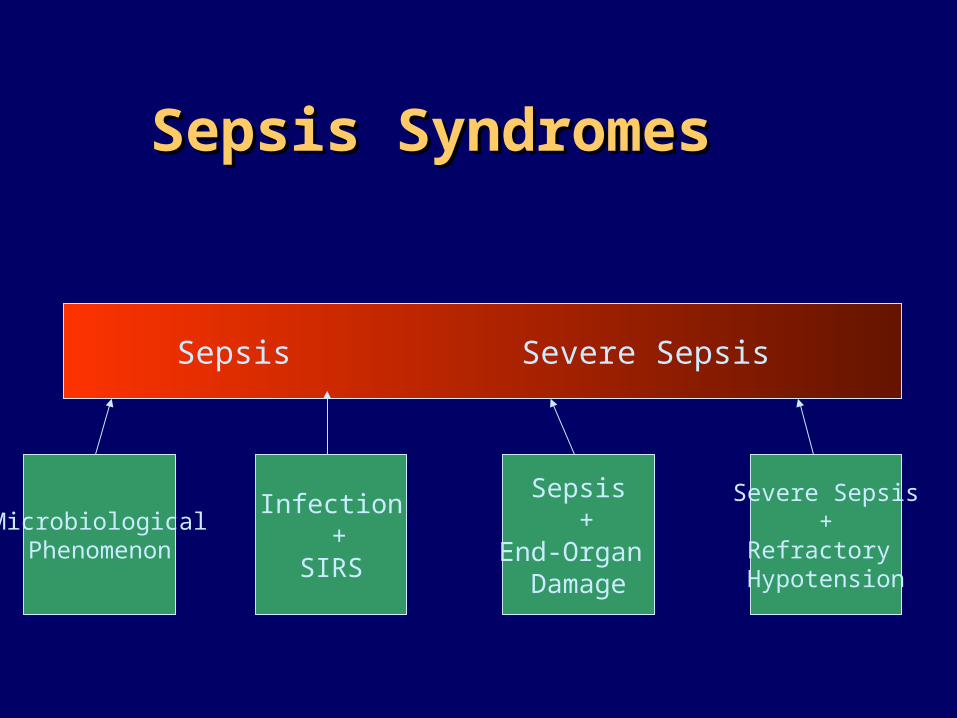
Sepsis SyndromesSepsis Syndromes
Infection Sepsis Severe Sepsis Septic Shock
MicrobiologicalPhenomenon
Infection +
SIRS
Sepsis +
End-Organ Damage
Severe Sepsis+
Refractory Hypotension
Sepsis Parameters:Sepsis Parameters:
Leukocytosis with left shiftLeukocytosis with left shift Bandemia Bandemia Toxic granulationToxic granulation Elevated sed. RateElevated sed. Rate C- reactive proteinC- reactive protein Acute phase reactant: fibrinogen, Acute phase reactant: fibrinogen,
haptoglobin,..haptoglobin,.. IL1, IL6, IL8IL1, IL6, IL8
2. Organ Localization of 2. Organ Localization of infection infection
SkinSkin Soft tissueSoft tissue CNSCNS Upper airwayUpper airway Lower airwayLower airway Head and neckHead and neck MediastinalMediastinal GI GI LiverLiver
Biliary tractBiliary tract Intra-abdominalIntra-abdominal Bones and jointsBones and joints Urinary tractUrinary tract Genital tractGenital tract Blood stream Blood stream
infectioninfection SystemicSystemic
3. Tissue Localization of 3. Tissue Localization of InfectionInfection
Skin and soft tissue:Skin and soft tissue:– Superficial epidermal layers Superficial epidermal layers
(impetigo)(impetigo)– Deeper epidermal layers Deeper epidermal layers
(Icthyma)(Icthyma)– Superficial subcutaneous: Superficial subcutaneous:
ErysipelasErysipelas– Deeper subcut.: cellulitisDeeper subcut.: cellulitis– FolliculitisFolliculitis– HydradenitisHydradenitis– Fascia: FasciitisFascia: Fasciitis– Fat: panuculitisFat: panuculitis
Lower respiratory Lower respiratory tract:tract:– Alveolar: Alveolar:
consolidative consolidative pneumoniapneumonia
– Interstitial: Interstitial: atypical atypical pneumoniapneumonia
– Pleural: empyemaPleural: empyema
4. Suspected Microbiology 4. Suspected Microbiology of Infectionof Infection
Host factorsHost factors– ImmunosuppressioImmunosuppressio
nn– AgeAge– GenderGender– Previous antibioticsPrevious antibiotics– Co-morbidity:Co-morbidity:
SSDSSD DMDM CGDCGD
EnvironmentalEnvironmental– Community:Community:
contactscontacts TravelTravel AnimalsAnimals
– Hospital:Hospital: LocationLocation
– Nursing homesNursing homes
4. Suspected Microbiology 4. Suspected Microbiology of Infectionof Infection
Community Community acquired acquired pneumonia: Lobar pneumonia: Lobar pneumoniapneumonia– Streptococcus Pn.Streptococcus Pn.– H. fluH. flu– Moraxella Moraxella
catarrhaliscatarrhalis– StaphylococcalStaphylococcal– KlebsiellaKlebsiella
Community Community acquired acquired pneumonia: pneumonia: interstitial:interstitial:– Mycoplasma Pn.Mycoplasma Pn.– LegionellaLegionella– ViralViral
4. Suspected Microbiology 4. Suspected Microbiology of Infectionof Infection
Intra-abdominal Intra-abdominal infectioninfection– E. coliE. coli– KlebsiellaKlebsiella– B. fragilisB. fragilis– EnterococcusEnterococcus– CandidaCandida
Urinary tract Urinary tract infectioninfection– E. coliE. coli– ProteusProteus– EnterococcusEnterococcus
4. Suspected Microbiology 4. Suspected Microbiology of Infectionof Infection
Meningitis: <1 Meningitis: <1 month:month:– Group B strep Group B strep
49%49%– E. Coli 18%E. Coli 18%– Listeria 7%Listeria 7%– Gram neg. 10%Gram neg. 10%
Meningitis: 1 mo-Meningitis: 1 mo-50 yrs:50 yrs:– S. pneumoniaeS. pneumoniae– MeningococciMeningococci– H. flu (very rare)H. flu (very rare)
5. Surgical Indication:5. Surgical Indication:
Foreign body: central line infectionForeign body: central line infection Prosthesis: PVE, Prosthetic infectionProsthesis: PVE, Prosthetic infection Sequestration: chronic osteomyelitisSequestration: chronic osteomyelitis Gangrene: wet gangreneGangrene: wet gangrene Obstructed normal draining procedure: Obstructed normal draining procedure:
cholecystitischolecystitis No penetration for antibiotics: No penetration for antibiotics:
empyema, abscessempyema, abscess
5. Empiric Treatment5. Empiric Treatment
Appropriate Appropriate coveragecoverage
Adequate dose: Adequate dose: MIC, MBC MIC, MBC
Appropriate routeAppropriate route
AbsorptionAbsorption PenetrationPenetration Tissue levelTissue level Cellular levelCellular level
4. Suspected Microbiology 4. Suspected Microbiology of Infectionof Infection
Meningitis: <1 Meningitis: <1 month:month:– Group B strep Group B strep
49%49%– E. Coli 18%E. Coli 18%– Listeria 7%Listeria 7%– Gram neg. 10%Gram neg. 10%
Ampicillin+CefotaAmpicillin+Cefotaximexime
Meningitis: 1 mo-Meningitis: 1 mo-50 yrs:50 yrs:– S. pneumoniaeS. pneumoniae– MeningococciMeningococci– H. flu (very rare)H. flu (very rare)
Vancomycin+CeftVancomycin+Ceftriaxone or riaxone or cefotaximecefotaxime
Empiric Treatment: Intra-Empiric Treatment: Intra-abdominal Infectionabdominal Infection
E. coli, KlebsiellaE. coli, Klebsiella– Amp/sulbactamAmp/sulbactam– Piperacillin/tazobactamPiperacillin/tazobactam– Ticarcillin/clavaulinateTicarcillin/clavaulinate– AztreonamAztreonam– ImipenemImipenem– CefazolinCefazolin– CefuroximeCefuroxime– CeftriaxoneCeftriaxone– CiprofloxacinCiprofloxacin
B. FragilisB. Fragilis– Amp/sulbactamAmp/sulbactam– Piperacillin/tazobactamPiperacillin/tazobactam– Ticarcillin/clavaulinateTicarcillin/clavaulinate– ImipenemImipenem– CefoxitinCefoxitin– ClindamycinClindamycin– MetronidazoleMetronidazole– ChloramphonicoleChloramphonicole
IntroductionIntroductionFever Work-UpFever Work-Up
Automatic set orderAutomatic set order Repeated several times within 24 Repeated several times within 24
hourshours Time consumingTime consuming CostlyCostly Disruptive and patient’s discomfortDisruptive and patient’s discomfort Considerable blood lossConsiderable blood loss Unneeded radiationUnneeded radiation
Practice ParametersPractice ParametersGoalsGoals
Rational consumption of Rational consumption of resourcesresources
Efficient evaluationEfficient evaluation
The Search for the The Search for the Underlying Cause of Underlying Cause of
Fever?Fever?
What temperature should elicit an What temperature should elicit an evaluation?evaluation?
When are blood cultures warrantedWhen are blood cultures warranted When should intravascular catheters be When should intravascular catheters be
cultured or removedcultured or removed When are cultures of respiratory When are cultures of respiratory
secretions, urine, stool, or CSF warrantedsecretions, urine, stool, or CSF warranted When are radiological studies warrantedWhen are radiological studies warranted
Initiating Fever EvaluationInitiating Fever EvaluationDefinition of FeverDefinition of Fever
Arbitrary: core temperature Arbitrary: core temperature >38.0°C, or two consecutive >38.0°C, or two consecutive elevation of > 38.3°Celevation of > 38.3°C
The lower the temperature that is The lower the temperature that is used to define fever, the more used to define fever, the more sensitive and less specific the sensitive and less specific the indicator is for detecting an indicator is for detecting an infectious etiologyinfectious etiology
Initiating Fever EvaluationInitiating Fever Evaluation Normal Body TemperatureNormal Body Temperature
Normal body temperature is Normal body temperature is 37.0°C37.0°C
Varies by 0.5°C to 1°C according to Varies by 0.5°C to 1°C according to circadian rhythm and menstrual circadian rhythm and menstrual cyclecycle
Exercise can increase temperature Exercise can increase temperature by 2°C to 3°Cby 2°C to 3°C
Initiating Fever EvaluationInitiating Fever Evaluation Variation of Temperature in ICUVariation of Temperature in ICU
Specialized mattressesSpecialized mattresses Hot lightsHot lights Air conditioningAir conditioning Cardiopulmonary bypassCardiopulmonary bypass Peritoneal lavagePeritoneal lavage Dialysis and continuous hemofiltrationDialysis and continuous hemofiltration Drugs altering thermoregulatory Drugs altering thermoregulatory
mechanismsmechanisms
Initiating Fever EvaluationInitiating Fever Evaluation Non-infectious Causes of Fever can be Life-Non-infectious Causes of Fever can be Life-
threateningthreatening
Adrenal insufficiencyAdrenal insufficiency Thyroid stormThyroid storm Malignant hyperthermiaMalignant hyperthermia Heat strokeHeat stroke
Initiating Fever EvaluationInitiating Fever Evaluation Infected Patient but AfebrileInfected Patient but Afebrile
ElderlyElderly Open abdominal woundsOpen abdominal wounds Large burnsLarge burns Extracorporeal membrane Extracorporeal membrane
oxygenationoxygenation Patients taking anti-inflammatory Patients taking anti-inflammatory
or anti-pyretic drugsor anti-pyretic drugs
Initiating Fever EvaluationInitiating Fever Evaluation Temperature MeasurementTemperature Measurement
Most accurately measured using Most accurately measured using intravascular or bladder thermistorintravascular or bladder thermistor
Mouth, rectal or external auditory Mouth, rectal or external auditory measurements using electronic measurements using electronic probes is acceptable in appropriate probes is acceptable in appropriate patientspatients
Axillary measurements should not Axillary measurements should not be used be used
Initiating Fever EvaluationInitiating Fever Evaluation Clinical EvaluationClinical Evaluation
A new onset of temperature to or A new onset of temperature to or above 38.3C is reasonable trigger for above 38.3C is reasonable trigger for a clinical assessment but not a clinical assessment but not necessarily a laboratory or necessarily a laboratory or radiological evaluationradiological evaluation
Clinical assessment may reveal a Clinical assessment may reveal a purulent wound or phlebitic leg, then purulent wound or phlebitic leg, then diagnosis and therapy for that diagnosis and therapy for that infectious process should commenceinfectious process should commence

Bacterial Synergistic Bacterial Synergistic GangreneGangrene
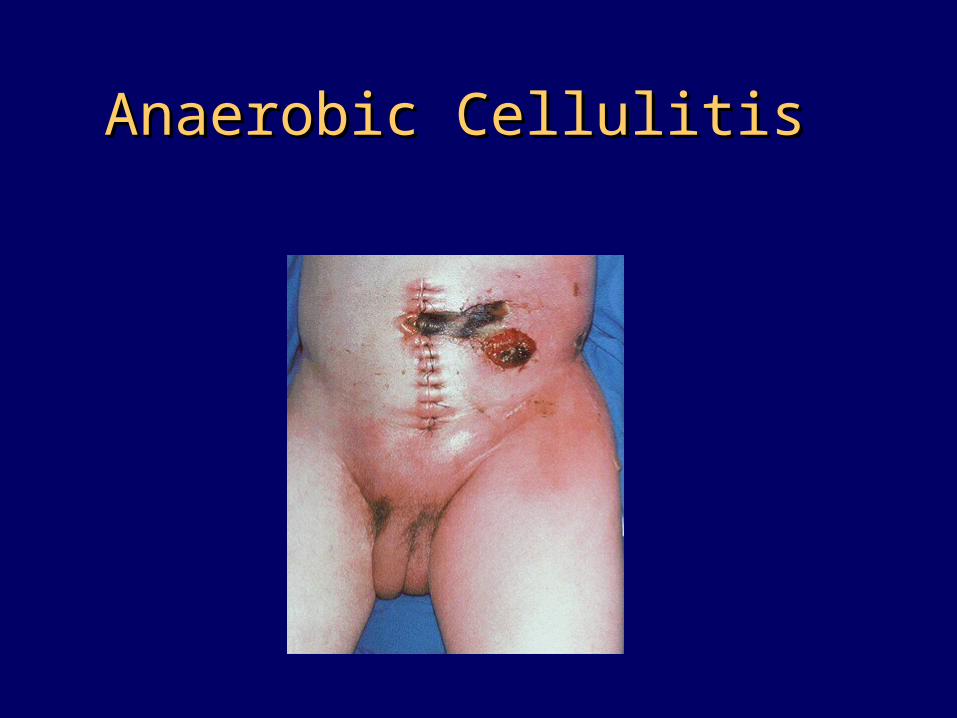
Anaerobic CellulitisAnaerobic Cellulitis
Initiating Fever EvaluationInitiating Fever Evaluation Obtaining Blood CulturesObtaining Blood Cultures
Skin PreperationSkin Preperation
The site of venipunture should be cleaned The site of venipunture should be cleaned with either 10% povidone iodine or 1-2% with either 10% povidone iodine or 1-2% tincture of iodine. If the patient is allergic to tincture of iodine. If the patient is allergic to iodine alcohol 70% swabs should be usediodine alcohol 70% swabs should be used
The access to intravascular device and to the The access to intravascular device and to the stopper on the culture bottle should be stopper on the culture bottle should be cleaned with 70% alcoholcleaned with 70% alcohol
Iodophors must be allowed to dry to provide Iodophors must be allowed to dry to provide maximal antiseptic activitymaximal antiseptic activity
Initiating Fever EvaluationInitiating Fever Evaluation Obtaining Blood CulturesObtaining Blood Cultures
Blood VolumeBlood Volume
One blood culture is defined as a One blood culture is defined as a sample of blood drawn at a single time sample of blood drawn at a single time at a single siteat a single site
One milliliter of blood is needed per five One milliliter of blood is needed per five milliliter of mediamilliliter of media
5 ml of blood is injected into each of 5 ml of blood is injected into each of two or three bottles for routine blood two or three bottles for routine blood culture culture
10-15 ml per one set of blood cultre10-15 ml per one set of blood cultre
Initiating Fever EvaluationInitiating Fever Evaluation Obtaining Blood CulturesObtaining Blood Cultures
Number of Cultures & SitesNumber of Cultures & Sites
Two cultures 10 minutes apart after the Two cultures 10 minutes apart after the onset of fever. Culture should not be onset of fever. Culture should not be repeated till 24 hours passedrepeated till 24 hours passed
Each culture should be drawn by separate Each culture should be drawn by separate venipuncturevenipuncture
One culture can be obtained from the One culture can be obtained from the most recently inserted catheter in case most recently inserted catheter in case venipuncture is difficult (the second B/C venipuncture is difficult (the second B/C from a venipuncture site)from a venipuncture site)
Initiating Fever EvaluationInitiating Fever EvaluationCXR & SputumCXR & Sputum
Chest x-ray in an erect sitting Chest x-ray in an erect sitting position during deep inspirationposition during deep inspiration
The absence of infiltrates, masses The absence of infiltrates, masses or effusion does not exclude or effusion does not exclude pneumonia, abscess or empyemapneumonia, abscess or empyema
Respiratory secretion obtained by Respiratory secretion obtained by suctioned or expectorated sputum suctioned or expectorated sputum is adequate for initial evaluationis adequate for initial evaluation
Initiating Fever EvaluationInitiating Fever EvaluationUrinalysis and Urine CultureUrinalysis and Urine Culture
Obtain urine for culture and for Obtain urine for culture and for determination of the presence of pyuriadetermination of the presence of pyuria
Patients who have Foley catheter in place Patients who have Foley catheter in place should have urine collected from the urine should have urine collected from the urine port of the catheter and not from the port of the catheter and not from the drainage bagdrainage bag
Urine should be transported to the laboratory Urine should be transported to the laboratory rapidly to avoid bacterial multiplication, rapidly to avoid bacterial multiplication, otherwise should be refrigeratedotherwise should be refrigerated

Initiating Fever EvaluationInitiating Fever EvaluationStool ExaminationStool Examination
Mandatory when more than 2 stools per day Mandatory when more than 2 stools per day conform to the container in which they are placed conform to the container in which they are placed in a patient at risk for C-difficilein a patient at risk for C-difficile
Stool should be sent for WBC or lactoferrin latex Stool should be sent for WBC or lactoferrin latex agglutination testagglutination test
Stool should be sent for c-diff assay for at least 2 Stool should be sent for c-diff assay for at least 2 times in 24 hourstimes in 24 hours
Stool should not be sent for other enteric pathogens Stool should not be sent for other enteric pathogens unless the patient is HIV or present to the hospital unless the patient is HIV or present to the hospital with diarrheawith diarrhea
Infectious Causes of FeverInfectious Causes of Fever
Catheter-related InfectionsCatheter-related Infections ICU acquired PneumoniaICU acquired Pneumonia Urinary Tract InfectionUrinary Tract Infection Pseudomembraneous colitisPseudomembraneous colitis Wound InfectionWound Infection SinusitisSinusitis Acaculous cholecystitisAcaculous cholecystitis
Vascular Devices & feverVascular Devices & fever
Localized infectionLocalized infection– Exit site infectionExit site infection– Tunnel infectionTunnel infection
Systemic infectionSystemic infection Allergic reactionAllergic reaction
Relative Risks of CR-BSIRelative Risks of CR-BSI Duration of catheter in placeDuration of catheter in place Anatomic site of insertionAnatomic site of insertion Type of the device:Type of the device:
– Catheter compositionCatheter composition– A-Line, Central line, Hickman’s catheterA-Line, Central line, Hickman’s catheter– Regular vs antibiotic-impregnated catheterRegular vs antibiotic-impregnated catheter
Patient populationPatient population Techniques used in insertion and maintenanceTechniques used in insertion and maintenance Frequency of manipulationFrequency of manipulation
Duration of Catheter UseDuration of Catheter UseOptimal Time for Catheter Removal?Optimal Time for Catheter Removal?
The incidence of CR-BSI is directly The incidence of CR-BSI is directly proportional to the length of time proportional to the length of time the catheter is usedthe catheter is used
The risk that any catheter may The risk that any catheter may cause CR-BSI is low if the catheter cause CR-BSI is low if the catheter is removed within 3 daysis removed within 3 days
The optimal time for catheter The optimal time for catheter removal is unknownremoval is unknown
Anatomic Site of InsertionAnatomic Site of InsertionIncidence of Catheter Colonization: Incidence of Catheter Colonization:
Kemp and associatesKemp and associates
Femoral line: 36%Femoral line: 36% Internal jugular: 17%Internal jugular: 17% Subclavian: 5%Subclavian: 5%
Type of the DeviceType of the DeviceRisk of CR-BSIRisk of CR-BSI
Short-term noncuffed central Short-term noncuffed central venous catheters: 5-10 cases per venous catheters: 5-10 cases per 1000 catheter days1000 catheter days
Peripheral IV catheter: less than Peripheral IV catheter: less than 0.2 cases per 1000 catheter days0.2 cases per 1000 catheter days
Permanent surgically implanted Permanent surgically implanted central device: 2 bacteremias per central device: 2 bacteremias per 1000 catheter days1000 catheter days
Catheter Related InfectionsCatheter Related InfectionsDefinitionsDefinitions
Colonized CatheterColonized Catheter
Positive culture from the catheter tip or Positive culture from the catheter tip or intracutaneous segment without evidence intracutaneous segment without evidence of systemic infectionof systemic infection
Semiquantitative culture of 15 or more CFU Semiquantitative culture of 15 or more CFU is used to consider culture as positiveis used to consider culture as positive
Values of less than 15 CFU are regarded as Values of less than 15 CFU are regarded as negative culture, contaminant, or negative culture, contaminant, or insignificant infection requiring no therapyinsignificant infection requiring no therapy
Catheter Related InfectionsCatheter Related InfectionsDefinitionsDefinitions
Catheter-Related Bloodstream InfectionCatheter-Related Bloodstream Infection
A positive catheter culture A positive catheter culture 15 CFU 15 CFU with concomitant positive blood culturewith concomitant positive blood culture
A quantitative blood culture drawn A quantitative blood culture drawn from the catheter shows marked step-from the catheter shows marked step-up in concentration of organisms (ten-up in concentration of organisms (ten-fold or greater) as compared with fold or greater) as compared with peripherally drawn quantitative blood peripherally drawn quantitative blood cultureculture
No other identifiable source of infectionNo other identifiable source of infection
Catheter Related InfectionsCatheter Related InfectionsDefinitionsDefinitions
Infusate-Related Bloodstream InfectionInfusate-Related Bloodstream Infection
Isolation of the same organism Isolation of the same organism from the infusate and from from the infusate and from separate percutaneous peripheral separate percutaneous peripheral blood cultureblood culture
No other identifiable source of No other identifiable source of infection infection
Catheter Related InfectionsCatheter Related InfectionsDefinitionsDefinitions
Local Catheter-Related InfectionLocal Catheter-Related Infection
Growth of 15 or more CFU from a Growth of 15 or more CFU from a catheter specimen by catheter specimen by semiquantitative culturesemiquantitative culture
Local signs of inflammation: Local signs of inflammation: erythema, swelling, tenderness, erythema, swelling, tenderness, purulent materialpurulent material
Negative peripheral blood cultureNegative peripheral blood culture
When the Catheter Should be When the Catheter Should be Removed in a Febrile Patient?Removed in a Febrile Patient?
No other identifiable SourceNo other identifiable Source
For stable patients with fever, there is For stable patients with fever, there is no necessity to remove or change all no necessity to remove or change all indwelling catheters unless CR-BSI or indwelling catheters unless CR-BSI or Local infection is documentedLocal infection is documented
If patients are in shock, manifest If patients are in shock, manifest peripheral embolization, DIC or ARDS, peripheral embolization, DIC or ARDS, removal of all intravascular catheters removal of all intravascular catheters and reinsertion at new sites is and reinsertion at new sites is indicated.indicated.
Pulmonary Infections & Pulmonary Infections & FeverFever
Diagnostic StrategiesDiagnostic Strategies
Empirical strategy based only on Empirical strategy based only on clinical evaluationclinical evaluation
Invasive strategy based on fiberoptic Invasive strategy based on fiberoptic bronchoscopy and quantitative cultures bronchoscopy and quantitative cultures of distal uncontaminated pulmonary of distal uncontaminated pulmonary secretionssecretions
Intermediate strategy based on Intermediate strategy based on quantitative culture of quantitative culture of nonbronchoscopic samplenonbronchoscopic sample
Diagnostic Strategy based Diagnostic Strategy based on Clinical Evaluation onlyon Clinical Evaluation only
Fever, cough, sputum production, new Fever, cough, sputum production, new pulmonary infiltrate and elevated pulmonary infiltrate and elevated leukocyte count.leukocyte count.
May not be present in the hospitalized May not be present in the hospitalized patients with nosocomial pneumoniapatients with nosocomial pneumonia
May be present but may not be caused May be present but may not be caused by pneumonia: CHF, ARDS, atelectasisby pneumonia: CHF, ARDS, atelectasis
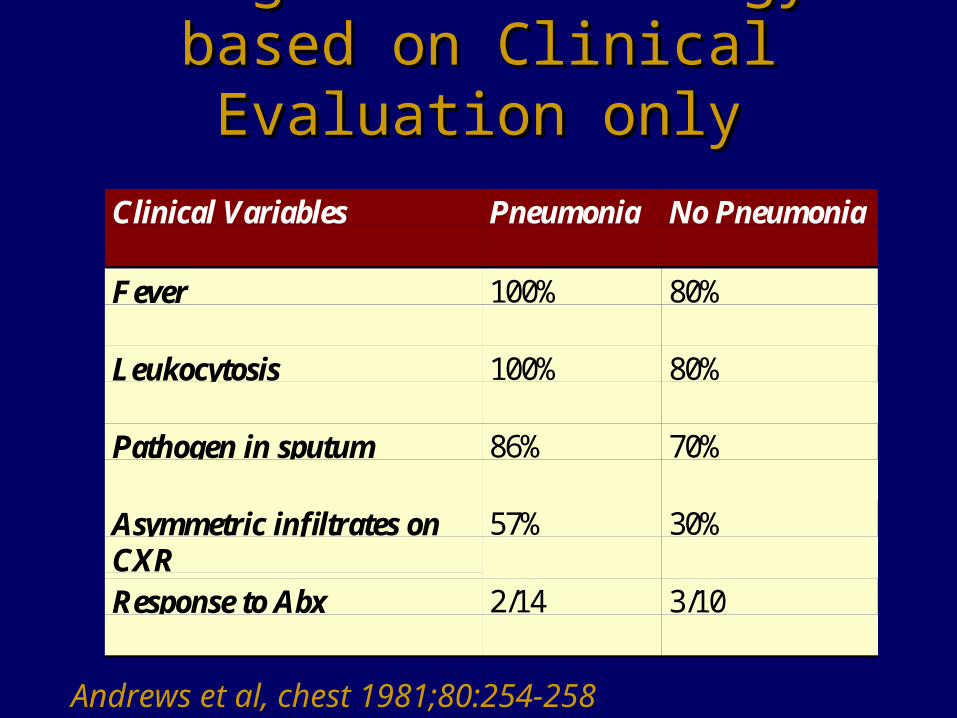
Diagnostic Strategy based Diagnostic Strategy based on Clinical Evaluation onlyon Clinical Evaluation only
Clinical Variables Pneumonia No Pneumonia
Fever 100% 80%
Leukocytosis 100% 80%
Pathogen in sputum 86% 70%
Asymmetric infiltrates onCXR
57% 30%
Response to Abx 2/14 3/10
Andrews et al, chest 1981;80:254-258
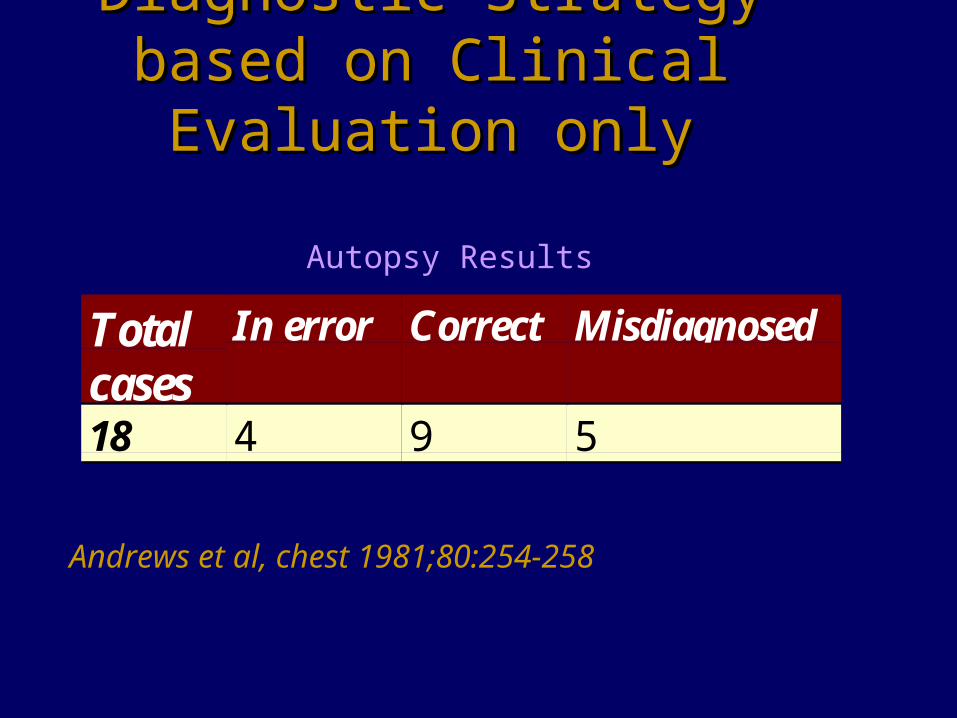
Diagnostic Strategy based Diagnostic Strategy based on Clinical Evaluation onlyon Clinical Evaluation only
Totalcases
In error Correct Misdiagnosed
18 4 9 5
Andrews et al, chest 1981;80:254-258
Autopsy Results
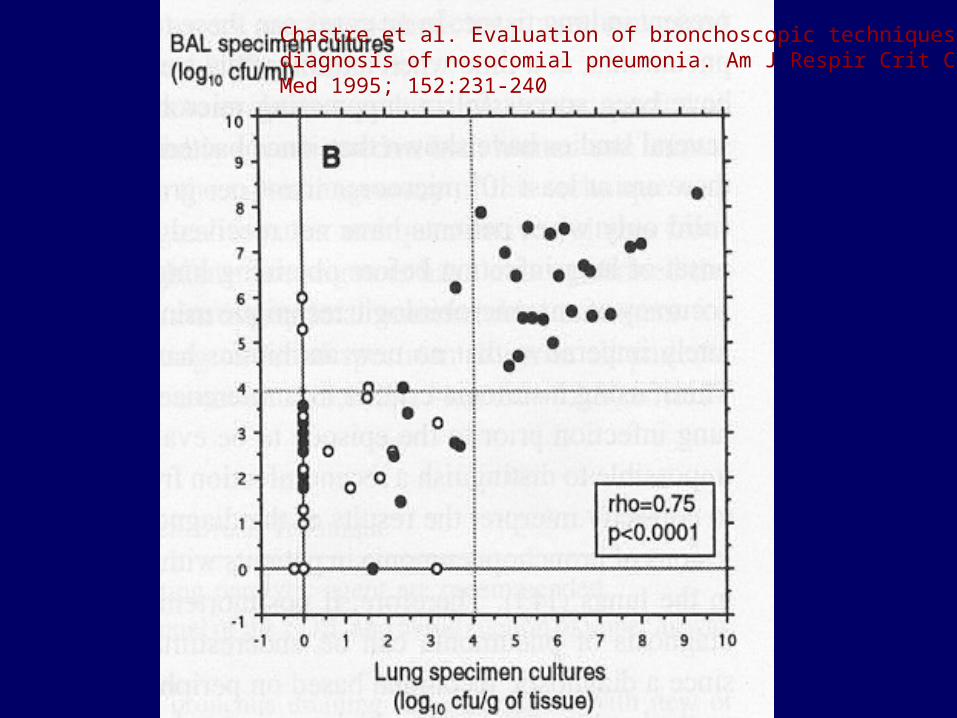
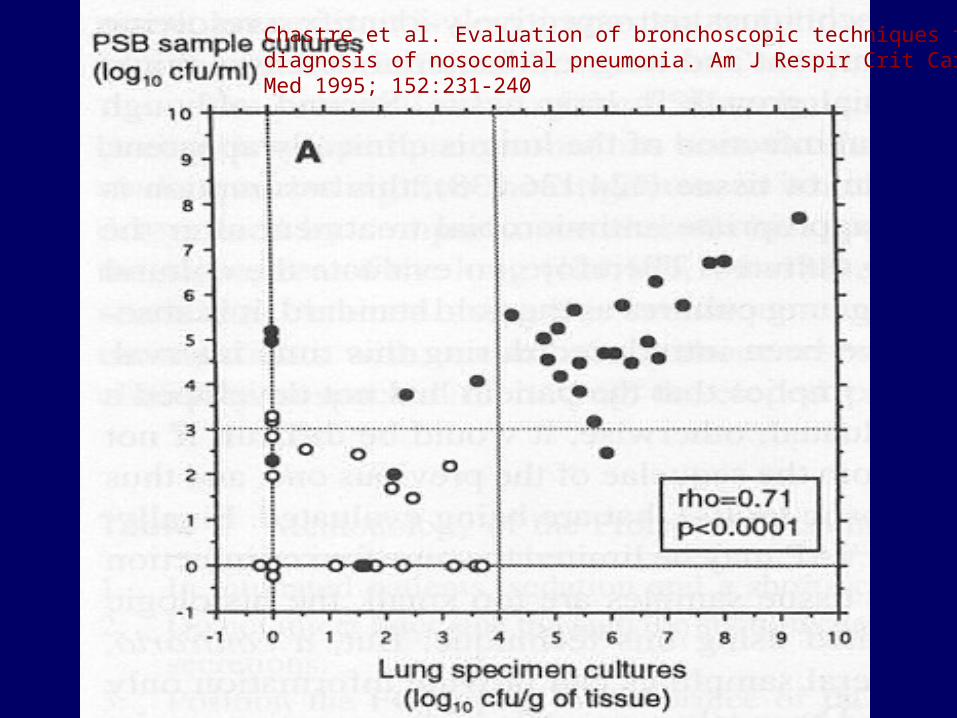
Chastre et al. Evaluation of bronchoscopic techniques for thediagnosis of nosocomial pneumonia. Am J Respir Crit Care Med 1995; 152:231-240
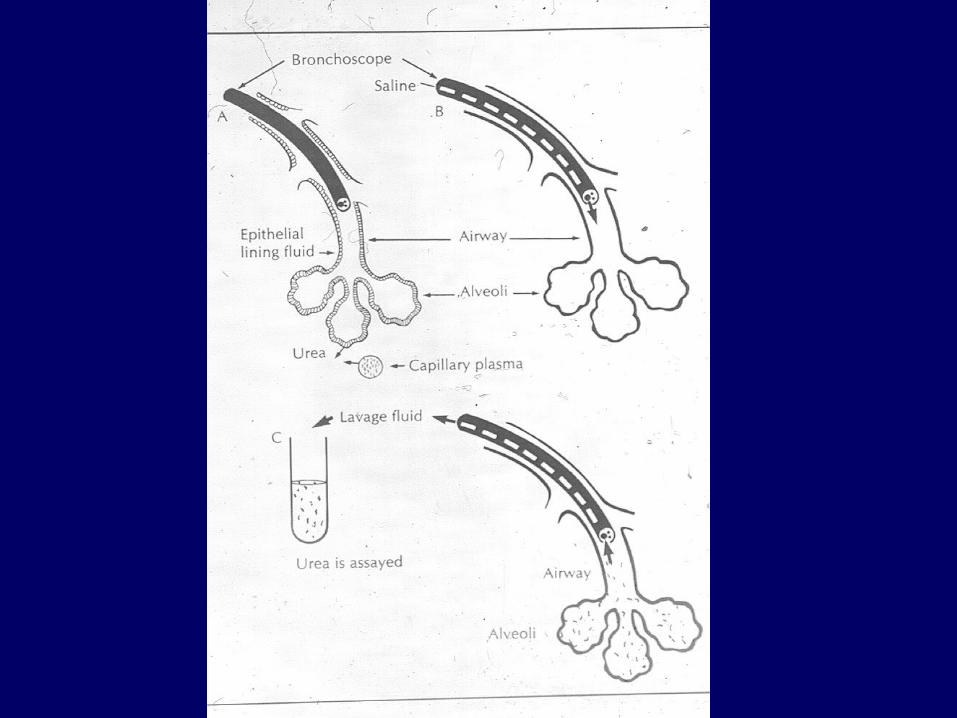
Diagnostic Strategy based Diagnostic Strategy based on Invasive Evaluationon Invasive Evaluation
Bronchoalveolar Lavage
Sensitivity Specificity
BAL 91% 78%
Chastre et al. Evaluation of bronchoscopic techniques for thediagnosis of nosocomial pneumonia. Am J Respir Crit Care Med 1995; 152:231-240
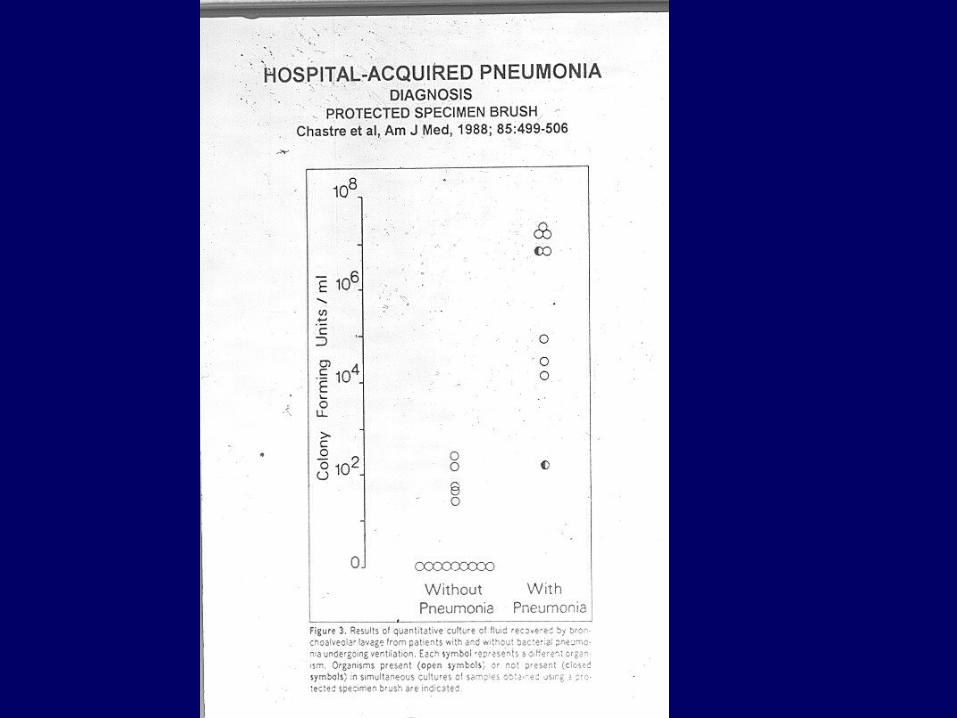
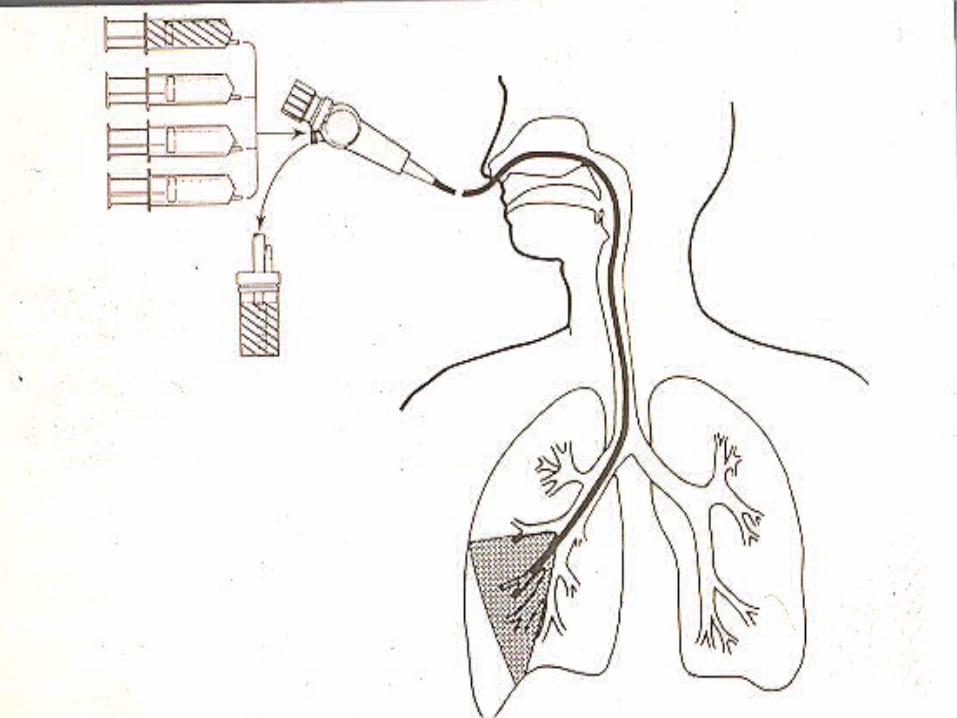
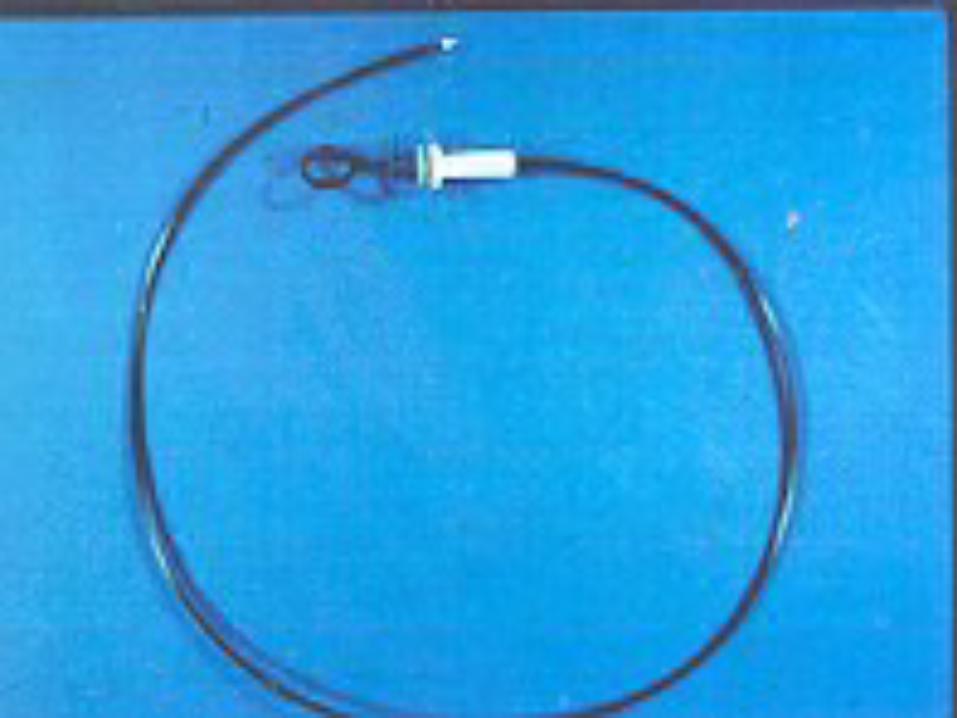
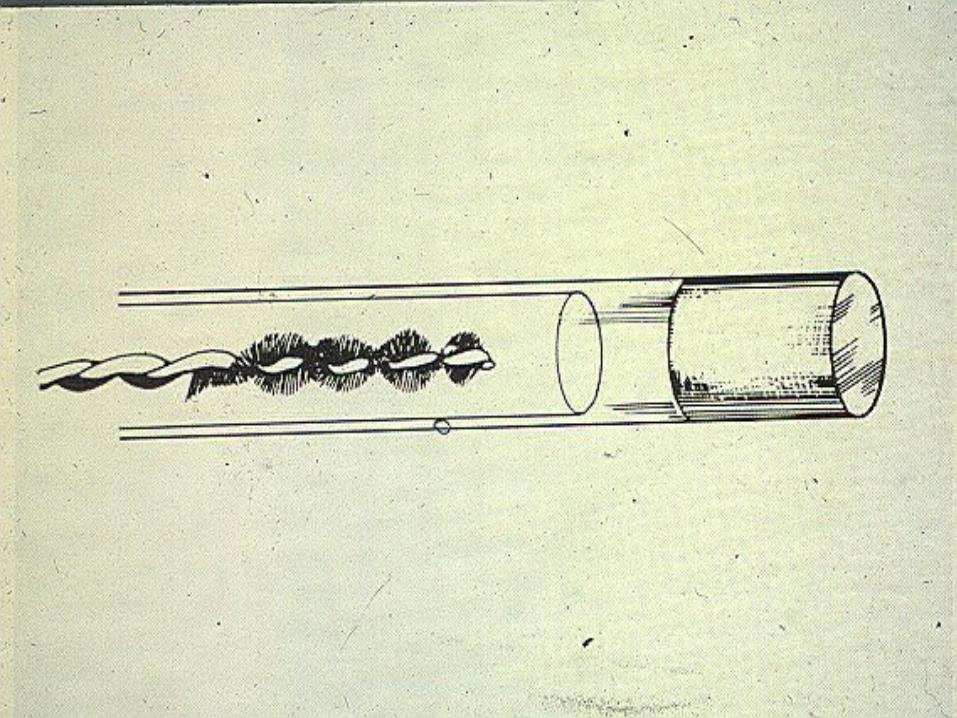
Diagnostic Strategy based on Invasive Diagnostic Strategy based on Invasive EvaluationEvaluation
Protected Brush SpecimenProtected Brush Specimen
Sensitivity Specificity
PSB 82% 89%
Diagnostic Strategy based on Invasive Diagnostic Strategy based on Invasive Evaluation Evaluation
Protected Brush SpecimenProtected Brush SpecimenDrawbacks: False Negative ResultsDrawbacks: False Negative Results
Bronchoscopy performed at an early Bronchoscopy performed at an early stage of infection with bacterial burden stage of infection with bacterial burden below the concentration necessary to below the concentration necessary to reach diagnostic significancereach diagnostic significance
Specimens obtained from unaffected Specimens obtained from unaffected segmentssegments
Specimens incorrectly processedSpecimens incorrectly processed Specimens obtained after initiation of a Specimens obtained after initiation of a
new antimicrobial therapynew antimicrobial therapy
Represents a good alternative in Represents a good alternative in patients with very unstable conditions patients with very unstable conditions and in patients for whom it is not and in patients for whom it is not possible to delay the initiation of possible to delay the initiation of antimicrobial treatment while awaiting antimicrobial treatment while awaiting bronchoscopybronchoscopy
Diagnosis can be missed, especially in Diagnosis can be missed, especially in the case of upper lobes or left lung the case of upper lobes or left lung infectioninfection
Intermediate Strategy Based on Intermediate Strategy Based on Quantitative Culture of Quantitative Culture of
Nonbronchoscopic SamplesNonbronchoscopic SamplesQuantitative Cultures of Nonbronchoscopic Distal
Protected Specimen
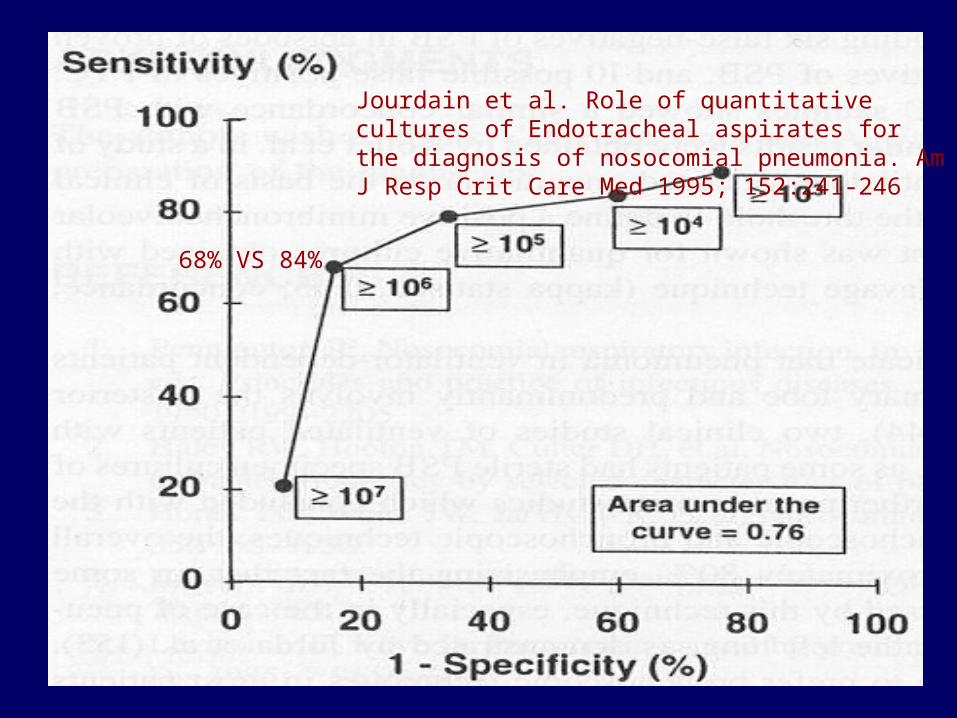
68% VS 84%
Jourdain et al. Role of quantitative cultures of Endotracheal aspirates for the diagnosis of nosocomial pneumonia. Am J Resp Crit Care Med 1995; 152:241-246

Quantitative Cultures of Endotracheal aspirates
Intermediate Strategy Based on Intermediate Strategy Based on Quantitative Culture of Quantitative Culture of
Nonbronchoscopic SamplesNonbronchoscopic Samples
Study CutoffValues
Sensitivity Specificity
Marquette et al 106 82% 83%
El-Ebiary et al 105 70% 72%
Diarrhea & Fever in ICUDiarrhea & Fever in ICU
Diarrhea is caused by enteral Diarrhea is caused by enteral feeding or drugsfeeding or drugs
The only common enteric cause of The only common enteric cause of fever in the ICU is fever in the ICU is Clostridium Clostridium difficiledifficile
C. difficileC. difficile accounts for about 25% accounts for about 25% of all cases of antibiotic-related of all cases of antibiotic-related diarrhea diarrhea
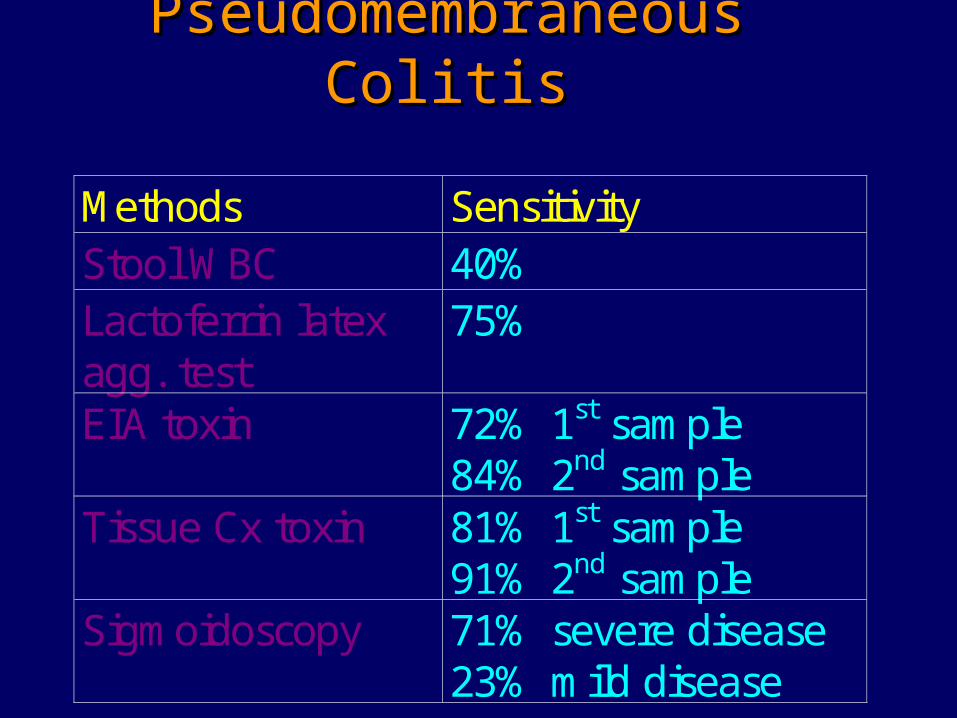
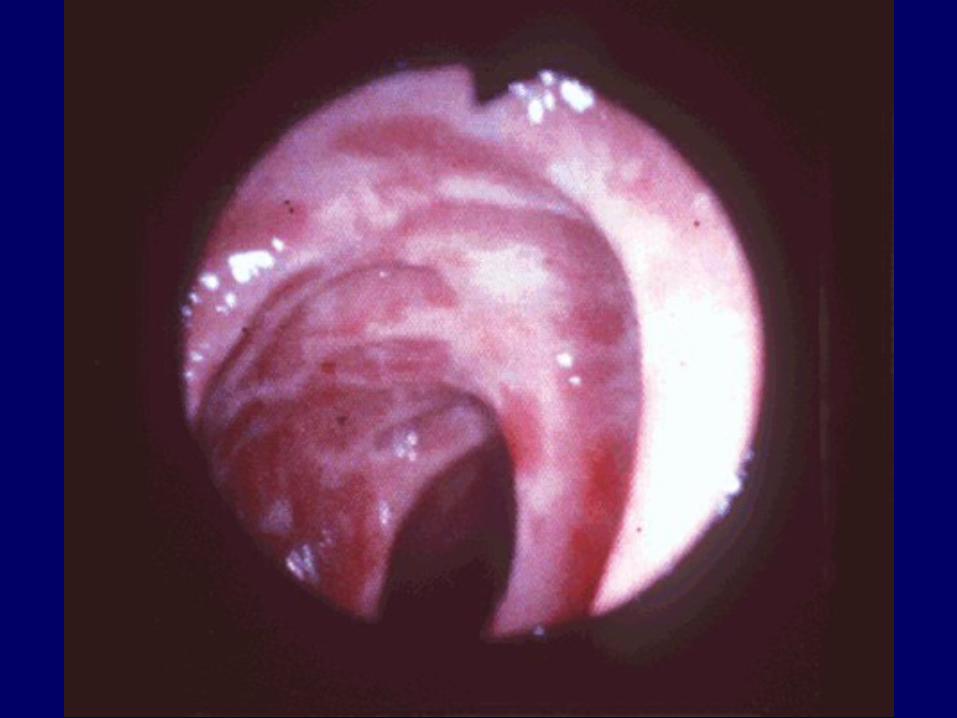
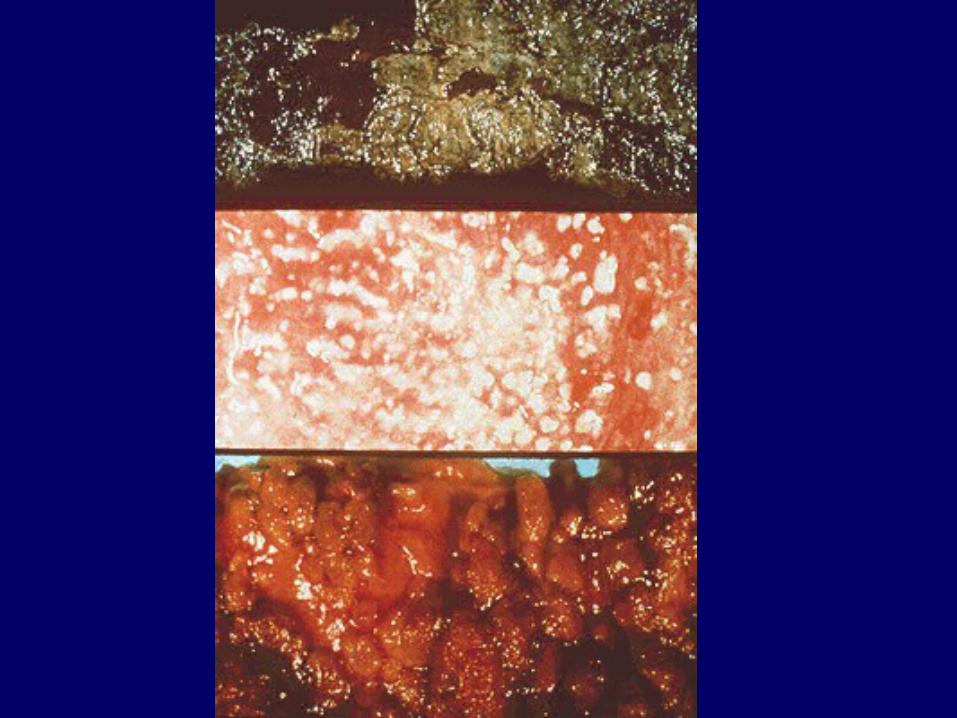
Pseudomembraneous Pseudomembraneous ColitisColitis
Methods SensitivityStool WBC 40%Lactoferrin latexagg. test
75%
EIA toxin 72% 1st sample84% 2nd sample
Tissue Cx toxin 81% 1st sample91% 2nd sample
Sigmoidoscopy 71% severe disease23% mild disease
Methylene Blue StainMethylene Blue Stain
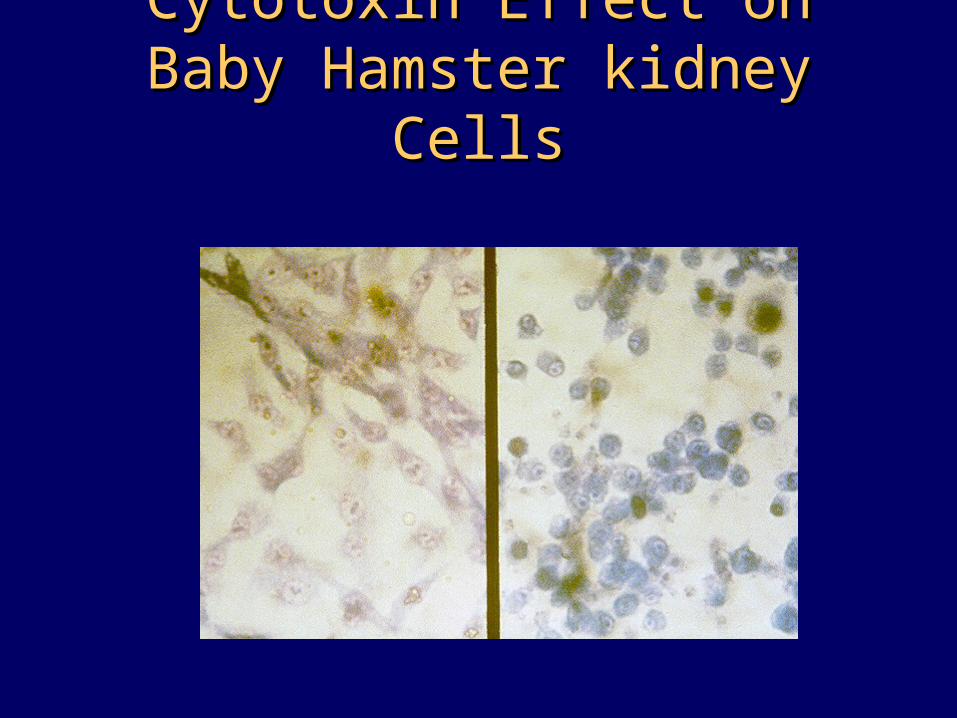
Cytotoxin Effect on Baby Cytotoxin Effect on Baby Hamster kidney CellsHamster kidney Cells
UTI & Fever in ICUUTI & Fever in ICU
The presence of pyuria can help The presence of pyuria can help establish the importance of urinary establish the importance of urinary bacteriabacteria
Leukocyte esterase dipstick test is Leukocyte esterase dipstick test is easy and simpleeasy and simple
Gram stain of a centrifuged urine Gram stain of a centrifuged urine sediment may provide clues to the sediment may provide clues to the type of microorganisms presenttype of microorganisms present
Other Causes of Fever in Other Causes of Fever in ICUICU
RespiratoryRespiratory
TracheobronchitisTracheobronchitis EmpyemaEmpyema Lung abscessLung abscess SinusitisSinusitis
Other Causes of Fever in Other Causes of Fever in ICUICU
Wound & Soft TissueWound & Soft Tissue
Wound infectionWound infection Decubitus ulcersDecubitus ulcers CellulitisCellulitis Deep-seated abscess: sub-Deep-seated abscess: sub-
diaphragmaticdiaphragmatic
Other Causes of Fever in Other Causes of Fever in ICUICU
GastrointestinalGastrointestinal
Ischemic colitisIschemic colitis Acalculous cholecystitisAcalculous cholecystitis CholangitisCholangitis Transfusion-related hepatitis: CMV, Transfusion-related hepatitis: CMV,
hepatitis C, and hepatitis Bhepatitis C, and hepatitis B Intraabdominal abscessIntraabdominal abscess DiverticulitisDiverticulitis
Other Causes of Fever in Other Causes of Fever in ICUICU
Prosthetic DevicesProsthetic Devices
Cardiac valve/pacemakerCardiac valve/pacemaker Joint replacement prosthesisJoint replacement prosthesis Peritoneal dialysis catheterPeritoneal dialysis catheter CNS intraventricular shuntCNS intraventricular shunt

Non-Infectious Source of Fever in Non-Infectious Source of Fever in ICUICU
DrugsDrugs
Antibiotics: B-lactam agentsAntibiotics: B-lactam agents Anti-epileptic drugs: phenytoinAnti-epileptic drugs: phenytoin Antiarrythmics: quinidine and Antiarrythmics: quinidine and
procainamideprocainamide Antihypertensive: methyldopaAntihypertensive: methyldopa
Non-Infectious Source of Fever in Non-Infectious Source of Fever in ICUICU
Post-operativePost-operative
Up till 72 hours postoperativeUp till 72 hours postoperative AtelectasisAtelectasis Post-pericardiotomy syndromePost-pericardiotomy syndrome
Non-Infectious Source of Fever in Non-Infectious Source of Fever in ICUICU
Vascular ConditionsVascular Conditions
Deep venous thrombophlebitisDeep venous thrombophlebitis Pulmonary embolism and infarctionPulmonary embolism and infarction Bowel ischemiaBowel ischemia Hemorrhage into CNS, Hemorrhage into CNS,
retroperitonium, joint, lung, and retroperitonium, joint, lung, and adrenalsadrenals
Myocardial infarction and Dressler’s Myocardial infarction and Dressler’s syndromesyndrome
Non-Infectious Source of Fever in Non-Infectious Source of Fever in ICUICU
Inflammatory ConditionsInflammatory Conditions
Reaction to blood productsReaction to blood products Proliferative phase of ARDSProliferative phase of ARDS Infusion of interleukin-2, granulocyte Infusion of interleukin-2, granulocyte
macrophage colony stimulating factor, macrophage colony stimulating factor, and granulocyte colony stimulating factorand granulocyte colony stimulating factor
Postpericardiotomy syndromePostpericardiotomy syndrome PancreatitisPancreatitis VasculitisVasculitis
Non-Infectious Source of Fever in Non-Infectious Source of Fever in ICUICU
Metabolic ConditionsMetabolic Conditions
Heat strokeHeat stroke Malignant hyperthermiaMalignant hyperthermia Neuroleptic malignant syndromeNeuroleptic malignant syndrome Adrenal insufficiencyAdrenal insufficiency Alcohol withdrawalAlcohol withdrawal SeizuresSeizures HyperthyroidismHyperthyroidism
Non-Infectious Source of Fever in Non-Infectious Source of Fever in ICUICU
NeoplasmsNeoplasms
LymphomaLymphoma Renal cell carcinomaRenal cell carcinoma HepatomaHepatoma Malignant metastatic to the liverMalignant metastatic to the liver Colon carcinomaColon carcinoma