Embed Size (px)
DESCRIPTION
Protective Lung Strategy Mazen Kherallah, MD, FCCP. Conventional Vs Protective. Actuarial 28-Day Survival among 53 Patients with the Acute Respiratory Distress Syndrome Assigned to Protective or Conventional Mechanical Ventilation. Amato M et al. N Engl J Med 1998;338:347-354. - PowerPoint PPT Presentation
Citation preview

Protective Lung StrategyMazen Kherallah, MD, FCCP

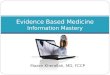
Conventional Vs Protective

Amato M et al. N Engl J Med 1998;338:347-354
Actuarial 28-Day Survival among 53 Patients with the Acute Respiratory Distress Syndrome Assigned to Protective or Conventional Mechanical
Ventilation

.ARDSnet N Engl J Med 2000;342:1301-1308
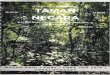
VENTILATION WITH LOWER TIDAL VOLUMES AS COMPARED WITHTRADITIONAL TIDAL VOLUMES FOR ACUTE LUNG INJURY
AND THE ACUTE RESPIRATORY DISTRESS SYNDROME

NIH ARDS Network TrialMechanical Ventilation in ARDS
P = 0.007
ARDSnet N Engl J Med 2000;342:1301-1308

SUMMARY OF RANDOMIZED CONTROLLED TRIALS OF VOLUME- AND
PRESSURE-LIMITED MECHANICAL VENTILATION
Hager DN et al . Am J RespirCrit Care Med 172:1241–1245

High PEEP Low Tidal Volume

A high PEEP-low tidal volume ventilatory strategy improves outcome in persistent ARDS
Villar et al. 2006 May;34(5):1311-8

LOVS StudyLung Open Ventilation Study

Results of 3 Trials of Aggressive vs Conservative PEEP
ALVEOLI LOVS ExPressN 583 983 767 Aggressive PEEP
15 cm H2O* 13 cm H2O* 15 cm H2O*
PaO2/FiO2 222 mm Hg* 187 mm Hg* 218 mm Hg*Pplat 27 cm H2O* 30 cm H2O* 27 cm H2O*Mortality 27% 36% 28% Conservative PEEP
8 cm H2O* 9 cm H2O* 7 cm H2O*
PaO2/FiO2 168 mm Hg* 149 mm Hg* 150 mm Hg*Pplat 24 cm H2O* 25 cm H2O* 21 cm H2O*Mortality 25% 40% 31

Prone Position

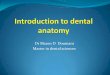
Kaplan-Meier Estimates of Survival at Six Months
Gattinoni L et al. N Engl J Med 2001;345:568-573

Gattinoni L et al. N Engl J Med 2001;345:568-573
Changes in Respiratory Variables during the 10-Day Treatment Period

Gattinoni L et al. N Engl J Med 2001;345:568-573
Incidence of Complications

A Multicenter Trial of Prolonged Prone Ventilation inSevere Acute Respiratory Distress Syndrome
Mancebo J, et al.Am J Respir Crit Care Med 173:1233–1239
mean of 17 h/d for a mean of 10 d.

Semirecumbent Position

Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial
86 patients: 95% CI for difference 10.0-42.0, p=0.003).
. Drakulovic MB 1999 Nov 27;354(9193):1851-8.

Noninvasive Ventilation in ALI/ARDS with mild/moderate Hypoxemic Respiratory Failure

Antonelli M et al. N Engl J Med 1998;339:429-435
The Ratio of the Partial Pressure of Arterial Oxygen to the Fraction of Inspired Oxygen (PaO2:FiO2) at Base Line and after One Hour of Mechanical Ventilation in Patients with Acute
Respiratory Failure in the Noninvasive-Ventilation and Conventional-Ventilation Groups

Antonelli M et al. N Engl J Med 1998;339:429-435
Serious Complications

Protocolized Weaning with Spontaneous Breathing Trials

Ely E et al. N Engl J Med 1996;335:1864-1869
Effect on the Duration of Mechanical Ventilation of Identifying Patients Capable of Breathing Spontaneously

Ely E et al. N Engl J Med 1996;335:1864-1869
Comparison of Outcomes between Study Groups

No Routine Use of PAC

Volume 354;21:2213-2224 May 25, 2006
Pulmonary-Artery versus Central Venous Catheter to Guide Treatment of Acute Lung Injury

Catheter-Related Complications

Conservative Fluid Strategy in Patient with no Tissue
Hypoperfusion

The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network N Engl J Med 2006;354:2564-2575
Comparison of Two Fluid-Management Strategies in Acute Lung Injury

Probability of Survival to Hospital Discharge and of Breathing without Assistance during the First 60 Days
after Randomization
The National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network N Engl J Med 2006;354:2564-2575

Ventilatory Support Target a tidal volume of 6ml/kg (predicted) body weight in patients with ALI/ARDS. (1B) Target an initial upper limit plateau pressure ≤30 cmH2O. Consider chest wall
compliance when assessing plateau pressure. (1C) Allow PaCO2 to increase above normal, if needed to minimize plateau pressures and
tidal volumes. (1C) Positive end expiratory pressure (PEEP) should be set to avoid extensive lung collapse
at end expiration. (1C)o Consider using the prone position for ARDS patients requiring potentially injurious
levels of FiO2 or plateau pressure, provided they are not put at risk from positional changes. (2C)
Maintain mechanically ventilated patients in a semi-recumbent position (head of the bed raised to 45 ◦) unless contraindicated (1B), between 30◦–45◦ (2C).
o Non invasive ventilation may be considered in the minority of ALI/ARDS patients with mild-moderate hypoxemic respiratory failure.
o Use a weaning protocol and a spontaneous breathing trial (SBT) regularly to evaluate the potential for discontinuing mechanical ventilation. (1A)
Do not use a PAC for the routine monitoring of patients with ALI/ARDS. (1A)