Embed Size (px)
Citation preview

11
Using Secondary Data in Using Secondary Data in Statistical AnalysisStatistical Analysis
Charles Natanson M.D.Charles Natanson M.D.Critical Care Medicine DepartmentCritical Care Medicine Department
Clinical CenterClinical CenterNational Institutes of HealthNational Institutes of Health
Bethesda, MDBethesda, MD
MetaMeta--analysis Definitionanalysis Definition•• Glass 1976, “the statistical analysis of a large Glass 1976, “the statistical analysis of a large
collection of results from individual literature collection of results from individual literature for the purpose of integrating their respective for the purpose of integrating their respective findings.”findings.”
•• Two basic purposes: Two basic purposes: p pp p1.1. Determine if similar treatment effects exist for a Determine if similar treatment effects exist for a
therapy in independent studies to estimate a net therapy in independent studies to estimate a net effect for this therapyeffect for this therapy
2.2. Alternatively, if treatment effects differ Alternatively, if treatment effects differ substantially for a therapy among independent substantially for a therapy among independent studies, to examine factors that may explain studies, to examine factors that may explain these differing effectsthese differing effects
Education Research 1976Education Research 1976
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step One: Formulating the QuestionStep One: Formulating the Question•• Validity and importance are contingent on Validity and importance are contingent on
this stepthis step•• Poorly conceived research hypothesis will Poorly conceived research hypothesis will
usually lead to an analysis of dubious valueusually lead to an analysis of dubious value

22
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Two: Defining Eligibility CriteriaStep Two: Defining Eligibility Criteria•• Protocols for study inclusion should be Protocols for study inclusion should be
prospective, systematic, and explicitprospective, systematic, and explicit•• Ideally, randomized trials similar in diagnosis, Ideally, randomized trials similar in diagnosis,
outcome, patient characteristics, and outcome, patient characteristics, and treatment groupstreatment groups
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Two: Defining Eligibility Criteria Cont’dStep Two: Defining Eligibility Criteria Cont’d•• Including all available studies, regardless of Including all available studies, regardless of
size, design, or quality results in an analysis size, design, or quality results in an analysis that is broadly representative but maythat is broadly representative but maythat is broadly representative but may that is broadly representative but may compromise accuracycompromise accuracy
•• Alternatively, exclusion of poorly done Alternatively, exclusion of poorly done studies may increase the statistical validity studies may increase the statistical validity but limit the ability to generalize findingsbut limit the ability to generalize findings
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Three: Identifying Studies and Data Step Three: Identifying Studies and Data AbstractionAbstraction
•• Usually begins with a search of online Usually begins with a search of online databases such as MEDLINE Currentdatabases such as MEDLINE Currentdatabases such as MEDLINE, Current databases such as MEDLINE, Current Contents, Best Evidence, Cochrane, and Contents, Best Evidence, Cochrane, and HealthSTARHealthSTAR
•• Title and abstract perused to exclude studiesTitle and abstract perused to exclude studies

33
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Three: Identifying Studies and Data Step Three: Identifying Studies and Data Abstraction Cont’dAbstraction Cont’d
•• Full texts of the remaining articles retrieved Full texts of the remaining articles retrieved and thoroughly studiedand thoroughly studiedand thoroughly studiedand thoroughly studied
•• Reference lists of these articles are reviewedReference lists of these articles are reviewed•• Once a study selected for inclusion, data Once a study selected for inclusion, data
should be extracted by more than one should be extracted by more than one reviewer onto structured formsreviewer onto structured forms
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Four: AnalysisStep Four: Analysis•• A common measure of treatment effect must A common measure of treatment effect must
be determinedbe determined•• Fixed versus random effect model used to Fixed versus random effect model used to
combine datacombine data
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Four: Analysis Cont’dStep Four: Analysis Cont’d•• Cochran’s Q statistic and ICochran’s Q statistic and I22 calculatedcalculated•• Consider metaregression when IConsider metaregression when I22 > 30% and > 30% and
P < 0.10P < 0.10•• Publication bias examinedPublication bias examined
–– Funnel PlotFunnel Plot

44
Techniques of MetaTechniques of Meta--AnalysisAnalysis
Step Five: Reporting and Interpreting ResultsStep Five: Reporting and Interpreting Results•• To improve overall quality of reporting for To improve overall quality of reporting for
metameta--analysis, a checklist and a flow chart analysis, a checklist and a flow chart should be constructedshould be constructedshould be constructedshould be constructed
•• Quality of Reporting of MetaQuality of Reporting of Meta--analyses analyses (QUOROM) conference provides guidelines (QUOROM) conference provides guidelines for reporting searches, study selection, for reporting searches, study selection, validity assessment, data abstraction, study validity assessment, data abstraction, study characteristics and data synthesischaracteristics and data synthesis
Lancet, 1999.Lancet, 1999.
MetaMeta--analysis of Clinical Trials in Sepsisanalysis of Clinical Trials in Sepsis
Septic Shock ManagementSeptic Shock Management
Early recognitionEarly recognition
The right antibiotics right awayThe right antibiotics right awayg g yg g y
Rapid fluid resuscitationRapid fluid resuscitation
Judicious use of vasopressorsJudicious use of vasopressors
Promptly address removablePromptly address removable nidinidi

55
McCabeMcCabe 19621962FriedFried 19681968BryantBryant 19711971KrogerKroger 19801980IshpahaniIshpahani 19871987ChowChow 19911991WeinsteinWeinstein 19931993Vid lVid l 19961996
Benefits of Starting Appropriate Benefits of Starting Appropriate Antibiotic TherapyAntibiotic Therapy
Odds Ratio of Survival (95% CI)Odds Ratio of Survival (95% CI)0.0010.001 0.010.01 0.10.1 11 1010 100100 10001000
VidalVidal 19961996SchiappaSchiappa 19961996Leibovici Leibovici 19971997LeiboviciLeibovici 19971997LeiboviciLeibovici 19981998KulleyKulley 19991999IbrahimIbrahim 20002000FaragofaFaragofa 20032003GarnachoGarnacho--MonteroMontero 20032003HorbarthHorbarth 20032003LeoneLeone 20032003
Benefit of Early Benefit of Early versusversus Late AntibioticsLate AntibioticsAuthorAuthor YearYear NN DiagnosisDiagnosisMinerMiner 20012001 171171 MeningitisMeningitisLarcheLarche 20022002 8888 Bact/pneumoniaBact/pneumonia**HouckHouck 20042004 13,77113,771 PneumoniaPneumoniaProulxProulx 20052005 118118 MeningitisMeningitisM hM h 19971997 14 06914 069 P iP i
Odds Ratio of Survival (95% CI)Odds Ratio of Survival (95% CI)
0.010.01 0.10.1 11 1010 100100BenefitBenefitHarmHarm
* Patients with cancer * Patients with cancer
MeehanMeehan 19971997 14,06914,069 PneumoniaPneumoniaGacouinGacouin 20022002 213213 LegionellaLegionellaIreguiIregui 20062006 107107 VAPVAPLodisLodis 20032003 167167 S. aureusS. aureusKangKang 20032003 123123 P. aeruginosaP. aeruginosa
The Host Inflammatory The Host Inflammatory Response Hypothesis:Response Hypothesis:Response Hypothesis: Response Hypothesis:
What went wrong?What went wrong?

66
Pathogenesis of Septic ShockPathogenesis of Septic ShockPathogensPathogens
andandToxinsToxins
Host Defenses Host Defenses ReleaseRelease
Inflammatory Inflammatory MediatorsMediators
InfectionInfection
Shock and Shock and InjuryInjury
Multiorgan FailureMultiorgan Failureand Deathand Death
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
BAY x 1351BAY x 1351
BAY x 1351BAY x 1351
BAY x 1351BAY x 1351
AntiAnti--TNF AntibodiesTNF Antibodies
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
MAK 195FMAK 195FBN52021BN52021
MAK 195FMAK 195F
CB0006CB0006CDP571CDP571
MAK 195FMAK 195F
Crit Care Med 1998Crit Care Med 1998

77
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
AntiAnti--TNF AntibodiesTNF AntibodiesBAY x 1351BAY x 1351PP--5555
BAY x 1351BAY x 1351
BAY x 1351BAY x 1351
PP--5555
Soluble TNF ReceptorsSoluble TNF Receptors
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
MAK 195FMAK 195F
PP--8080MAK 195FMAK 195F
CB0006CB0006CDP571CDP571
MAK 195FMAK 195F
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
BAY x 1351BAY x 1351PP--5555
AntrilAntrilBAY x 1351BAY x 1351
BAY x 1351BAY x 1351
AntrilAntril
PP--5555
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
AntiAnti--TNF AntibodiesTNF Antibodies
ILIL--1ra1raSoluble TNF ReceptorsSoluble TNF Receptors
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
MAK 195FMAK 195F
PP--8080MAK 195FMAK 195F
AntrilAntrilCB0006CB0006
CDP571CDP571MAK 195FMAK 195F
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
BAY x 1351BAY x 1351PP--5555
AntrilAntrilBAY x 1351BAY x 1351
BN52021BN52021BAY x 1351BAY x 1351
AntrilAntril
PP--5555
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
AntiAnti--TNF AntibodiesTNF Antibodies
PAFraPAFraILIL--1ra1raSoluble TNF ReceptorsSoluble TNF Receptors
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
MAK 195FMAK 195FBN52021BN52021
PP--8080MAK 195FMAK 195F
AntrilAntrilCB0006CB0006
CDP571CDP571MAK 195FMAK 195F
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI

88
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
BAY x 1351BAY x 1351PP--5555
AntrilAntrilBAY x 1351BAY x 1351
BN52021BN52021BAY x 1351BAY x 1351
IbuprofenIbuprofen
AntrilAntril
PP--5555
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
AntiAnti--TNF AntibodiesTNF Antibodies
AntiAnti--ProstaglandinProstaglandinPAFraPAFraILIL--1ra1raSoluble TNF ReceptorsSoluble TNF Receptors
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
IbuprofenIbuprofenMAK 195FMAK 195F
BN52021BN52021
PP--8080MAK 195FMAK 195F
AntrilAntrilCB0006CB0006
CDP571CDP571MAK 195FMAK 195F
IbuprofenIbuprofenIbuprofenIbuprofen
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
BAY x 1351BAY x 1351PP--5555
AntrilAntrilBAY x 1351BAY x 1351
BN52021BN52021BAY x 1351BAY x 1351
IbuprofenIbuprofen
CPOCPO--127127
AntrilAntril
PP--5555
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
AntiAnti--TNF AntibodiesTNF Antibodies
AntiAnti--BradykininBradykininAntiAnti--ProstaglandinProstaglandinPAFraPAFraILIL--1ra1raSoluble TNF ReceptorsSoluble TNF Receptors
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
IbuprofenIbuprofenMAK 195FMAK 195F
BN52021BN52021CPOCPO--127127
PP--8080MAK 195FMAK 195F
AntrilAntrilCB0006CB0006
CDP571CDP571MAK 195FMAK 195F
IbuprofenIbuprofenIbuprofenIbuprofen
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI
Number of Patients EnrolledNumber of Patients Enrolled00 10001000 20002000
BAY x 1351BAY x 1351PP--5555
AntrilAntrilBAY x 1351BAY x 1351
BN52021BN52021BAY x 1351BAY x 1351
IbuprofenIbuprofen
CPOCPO--127127
AntrilAntril
PP--5555
Human Clinical Trials of AntiHuman Clinical Trials of Anti--Inflammatory Inflammatory Therapies in Sepsis Therapies in Sepsis Ranked by SizeRanked by Size
AntiAnti--TNF AntibodiesTNF Antibodies
AntiAnti--BradykininBradykininAntiAnti--ProstaglandinProstaglandinPAFraPAFraILIL--1ra1raSoluble TNF ReceptorsSoluble TNF Receptors
Increasing HarmIncreasing Harm Increasing BenefitIncreasing BenefitNo EffectNo Effect
0.10.1 0.30.3 0.50.5 11 2.02.0 4.04.0 8.08.0
IbuprofenIbuprofenMAK 195FMAK 195F
BN52021BN52021CPOCPO--127127
PP--8080MAK 195FMAK 195F
AntrilAntrilCB0006CB0006
CDP571CDP571MAK 195FMAK 195F
IbuprofenIbuprofenIbuprofenIbuprofen
Crit Care Med 1998Crit Care Med 1998
Odds Ratio of SurvivalOdds Ratio of Survival
95% CI95% CI

99
Control Arm Mortality Rates by Control Arm Mortality Rates by Type ofType of AntiAnti--inflammatory inflammatory AgentAgent
nt M
orta
lity
(nt
Mor
talit
y (±±
SEM
)SE
M) 100100
9090
8080
7070
6060
5050
Mea
n Pe
rcen
Mea
n Pe
rcen 4040
3030
2020
1010
00# of Trials# of Trials
# of# ofDeathsDeaths
# of# ofPatientsPatients 102/258102/258
N = 3N = 3256/853256/853
N = 3N = 3602/1493602/1493
N = 7N = 7218/438218/438
N = 2N = 2276/783276/783
N = 3N = 376/21076/210N = 2N = 2
Crit. Care Med 1997Crit. Care Med 1997
Preclinical Studies of Preclinical Studies of AntiAnti--inflammatory Agentsinflammatory Agents
P < 0.0001P < 0.0001
Favo
rs T
hera
pyFa
vors
The
rapy
ds R
atio
ds R
atio
10001000
100100
1010
11
BeneficialBeneficial
Am J Respir Crit Care Med 2002;166:1197 Am J Respir Crit Care Med 2002;166:1197
25255050
100100
AnimalsAnimals
Favo
rs C
ontr
olFa
vors
Con
trol
Odd
Odd 0.10.1
0.010.01
0.0010.001
0.00010.00010.010.01 0.10.1 11 1010 100100
Control Odds of DyingControl Odds of Dying
PatientsPatientsHarmfulHarmful
Prospective Animal Studies of Prospective Animal Studies of Selected AgentsSelected Agents
P < 0.0001P < 0.000110001000
100100
1010
11
ololFa
vors
The
rapy
Favo
rs T
hera
pys
Rat
ios
Rat
io
PP--80 TNF80 TNFαα soluble receptorsoluble receptorTyrosine kinase inhibitorTyrosine kinase inhibitor
Am J Respir Crit Care Med 2002;166:1197 Am J Respir Crit Care Med 2002;166:1197
0.10.1
0.010.01
0.0010.001
0.00010.0001
Favo
rs C
ontr
oFa
vors
Con
tro
Odd
Odd
0.010.01 0.10.1 11 1010 100100Control Group Odds of DyingControl Group Odds of Dying
25255050100100
RatsRatsEndotoxinEndotoxinGramGram--negativenegativeGramGram--positivepositivei.v.i.v. challengechallengePneumoniaPneumonia
DogsDogs PatientsPatients

1010
Randomized Clinical Trials in Sepsis Randomized Clinical Trials in Sepsis Divided by Severity of Illness ScoresDivided by Severity of Illness Scores
Favo
rs T
hera
pyFa
vors
The
rapy
of S
urvi
val
of S
urvi
val 1010
44
P = 0.0002P = 0.0002
Am J Respir Crit Care Med 2002;166:1197 Am J Respir Crit Care Med 2002;166:1197
Favo
rs C
ontr
olFa
vors
Con
trol
FF
Odd
s R
atio
oO
dds
Rat
io o
11
0.250.25
0.10.1
0.10.1 0.250.25 11 101044Control Odds of DyingControl Odds of Dying
Activated Protein CActivated Protein CILIL--1ra1ra
pp--5555--TNFsrTNFsr
SummarySummaryAntiAnti--Inflammatory Agents in Sepsis Inflammatory Agents in Sepsis
•• MetaMeta--analysis:analysis:–– treatment effects are small (3%), treatment effects are small (3%),
but statistically significantbut statistically significanty gy g•• MetaMeta--regression analysis:regression analysis:
–– Efficacy dependent on risk of Efficacy dependent on risk of deathdeath»»Beneficial at high risks of death, Beneficial at high risks of death, »»ineffective or harmful when risk ineffective or harmful when risk
was moderate or lowwas moderate or low
Paradox of Paradox of Corticosteroids in SepsisCorticosteroids in Sepsis
Less may have benefits, Less may have benefits, but only in sickest patientsbut only in sickest patients

1111
Corticosteroids in SepsisCorticosteroids in Sepsis
•• Investigated since the 1960sInvestigated since the 1960s
•• By early 1990s, shown to be By early 1990s, shown to be ineffective or possibly harmfulineffective or possibly harmful
•• Renewed interest and new Renewed interest and new trials over the last decadetrials over the last decade
Trials of Corticosteroids in SepsisTrials of Corticosteroids in SepsisAuthorAuthor Year PublishedYear Published Odds ratioOdds ratio
95% CI95% CI
Ann Intern Med 2004; 141:47Ann Intern Med 2004; 141:47Clin Microbiol Infect 2009; 15: 308Clin Microbiol Infect 2009; 15: 308 Odds Ratio of SurvivalOdds Ratio of Survival
0.140.14 1.001.00 7.407.40 55.0055.00Favors SteroidsFavors SteroidsFavors ControlFavors Control
BennettBennettKlasterskyKlasterskySchumerSchumerThompsonThompsonLucasLucasSprungSprungBoneBoneVAVALuceLuce
196319631971197119761976197619761984198419841984198719871987198719881988
Trials of Corticosteroids in SepsisTrials of Corticosteroids in SepsisAuthorAuthor Year PublishedYear Published Odds ratioOdds ratio
95% CI95% CI
II22 = 70%= 70%
Odds Ratio of SurvivalOdds Ratio of Survival
0.140.14 1.001.00 7.407.40 55.0055.00Favors SteroidsFavors SteroidsFavors ControlFavors ControlAnn Intern Med 2004; 141:47Ann Intern Med 2004; 141:47
Clin Microbiol Infect 2009; 15: 308Clin Microbiol Infect 2009; 15: 308

1212
Trials of Corticosteroids in SepsisTrials of Corticosteroids in SepsisAuthorAuthor Year PublishedYear Published Odds ratioOdds ratio
95% CI95% CI
II22 = 0%= 0%
Short course (24 h) high dose Short course (24 h) high dose
BennettBennettKlasterskyKlasterskySchumerSchumerThompsonThompsonLucasLucasSprungSprungBoneBoneVAVALuceLuce
196319631971197119761976197619761984198419841984198719871987198719881988
Odds Ratio of SurvivalOdds Ratio of Survival
0.140.14 1.001.00 7.407.40 55.0055.00Favors SteroidsFavors SteroidsFavors ControlFavors ControlAnn Intern Med 2004; 141:47Ann Intern Med 2004; 141:47
Clin Microbiol Infect 2009; 15: 308Clin Microbiol Infect 2009; 15: 308
corticosteroids (median corticosteroids (median --24,000 mg of hydrocortisone 24,000 mg of hydrocortisone equivalents) worsened survivalequivalents) worsened survival
SummarySummaryPre 1989 studies (N = 8)Pre 1989 studies (N = 8) P = 0.008P = 0.008
Trials of Corticosteroids in SepsisTrials of Corticosteroids in SepsisAuthorAuthor Year PublishedYear Published Odds ratioOdds ratio
95% CI95% CI
II22 = 0%= 0%
BennettBennettKlasterskyKlasterskySchumerSchumerThompsonThompsonLucasLucasSprungSprungBoneBoneVAVALuceLuce
196319631971197119761976197619761984198419841984198719871987198719881988
BollaertBollaertBriegelBriegelChawlaChawlaYildizYildiz
19981998199919991999199920022002
Stress dose corticosteroids Stress dose corticosteroids (median (median -- 1200 mg of 1200 mg of hydrocortisone equivalents)hydrocortisone equivalents)
Odds Ratio of SurvivalOdds Ratio of Survival
0.140.14 1.001.00 7.407.40 55.0055.00Favors SteroidsFavors SteroidsFavors ControlFavors ControlAnn Intern Med 2004; 141:47Ann Intern Med 2004; 141:47
Clin Microbiol Infect 2009; 15: 308Clin Microbiol Infect 2009; 15: 308
YildizYildizAnnaneAnnaneConfalonieriConfalonieriMussackMussackOppertOppertTandanTandanRinaldiRinaldiCicarelliCicarelliSprungSprungSummarySummary
200220022002200220052005200520052005200520052005200620062007200720082008
hydrocortisone equivalents) hydrocortisone equivalents) tapered over 6 days were tapered over 6 days were associated with improved associated with improved survivalsurvival
Pre 1989 studies (N = 8)Pre 1989 studies (N = 8) P = 0.008P = 0.008Post 1997 studies (N = 12)Post 1997 studies (N = 12) P < 0.001P < 0.001
Trials of Corticosteroids in SepsisTrials of Corticosteroids in SepsisAuthorAuthor Year PublishedYear Published Odds ratioOdds ratio
95% CI95% CI
II22 = 25%= 25%
II22 = 0%= 0%
BennettBennettKlasterskyKlasterskySchumerSchumerThompsonThompsonLucasLucasSprungSprungBoneBoneVAVALuceLuce
196319631971197119761976197619761984198419841984198719871987198719881988
BollaertBollaertBriegelBriegelChawlaChawlaYildizYildiz
19981998199919991999199920022002
Odds Ratio of SurvivalOdds Ratio of Survival
0.140.14 1.001.00 7.407.40 55.0055.00Favors SteroidsFavors SteroidsFavors ControlFavors ControlAnn Intern Med 2004; 141:47Ann Intern Med 2004; 141:47
Clin Microbiol Infect 2009; 15: 308Clin Microbiol Infect 2009; 15: 308
II 25% 25%YildizYildizAnnaneAnnaneConfalonieriConfalonieriMussackMussackOppertOppertTandanTandanRinaldiRinaldiCicarelliCicarelliSprungSprungSummarySummary
200220022002200220052005200520052005200520052005200620062007200720082008
Post 1997 studies (N = 12)Post 1997 studies (N = 12) P < 0.001P < 0.001Pre 1989 studies (N = 8)Pre 1989 studies (N = 8) P = 0.008P = 0.008
Corticus TrialCorticus Trial

1313
Trials of Corticosteroids in SepsisTrials of Corticosteroids in SepsisAuthorAuthor Year PublishedYear Published Odds ratioOdds ratio
95% CI95% CI
II22 = 0%= 0%
BennettBennettKlasterskyKlasterskySchumerSchumerThompsonThompsonLucasLucasSprungSprungBoneBoneVAVALuceLuce
196319631971197119761976197619761984198419841984198719871987198719881988
BollaertBollaertBriegelBriegelChawlaChawlaYildizYildiz
19981998199919991999199920022002 II22 = 0%= 0%
Odds Ratio of SurvivalOdds Ratio of Survival
0.140.14 1.001.00 7.407.40 55.0055.00Favors SteroidsFavors SteroidsFavors ControlFavors ControlAnn Intern Med 2004; 141:47Ann Intern Med 2004; 141:47
Clin Microbiol Infect 2009; 15: 308Clin Microbiol Infect 2009; 15: 308
YildizYildizAnnaneAnnaneConfalonieriConfalonieriMussackMussackOppertOppertTandanTandanRinaldiRinaldiCicarelliCicarelliSprungSprungSummarySummary
200220022002200220052005200520052005200520052005200620062007200720082008
Post 1997 studies (N = 12)Post 1997 studies (N = 12) P < 0.001P < 0.001
II 0% 0%
Post 1997 studies (N = 11)Post 1997 studies (N = 11) P < 0.001P < 0.001
Pre 1989 studies (N = 8)Pre 1989 studies (N = 8) P = 0.008P = 0.008
How is Corticus Different How is Corticus Different from the 11 Other Trials offrom the 11 Other Trials offrom the 11 Other Trials of from the 11 Other Trials of
LowLow--Dose Steroids?Dose Steroids?
P = 0.03P = 0.03
of S
urvi
val
of S
urvi
val
2 702 70
7.407.40
20.0020.00
vors
Ste
roid
svo
rs S
tero
ids
Effect of Corticosteroids During Sepsis Effect of Corticosteroids During Sepsis Dependent on the Severity of IllnessDependent on the Severity of Illness
Control Odds of DeathControl Odds of Death0.10.1 1.01.0 10.010.0
Odd
s R
atio
oO
dds
Rat
io o
0.140.14
0.370.37
1.001.00
2.702.70
Favo
rs C
ontr
olFa
vors
Con
trol
Fav
Fav
Corticus TrialCorticus Trial

1414
Funnel Plot of Sepsis Trials of Funnel Plot of Sepsis Trials of Low Dose SteroidsLow Dose Steroids
1/St
d Er
r)1/
Std
Err)
66
44
55
Prec
isio
n (1
Prec
isio
n (1
Log OR of deathLog OR of death00--11--22--33
11
22
33
00332211
Favors SteroidsFavors Steroids Favors ControlFavors Control
Corticosteroid Effect on ShockCorticosteroid Effect on Shock
Low Dose Corticosteroids Trials Low Dose Corticosteroids Trials Reporting Shock ReversalReporting Shock Reversal
BriegelBriegelBollaertBollaertChawlaChawlaAnnaneAnnane
AuthorsAuthors II22 = 0%= 0%
Odds Ratio of Shock ReversalOdds Ratio of Shock Reversal
0.020.02 0.140.14 1.001.00 7.397.39 54.6054.60
AnnaneAnnaneMussackMussackTandanTandanCORTICUSCORTICUS
Overall (N = 7)Overall (N = 7)
Favors CorticosteroidsFavors CorticosteroidsFavors ControlFavors Control
P < 0.001P < 0.001

1515
SummarySummary
•• Corticosteroid effects during Corticosteroid effects during sepsis depend on sepsis depend on dosedose andandseverityseverity of illnessof illness
•• Low dose steroids decrease Low dose steroids decrease vasopressor requirements vasopressor requirements and enhance shock reversaland enhance shock reversal
High dose corticosteroids High dose corticosteroids increase mortalityincrease mortality
Low dose corticosteroids Low dose corticosteroids improve survival in improve survival in severely ill patientsseverely ill patients
•• At present, the beneficial effects of low At present, the beneficial effects of low doses of corticosteroids are based on doses of corticosteroids are based on small trials (median 40 patients, IQR 41small trials (median 40 patients, IQR 41--44) 44) confounded by publication biasconfounded by publication bias
LimitationsLimitations
•• The largest trial of low dose corticoThe largest trial of low dose cortico--steroids (CORTICUS, n = 499) studied a steroids (CORTICUS, n = 499) studied a relatively low risk populationrelatively low risk population
•• Benefit from low dose corticosteroids has Benefit from low dose corticosteroids has not been confirmed in a large multicenter not been confirmed in a large multicenter trial of high risk patientstrial of high risk patients
•• Until new data are available, the Until new data are available, the decision to administer low dose decision to administer low dose steroids for septic shock shouldsteroids for septic shock should
ConclusionsConclusions
steroids for septic shock should steroids for septic shock should be individualized:be individualized:
–– Severity of illnessSeverity of illness–– Assessment of riskAssessment of risk

1616
Intensive Insulin Therapy Intensive Insulin Therapy in Patients with Sepsisin Patients with Sepsis
How much risk and how much benefit?How much risk and how much benefit?
Endorsement of Glycemic Control as Endorsement of Glycemic Control as Standard of Care for the Critically IllStandard of Care for the Critically Ill
•• JCAHOJCAHO–– Core quality of care Core quality of care -- all Medicare hospitalsall Medicare hospitals
•• American College of EndocrinologyAmerican College of Endocrinology•• Volunteer Hospital AssociationVolunteer Hospital Association•• Volunteer Hospital AssociationVolunteer Hospital Association
–– Care bundleCare bundle
•• Institute for Healthcare ImprovementInstitute for Healthcare Improvement–– Sepsis bundleSepsis bundle–– Post cardiac surgeryPost cardiac surgery
•• Surviving Sepsis CampaignSurviving Sepsis Campaign–– Sepsis bundleSepsis bundle
Am J Resp Crit Care Med 2005; 172:1358Am J Resp Crit Care Med 2005; 172:1358
Selected Baseline CharacteristicsSelected Baseline CharacteristicsConventionalConventional
Insulin: glucoseInsulin: glucose180 180 -- 200 mg/dl200 mg/dl
N = 783N = 783
Intensive Intensive Insulin: glucose Insulin: glucose 80 80 -- 110 mg/dl110 mg/dl
N = 765N = 765
MenMen 557 (71%)557 (71%) 544 (71%)544 (71%)
Age (yr)Age (yr) 62.2 62.2 ±± 13.913.9 63.4 63.4 ±± 4.44.4
Reason for ICU care:Reason for ICU care:Cardiac SurgeryCardiac SurgeryNonNon--cardiac indicationscardiac indications
493 (63%)493 (63%)290 (37%)290 (37%)
477 (62%)477 (62%)288 (38%)288 (38%)
Apache II (median, IQR)Apache II (median, IQR) 9 (7 9 (7 -- 13)13) 9 (7 9 (7 -- 13)13)N Engl J Med 2001;345:1359 N Engl J Med 2001;345:1359

1717
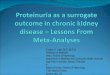
Mortality Associated with Mortality Associated with Conventional Conventional versusversus Intensive InsulinIntensive Insulin
Death in ICUDeath in ICU # of # of patientspatients
ConventionalConventionalInsulin Insulin
Intensive Intensive Insulin Insulin
∆ ∆ deathsdeaths
Cardiac SurgeryCardiac Surgery 970970 25 (5%)25 (5%) 10 (2%)10 (2%) 1515Th iTh i 122122 10 (18%)10 (18%) 5 (7 6%)5 (7 6%) 55ThoracicThoracic 122122 10 (18%)10 (18%) 5 (7.6%)5 (7.6%) 55OtherOther 7070 6 (17%)6 (17%) 0 (0%)0 (0%) 66Neuro, Vascular, Neuro, Vascular, Trauma,TransplantTrauma,Transplant 386386 22 (11%)22 (11%) 20 (11%)20 (11%) 2 2
All patientsAll patients 15481548 63 (8%)63 (8%) 35 (5%)35 (5%) 28*28*
** P < 0.04P < 0.04N Engl J Med 2001;345:1359 N Engl J Med 2001;345:1359
LimitationsLimitations
•• Single center, unblinded study Single center, unblinded study •• Relatively high mortality among cardiac Relatively high mortality among cardiac
surgery patients in control group (5.1%)surgery patients in control group (5.1%)•• Immediate postImmediate post--operative operative i.v.i.v. glucose glucose
(200(200--300 g per day: ~ 2 300 g per day: ~ 2 -- 3 L D10 or D20) 3 L D10 or D20) and early feeding (enteral or parenteral)and early feeding (enteral or parenteral)
–– Not routine care for cardiothoracic Not routine care for cardiothoracic surgery patientssurgery patients
N Engl J Med 2001;345:1359 N Engl J Med 2001;345:1359
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevos/GLUCONTROLDevos/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
27 trials of tight 27 trials of tight
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Mackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
20052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
glucose controlglucose control(N = 8315; I(N = 8315; I22 = 17%)= 17%)
OverallOverall
Sensitivity Sensitivity AnalysisAnalysis

1818
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevos/GLUCONTROLDevos/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Devos/GLUCONTROLDevos/GLUCONTROLMackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
2007200720052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
Glucose < 110 mg/dlGlucose < 110 mg/dl 14 trials very tight control14 trials very tight control
OverallOverall
Sensitivity Sensitivity AnalysisAnalysis
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevos/GLUCONTROLDevos/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Mackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
20052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
Glucose < 110 mg/dlGlucose < 110 mg/dlGlucose < 150 mg/dlGlucose < 150 mg/dl 13 trials moderate control13 trials moderate control
OverallOverall
Sensitivity Sensitivity AnalysisAnalysis
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevos/GLUCONTROLDevos/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Mackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
20052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
SurgicalSurgical
Glucose < 110 mg/dlGlucose < 110 mg/dlGlucose < 150 mg/dlGlucose < 150 mg/dl
7 trials in SICUs7 trials in SICUs
OverallOverall
Sensitivity Sensitivity AnalysisAnalysis

1919
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevos/GLUCONTROLDevos/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Devos/GLUCONTROLDevos/GLUCONTROLMackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
2007200720052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
MedicalMedicalSurgicalSurgical
Glucose < 110 mg/dlGlucose < 110 mg/dlGlucose < 150 mg/dlGlucose < 150 mg/dl
8 trials in MICUs8 trials in MICUs
OverallOverall
Sensitivity Sensitivity AnalysisAnalysis
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevos/GLUCONTROLDevos/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Mackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
20052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
MedicalMedicalMed / SurgMed / Surg
SurgicalSurgical
Glucose < 110 mg/dlGlucose < 110 mg/dlGlucose < 150 mg/dlGlucose < 150 mg/dl
12 trials in mixed ICUs12 trials in mixed ICUsOverallOverall
Sensitivity Sensitivity AnalysisAnalysis
MetaMeta--analysis of Tight Glucose Control in Critically Illanalysis of Tight Glucose Control in Critically IllVan den BergheVan den BergheStecherStecherKiaKiaGreyGreyBilottaBilottaBilottaBilottaChanChanVan den BergheVan den BergheFernandezFernandezBlandBlandOksanenOksanenDaviesDaviesWaltersWaltersGray/GISTGray/GIST--UKUKBruno/THISBruno/THISBrunkhorst/VISEPBrunkhorst/VISEPDevosDevos/GLUCONTROL/GLUCONTROL
20012001200620062005200520042004200720072008200820082008
2005200520062006
2005200520072007199119912006200620072007200820082008200820072007
Favors Tight GlucoseFavors Tight Glucose Favors Usual CareFavors Usual Care
RR and 95% CIRR and 95% CI
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933 Relative Risk of Hospital MortalityRelative Risk of Hospital Mortality
Mackenzie/GLYCOGENICMackenzie/GLYCOGENICArabiArabiWangWangYuYuMitchellMitchellDeLaRosaDeLaRosaFarahFarahMcMullin/LOGICMcMullin/LOGICHenderson/SUGARHenderson/SUGARAzevedoAzevedo
20052005200620062006200620052005200620062006200620072007200720072005200520082008
1001000.010.01 0.10.1 11 1010
MedicalMedicalMed / SurgMed / Surg
SurgicalSurgical
Glucose < 110 mg/dlGlucose < 110 mg/dlGlucose < 150 mg/dlGlucose < 150 mg/dl
OverallOverall
Sensitivity Sensitivity AnalysisAnalysis P = NS for allP = NS for all

2020
Tight Glucose Control and Tight Glucose Control and the Risk of Hypoglycemiathe Risk of Hypoglycemia
RR and 95% CIRR and 95% CIHypoglycemiaHypoglycemia
Favors Tight ControlFavors Tight Control Favors Usual CareFavors Usual Care
Glucose goal Glucose goal << 110 mg/dL110 mg/dL
Tight glucose controlTight glucose controlincreasedincreased 7 7 -- 8 fold the risk of 8 fold the risk of
Modified from Wiener RS, Modified from Wiener RS, et al. JAMA 2008; 300:933et al. JAMA 2008; 300:933
OverallOverall
0.010.01 0.10.1 11 1010 100100Relative RiskRelative Risk
Glucose goal Glucose goal << 150 mg/dL150 mg/dLSurgical ICUSurgical ICUMedical ICUMedical ICUMedicalMedical--Surgical ICUSurgical ICU
II22 = 0%= 0%N = 15N = 15
hypoglycemia (< 40 mg/dl) hypoglycemia (< 40 mg/dl) independent of target glucose independent of target glucose ((<< 150 or 150 or << 110 mg/dL) or type 110 mg/dL) or type of ICU (medical, surgical or of ICU (medical, surgical or combined)combined)
NICENICE--Sugar TrialSugar TrialBaseline CharacteristicsBaseline Characteristics
Intensive Intensive InsulinInsulin
ConventionaConventional Insulinl Insulin
Enrolled (N)Enrolled (N) 30543054 30503050Enrolled (N)Enrolled (N) 30543054 30503050SurgicalSurgical 37%37% 37%37%Apache II > 25Apache II > 25 31%31% 31%31%Severe SepsisSevere Sepsis 22%22% 21%21%MechMech VentilatorVentilator 94%94% 94%94%
N Engl J Med 2009; 360:1283N Engl J Med 2009; 360:1283

2121
Intensive Intensive InsulinInsulin
ConvenConven--tional tional
OROR(95% CI)(95% CI)
PP--ValueValue
NICENICE--Sugar TrialSugar TrialOutcomesOutcomes
In 6014 critically ill patients, tight glucose In 6014 critically ill patients, tight glucose control was associated with hypoglycemia control was associated with hypoglycemia
Mortality (90d)Mortality (90d) 27.5%27.5% 24.9%24.9% 1.141.14(1.02 (1.02 -- 1.28)1.28)
0.020.02
HypoglycemiaHypoglycemia 6.8%6.8% 0.5%0.5% 14.714.7(9 (9 -- 25.9)25.9)
<0.001<0.001
N Engl J Med 2009; 360:1283N Engl J Med 2009; 360:1283
and increased mortality at 90 days. and increased mortality at 90 days.
“On the basis of [these] results we do not “On the basis of [these] results we do not recommend use of the lower target (81 recommend use of the lower target (81
-- 110 mg/dL) in critically ill patients.”110 mg/dL) in critically ill patients.”
MetaMeta--analyses of Sepsis Trials analyses of Sepsis Trials with at Leastwith at Least
One Significant Benefical TrialOne Significant Benefical Trial
SummarySummaryAntiAnti--EndotoxinEndotoxin
J5 AntiserumJ5 Antiserum MonoclonalsMonoclonals
** **
p = 0.59p = 0.59 p = 0.60p = 0.60
High DoseHigh DoseCorticosteroidsCorticosteroids
**p = 0.009p = 0.009
Shift from beneficial to last trial, p = 0.003Shift from beneficial to last trial, p = 0.003**
ILIL--1RA1RA
**
p = 0.14p = 0.14
Activated Protein CActivated Protein C
**
p = 0.55p = 0.55
Intensive InsulinIntensive Insulin
**p = 0.32p = 0.32

2222
The randomized control trial minimizes The randomized control trial minimizes bias but does not eliminate the need for bias but does not eliminate the need for reproducibility which is thereproducibility which is the sine qua nonsine qua nonreproducibility which is the reproducibility which is the sine qua nonsine qua non(i.e. the indispensable and essential (i.e. the indispensable and essential condition) of scientific evidencecondition) of scientific evidence