Embed Size (px)
Citation preview

The Special Supplemental Nutrition Program for Women,
Infants, and Children
(WIC)
Meta-Analysis
University of North Florida
Department of Sociology
Nicholas Jones

Table of Contents
Abstract…………………………………………………………...3
Program Processes…………………………………………..4
Program Impact/Outcome…………………………..…..7
Data/Literature………………………………………………..8
Shortcomings………………………………………………....13
Conclusions…………………………………………….……..14
Utilization and Synthesis……………………….….……16
References…………………………………………………….18

Abstract
The Special Supplemental Nutrition Program For Women, Infants, and Children (WIC) was established in
the early 70’s as a response to an increase in reported health issues surrounding pregnant and nursing
women and their children. The majority of these issues were found among low income mothers and
were the result of malnutrition and a lack of education regarding childcare and rearing, ultimately
leading to poor health outcomes for both the mother and child. Poorer health outcomes in poorer
communities creates a deficit in spending where the cost of health care which is normally paid for by
one’s insurance company must instead picked up by the state and/or federal government due to an
individual’s lack of coverage. WIC helps dramatically shrink this deficient by supplementing nutritionally
valuable foods for low income families, educating participants about healthy behaviors and lifestyle
choices, and providing a basis for regular medical examination that aids and reinforces the preventative
care needed by all individuals to maintain good health outcomes. Increased enrollment in WIC,
especially in the early stages fetal development, is associated with a decrease in low and very low
birthrates and fetal and infant mortality. Eligibility cut offs on the state level prevent a large population
of mothers, infants, and children at risk of malnutrition from receiving support. A strong outreach policy
to the entire population at risk would be more favorable than weak policy geared strictly to pregnant
women, but policy amendment must take into account the geographic clustering of poverty as income is
also strongly associated with enrollment.

Program Processes
Mission Statement and Program Theory
The USDA’s Food and Nutrition Service’s website states that WIC aims to “To safeguard the health of
low-income women, infants, and children up to age 5 who are at nutrition risk by providing nutritious
foods to supplement diets, information on healthy eating, and referrals to health care.”
Supplemental nutrition + nutrition education + health monitoring -> better health outcomes for
women, infants, and children at risk of malnutrition
Population
WIC assists nutritionally at risk women during and up to 6 weeks after pregnancy, breastfeeding
women up to their infants 1st birthday, and non-breastfeeding women up to 6 months postpartum. WIC
also assists infants up to their 1st birthday and children up to their 5th birthday. In 2014 there were a
reported 8,258,476 individuals participating in the WIC program consisting of 1,972,833 women,
1,964,393 infants and 4,432,290 children. (NSA 2014)
Eligibility
Must be pregnant and have a family income between 100 and 185% lower than the issued federal
poverty level. (Set by state agency)
Must live in the same state in which they apply
Must be examined by a health professional and evaluated for their risk of malnutrition
Can become eligible through enrollment in other assistance programs such as SNAP, TANF, and
Medicaid

Implementation
WIC is federally funded with a yearly congressional grant. In 1974 the total cost of WIC consisting of
the NSA and all their services along with the total cost of the supplemental food itself was 10 million
dollars. In 2014 that same total exceeded 6.2 billon (FNS yearly fiscal reports) and now funds the efforts
of 90 different state agencies in all 50 states 47,000 retailers 1,900 local agencies and over 10,000 clinic
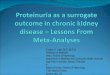
sites. WIC’s annual budget is broken into 7 US regions, each representing a branch office of the NSA. By
far the largest spending is in the South-Eastern region which comprises of Alabama, Florida, Georgia,
Kentucky, Mississippi, North Carolina, South Carolina, Tennessee and the Choctaw MS and Eastern
Cherokee tribes. This is a result of denser populations and concentrated poverty. In 2014 the NSA
estimated that the average cost of supplemental nutrition per person per month was around 43 dollars
(NSA, Table 1)
NSA Regional Branches (NSA) % living in poverty based on 2007 US census (Mulbrandon)
*Any information not exclusively cited by author or study was published by the USDA’s NSA branch and can be found on WIC’s
national web page.

WIC Program Costs per Fiscal Year

Self-Reported Impact and Measurement Criteria
The Food and Nutrition Services branch of the USDA provides extensive state level participation data
and finance reports in accordance with the Office of Policy Support (OPS) which frequently conducts
evaluative research to assess the program and amend policy. Using this collection of data they claim that
participation in the WIC program is associated with:
“Improved birth outcomes and savings in health care costs,” measured by premature births, low birth
weight (LBW) and very low birth weight (VLBW) rates, infant death, and total adverted expenditures.
“Improved diet and diet-related outcomes,” measured by prevalence of anemia and nutrition intake
vs overall caloric consumption.
“Improved infant feeding practices,” measured by breastfeeding rates and rates of use of iron fortified
formula in non-breast feeders.
“Immunization rates and regular source of medical care,” measured by childhood immunization rates
and regularity of medical care.
“Improved cognitive development,” measured by vocabulary scores and memory after 1st year of life.
“Improved preconception nutritional status,” measured by hemoglobin levels and maternal obesity at
onset of subsequent pregnancy.
*All self-reported impacts, criteria, funding and population information accessed through from NSA’s
WIC website.

Literature/Data
The following literature and data have been categorized according to what is addressed
Eligibility
The CPS and SIPP (Current Population Survey and Survey of Income and Program Participation) grossly
undercounts those individuals enrolled and eligible to be enrolled in WIC. Undercounting is due to the
complex matter of determining whether or not an individual is at nutritional risk, a basic criteria of
eligibility. Eligibility also wrestles with the fact that many low income individuals have unstable home
environments and will often live where they receive the most support which can further alter their
eligibility. “The National Survey of WIC Participants implies that over 94 percent of WIC recipients have
incomes below 185 percent of poverty, suggesting that most adjunctively-eligible WIC households would
also be income eligible. The CPS data imply that roughly 13 percent of WIC recipients have incomes
above 185 percent of poverty, while SIPP data imply that 23 percent have incomes above 185 percent of
poverty.” (Bitler 2003: 21) Expanding eligibility to larger populations and increasing participation by
eligible individuals would increase the measurable effectiveness of the program. WIC participant and
program characteristic surveys show that enrollment is higher among Hispanics, African Americans and
married women and lower among Asians and individuals living in metropolitan areas. A lack of reliable
data regarding the income, living, and health statuses of eligible non participants inhibits the program
from reaching a core population at risk.
Access to early prenatal care by WIC is greatly limited. (Ku 1989) There is a correlation between
beginning of enrollment and length during pregnancy with overall birth outcomes. Race, local policy,
and coordination between programs were found unassociated with early enrollment, the only
association being previous enrollment. There is the possibility of using previous participants to as
liaisons to eligible non participants. Overall the benefit of WIC not being fully met. Information collected

on 1,181 pregnant women from 356 clinics in 208 local programs from 28 different states as well as
National Center for Health Statistics data. Suggests strong outreach policy to woman infants and
children better than weak policy geared strictly to pregnant women. Special outreach policy on a local
level also had little effect on early enrollment.
In 2005 Bitler argued that due to limitations set by state agencies larger population of eligible
individuals were still not receiving WIC support. “73 percent of eligible infants, 67 percent of eligible
pregnant and postpartum women, and 38 percent of eligible children one to four receive benefits.”
(Bitler, 2005: 38) Participants who are enrolled in the program are on average economically worse off
than those who are eligible but who do not receive care. WIC is intended to reach the entire population
of women, infants, and children at risk of malnourishment and falling between 100% and 185% below
the poverty line but the majority of those accepted are closer to 185%. Eligibility must be adjusted to
increase the amount of enrollees who are still at risk but who do not reach the level of poverty that is
strongly associated with enrollment. There is an overall lack of data needed to establish a good control
group so comparisons are made to programs like SNAP and TANF on the basis that the alleviation of
food insecurity itself partially deals with malnutrition. Close to a third of eligible WIC recipients receive
food stamps and do not participate in WIC although they are still at risk of malnutrition due to spoilage
and improper diet. This association holds true only if participation in WIC has no effect on household
food insecurity. The CPS and SIPP also underestimate enrollment in these programs, but not to the
degree that they do with WIC.
Impact
Children who participate in WIC program are 5-11 % more likely to be in “excellent health” than those
who do not. (Carlson, 2003: 489) If the income of a family at poverty line level were to double it is
speculated that the likeliness of the children in that same family being in ”excellent health” would only

increase 3-10%. This not only confirms the value of supplemental nutrition and but illustrates its
importance weighed against income alone, though income possesses positive health associations
through indirect effects such as the availability of resources in a particular time of need. Research
indicates that the most substantial positive health benefit associated with participation in WIC is found
among the population with the lowest income, but findings such as these may be erroneous as low
income mothers have lower than average health outcomes when it comes to pregnancy, birthing, and
child rearing.
The relationship between reported enrollment in WIC and birth outcomes in New York City between
1988 and 2001 has been found to be modest at best (Joyce 2005) Using a sample of over 800,000 births
reported by the New York City Department of Health and Mental Hygiene research was aimed at
determining WIC’s association with fetal growth rather than preterm delivery. This was done in an
attempt to separate the perceived and actual effects of the program and New York City was chosen to
better grasp the outcome of WIC in densely populated urban areas, particularly in the northeast region
where enrollment rates are typically higher. Limiting the sample population to women who were
currently receiving Medicade, who had no previous live births, and who had enrolled in prenatal care
within first 4 months of pregnancy greatly reduced the heterogeneity of WIC and non WIC “highly
motivated” mothers. Multiple fetus pregnancies were also taken into account as they were more
commonly associated with a higher risk of mental retardation and anemia. Overall it was concluded that
participation in WIC during the prenatal stages of pregnancy had little effect on birth outcomes in New
York City. The use of such a large data set solidifies these claims but it can never be assumed that what
works in one area will work in another. The overall implication of policy advisors suggesting WIC’s
benefit in regard to fetal development is repeatedly undermined by clinical studies showing that “WIC is
unrelated to fetal growth among singleton births across race and ethnicity…” and that any “…association

between WIC and other less clinically supportable birth outcomes diminished over time and varied by
race and ethnicity.” (Joyce, 2005: 681)
There is a significant association between WIC participation and smoking, weight gain during
pregnancy, birth outcomes and likelihood of breastfeeding. (Joyce 2008) Overall it was found that WIC
possessed lower effects on and associations with health than previously suggested by researchers.
Effects are subject to age gestational biases and while evidence supports the notion that WIC works its
effect is often overestimated. Addressing lifestyle choices and behavior like smoking, diet, breastfeeding,
and immunization is known benefit mothers and children and it is suggested that more resources be
used to emphasis their role in WIC
Meta-Analysis
Avruch (1995) analyzes WIC using 13 studies ranging from 1981-1988 and suggests that the program
reduces low birth rates by 25 percent and very low birth rates by up to 44%. There is an association
between decreased levels of low birth weight in infants and mothers who were enrolled in the program.
LBW averages among WIC and non WIC recipients were totaled, LBW due to VLBW ruled out, and the
proportional average between the two used to calculate probable number of VLBW across each of the
13 studies. Infant survival rates, birth rates and population data including income were compared with
proportional average calculations to estimate whether or not WIC was cost effective. Using this data she
suggests that “prenatal WIC enrollment is estimated to have reduced first year medical costs for U.S.
infants by $1.19 billion in 1992.” (Avruch, 1995: 27) The federal government saves an estimated $.93
and State $.73 on every dollar spent on preventative care through WIC and it is suggested that savings
could reach $804,653,673

Selection bias was found to have an impact on past research and attempts at removing it have been
made, notably that of Yunwei Gai (2012) who examined a birth cohort of 14,000 adolescents in a
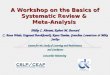
longitudinal study started in 2001. “WIC does not affect average birth weight and average gestational
week after correcting for selection bias using the instrumental variable method. However, WIC
participation has significantly reduced the probability of very premature birth and (very) low birth
weight after controlling selection bias by bivariate probit models.” (Gai, 2012: 61) (Table 2)
BIVARIATE) PROBIT: (VERY) LOW BIRTH
Graph Courtesy of Yunwei Gai, Economics Professor at Babson College

Shortcomings
Impact
Larger differences in health outcomes have been found between WIC and non WIC individuals in
communities with lower than average BWs.
WIC’s impact is exacerbated in poorer states like North Carolina and underestimated in wealthier
ones like Maryland.
WIC’s greatest impact is found among individuals enrolled in Medicaid as well as WIC, a sub-
population whose income is on average lower than those enrolled in WIC alone and is therefore not an
ideal representation of the program’s target population.
The effects of program greatly subject to gestation age
Data
A program intended to suit the needs of an exceptionally large and vulnerable population (8,258,476
individuals) will eventually find itself at the crossroads of available and pertinent data. Because of the
programs relative young age any analysis of WIC must make use of the former rather than the latter and
deeper understanding of its benefits and drawbacks are merely speculative.
The indirect but beneficial associations between income and health greatly underplay the importance
of nutrition
Much of the older state data regarding at risk population uses existing records of Medicare, Medicaid,
TANF, and Food Stamps recipients and must be evaluated differently than if recipients were enrolled
exclusively in WIC.

Using probit models helps eliminates variability which while necessary tends to hide the greater
distribution of participants and emphasize the effect of singled out variables
There is an inadequate amount of data comparing VLBWs of WIC and non WIC recipients and there
are few longitudinal studies that follow large enough populations while also extracting from them the
appropriate data needed to draw conclusions.
Theory/Implementation
By using such a broad theory WIC opens itself up to the possibility of helping a very large population in
need but closes the door to the possibility of reaching them all.
Frequent process evaluation and policy amendment may increase the efficiency of the program and
its ability to reach its target population but by leaving the overall target population relatively unaltered
and its parameters subject to state mandate WIC greatly reduces its ability to progress further.
Conclusion
1. Expanding eligibility further would help reach the larger population in need. An individual’s
eligibility to participate is determined by his or her state of residence and is very much dependent on
how far below the poverty line they fall. The population of eligible individuals has been estimated to be
close to 14 million and while there are already close to 6 million that would benefit from participation it
is suggested that imposing national cutoffs for eligibility at 100% below the poverty line rather than
state selected cutoffs anywhere between 100% and 185% would help reach the larger population at risk.
Supplemental programs like TANF and SNAP have been geared towards feeding lower income
individuals but data suggests that because WIC specifically targets nutrition it is better suited to meet
the needs of its target population. Needs are met through discounted nutritionally rich food items,
increased awareness of good health practices before, during, and after pregnancy, and continual

evaluation and preventative checkups that serve to monitor the well-being of participants whose
financial circumstance may not allow for the acquisition of the resources needed to keep their families
healthy. A balance must be struck between eligibility and financing as too few participants will reduce
the WIC’s beneficial impact and too many will reduce WIC’s perceived impact.
2. There is conclusive evidence that mothers, infant, and children who enroll in WIC have better
health outcomes than those who do not, but any supplemental service will likely aid those in need and
WIC’s true benefit is still up for debate. There is though supporting evidence of a positive association
between enrollment (especially in the early stages of fetal development) and birth weight,
breastfeeding, and immunization. This evidence is also up for debate as birth weight alone is not as
strongly associated with enrollment as very low birth weight, but coupled with definite negative
associations between enrollment and behavior that adversely effects health such as smoking and poor
diet WIC asserts its feasibility for aiding the larger population at risk of malnourishment. The majority of
WIC’s fiscal allotment from congress goes towards purchasing food for participants, each averaging each
close to 43 dollars a month. While this may not seem enough to impact one’s health we must keep in
mind that WIC also supplements formula and that the smaller portion of this allotment goes to the NSA
who help ensure that participants receive educational and medical resources they need as well as fund
frequent program evaluations guarantee impact.
3. The initial cost of WIC is made up for by the resulting savings in health care costs to federal and
state governments that are commonly associated with low birth weight. Regular medical
examinations, preventative care, and dietary education greatly impact the health of individuals and are
associated with better health outcomes. WIC was found to have similar health benefits to increased
income (assuming the income of a family at poverty line were to double) but lacked the secondary

benefits like monetary reserves, health insurance, and available transportation that often come with it.
Better health, regardless of income, means less government spending.
4. The greater a state’s overall poverty, the greater impact WIC will have on its inhabitants. Likewise
the poorer an individual, the greater the impact of WIC. This is primarily because the lower a states
average income the lower the states average birth weight. This holds true with individuals of any state,
but a larger part of the budget is used in regions that have densely populated areas with lower than
average earnings leaving eligible populations elsewhere vulnerable.
Utilization and Synthesis
It is strongly recommended that WIC reevaluate its target population to find an appropriate balance
between eligibility and impact. Decreasing the number of eligibles and moving the cutoff closer to 185%
lower than the poverty line would increase the impact overall but would leave a larger population
vulnerable. Increasing the number of eligibles and moving the cut off closer to 100% would address the
larger population at risk but decrease the impact overall and would lower the per dollar cost/benefit. By
directing more resources to the poorest populations WIC may increase savings to federal and state
governments but not without disadvantaging those who still fall below the poverty line and would
benefit from enrollment. State mandated cutoffs under address the larger population of eligibles, but
national mandate will never be appropriate as it cannot address the disparities in income between
states.
There is great potential for using past participants as liaisons to eligibles who are not enrolled. This
would not only be a cost effective solution as past participants have already received the kinds of
educational resources they need to maintain healthy lifestyle’s, but it would also allow the program to
impact a core population of at risk individuals that would be otherwise hard to reach while providing a
regenerative structure proven effective through facilitation in other social programs.

It is necessary for morality’s sake that a government secure the well-being of its people, but also
economically responsible to ensure that its people need not rely solely on the government. WIC seeks to
relieve those at risk of malnourishment with the nutritious resources they need to achieve healthy
outcomes, but also ensures that they receive the educational resources they need to maintain them. It is
therefore imperative that proper data continue to be collected in order to continue to adjust the
program to meet its maximum potential.

References
Avruch, S., and A.P. Cackley. 1995. "Savings Achieved by Giving WIC Benefits to Women
Prenatally." Public Health Reports 110(1):27-34.
Bitler, M., J. Currie and J. Scholz. 2003. " WIC Eligibility and Participation " Journal of Human
Resources 38(Volatility and Implications for Food Assistance Programs):1139-1179.
Bitler, M., C. Gunderson and G. Marquis. 2005. " Are WIC Nonrecipients at Less Nutritional Risk than
Recipients? an Application of the Food Security Measure." Review of Agricultural
Economics 27(3):433-438.
Carlson, A. and B. Senauer. 2003. "The Impact of the Special Supplemental Nutrition Program for
Women, Infants, and Children on Child Health." American Journal of Agricultural
Economics 85(2):479-491.
Food and Nutrition Services. 2015. "Women, Infants, Children (WIC)." USDA, Retrieved 11/29, 2015.
(http://www.fns.usda.gov/wic/women-infants-and-children-wic).
Gai, Y. and L. Feng. 2012. "Effects of Federal Nutrition Program on Birth Oucomes." Atlantic Economic
Journal 40(1):61-83.
Joyce, T., D. Gibson and S. Colman. 2005. "The Changing Association between Prenatal Participation in
WIC and Birth Outcomes in New York City." Journal of Policy Analysis and Managment 24(4):661-
685.
Joyce, T., A. Racine and C. Yunzal-Butler. 2008. " Reassessing the WIC Effect: Evidence from the
Pregnancy Nutrition Surveillance System " Journal of Policy Analysis and Managment 27(2):277-
303.
Ku, L. 1989. "Factors Influencing Early Prenatal Enrollment in the WIC Program Leighton Ku Public
Health Reports." Public Health Reports 104(3):301-306.

Ludwig, J. and M. Miller. 2005. "Interpreting the WIC Debate Jens Ludwig and Matthew Miller Journal of
Policy Analysis and Management." Journal of Policy Analysis and Managment 24(4):691-701.
Mulbrandon, C. 2007. "United States Poverty Map." VisualizingEconomics, Retrieved 12/7/14, 2014.
(http://visualizingeconomics.com/blog/2007/08/11/united-states-poverty-map).