Embed Size (px)
DESCRIPTION
medical student tutorial
Citation preview
Acc
epte
d A
rtic
le
This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as an 'Accepted Article', doi: 10.1111/codi.12403 This article is protected by copyright. All rights reserved.
Received Date : 24-Jan-2013 Revised Date : 11-Jul-2013 Accepted Date : 03-Aug-2013 Article type : Narrative Review 066-2013.R1
Narrative Review
The SECCA procedure for faecal incontinence: a review
Marco Frascio, MD1, Francesca Mandolfino, MD Ph D1, Mikaela Imperatore, MD1, Cesare
Stabilini, MD, Ph D1, Rosario Fornaro, MD1, Ezio Gianetta, MD1, Steven D Wexner, MD, PhD2.
1. Patologia Chirurgica ad Indirizzo Gastroenterologico , DISC-Department of Surgical Sciences
and Integrated Methodologies , School of Medical and Pharmaceutical Sciences ,University of
Genova , Largo Rossana Benzi 8, 16132 Genova - Italy
2. Department of Colorectal Surgery, Cleveland Clinic Florida, Weston, USA
Correspondence:
Marco Frascio, MD
Patologia Chirurgica ad Indirizzo Gastroenterologico
DISC-Department of Surgical Sciences and Integrated Methodologies
School of Medical and Pharmaceutical Sciences
University of Genoa
Largo Rossana Benzi 8
16132 Genova – Italy
Phone +1-954-659-56409
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Email: [email protected]
Authors’ contribution:
Marco Frascio: Study conception and design, Acquisition of data, Analysis and interpretation of
data, Writing manuscript
Francesca Mandolfino: Study conception and design, Acquisition of data, Analysis and
interpretation of data
Mikaela Imperatore: Study conception and design, Acquisition of data, Analysis and
interpretation of data
Cesare Stabilini: Study conception and design, Acquisition of data, Analysis and interpretation of
data
Rosario Fornaro: Study conception and design, Acquisition of data, Analysis and interpretation
of data
Ezio Gianetta: Study conception and design, Acquisition of data, Analysis and interpretation of
data
Steven D Wexner: Study conception and design; Manuscript writing
Disclosures:
Marco Frascio, MD: None
Francesca Mandolfino: None
Mikaela Imperatore: None
Cesare Stabilini: None
Rosario Fornaro: None
Ezio Gianetta: None
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Steven D. Wexner: Paid consultant, Mediri Therapeutics, Medtronic Corp, Incontinence Devices,
Renew medical, and Salix Pharmaceuticals.
Running head: The SECCA procedure for fecal incontinence: a review
ABSTRACT
Aim: The SECCA system is a treatment option for patients suffering from fecal incontinence,
introduced into clinical practice in 2002. Clinical studies of radiofrequency energy to treat
patients with fecal incontinence have been published. This article aimed to review all published
series to assess the results of this treatment.
Method: Twelve studies were included. Outcomes analyzed included quality of life, Wexner
incontinence score, anorectal manometry, and endoanal ultrasound findings.
Results: A total of 220 patients from 10 studies were included. In the majority of clinical studies,
the SECCA procedure has been shown to effectively treat mild-to-moderate fecal incontinence.
Conclusions: When patient selection is appropriate, this treatment has demonstrated clinically
significant improvements in symptoms as demonstrated by statistically significant reductions in
the Wexner incontinence and quality of life scores.
Key words: FAecal incontinence; Wexner incontinence score; Quality of life score;
Radiofrequency; SECCA procedure
Introduction
Faecal incontinence (FI) is defined as recurrent and uncontrolled passage of solid or liquid stool
persisting for at least one month. Although not life threatening, it can seriously adversely affect
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
quality of life (QOL) and frequently results in disability. Its incidence has been reported in
community-based studies to range from 2% to 17%. It occurs more frequently among the elderly
and in females.1 In particular, a recent Nielsen-conducted household survey study has shown that
nearly 20% of mature American women suffer from troublesome leakage of stool.2 Treatment
normally depend on the specific cause of the FI and various modalities are used, including
medical treatment, biofeedback, and surgery. Patients with FI are generally initially managed
with non-invasive low-risk treatments, including diet modification, antimotility agents, pelvic
floor exercises, biofeedback, or controlled evacuation.3,4 However, there are no randomized
controlled trials available and there are no internationally and universally accepted guidelines for
the treatment of FI.
The SECCA procedure, which involves the administration of temperature-controlled
radiofrequency (RF) energy to the anal canal, was first used for the treatment of FI in Mexico in
1999. The predicate RF procedure, Stretta, revealed a therapeutic effect in the treatment of
gastroesophageal reflux.5 In 2002, the Food and Drug Administration (FDA) of the United States
approved the SECCA system for use specifically in the treatment of patients with FI to solid or
liquid stool occurring at least once per week, and who already had failed more conservative
therapies.
The therapeutic effect of the procedure has been related to the improvement of sphincter function
and restored anorectal sensitivity. Various modes of actions have been proposed including an
improvement in anorectal sensation and coordination through C and A delta afferent fibre
neuromodulation, collagen and smooth muscle remodeling and a modulation of interstitial Cajal
cell function. RF also induces fibrosis and this may help continence 6.
The current review has been conducted to analyze the safety and efficacy of the SECCA
procedure for the treatment of FI.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Method Literature search
A comprehensive and systematic search of the English literature, indexed in PubMed and
Medline databases (2002 - 2012), was undertaken in July 2012 with the key terms ‘SECCA’ and
‘Radiofrequency fecal incontinence’. Owing to the paucity of publications, all English-language
publications were included in this review. The small number of studies precluded the creation of
a flow diagram. The studies are listed in Table 1 and include the level of evidence for each
study. The reference list of each article obtained was assessed for further potential studies. The
search included all clinical studies available in the literature. All studies demonstrated adequate
quality methodology. Eight groups reported their own (single) experience, while two by Efron et
al10,11 and one by Parisien and Corman12 were based on data from several centres. The full text
and abstract of each publication were reviewed.
Published results on the SECCA procedure
Ten clinical studies published between 2002 and 2011 on the SECCA procedure for FI were
included. Takahashi et al7 conducted a pilot study on 10 patients treated by the SECCA
procedure. There was a substantial improvement in the FI-related QOL (lifestyle (from 2.3 to
3.4), coping (from 1.4 to 2.7), depression (from 2.2 to 3.5), and embarrassment (from 1.3 to 2.8);
P < 0.05 for all parameters). Median discomfort by visual analogue scale (0–10) was 3.8 during
and 0.9 two hours after the procedure. Bleeding occurred in four patients (14–21 days after the
procedure) with spontaneous resolution in three patients, while suture ligation was necessary in
one patient.
At 12 months, the median Wexner incontinence score improved from 13.5 to 5 (P < 0.001), with
80% of patients considered to be responders. All protective pad use was eliminated in five of the
seven who used this precaution at baseline. At six months, there was a significant reduction in
initial and maximum tolerated rectal distension volume. Anoscopy was normal in all patients at
six months. The same group subsequently presented their results of a two-year follow-up8
suggesting that the improvement in symptoms of FI and QOL persisted for at least two years

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
after RF delivery to the anal canal. At five-year follow-up, in 2008,9 the mean Wexner
incontinence score had improved from 14 to 8 (P<0.00025) with 16 (84.2%) patients
demonstrating more than 50% improvement. All FI-related QOL scores improved, including
lifestyle (2.43 to 3.15; P<0.00075), coping (1.73 to 2.6; P<0.00083), depression (2.24 to 3.15;
P<0.0002), and embarrassment (1.56 to 2.51; P<0.0003). The social function component of the
Short-Form 36 (SF-36) improved from 38.3 to 60 (P<0.05). There was a trend toward
improvement in the mental component summary of the SF- 36 from 38.1 to 48.14. No long-term
complications were reported. The series from Takahashi and his group9 is the longest follow-up
study to date and also presented the most favorable results of RF treatment.
Between 2003 and 2006, three studies were published 10,11 12 13. The multicenter study conducted
by Efron et al10 enrolled 50 patients across five centers. All patients reported FI at least once per
week for a minimum of three months and medical and/or surgical management had failed. At
baseline and six months patients completed Wexner incontinence score [0-20], the Fecal
Incontinence Quality of Life (FIQOL) scale, the SF-36 and visual analog scale questionnaire.
They underwent anorectal manometry, endoanal ultrasound, and pudendal nerve terminal motor
latency (PNTML) testing. At six months, the mean Wexner incontinence score had improved
from 14.5 to 11.1 (P<0.0001). All parameters in the FIQOL scales were improved [lifestyle
(from 2.5-3.1; P<0.0001); coping (from 1.9-2.4; P<0.0001), depression (from 2.8-3.3;
P=0.0004); embarrassment (from 1.9-2.5; P<0.0001)]. Responders, as assessed by a systematic
referenced analogue scale, reported a median 70% resolution of symptoms. The mean SF-36
social function score improved from 64.3 to 76 (P+0.003). There were no changes in endoanal
ultrasound, PNTML assessment, or anal manometry. Complications included mucosal ulceration
(n=1: superficial with underlying muscle injury) and delayed bleeding (n=1). This multicentre
trial concluded that RF energy could be safely delivered to the lower rectum and anal canal and
that the SECCA procedure significantly improved the Wexner incontinence score and overall
QoL for most patients who underwent this procedure.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
The second multicenter study11 involved five centres including 50 patients (43 female) with FI,
all of whom had failed medical or surgical management. At baseline and at six months, the
patients completed the Wexner incontinence score and the FIQOL questionnaires and the SF-36
questionnaire. All patients underwent anorectal manometry, PNTML, and anorectal ultrasound
testing at baseline and six months. At six months, the mean Wexner incontinence score had
improved from 14.5 to 11.1 (p<0.0001). All parameters in the FIQOL were improved (p<0.001).
There was an overall statistically significant improvement in the number of days with FI, flatus
incontinence, the incidence of pad soiling, number of days with urgency and number of days
with fear of FI. With the exception of data from one centre, no objective changes were noted in
physiologic studies with the exception that resting anal sphincter length increased by 25%.
Complications included mucosal ulceration (n=2) and delayed bleeding (n=1).
In 2006, a Dutch group13 published the results of 11 females with FI treated by SECCA. The
authors gave oral antibiotics eight hours before and eight hours after the procedure. At three
months six of 11 patients were improved and five were not. This persisted during follow up to
six to nine months. At three months, the Vaizey score fell from 19 to 15 (p=0.056) and in
improved patients from 18.3 to 11.5 (p<0.001). Side effects included local haematoma formation
(n=2), bleeding for 3 days (n=1), pain persisting 2-3 weeks (n=4) and laxative-related diarrhoea
for one to three weeks (n=4). They concluded that the SECCA procedure seemed promising.
Similar positive results was noted by Walega et al,14 who reported on a 20 patient clinical study.
They observed no intra or postoperative complications. During postoperative follow-up, three
patients developed minor complications, which did not require surgical intervention. The degree
of bowel control assessed by the Wexner incontinence score significantly improved. The overall
Fecal Incontinence Severity Index (FISI) score was not statistically significant. Six months after
surgery, a clear improvement in QOL was noted compared to the preoperative status in all
FIQOL components (Lifestyle, Coping, Depression, and Embarrassment). A significant increase
of basal anal pressure (BAP) and squeeze anal pressure (SAP) was noticed after six months. In
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
addition, the high pressure zone length significantly increased throughout the entire follow-up
period. The authors stressed that, prior to surgery, none of the patients had normal rectoanal
inhibitory reflex (RAIR) whereas six months after the SECCA procedure, a gradual return and
normalization of the RAIR was observed. The RAIR was still absent in six patients and a
paradoxical RAIR was noted in the remaining eight.
Ruiz et al15 showed an improvement in the FIQOL score in all components except for depression
indicating a positive impact on QoL. Twenty four patients were included in the study and 16
were available for 12 month follow-up. Although the Wexner incontinence score fell from 15.6
to 12.9, most patients continued to have moderate FI. The improvement in three of four QoL
subscales may indicate that even this modest improvement in FI translated into significant
improvements in daily life.
Lefebure et al16 presented a single centre, non-randomized prospective clinical study which
reported the results in 15 patients at 12 months. The mean Wexner incontinence score fell from
14.07 (±4.5) at baseline to 12.33 (±4.6) at one year (p=0.02). The mean FIQOL score had only
improved in the domain of depression. There were no changes on endoanal ultrasound and
anorectal manometry. Early postoperative complications included self-limiting minor rectal
bleeding and anal pain in 10% to 45% of patients.
Very different results were reported from a prospective study of eight patients.17 At six-months
FI measured by the FISI showed no improvement. FIQOL score showed improvements only in
the embarrassment scale. Neither anorectal manometry nor endoanal ultrasonography showed
any functional or anatomic improvement of the anal sphincter. When compared with previous
studies, the SECCA procedure resulted in a relatively poor outcome. The authors also
documented a significantly higher complication rate compared with other studies. This study
had certain limitations. First, the number of patients was small and the duration of follow-up was
relatively when compared with other studies. All previous studies excluded patients who suffered
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
from inflammatory bowel disease, chronic diarrhoea, chronic constipation, history of laxative
abuse and pelvic irradiation.
Discussion
Patient selection was similar in almost all studies included in this review, with the exception of
the study by Kim et al, which included all incontinent patients regardless of aetiology. In the
others the exclusion criteria were inflammatory bowel disease, chronic diarrhoea, chronic
constipation, history of laxative abuse, and pelvic irradiation.
All studies reported SECCA to be an easy, well-tolerated and safe procedure.
The same technique of RF energy (RFE) delivery was used in all the studies. Power to the
electrode is automatically discontinued when the temperature exceeds 85°C. The mucosa is
constantly cooled by chilled water (45 mL/min) at the base of each needle. The aim is the muscle
while preserving the mucosal integrity via surface irrigation. Once the needles are inserted into
the anal sphincter, each creates a thermal lesion in all four quadrants between 2 cm and 1.5 cm
above and below the dentate line.
SECCA is targeted to the smooth and striated muscle of the anal sphincter and on the collagen
component. Thus, sufficient muscle must be present for the treatment to be feasible. The role of
physiologic and functional testing is uncertain. The results of manometry, endoanal ultrasound,
and PNTML testing are not useful, in contrast more uniform results have been collected by QoL
questionnaire.
Improvement following the SECCA procedure persists for at least six months and seems to
continue for five further years. Nevertheless in judging the technique, the present review
included only11 articles containing 220 patients with only 39 followed for five years. The short
duration of follow up might be explained by the fact that the company producing the SECCA
device was no longer active from the late 1990s and clinical research was halted. This may
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
explain why there are no published randomized or controlled large series. For this reason, we
reviewed the available data after the SECCA device was re-introduced into the market. Another
crucial point is the follow up flowchart in which manometry and endoanal ultrasound were used
as end points. Anorectal manometry was stated to demonstrate a significant improvement of
rectal sensitivity by Felt Bersma et al13 and Walega et al14. These studies indicated that good
part of the improvement was due to improvements of basal anal pressure (BAP), squeeze
pressure (SAP) and rectal compliance (RC). Sphincter length or thickness determined by
endoanal ultrasound did not show any change indicating that this form of assessment is of little
value.
Despite the small number of patients and the short follow up in the studies included in this
review, the results seem to be encouraging in well-selected patients with FI, who have adequate
muscle or collagen tissue for the RF action to take effect. As shown in Table 1, early
postoperative complications included minor rectal bleeding and anal pain in 10% to 45% of
patients. Nearly all were self-limited. Anal pain usually resolved spontaneously within one week
of the procedure.
According to these observations, a major advantage of SECCA compared with other treatments
such as bulking injections, sacral nerve stimulation (SNS), and surgery, is the relatively low
morbidity.18 Reports of several bulking 19,20, 21 demonstrate variability in the method of
application making interpretation of the results difficult. In a study of 136 patients 52% treated
with NASHA Dx experienced a 50% reduction in incontinence episodes, compared with 31%
treated with placebo. Although these results were statistically significant, the clinical relevance
has been questioned as the patient-reported outcome was not included and no anorectal
physiological tests were undertaken. SNS F22,26 and surgical repair are more invasive treatments
and the results are not uniformly satisfactory. 27 RF may be an initial option prior these are
considered.
Despite the small number of patients reported in the literature to have had the SECCA procedure
and the short period of follow up, the available data on RF for FI in appropriately selected
patients indicates a trend towards improvemtn of symptoms and QoL.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
References
1. Nelson R, Norton N, Cautley E, Furner S. Community-based prevalence of anal
incontinence. JAMA 1995;274:559–61.
2. Brown HW, Wexner SD, Segall MM, Brezoczky KL, Lukacz ES. Accidental bowel
leakage in the mature women's health study: prevalence and predictors Int J Clin Pract.
2012;66(11):1101-8.
3. Jorge JM, Wexner SD. Etiology and management of fecal incontinence. Dis Colon
Rectum 1993;36:77-97.
4. Rockwood TH, Church JM, Fleshman JW, Kane RL, Mavrantonis C, Thorson AG,
Wexner SD, Bliss D, Lowry AC.. Fecal Incontinence Quality of Life Scale: quality of life
instrument for patients with fecal incontinence. Dis Colon Rectum 2000;43:9-17.
5. Triadafilopoulos G, Dibaise JK, Nostrant TT, Stollman NH, Anderson PK, Edmundowicz
SA, Castell DO, Kim MS, Rabine JC, Utley DS.. Radiofrequency energy delivery to the
gastroesophageal junction for the treatment of GERD. Gastrointest Endosc 2001;53:407-
15
6. Arts J, Bisschops R, Blondeau K, Farré R, Vos R, Holvoet L, Caenepeel P, Lerut A, Tack
J.. A double-blind sham-controlled study of the effect of radiofrequency energy on
symptoms and distensibility of the gastro-esophageal junction in GERD. Am J
Gastroenterol 2012 Feb;107(2):222-30
7. Takahashi T, Garcia-Osogobio S, Valdovinos MA, Mass W, Jimenez R, Jauregui LA,
Bobadilla J, Belmonte C, Edelstein PS, Utley DS . Radiofrequency Energy Delivery to
the Anal Canal for the Treatment of Fecal Incontinence. Dis Colon Rectum 2002;45:915-
922
8. Takahashi T, Garcia-Osogobio S, Valdovinos MA, Belmonte C, Barreto C, Velasco L..
Extended Two-Year Results of Radio-Frequency Energy Delivery for the Treatment of
Fecal Incontinence (the SECCA Procedure). Dis Colon Rectum 2003;46:711-715
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
9. Takahashi-Monroy T, Morales M, Garcia-Osogobio S, Valdovinos MA, Belmonte C,
Barreto C, Zarate X, Bada O, Velasco L. SECCA Procedure for the Treatment of Fecal
Incontinence: Results of a Five-Year Follow-Up. Dis Colon Rectum. 2008;51(3):355-9.
Epub 2008 Jan 19
10. Efron JE, Corman ML, Fleshman J, Barnett J, Nagle D, Birnbaum E, Weiss EG,
Nogueras JJ, Sligh S, Rabine J, Wexner SD.. Safety and Effectiveness of Temperature-
Controlled Radiofrequency Energy Delivery to the Anal Canal (Secca Procedure) for the
Treatment of Fecal Incontinence. Dis Colon Rectum 2003;46(12):1606-16; discussion
1616-8
11. Efron JE. The SECCA Procedure: A New Therapy for Treatment of Fecal Incontinence.
Surg Tech Intl XIII December 2004;107-110
12. Parisien CJ, Corman ML. The SECCA procedure for the treatment of fecal incontinence:
definitive therapy or short-term solution. Clin Colon Rectal Surg 2005;18(1):42-5
13. Felt-Bersma RF, Mulder CJ. Temperature controlled radiofrequency energy (Secca®) to
the anal canal for the treatment of fecal incontinence: pilot seems promising. Presented at
DDW 2006
14. Walega P, Jasko K, Kenig J, Herman RM, Nowak W. Radiofrequency waves in the
treatment of faecal incontinence. Preliminary report. Proktologia 2009;10(2):134-143
15. Ruiz D, Pinto RA, Hull TL, Efron JE, Wexner SD.,Does the Radiofrequency Procedure
for Fecal Incontinence Improve Quality of Life and Incontinence at 1-Year Follow-Up?
Dis Colon Rectum 2010; 53:1041-1046
16. Lefebure B, Tuech JJ, Bridoux V, Gallas S, Leroi AM, Denis P, Michot F. . Temperature-
controlled radio frequency energy delivery (Secca® procedure) for the treatment of fecal
incontinence: results of a prospective study. Int J Colorectal Dis 2008;23:993–997
17. Kim DW, Yoon HM, Park JS, Kim YH, Kang SB.. Radiofrequency energy delivery to
the anal canal: is it a promising new approach to the treatment of fecal incontinence? Am
J Surg 2009;197(1):14-8

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
18. NICE Clinical Guidelines, National Collaborating Centre for Acute Care (UK). Faecal
Incontinence: The Management of Faecal Incontinence in Adults. 2007, No 49.
19. Vaizey CJ, Kamm MA. Injectable bulking agents for treating faecal incontinence. Br J
Surg 2005;92:521–527
20. Danielson J, Karlbom U, Sonesson AC, Wester T, Graf W. Submucosal injection of
stabilized nonanimal hyaluronic acid with dextranomer: a new treatment option for fecal
incontinence. Dis Colon Rectum 2009;52:1101–1106
21. Graf W, Mellgren A, Matzel KE, Hull T, Johansson C, Bernstein M, NASHA Dx Study
Group. Efficacy of dextranomer in stabilised hyaluronic acid for treatment of faecal
incontinence: a randomised sham-controlled trial. Lancet 2011;19:997–1003
22. Conaghan P, Farouk R. Sacral nerve stimulation can be successful in patients with
ultrasound evidence of external anal sphincter disruption. Diseases of the Colon and
Rectum 2005;48(8):1610-4.
23. Ganio E, Ratto C. Neuromodulation for fecal incontinence: outcome in 16 patients with
definitive implant: the initial Italian Sacral Neurostimulation Group (GINS) experience.
Dis Col Rectum 2001;44(7):965-70
24. Jarrett MED, Matzel KE, Christiansen J, Baeten C-GM, I, Rosen H, Bittorf B, Tösser M,
Madoff R, Kamm MA.. Sacral nerve stimulation for faecal incontinence in patients with
previous partial spinal injury including disc prolapse. Br J Surg 2005;92(6):734-9.
25. Jarrett MED, Matzel KE, Stösser M, Baeten CGMI, Kamm MA. Sacral nerve stimulation
for fecal incontinence following surgery for rectal prolapse repair: a multicenter study.
Dis Colon Rectum 2005;48(6):1243-8.
26. Jarrett MED, Mowatt G, Glazener C-MA, Fraser C, Nicholls RJ, Grant AM et al.
Systematic review of sacral nerve stimulation for faecal incontinence and constipation. Br
J Surg 2004;91(12):1559-69.
27. Adang EMM, Engel GL, Konsten J, Baeten CGMI. Quality of life after dynamic
graciloplasty for faecal incontinence: First results. Theoretical Surgery 1993;8(3):122-4.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
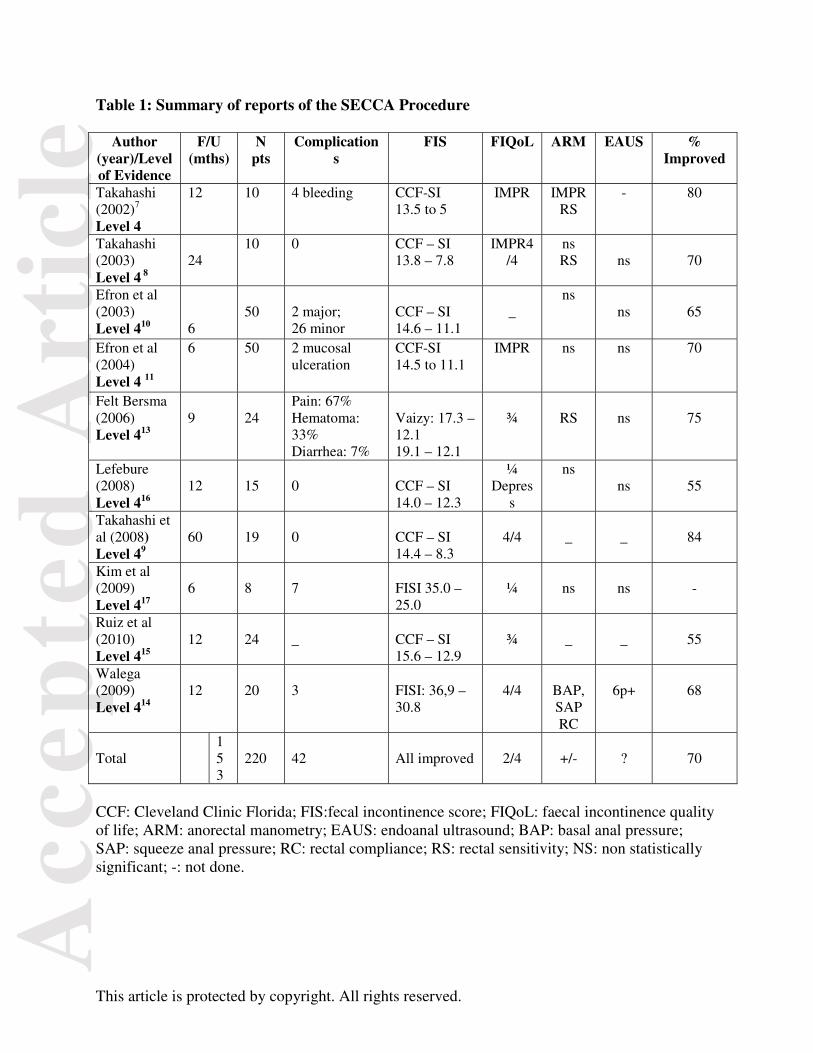
Table 1: Summary of reports of the SECCA Procedure
Author (year)/Level of Evidence
F/U (mths)
N pts
Complications
FIS FIQoL ARM EAUS % Improved
Takahashi (2002)7 Level 4
12 10 4 bleeding CCF-SI 13.5 to 5
IMPR IMPR RS
- 80
Takahashi (2003) Level 4 8
24
10 0 CCF – SI 13.8 – 7.8
IMPR4/4
ns RS
ns
70
Efron et al (2003)
Level 410
6
50
2 major; 26 minor
CCF – SI 14.6 – 11.1
_
ns
ns
65
Efron et al (2004) Level 4 11
6 50 2 mucosal ulceration
CCF-SI 14.5 to 11.1
IMPR ns ns 70
Felt Bersma (2006)
Level 413
9
24
Pain: 67% Hematoma: 33% Diarrhea: 7%
Vaizy: 17.3 – 12.1 19.1 – 12.1
¾
RS
ns
75
Lefebure (2008)
Level 416
12
15
0
CCF – SI 14.0 – 12.3
¼ Depres
s
ns ns
55
Takahashi et al (2008)
Level 49
60
19
0
CCF – SI 14.4 – 8.3
4/4
_
_
84
Kim et al (2009)
Level 417
6
8
7
FISI 35.0 – 25.0
¼
ns
ns
-
Ruiz et al (2010)
Level 415
12
24
_
CCF – SI 15.6 – 12.9
¾
_
_
55
Walega (2009)
Level 414
12
20
3
FISI: 36,9 – 30.8
4/4
BAP, SAP RC
6p+
68
Total
153
220
42
All improved
2/4
+/-
?
70
CCF: Cleveland Clinic Florida; FIS:fecal incontinence score; FIQoL: faecal incontinence quality of life; ARM: anorectal manometry; EAUS: endoanal ultrasound; BAP: basal anal pressure; SAP: squeeze anal pressure; RC: rectal compliance; RS: rectal sensitivity; NS: non statistically significant; -: not done.