Embed Size (px)
Citation preview
Evaluating a School-based Cognitive Behavioural Therapy for Anxiety in Adolescents with Autism Spectrum Disorder
Hanna Kovshoff & Julie A. Hadwin
Centre for Innovation in Mental Health
Scottish Autism Research Group (SARG)
2nd March, 2017
Outline of talk
• Anxiety and Autism
• Evaluation of a manualised CBT intervention in a
mainstream school
• Related work- overview of our research programme @ CIMH
Anxiety Disorder
• Anxiety categories include
– Generalised anxiety disorder, Specific phobia, Social anxiety disorder, Separation anxiety disorder
• Core anxiety features
– Physiological change, intrusive worrisome thoughts, behavioural avoidance
• Attentional characteristics
– Lowered attentional control and increased attention to threat
• Poorer Outcomes
– social and educational underachievement
Autism Spectrum Disorder and Anxiety
• High prevalence of co-occurring psychiatric conditions
• Anxiety is one of the primary reasons for mental health referrals (Skokauskas & Gallagher, 2012)
• Anxiety contributes to functional impairment over and above any functional impairment associated with the ASD symptoms– Up to 84% of children with ASD experience some
degree of impairing anxiety (White et al., 2009)
– 42% (Simonoff et al., 2008) – 55% (De Bruin et al., 2007) Anxiety disorder
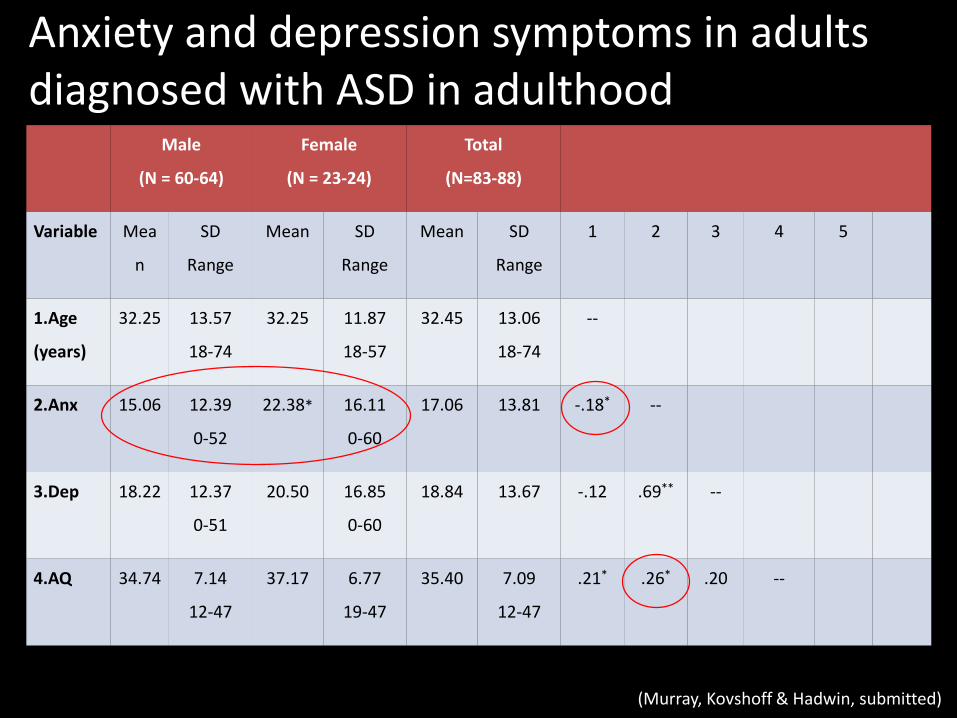
Anxiety and depression symptoms in adults diagnosed with ASD in adulthood
Male
(N = 60-64)
Female
(N = 23-24)
Total
(N=83-88)
Variable Mea
n
SD
Range
Mean SD
Range
Mean SD
Range
1 2 3 4 5
1.Age
(years)
32.25 13.57
18-74
32.25 11.87
18-57
32.45 13.06
18-74
--
2.Anx 15.06 12.39
0-52
22.38* 16.11
0-60
17.06 13.81 -.18* --
3.Dep 18.22 12.37
0-51
20.50 16.85
0-60
18.84 13.67 -.12 .69** --
4.AQ 34.74 7.14
12-47
37.17 6.77
19-47
35.40 7.09
12-47
.21* .26* .20 --
(Murray, Kovshoff & Hadwin, submitted)
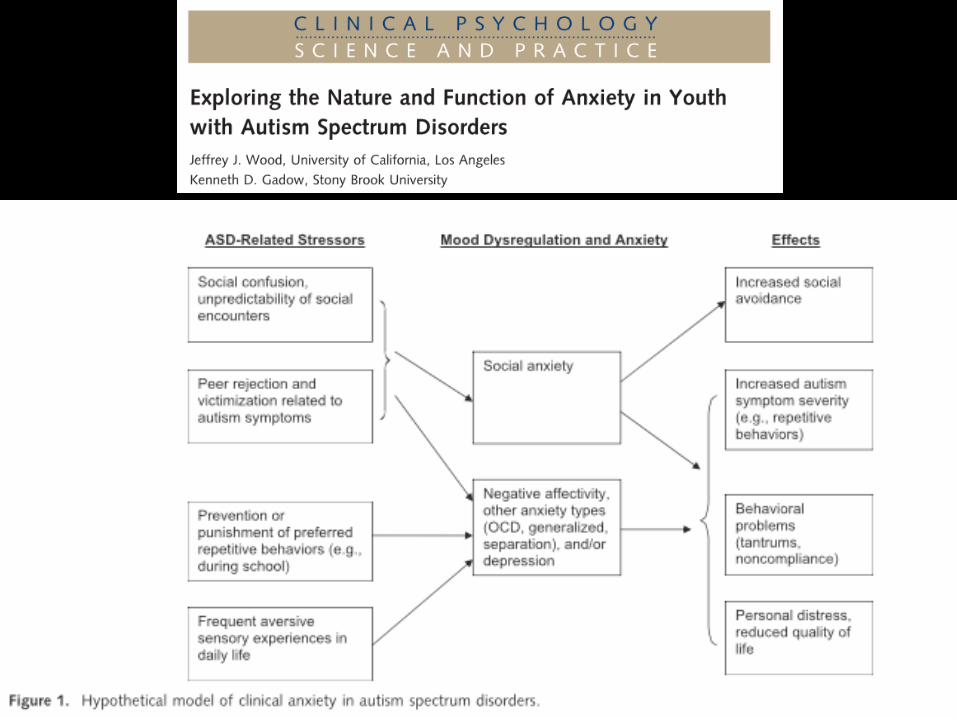
Challenges to Identifying Anxiety in ASD• Diagnostic overshadowing
– Overlapping symptoms – e.g. social phobia, perseverative thinking
• True comorbidity?
– Phenotypically and etiologically identical to anxiety in TD populations?
• ASD specific variant of anxiety?
– Anxiety phenotypically altered by the ASD
– not a manifestation of the ASD
• Specific phenotype/subtype of ASD?
– Differing etiology from those with ASD who do not experience anxiety rather than true comorbidity
(Wood & Gadow, 2010)
Treatment Approaches –Cognitive Behaviour Therapy (CBT)
• The efficacy of CBT for childhood anxiety is well supported in the literature (Cartwright-Hatton et al., 2004)
• Addresses behavioural manifestations of anxiety and underlying maladaptive cognitions
• Efficacy of CBT for children with ASD (with careful adaptations to accommodate unique needs of children with ASD) – Meta-analysis (Sukhodolsky et al 2013) 1.21 for clinician
reported outcomes and 1.19 for parent reported outcomes 0.68 self report
• Effect of CBT on school based samples?
Study Aims – CBT for Anxiety in Mainstream Schools
• CBT intervention group vs a wait-list control group– RCT design
• Primary outcome– Anxiety symptoms across three time-points: pre-intervention,
post-intervention and 6 week follow-up
• Secondary outcomes including– social worry– social responsiveness– attentional control– attention to threat.
• Where possible to gather reports of symptoms/impairment across informants
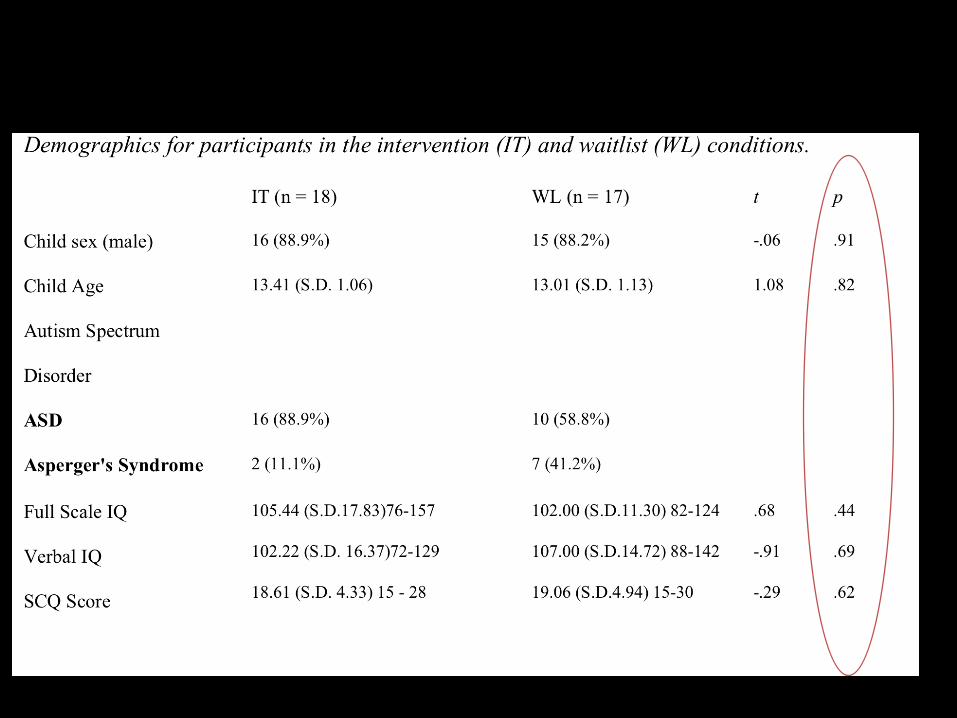
Participants• Inclusion criteria
- Formal clinical diagnosis of ASD (validated through the SCQ)
- Experiencing clinically significant symptoms of anxiety as measured by elevated scores on either teacher or parent measures
- Verbal and total IQ >70
• 35 participants in total– recruited from four mainstream secondary schools located
within the south-east of England
– 31 boys and 4 girls (Mean age = 13.2, SD = 1.1, range = 11.1 -15.8)
Methodology - Primary
Pre-Assessment Measures:
Social Communication Questionnaire (SCQ; Rutter, Bailey & Lord, 2003)
Weschler Abbreviated Scale of Intelligence – second edition (WASI-II; Weschler, 1999)
Anxiety:
School Anxiety Scale—Teacher Report (SAS-TR; Lyneham, Street, Abbott & Rapee, 2008
Spence Children's Anxiety Scale (SCAS; Spence, 1998
Spence Child Anxiety Scale for Parents (SCAS-P; Spence, 1998)
Methodology - Secondary• Social Responsiveness:
– Social Responsiveness Scale (SRS, Constantino & Gruber, 2002)
– measures the severity of ASD symptoms as they occur in natural social settings
– assesses social awareness, social information processing, capacity for reciprocal social communication, social anxiety/avoidance, and autistic preoccupations and traits
• Social Worry:– Social Worries Questionnaire (SWQ - P; Spence, 1995)– Assesses social anxiety
• Attentional control:– Flanker (Erikson & Schultz, 1979)
• Attention to threat:– Schematic Emotional Face Stroop Task
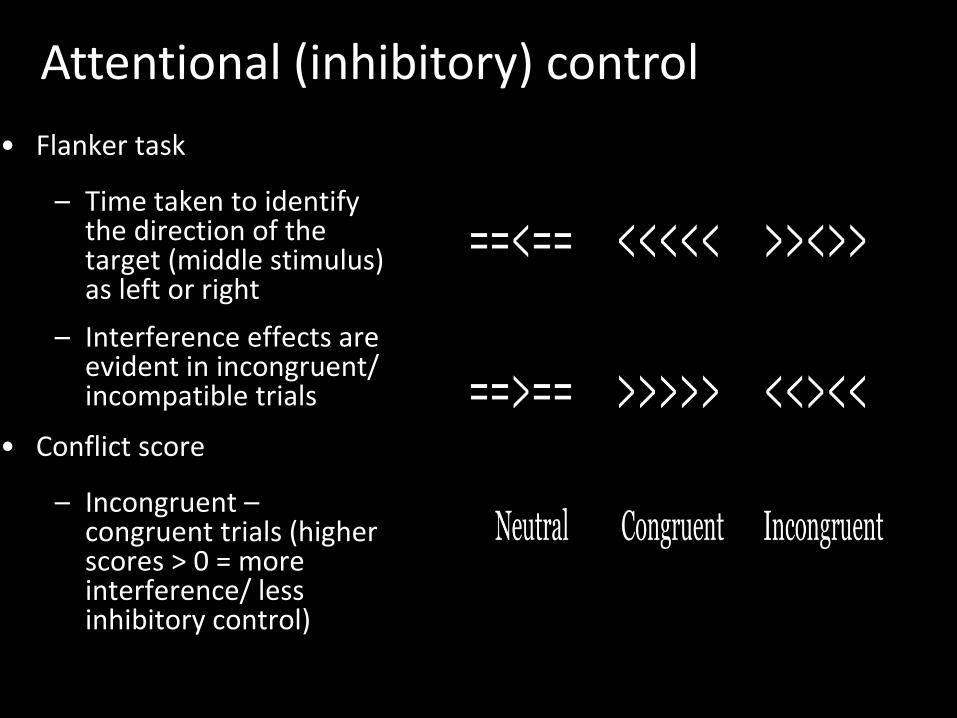
Attentional (inhibitory) control
• Flanker task
– Time taken to identifythe direction of the target (middle stimulus) as left or right
– Interference effects are evident in incongruent/ incompatible trials
• Conflict score
– Incongruent –congruent trials (higherscores > 0 = more interference/ lessinhibitory control)
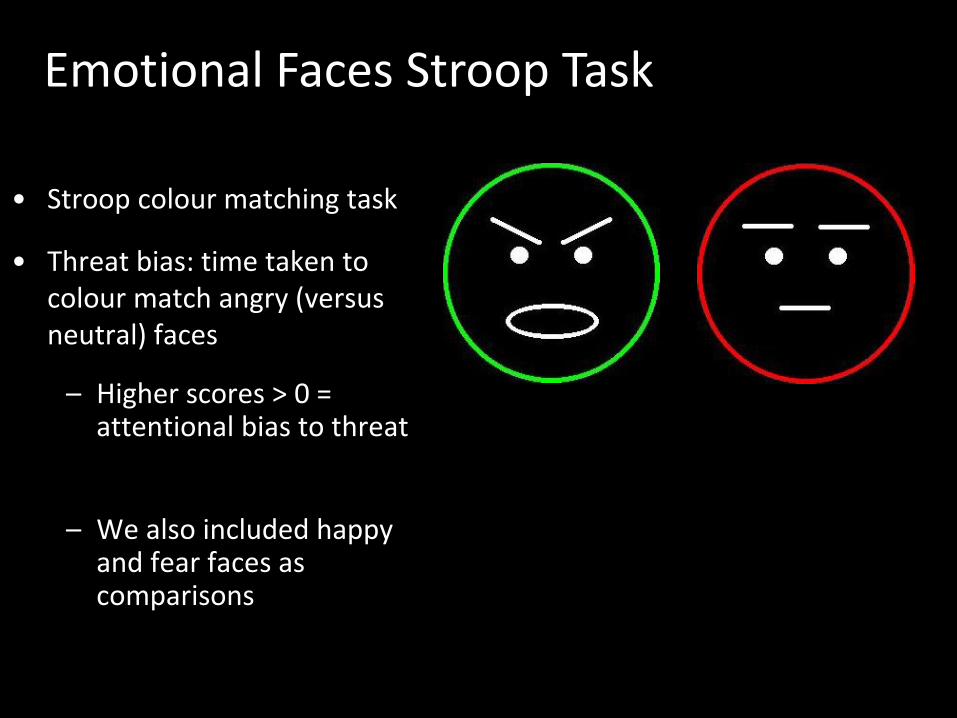
Emotional Faces Stroop Task
• Stroop colour matching task
• Threat bias: time taken to colour match angry (versus neutral) faces
– Higher scores > 0 = attentional bias to threat
– We also included happy and fear faces as comparisons
– 6 week programme x 1.5 hour sessions/6 week follow up
– 4-6 participants per group
– Understand the specific feelings of being happy, relaxed and anxious
– ‘Tool Box' of anxiety management strategies
– Reduction in parent-report anxiety and self-report social worry for the intervention group (n = 23) in comparison to the wait-list group (n = 23)
– Our aim – to deliver intervention in the school setting
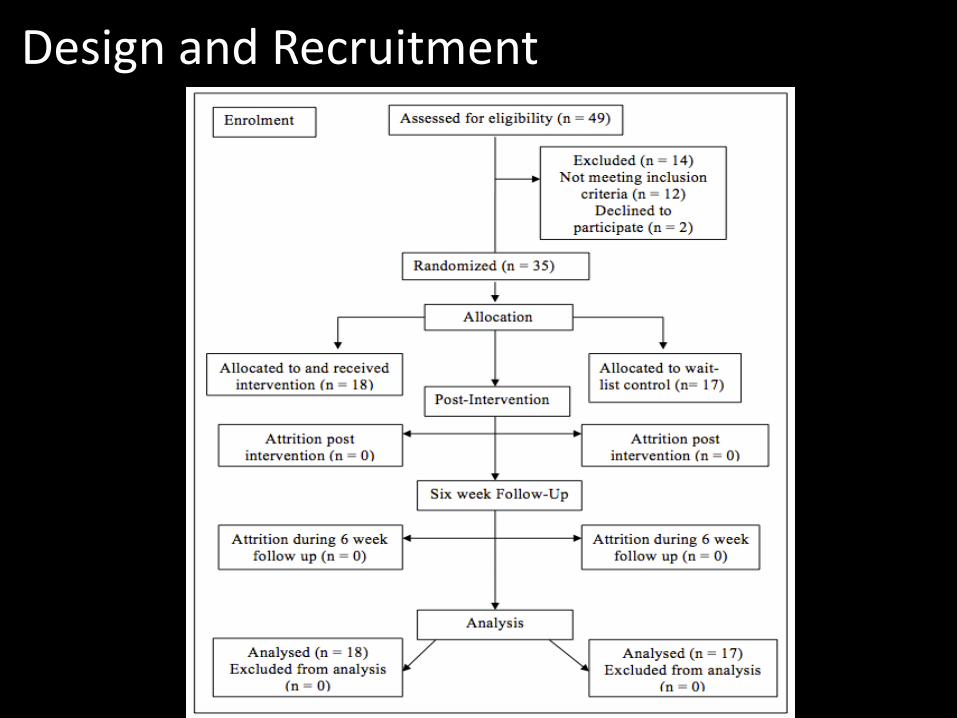
Design and Recruitment
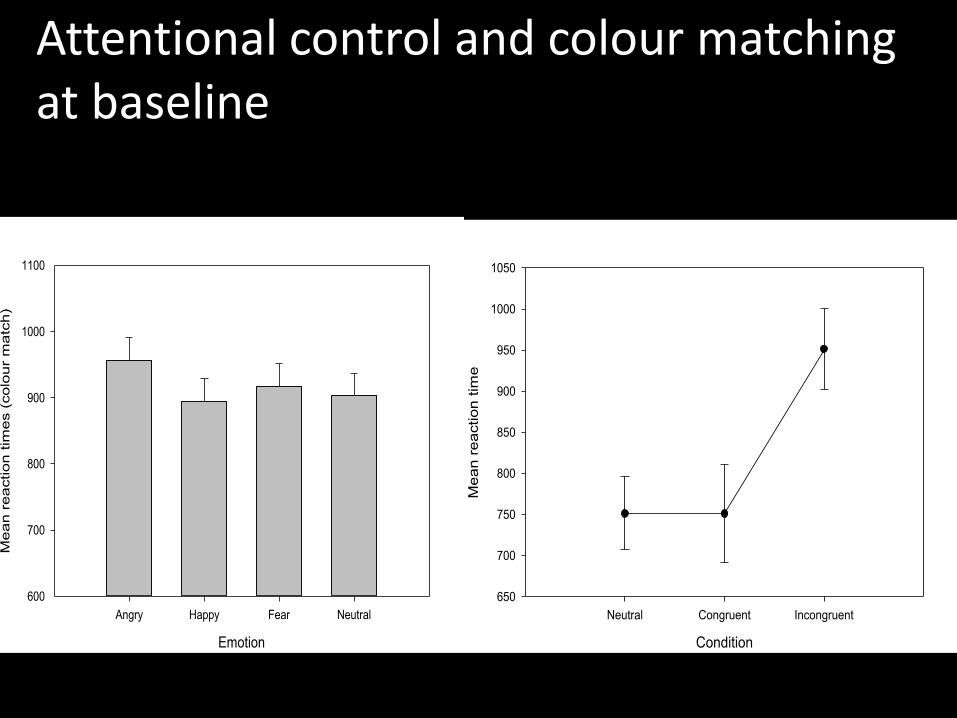
Attentional control and colour matching at baseline
Emotion
Angry Happy Fear Neutral
Me
an
re
actio
n t
ime
s (
co
lou
r m
atc
h)
600
700
800
900
1000
1100
Condition
Neutral Congruent Incongruent
Me
an
re
actio
n t
ime
650
700
750
800
850
900
950
1000
1050
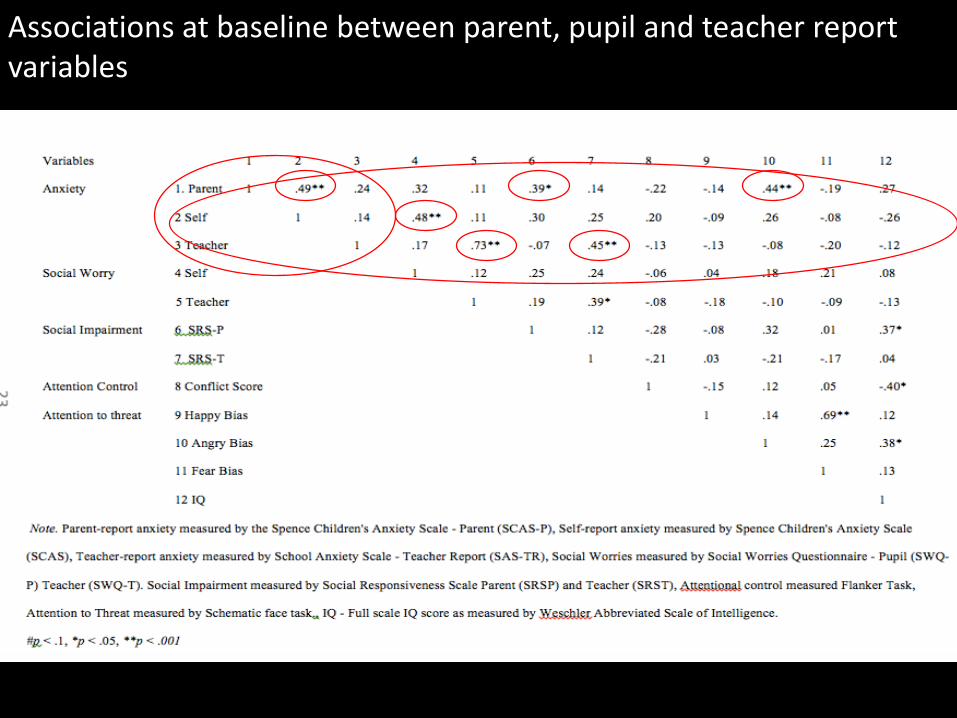
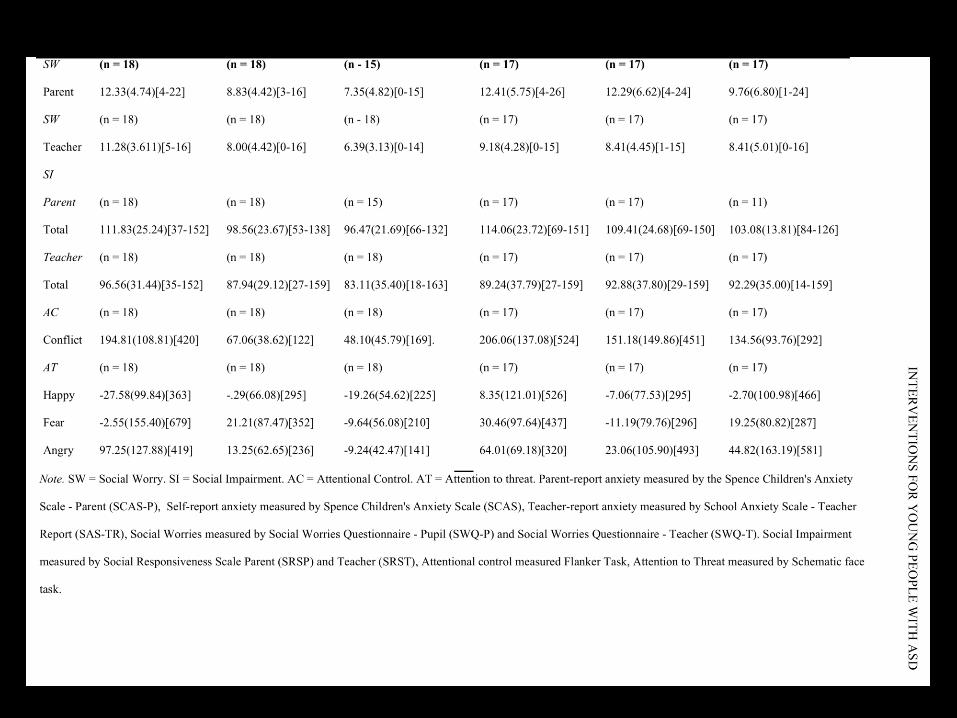
Associations at baseline between parent, pupil and teacher report variables
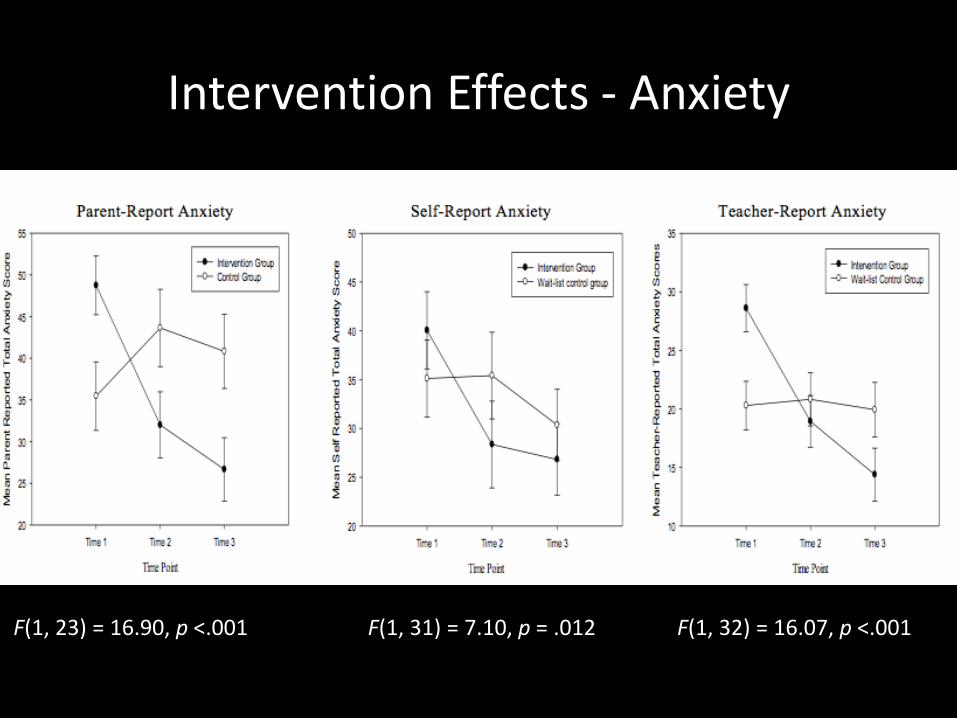
Intervention Effects - Anxiety
F(1, 23) = 16.90, p <.001 F(1, 31) = 7.10, p = .012 F(1, 32) = 16.07, p <.001
Results – Secondary Outcomes
• Social Worries/Social Impairment
– self, parent, teacher – no main effect of group
• Attention to threat/Inhibitory control
– Greater interference from angry faces across the sample but no effect of intervention
– No group X time interaction for flanker task
Implications CBT for Anxiety
• Preliminary evidence that a school-based CBT intervention can reduce anxiety symptoms in a community derived sample of adolescents with ASD with elevated levels of anxiety as reported by multiple-informants
• Skills taught were generalised to contexts outside of the intervention setting, with notable effects reported both at school and at home
• Group differences were maintained six weeks post-intervention, both at school and at home
Limitations
• Treatment integrity was not formally measured
• No active control group
• Raters were not blinded to condition allocation at post-intervention or follow-up
• Relatively short follow up
Ongoing Related Research• Understanding the physiological and environmental
correlates of anxiety in adolescents with ASD across the school day (Emma Lee)
• Mapping the Landscape of Fear – Understanding whether/which lessons, time points or geographical locations are anxiety provoking in young people with ASD (Ellie Hayes and Caitlin Murray)
• Understanding the cognitive and psychiatric profile of a clinic based group referred for ASD diagnosis in adulthood (Caitlin Murray & Vicki Russ)
• Social anxiety in girls with ASD (Leanne Pickering)
• Developing a co-constructed parent-delivered CBT intervention for anxious autistic children (with Cathy Cresswell/Fiona Knott @ Reading)
References
• Attwood, T. (2004). Exploring Feelings: Anxiety: Cognitive Behaviour Therapy to Manage Anxiety. Future Horizons.
• Bellini, S. (2004). Social skills deficits and anxiety in higher functioning adolescents with autism spectrum disorders. Focus on Autism and Other Developmental Disabilities, 19 (3), 78-86. doi: 10.1177/10883576040190020201.
• Sofronoff, K., Attwood, T., & Hinton, S. (2005). A randomised controlled trial of a CBT intervention for anxiety in children with Asperger syndrome. Journal of Child Psychology and Psychiatry, 46(11), 1152-1160. doi: 10.1111/j.1469-7610.2005.00411.x.
• Sukhodolsky, D. G., Scahill, L., Gadow, K. D., Arnold, L. E., Aman, M. G., McDougle, C. J., McCracken, J. T., Tierney, E., Williams White, S.,Lecavalier, L., & Vitiello, B. (2008). Parent-rated anxiety symptoms in children with pervasive developmental disorders: Frequency and association with core autism symptoms and cognitive functioning. Journal of Abnormal Child Psychology, 36, 117–128. doi: 10.1007/s10802-007-9165-9.
• Sze, K., & Wood, J. (2007). Cognitive behavioral treatment of comorbid anxiety disorders and social difficulties in children with high-functioning autism: A case report. Journal of Contemporary Psychotherapy, 37, 133–143. doi: 10.1007/s10879-007-9048-y.
• White, S. W., Oswald, D., Ollendick, T., & Scahill, L. (2009). Anxiety in children and adolescents with autism spectrum disorders. Clinical Psychology Review, 29, 216–229. doi: 10.1016/j.cpr.2009.01.003.