Embed Size (px)
Citation preview
Strictly Confidential
Suite 9 / 336 Churchill Avenue SUBIACO 6008 PO Box 502 SUBIACO WA 6904
Phone: (08) 9388 8044 www.pecs.net.au
Autism Spectrum Disorder Assessment Report:
John Smith
CONFIDENTIAL – NOT TO BE RELEASED WITHOUT PERMISSION OF THE
PARENT/GUARDIAN

2
CONTENTS
(1) Biographical Details (2) Referral Information (3) Brief Background Information (4) Parents’ Current Concerns (5) Autism Spectrum Disorder Diagnostic Criteria as per DSM-5 and Level of Support Required (6) Cognitive Assessment (7) Adaptive Behaviour Assessment (8) Comorbidity and Differential Diagnosis Screening Assessment (9) ADHD Behavioural Assessment (10) Summary (11) Conclusion and Statement of Diagnosis (12) Recommendations
This report adheres to the diagnostic criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders – Fifth Edition (DSM-5TM) for Autism Spectrum Disorder.
BIOGRAPHICAL DETAILS
Name: John Smith Date of Birth: 30/09/2006 Date of Assessment: 29/06/2015 Age at Assessment: 8 years 8 months Gender: Male School: Albany Primary School Grade: 3 Home Address: 24 Havelock Street, MIDDLETON WA 6330 Parent’s Name: Rebecca Smith Parent’s Phone Number: 0431 111 111 Parent’s Email: [email protected]
REFERRAL INFORMATION
John was referred to Psychological and Educational Consultancy Services (PECS) by Dr Greg White (General Practitioner) for a Comprehensive Psychological Assessment and indication of whether the results are reflective of an individual with Autism Spectrum Disorder (ASD).
PARENTS’ CURRENT CONCERNS
From a presented list, John identified concerns in the following areas: • Academic problems • Attention problems • Learning problems • Written language problems • Receptive language problems • Expressive language problems • Behaviour problems • Anxiety problems • Bullying issues • Memory problems • Suspected hyperactivity • Possible education support placement • Social skills problems
3
BRIEF BACKGROUND INFORMATION
Relevant information reported during the initial interview session with Rebecca Smith, John’ mother:
• John was born prematurely (4 weeks early) • John required assistance with breathing • John reached most major developmental milestones (e.g. crawling, standing alone, speaking)
within the normal time frame except for walking alone which was achieved early • Is solely right-handed/footed • Normal visual and auditory acuity reported • John has been previously diagnosed with an attention-deficit and hyperactivity disorder (2011) • He is currently taking medication for attention and hyperactivity problems (Ritalin – 30 mg and
Catapres – nightly as he experiences lack of sleep) • Ms Smith reported that she was diagnosed with ADHD as a teenager; she is not currently taking
medication for ADHD • Ms Smith also reported that John’ father suffered from depression • John younger sister (aged 7) is on a waiting list for speech therapy. • In regards to John’ behaviour, Ms Smith reported that John touches people inappropriately, puts
his head on people’s lap, has hit a teacher splitting her lip, and his social skills are around at a Kindy level
• Ms Smith has also noticed a lack of empathy/emotion from John and his anxiety levels have increased in the past 6 months
Current concerns from the school, according to the Learning Support Coordinator, include: o Lack of understanding of personal space (e.g. sits uncomfortably close to other students) o Often touches other students inappropriately (including squeezing an older boy’s genital
area during swimming lessons) o When agitated, John often grunts and screams, rocks back and forth, hides under or behind
furniture, and directs his aggression towards himself by banging his head against walls or scratching at his arms
o He is also destructive, often ripping work into tiny pieces, cutting up pencils and rulers with his scissors, throwing things across the floor and deliberately breaking toys and small objects. While these items usually belong to John he has recently started to throw objects belonging to others and has started directing his anger at others by throwing things at them, kicking and punching
o Difficulty in making friends; he is often isolated and he alternates between clinging possessively to a child who plays with him and being aggressive to that child
o John is extremely immature in his speech and behaviour and while he is capable of completing Year 3 level tasks, his rapid mood swings often result in unfinished or destroyed work
o When extremely angry or distressed, John will start removing clothing and making statements like “I’ll take my clothes off”, “I’ll show you this (gestures towards his genitals)”, and “Do you want to see this?”
o Currently, the school has a Behaviour Management Plan in place in order to find the triggers and corresponding appropriate strategies to prevent John losing control in and out of class
o Sensory breaks and making him aware of changes before they occur have also been helpful
4
Past assessments and/or interventions include: o Speech Therapy and Occupational Therapy o School Psychologist o Paediatrician
Past testing: • School Psychologist Observations in 2015: John was observed on three separate occasions. Some
behaviours of interest include: o Continuously moving his bottom around on his seat and swinging his legs while reading a
book o Difficulty with some speech sounds and difficulty paying attention to students asking him
questions during news telling o John was observed to sit very close to others on the mat and he covered his ears when the
class was too noisy or when they all joined in saying “good afternoon) o John was also observed to put his face close to his peers when they were talking to him o After the recess break, John had difficulty returning to class o Calling out to students at inappropriate times
• General Practitioner Mental Status Examination in June 2015: o Review of Mental Health Plan (24/06/2015) o Management: Psychological assessment and counselling, review by Paediatrician, review
by Child Psychiatrist, and follow up by child mental health nurses/counsellors o Main problems: ADHD, behavioural problems and possible Autistic Spectrum Disorder.
See checklists for more behavioural information.
5
AUTISM SPECTRUM DISORDER DIAGNOSTIC CRITERIA AS PER DSM-5 There are seven DSM-5™ criteria for Autism Spectrum Disorder, separated into two domains: Social Communication and Interaction (A) and Restricted, Repetitive Patterns of Behaviour (B). To meet the diagnostic criteria for Autism Spectrum Disorder, all three criteria from the Social Communication and Interaction domain (A) and at least two criteria from the Restricted, Repetitive Patterns of Behaviour domain (B) must be met. The difficulties must have been present in the early developmental period; cause clinically significant impairment in social, occupational, or other important area of functioning; and not be better explained by intellectual disability or global developmental delay. These criteria are addressed below for John, based on information gathered from direct observation, parent interview, and parent and teacher checklists.
DSM-5 CRITERIA
A. PERSISTENT DEFICITS IN SOCIAL COMMUNICATION AND SOCIAL INTERACTION ACROSS MULTIPLE CONTEXTS, AS MANIFESTED BY THE FOLLOWING, CURRENTLY OR BY HISTORY:
1. Deficits in social-emotional reciprocity.
Examples of behaviours relevant to this criterion displayed by John: • Often displays abnormalities in relation to social interaction • Sometimes does not notice others’ distress • Sometimes does not seem to understand simple questions, directions, or jokes • Tends not to spontaneously seek to share enjoyment, interests, or activities with other people • Reduced emotions to the extent of hurting others (sometimes intentionally; sometimes
unintentionally). • Unable to have back and forth conversation when upset • Will often interrupt social conversations (although has shown some improvement).
This criterion is rated as having been Met.
2. Deficits in nonverbal communicative behaviours used for social interaction.
Examples of behaviours relevant to this criterion displayed by John: • Often is observed to display abnormalities in relation to social interaction • Often displays abnormalities with regard to mood • Often invades others’ personal space • Put his face too close to his peers when they are talking to him • During the assessment was observed to invade the assessment administrator’s personal space by
tapping him on the top of the hand. • Will touch and sometimes hit when greeting people • Often touches people inappropriately e.g. puts his head on people’s lap and once squeezed an
older boy’s genital area during a swimming lesson. • When he is extremely angry or distressed, John will start removing clothing and make makes
statements such as “I’ll take my clothes off, I’ll show you this (points toward his genitals), do you want to see this?”
• During the assessment at PECS John left his seat, came and sat next to the examiner on the couch, and proceeded to put his hand on the examiner’s shoulder and asked if it was relaxing.
• Has difficulty maintaining eye contact, even when his parents or teachers are at his level. • When John is upset he displays gaze avoidance and there is no verbal communication at all.

6
This criterion is rated as having been Met.
3. Deficits in developing, maintaining, and understanding relationships.
Examples of behaviours relevant to this criterion displayed by John: • John’ mother believes that his social skills are at a kindy level • Often prefers to be involved in solitary activities • Does have an interest in peers but is unable to approach and interact appropriately with them. • Unable to attend events involving 10 or more people; he gets easily overwhelmed and will
lash out at peers/siblings/parents (e.g. John did not attend a recent family tea). • John’ mother reported a lack of empathy/emotion from John • Difficulty in making friends; he is often isolated and he alternates between clinging
possessively to a child who plays with him and being aggressive to that child • Prefers to be involved in solitary activity • Sometimes displays a lack of imaginative play
This criterion is rated as having been Met.
B. RESTRICTED, REPETITIVE PATTERNS OF BEHAVIOUR, INTERESTS, OR
ACTIVITIES, AS MANIFESTED BY AT LEAST TWO OF THE FOLLOWING, CURRENTLY OR BY HISTORY:
1. Stereotyped or repetitive motor movements, use of objects, or speech.
Examples of behaviours relevant to this criterion displayed by John: • Sometimes displays abnormalities in speech • When John gets agitated he often grunts, screams and rocks back and forth • Sometimes information tends to be repeated over and over regardless of appropriateness or
relevance • Tends to repeat phrases, jingles, or commercials • Sometimes displays a stereotyped, repetitive use of language, or repeats what people say • Sometimes uses language that can only be understood by his family or those close to him • Sometimes exhibits repetitive whole-body movements • Sometimes whirls around and around an object or on the floor • Sometimes lines the exact number of play things up in the same manner over and over • When agitated, John often grunts and screams, rocks back and forth, hides under or behind
furniture and directs his aggression towards himself by banging his head against walls or scratching at his arms.
• Demetrious will call out to his mother continually and as soon as she answers, John will say “I love you”. After 2 minutes he does it again. This is continuous throughout day and night.
• John will call out to his peers at inappropriate times. On one occasion, when the teacher aid left the classroom, John said “See you babe” and continued to repeat it several times.
• Displays an abnormal level of activity (hyperactive) • Experiences sleeping difficulties
This criterion is rated as having been Met.

7
2. Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behaviour.
Examples of behaviours relevant to this criterion displayed by John: • Often exhibits an inflexible adherence to specific non-functional routines or rituals • Has many abnormalities with regard to eating • Experiences extreme stress in regards to change in daily routines. He needs plenty of notice
(sometimes days in advance) if change is happening in the near future. • John will have meltdowns in regards to family gatherings or social events. Everything needs to
be completed and done at the same time and the same way every day. • Reported to have abnormalities with regard to clothing preferences
This criterion is rated as having been Met.
3. Highly restricted, fixated interests that are abnormal in intensity or focus.
Examples of behaviours relevant to this criterion displayed by John: • Is fixated towards the subject of birth/life/death. He will refer to “birth” as “living” and “seeing”
and “death” as “being nothing” and “blackness”. He will talk to anyone (including strangers) about death.
• Has a moderately inappropriate interest in, and use of toys or other objects • Has a tendency to dismantles objects
This criterion is rated as having been Partially Met.
4. Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment.
Examples of behaviours relevant to this criterion displayed by John:
• Very often exhibits odd responses to sensory stimuli • Is often fascinated with movement • Sometimes displays abnormalities in relation to fear • Parental and teacher report indicated that John’ reaction sensory inputs are extreme.
o Is unable to get haircuts without a big meltdown o Hates socks as sensory stimulus on his toes o Will rather use his hands to eat instead of using a fork and a knife – will have a melt-
down if made to use a fork • John has an adverse response to certain sounds, specially shouting – though he does not have
an ‘inside’ voice himself. • At school, sensory breaks have been found to help control his behaviour and also make him
more aware of changes before they occur • Often does not respond to his parents’ voice
This criterion is rated as having been Met.

8
C. SYMPTOMS MUST BE PRESENT IN THE EARLY DEVELOPMENTAL PERIOD (BUT
MAY NOT BECOME FULLY MANIFEST UNTIL SOCIAL DEMANDS EXCEED LIMITED CAPACITIES, OR MAY BE MASKED BY LEARNED STRATEGIES IN LATER LIFE):
Parental and teacher reports indicated that John’ mother and teachers had become concerned regarding John’ social skills since his early childhood (pre-primary years of schooling).
This criterion is rated as having been Met.
D. SYMPTOMS CAUSE CLINICALLY SIGNIFICANT IMPAIRMENT IN SOCIAL, OCCUPATIONAL, OR OTHER IMPORTANT AREAS OF CURRENT FUNCTION.
Parental and teacher reports and observations from the assessment setting indicated that John’ difficulties cause significant impairment in all areas of his current functioning (i.e., social, communication, occupational, etc).
This criterion is rated as having been Met.
E. THE DISTURBANCE IS NOT BETTER ACCOUNTED FOR BY INTELLECTUAL DISABILITY OR GLOBAL DEVELOPMENTAL DELAY.
John’ cognitive profile illustrates an average intelligent individual (VCI=13th percentile, PRI=55th percentile, WMI=27th percentile and PSI=27th percentile).
This criterion is rated as having been Met.
SUMMARY OF THE ASD DSM-5 CRITERIA AND LEVEL OF SUPPORT REQUIRED A. Social Communication and Interaction B. Restricted, Repetitive Patterns of Behaviour
1. Criterion Met 1. Criterion Met 2. Criterion Met 2. Criterion Met 3. Criterion Met 3. Criterion Partially Met
4. Criterion Met Total Met 3 Total Met 3.5 Severity Requiring substantial support Severity Requiring moderate support C. Present in Early Developmental Period D. Symptoms Cause Clinically Significant Impairment
1. Criterion Met 1. Criterion Met E. No Intellectual Disability/Global Delay F. Specifiers
1. Criterion Met 1. Without accompanying Intellectual Impairment 2. With accompanying Language Impairment As indicated in the summary table above, John meets sufficient DSM-5 criteria for a diagnosis of Autism Spectrum Disorder; requiring substantial support for deficits in social communication, and moderate support for restricted, repetitive behaviours.

9
COGNITIVE ASSESSMENT
Please note, a Cognitive Assessment is conducted due to Intellectual Disability/Global Developmental Delay needing to be ruled out before an Autism Spectrum Disorder diagnosis can be given. Psychometric Tests Administered:
Test Date of Administration Wechsler Intelligence Scale for Children-Fourth Edition (WISC-IV, 2003) 29/06/2015 WISC-IV Overview: The Wechsler Intelligence Scale for Children- Fourth Edition (WISC-IV) is an individually administered clinical instrument for assessing cognitive ability of children between the ages of 6 years through to 16 years 11 months. The test provides subtest and composite scores which represent intellectual functioning in specific cognitive domains as well as a composite score which represents general intellectual ability. The WISC-IV has Australian norms and Australian language adaptation, and it takes from 1 ½ to 2 hours to complete. WISC-IV Subtests:
Table 1: WISC-IV Subtest Descriptions
VERBAL COMPREHENSION Similarities The Similarities subtest involves the child being presented with two words that
represent common objects or concepts and describing how they are similar. It is designed to measure verbal reasoning and concept formation. It also involves auditory comprehension, memory, distinction between non-essential and essential features, and verbal expression.
Vocabulary The Vocabulary subtest comprises both picture and verbalised items. For picture items the child names pictures that are displayed in the Stimulus Book. For verbal items the child gives definitions for words that the examiner reads aloud. Vocabulary is designed to measure a child’s word knowledge and verbal concept formation. It also measures a child’s fund of knowledge, learning ability, long-term memory, and degree of language development. Other abilities that may be used by the child during this task include auditory perception and comprehension, verbal conceptualisation, abstract thinking, and verbal expression.
Comprehension The Comprehension subtest requires the child to answer questions based on their understanding of general principles and social situations. It measures verbal reasoning and conceptualisation, verbal comprehension and expression, the ability to evaluate and use past experience, and the ability to demonstrate practical information. It also involves knowledge of conventional standards of behaviour, social judgment and maturity, and common sense.
Information * The Information subtest involves the child answering verbally presented questions that address a broad range of general knowledge topics. It is designed to measure a child’s ability to acquire, retain, and retrieve general factual knowledge. It involves crystallised intelligence, long-term memory, and the ability to retain and retrieve information from school and the environment. Other skills that may be used by the child include auditory perception and comprehension, and verbal expressive ability.
Word Reasoning * Word Reasoning involves the child identifying the common concept being described by a series of clues. This task measures verbal comprehension, analogical and general reasoning ability, verbal abstraction, domain knowledge, the ability to integrate and synthesize different types of information, and the ability to generate alternative concepts.

10
PERCEPTUAL REASONING Block Design All items of the Block Design subtest require the child to view a constructed
model or a picture in the Stimulus Book, and use red-and-white blocks to re-create the design within a specified time limit. This subtest measures the child’s ability to analyses and synthesise abstract visual stimuli, It also involves nonverbal concept formation, visual perception and organisation, simultaneous processing, visual-motor coordination, learning, and the ability to separate figure and ground in visual stimuli. The subtest also involves visual observation and matching abilities for younger children, as well as the ability to integrate visual and motor processes.
Picture Concepts Picture Concepts involves the child being presented with two or three rows of pictures and them choosing one picture in each row to form a group with a common characteristic. This subtest measures abstract, categorical reasoning ability. Items are sequenced to reflect increasing demands on abstract reasoning ability.
Matrix Reasoning The child views an incomplete matrix and selects the missing portion from 5 response options on the Matrix Reasoning test. It measures fluid intelligence, visual information processing ability, and abstract reasoning skill.
Pictre Completion * Picture Completion requires the child to view a picture and point or name the important part that is missing from the picture, within a specified time limit. It measures visual perception and organisation, concentration, and visual recognition of essential details of objects.
WORKING MEMORY Digit Span The Digit Span subtest is composed of two parts: Digit Span Forward and Digit
Span Backward. Digit Span Forward requires John to repeat numbers in the same order as read aloud by the examiner, and the Digit Span Backward requires the child to repeat the numbers in the reverse order of that presented by the examiner. This subtest measures auditory short-term memory, sequencing skills, attention and concentration. The Digit Span Forward task involves rote learning and memory, attention, encoding, and auditory processing. Digit Span Backward involves working memory, transformation of information, mental manipulation, and visuospatial imaging. The shift from Digit Span Forward to Digit Span Backward requires cognitive flexibility and alertness.
Letter-Number Sequencing Letter-Number sequencing requires the child to read a sequence of numbers and letters and recall the numbers in ascending order and the letters in alphabetical order. The task requires sequencing, mental manipulation, attention, short-term auditory memory, visuospatial imaging, and processing speed.
Arithmetic * The child mentally solves a series of orally presented Arithmetic problems within a specified time limit on the Arithmetic subtest. It involves mental manipulation, concentration, attention, short-term and long-term memory, numerical reasoning ability, and mental alertness. It also involves sequencing, fluid reasoning, and logical reasoning.
PROCESSING SPEED Coding The Coding subtest involved John copying symbols that are paired with simple
geometric shapes or numbers. Using a key, John drew each symbol in its corresponding shape or box within a specified time limit. In addition to processing speed, the subtest measures short-term memory, visual and sequential processing, learning ability, cognitive flexibility, attention, and motivation.
Symbol Search John was required to scan a search group and indicate whether the target symbol(s) matches any of the symbols in the search group within a specified time limit on the Symbol Search subtest. In addition to processing speed, the Symbol Search subtest also involves short-term visual memory, visual-motor coordination, cognitive flexibility, visual discrimination, and concentration. It also taps auditory comprehension, perceptual organisation, and planning and learning ability.
*Cancellation * On the Cancellation subtest, John was required to scan both a random and structured arrangement of pictures and mark target pictures within a specified time limit. This subtest measures processing speed, visual selective attention, vigilance, and visual neglect.
* denotes supplementary subtest which may not be administered unless deemed necessary
11
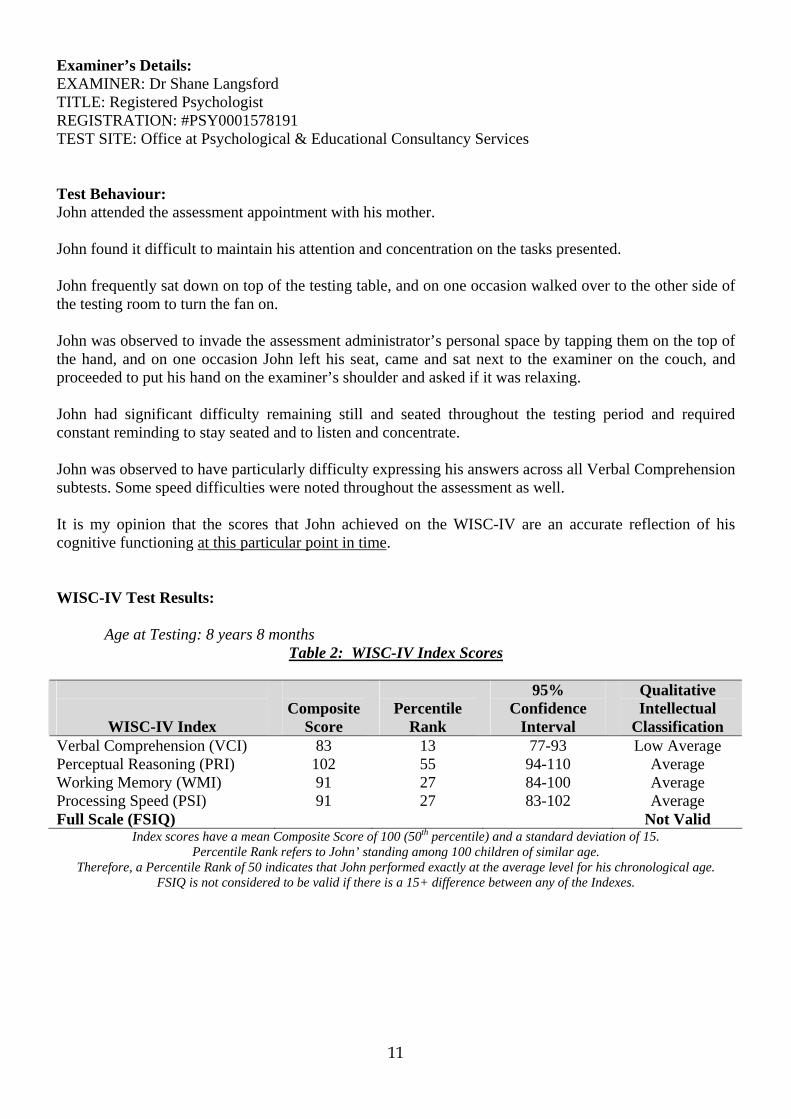
Examiner’s Details: EXAMINER: Dr Shane Langsford TITLE: Registered Psychologist REGISTRATION: #PSY0001578191 TEST SITE: Office at Psychological & Educational Consultancy Services Test Behaviour: John attended the assessment appointment with his mother. John found it difficult to maintain his attention and concentration on the tasks presented. John frequently sat down on top of the testing table, and on one occasion walked over to the other side of the testing room to turn the fan on. John was observed to invade the assessment administrator’s personal space by tapping them on the top of the hand, and on one occasion John left his seat, came and sat next to the examiner on the couch, and proceeded to put his hand on the examiner’s shoulder and asked if it was relaxing. John had significant difficulty remaining still and seated throughout the testing period and required constant reminding to stay seated and to listen and concentrate. John was observed to have particularly difficulty expressing his answers across all Verbal Comprehension subtests. Some speed difficulties were noted throughout the assessment as well. It is my opinion that the scores that John achieved on the WISC-IV are an accurate reflection of his cognitive functioning at this particular point in time. WISC-IV Test Results:
Age at Testing: 8 years 8 months
Table 2: WISC-IV Index Scores
WISC-IV Index
Composite
Score
Percentile
Rank
95% Confidence
Interval
Qualitative Intellectual
Classification Verbal Comprehension (VCI) 83 13 77-93 Low Average Perceptual Reasoning (PRI) 102 55 94-110 Average Working Memory (WMI) 91 27 84-100 Average Processing Speed (PSI) 91 27 83-102 Average Full Scale (FSIQ) Not Valid
Index scores have a mean Composite Score of 100 (50th percentile) and a standard deviation of 15. Percentile Rank refers to John’ standing among 100 children of similar age.
Therefore, a Percentile Rank of 50 indicates that John performed exactly at the average level for his chronological age. FSIQ is not considered to be valid if there is a 15+ difference between any of the Indexes.
12
The Verbal Comprehension Index (VCI) incorporates the 3 subtests of Similarities, Vocabulary, and Comprehension and is designed to measure verbal abilities utilising reasoning, comprehension, and concept formation. The Perceptual Reasoning Index (PRI) comprises the 3 subtests of Block Design, Picture Concepts, and Matrix Reasoning and is designed to measure perceptual reasoning and perceptual organisation. The Working Memory Index (WMI) measures John’ ability to sustain attention, concentrate, and exert mental control. Mental control is the ability to attend to and hold information in conscious awareness whilst performing some operation or manipulation with it, and producing the correct result. Good mental control may facilitate the processing of complex information and ease the learning of new material. The Processing Speed Index (PSI) is an indication of the rapidity with which John can perform mental and graphomotor processing without making errors. Good speed of information processing may free cognitive resources for the processing of more complex information and ease new learning. The Full Scale (FSIQ) refers to John’ performance across all 10 of the core subtests of the WISC-IV and is generally considered the best estimate of general cognitive ability unless there is marked variability among the Index Composite Scores (ie 15+ difference between the Indexes).
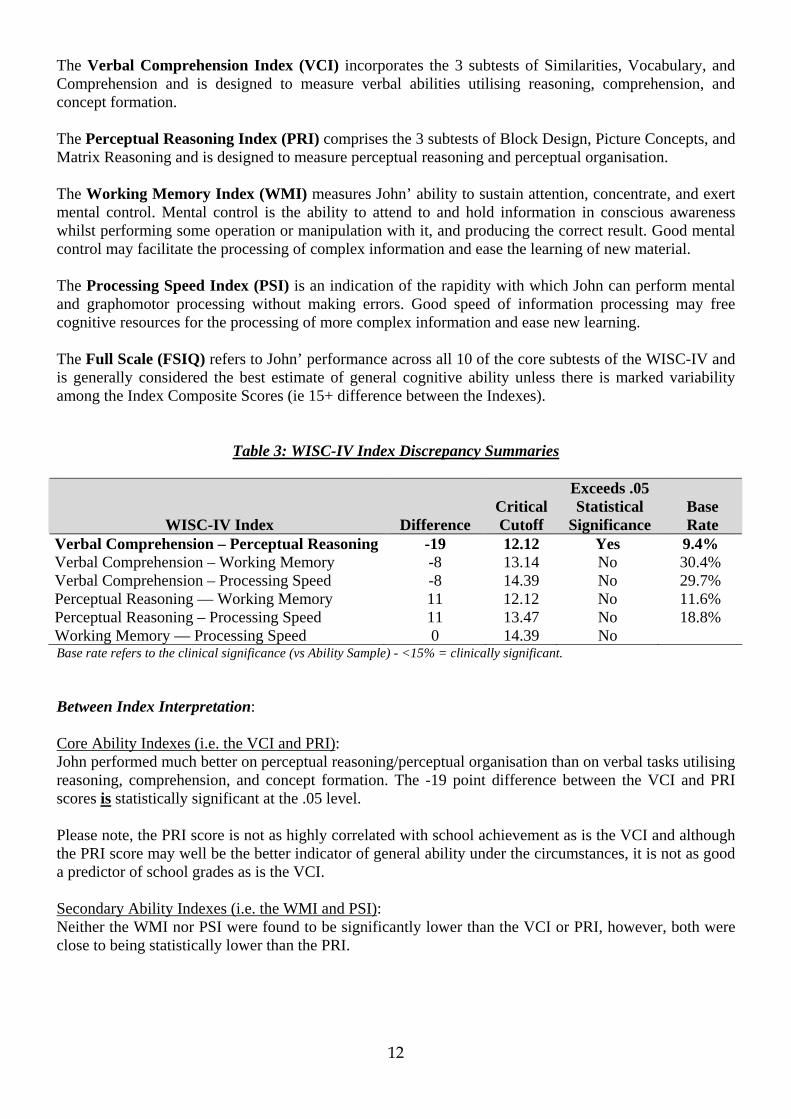
Table 3: WISC-IV Index Discrepancy Summaries
WISC-IV Index
Difference
Critical Cutoff
Exceeds .05 Statistical
Significance
Base Rate
Verbal Comprehension – Perceptual Reasoning -19 12.12 Yes 9.4% Verbal Comprehension – Working Memory -8 13.14 No 30.4% Verbal Comprehension – Processing Speed -8 14.39 No 29.7% Perceptual Reasoning — Working Memory 11 12.12 No 11.6% Perceptual Reasoning – Processing Speed 11 13.47 No 18.8% Working Memory — Processing Speed 0 14.39 No Base rate refers to the clinical significance (vs Ability Sample) - <15% = clinically significant. Between Index Interpretation: Core Ability Indexes (i.e. the VCI and PRI): John performed much better on perceptual reasoning/perceptual organisation than on verbal tasks utilising reasoning, comprehension, and concept formation. The -19 point difference between the VCI and PRI scores is statistically significant at the .05 level. Please note, the PRI score is not as highly correlated with school achievement as is the VCI and although the PRI score may well be the better indicator of general ability under the circumstances, it is not as good a predictor of school grades as is the VCI. Secondary Ability Indexes (i.e. the WMI and PSI): Neither the WMI nor PSI were found to be significantly lower than the VCI or PRI, however, both were close to being statistically lower than the PRI.

13
Below is a set of characteristic difficulties relevant to lower ability in each Index. These are generic difficulties and are not provided as an illustration of John’ individual difficulties. Verbal Comprehension weaknesses can cause difficulty learning in the classroom and performing to ability in exams by:
• Trouble understanding verbal directions and/or instructions. This will be more so with complex language, or when multiple steps are included in an instruction.
• Increased difficulty completing exams that require a large written output (i.e. essays, long answer questions).
• Being seen as ‘poor listeners’. These children can appear to be easily distracted and inattentive at times, especially when faced with high verbal task demands.
• Difficulty with ‘word based maths problems’ –generally these children will have adequate maths abilities but the child will find it difficult to demonstrate this when the maths questions is buried in text.
• Being stronger at maths, and science, where they can ‘show’ what they know in ways that are not heavily language based.
• Improved learning from charts, visual materials, diagrams, videos, or hands-on learning demonstrations.
• Difficulty in terms of reading comprehension – they may need to re-read a given text in order to fully understand the meaning.
• Difficulty in understanding abstract concepts, particularly when asked to perform tasks that rely heavily on verbal abstract reasoning.
• Difficulty in understanding social conventions (i.e. what should you do if you find a wallet in a store).
Table 4: WISC-IV Within-Index Discrepancies
Discrepancy Comparisons
Difference
Critical Cutoff
Exceeds .05 Statistical
Significance
Base Rate
Digit Span — Letter-Number Sequencing -1 3.20 No 46.1% Coding — Symbol Search 1 3.90 No 42% Similarities — Picture Concepts -2 3.61 No 34.1% Base rate refers to the clinical significance (vs Ability Sample) - <15% = clinically significant. Within Index/Within-Factor Interpretation: John’ within-Index and within-Factor score pattern illustrated no statistically significant discrepancies, therefore, the Indexes of Working Memory and Processing Speed, and the Abstract Categorical Reasoning and Concept Formation Factor, can all be considered stable.

14
Table 5: WISC-IV Subtest Scaled Scores
Subtests
Scaled Score
Test Age
Equivalent
Percentile
Rank Verbal Comprehension Index Similarities 7 6:10 16 Vocabulary 8 7:2 25 Comprehension 6 6:6 9 Perceptual Reasoning Index Block Design 11 9:6 63 Picture Concepts 9 8:2 37 Matrix Reasoning 11 9:6 63 *Picture Completion 7 6:10 16 Working Memory Index Digit Span 8 6:10 25 Letter-Number Sequencing 9 7:10 37 Processing Speed Index Coding 9 8:2 37 Symbol Search 8 8:2 25 See Appendix 1 for complete subtest descriptions. *Non-core subtest.
Figure 1: WISC-IV Subtest Scaled Scores
Vertical bar represents the Standard Error of Measurement.
15
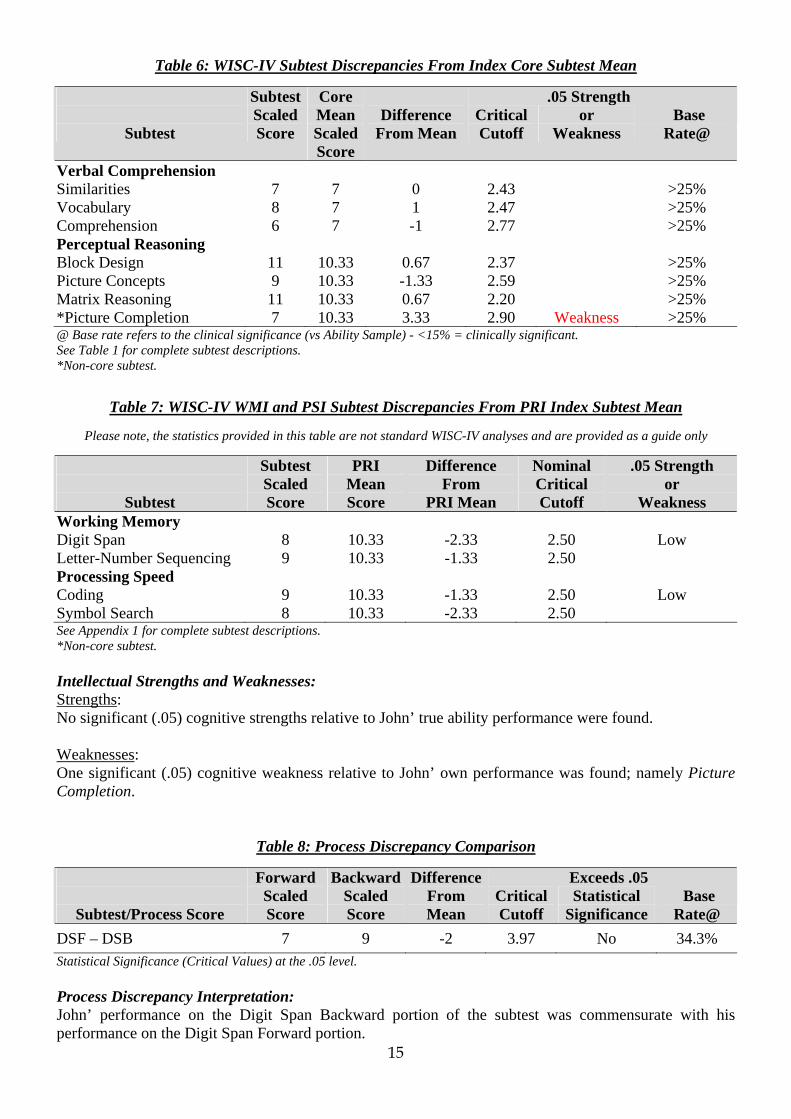
Table 6: WISC-IV Subtest Discrepancies From Index Core Subtest Mean
Subtest
Subtest Scaled Score
Core Mean ScaledScore
Difference
From Mean
Critical Cutoff
.05 Strength or
Weakness
Base
Rate@
Verbal Comprehension Similarities 7 7 0 2.43 >25% Vocabulary 8 7 1 2.47 >25% Comprehension 6 7 -1 2.77 >25% Perceptual Reasoning Block Design 11 10.33 0.67 2.37 >25% Picture Concepts 9 10.33 -1.33 2.59 >25% Matrix Reasoning 11 10.33 0.67 2.20 >25% *Picture Completion 7 10.33 3.33 2.90 Weakness >25% @ Base rate refers to the clinical significance (vs Ability Sample) - <15% = clinically significant. See Table 1 for complete subtest descriptions. *Non-core subtest.
Table 7: WISC-IV WMI and PSI Subtest Discrepancies From PRI Index Subtest Mean
Please note, the statistics provided in this table are not standard WISC-IV analyses and are provided as a guide only
Subtest
Subtest Scaled Score
PRI Mean Score
Difference From
PRI Mean
Nominal Critical Cutoff
.05 Strength or
Weakness Working Memory Digit Span 8 10.33 -2.33 2.50 Low Letter-Number Sequencing 9 10.33 -1.33 2.50 Processing Speed Coding 9 10.33 -1.33 2.50 Low Symbol Search 8 10.33 -2.33 2.50 See Appendix 1 for complete subtest descriptions. *Non-core subtest. Intellectual Strengths and Weaknesses: Strengths: No significant (.05) cognitive strengths relative to John’ true ability performance were found. Weaknesses: One significant (.05) cognitive weakness relative to John’ own performance was found; namely Picture Completion.
Table 8: Process Discrepancy Comparison
Subtest/Process Score
Forward Scaled Score
BackwardScaled Score
Difference From Mean
Critical Cutoff
Exceeds .05 Statistical
Significance
Base
Rate@ DSF – DSB 7 9 -2 3.97 No 34.3% Statistical Significance (Critical Values) at the .05 level. Process Discrepancy Interpretation: John’ performance on the Digit Span Backward portion of the subtest was commensurate with his performance on the Digit Span Forward portion.
16
ADAPTIVE BEHAVIOUR ASSESSMENT
Adaptive Behaviour Tests Administered:
Test Date of Administration
Adaptive Behaviour Assessment System–Second Edition (ABAS-II, 2008) 29/06/2015 The Adaptive Behaviour Assessment System – Second Edition provides a comprehensive, norm-referenced assessment of adaptive skills for individuals ages birth to 89 years. The ABAS-II may be used to assess an individual’s adaptive skills for diagnosis and classification of disabilities and disorders, identification of strengths and limitations, and to document and monitor an individual’s progress over time. The comprehensive range of specific adaptive skills and broad adaptive domains measured by the ABAS-II correspond to the specifications identified by the American Association of Mental Retardation (AAMR; 1992, 2002b) and the Diagnostic and Statistical Manual of Mental Disorders – Fourth Edition Text Revision (DSM-IV-TR; American Psychiatric Association, 2000). The ABAS-II consists of 5 rating forms, which can be completed independently by a respondent or may be read aloud to a respondent who has limited reading skills. Each rating form is easy to complete and score, requiring approximately 20 minutes to complete and 5-10 minutes to hand score. Respondents read and respond to all items and rate the extent to which the individual performs the adaptive skills when needed. The rating scale for the items allows respondents to indicate if the individual is able to independently perform an activity and, if so, how frequent he or she performs the activity when it is needed; 0 (Is not able), 1 (Never or Almost Never When Needed), 2 (Sometimes When Needed), or 3 (Always or Almost Always When Needed). Although it is possible to assess the adaptive skills of an individual with a single rating form, the use of multiple rating forms is recommended to provide a comprehensive assessment across a variety of settings. Significant limitations in adaptive behaviour are defined as performance at least 2 Standard Deviations below the mean on (a) the Conceptual, Social or Practical Domain, or (b) an overall score on a standardised measure that assesses these three adaptive domains (e.g. GAC).

17
Skill Areas for Teacher and Parent Forms
Communication Speech, language, and listening skills needed for communication with other people, including vocabulary, responding to questions, conversation skills, nonverbal communication skills etc
Community Use Skills needed for functioning and appropriate behaviour in the community, including getting around in the community, expression of interest in activities outside the home, recognition of different facilities, etc
Functional Academics Basic pre-academics skills that form the foundations for reading, writing, mathematics and other skills needed for daily, independent functioning, including letter recognition, counting, drawing simple shapes etc
School/Home Living Skills needed for basic care of a home or living setting or a school or classroom setting, including cleaning, straightening, helping adults with household tasks, taking care of personal possessions etc
Health and Safety Skills needed for protection of health and to respond to illness and injury, including following safety rules, using medicines, showing caution, keeping out of physical danger etc
Leisure Skills needed for engaging in and planning leisure and recreational activities, including playing with others, playing with toys, engaging in recreation at home, following rules in games etc
Self-Care Skills needed for personal care including eating, dressing, bathing, toileting, grooming, hygiene etc
Self-Direction Skills needed for independence, responsibility and self-control, including making choices about food and clothing, starting and completing tasks, following a daily routine, following directions etc
Social Skills needed to interact socially and get along with other people, including expressing affection, having friends, showing and recognising emotions, assisting others, using manners etc
Motor Basic fine and gross motor skills needed for locomotion, manipulation of the environment and the development of more complex activities such as sports, including sitting, pulling up to a standing position, walking, fine motor control, kicking etc
Composite Score Scales
The Conceptual Domain Composite score is derived from the sum of scaled scores from the Communication, Functional Academics and Self-Direction Skill Areas. Conceptual skills include receptive and expressive language, reading and writing, money concepts and self-direction. The Social Domain Composite score is derived from the sum of scaled scores from the Social and Leisure Skill Areas. Social skills include interpersonal relationships, responsibility, self-esteem, gullibility, naiveté, following rules, obeying laws and avoiding victimisation. The Practical Domain Composite score is derived from the sum of scaled scores from the Self-Care, Home/School Living, Community Use, Health and Safety and Work Skill Areas. Practical skills include basic maintenance activities of daily living (e.g., eating, mobility, toileting, dressing), instrumental activities of daily living (e.g., meal preparation, housekeeping, transportation, taking medications, money management, telephone use) together with occupational skills and maintenance of safe environments. The General Ability Composite (GAC) score is derived from the sum of scaled scores from seven, nine or ten skill areas, depending on the age of the individual and the type of rating form. The GAC represents a comprehensive and global estimate of an individual’s adaptive functioning. The GAC describes the degree to which an individual’s adaptive skills generally compare to the adaptive skills of other individual’s within the same age group.

18
Adaptive Behaviour Test Results: (1) Parent Form (Ages 5-21) The Parent Form is a comprehensive, diagnostic measure of the adaptive skills that have primary relevance for the functioning of children, adolescents and young adults in the home and other settings. The Parent Form is used for individuals aged 5-21 years, and includes 241 items, with 22 to 27 items per skill area.
Age at Testing: 8 years 8 months
Table 1: Sum of Scaled Scores to Composite Score Conversions
Composite
Sum of Scaled Scores
Composite
Score
Percentile
Rank
95% Confidence
Interval
Qualitative
Range Conceptual Not calculated Social 2 55 0.1 48-62 Extremely Low Practical Not calculated GAC Not calculated
Adaptive Domain scores have a mean of 100 (50th percentile) and a standard deviation of 15. Percentile Rank refers to John’ standing among 100 individuals of a similar age.
Parent scores for the Conceptual Domain, Practical Domain and General Ability Composite could not be calculated due to an insufficient number of responses.
Figure 1: ABAS-II Skill Area Scaled Score Profile

19
Table 2: Raw Score to Scaled Score Conversions
Skill Areas
Scaled Scores
Qualitative Range
Communication (Com) Community Use (CU) Functional Academics (FA) Home Living (HL) 3 Extremely Low Health and Safety (HS) 3 Extremely Low
Leisure (LS) 1 Extremely Low
Self-Care (SC) 2 Extremely Low
Self-Direction (SD) 1 Extremely Low
Social (Soc) 1 Extremely Low
Motor (MO) Scaled scores have a mean of 10 (50th percentile) and a standard deviation of 3. Percentile Rank refers to John’ standing among 100 individuals of a similar age.
Parent scores on the Conceptual Domain, Practical Domain and General Ability Composite could not be calculated due to an insufficient number of responses.
Table 3: ABAS Strengths and Weaknesses
Skill Areas
Skill Area
Scaled Score
Mean Scaled Score
Differencefrom Mean
CriticalValue
Strength or
Weakness
Base RateConceptual Communication Functional Pre-Academics Self-Direction 1 Social Leisure 1 Social 1 Practical Community Use Home Living 3 Health and Safety 3 Self-Care 2 Statistical Significance (Critical Values) at the .05 level Skill Area Strengths and Weaknesses: Statistical analysis of the results revealed the following skill areas to be significant (.05) adaptive behaviour strengths or weaknesses relative to John’ own performance. Strengths: One significant (.05) adaptive behaviour strength relative to John’ own performance was found; namely Functional Pre-Academics. Weaknesses: No significant (.05) adaptive behaviour weaknesses relative to John’ own performance were found.

20
(2) Teacher Form (Ages 5-21) The Teacher Form is a comprehensive, diagnostic measure of the adaptive skills that have primary relevance for children, adolescents and young adults in the school setting or any other educational setting. Teachers and teacher’s aides can complete this form. The Teacher Form is used for individuals aged 5-21 years and includes 216 items, with 21 to 27 items per skill area.
Age at Testing: 8 years 8 months
Table 1: Sum of Scaled Scores to Composite Score Conversions
Composite
Sum of Scaled Scores
Composite
Score
Percentile
Rank
95% Confidence
Interval
Qualitative
Range Conceptual 8 63 1 59-67 Extremely Low Social 3 58 0.3 53-63 Extremely Low Practical 19 70 2 66-74 Extremely Low GAC 30 61 0.5 58-64 Extremely Low
Adaptive Domain scores have a mean of 100 (50th percentile) and a standard deviation of 15. Percentile Rank refers to Demetrious’ standing among 100 individuals of a similar age.
GAC is not considered to be valid if considerable scatter exists among the skill area scaled scores.
Table 2: ABAS-II Discrepancy Summaries
Domain Composite
Difference
Critical Cutoff
Exceeds .05 Statistical
Significance
Base Rate Conceptual - Social 5 6.58 No 27.0% Conceptual - Practical -7 5.88 Yes 26.9% Social - Practical -12 6.58 Yes 13.3%
Statistical Significance (Critical Values) at the .05 level Base rate refers to the clinical significance (vs Ability Sample) - <15% = clinically significant
Figure 1: ABAS-II Skill Area Scaled Score Profile

21
Table 3: Raw Score to Scaled Score Conversions
Skill Areas
Scaled Scores
Qualitative Range
Communication (Com) 2 Extremely Low Community Use (CU) 7 Below Average
Functional Academics (FA) 5 Borderline
School Living (SL) 1 Extremely Low
Health and Safety (HS) 3 Extremely Low
Leisure (LS) 2 Extremely Low
Self-Care (SC) 8 Average
Self-Direction (SD) 1 Extremely Low
Social (Soc) 1 Extremely Low Scaled scores have a mean of 10 (50th percentile) and a standard deviation of 3. Percentile Rank refers to John’ standing among 100 individuals of a similar age.
Table 4: ABAS Strengths and Weaknesses
Skill Areas
Skill Area
Scaled Score
Mean Scaled Score
Differencefrom Mean
CriticalValue
Strength or
Weakness
Base RateConceptual Communication 2 3.33 -1.33 1.92 >25% Functional Academics 5 3.33 1.67 1.67 Strength >25% Self-Direction 1 3.33 -2.33 1.65 Weakness 10-25% Social Leisure 2 3.33 -1.33 1.98 >25% Social 1 3.33 -2.33 1.73 Weakness 10-25% Practical Community Use 7 3.33 3.67 2.61 Strength 5-10% School Living 1 3.33 -2.33 1.92 Weakness 10-25% Health and Safety 3 3.33 -0.33 2.01 >25% Self-Care 8 3.33 4.67 2.12 Strength 5-10% Statistical Significance (Critical Values) at the .05 level Skill Area Strengths and Weaknesses: Statistical analysis of the results revealed the following skill areas to be significant (.05) adaptive behaviour strengths or weaknesses relative to John’ own performance. Strengths: Three significant (.05) adaptive behaviour strengths relative to John’ own performance were found; namely the Functional Academics, Community Use, and Self-Care Skills Areas. Weaknesses: Three significant (.05) adaptive behaviour weaknesses relative to John’ own performance were found; namely the Self-Direction, Social, and School Living Skills Areas.

22
Adaptive Behaviour Summary: John’ parent-report score for the Social Domain was found to be at the 0.1st percentile (Extremely Low). Parent scores for the Conceptual Domain, Practical Domain and General Ability Composite could not be calculated due to insufficient responses. John’ teacher-report scores for the Conceptual Domain, Social Domain, and Practical Domain all fell in the Extremely Low category, culminating in a General Ability Composite at the 0.5th percentile (Extremely Low).

23
COMORBIDITY ANDDIFFERENTIAL DIAGNOSIS SCREENING ASSESSMENT
Screening Tests Administered:
Test Date of Administration *child & adolescent psychprofiler (CAPP; Langsford, Houghton, & Douglas 2014) 29/06/2015 CAPP Outline: The CAPP comprises 126 items and utilises three separate screening forms; the Self-report Form (SRF: 126 items), Parent-report Form (PRF: 126 items), and Teacher-report Form (TRF: 126 items) for the simultaneous screening of 14 of the most prevalent disorders in children and adolescents. The CAPP comprises screening criteria that closely resemble the diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (DSM-5: American Psychiatric Association: APA, 2013). The CAPP is appropriate for the screening of behaviour of children and adolescents between the ages of 2 and 17 years, however, only the Parent-report and Teacher-report Forms are administered for children aged below 10 years due to the reading level requirements of the Self-report Form. All items of the CAPP require responses to be made on a six-point scale pertaining to the perceived frequency of the behaviour (ie., Never, Rarely, Sometimes, Regularly, Often, or Very Often). When calculating disorder screening scores, the items are coded as follows: Never = 0, Rarely = 0, Sometimes = 0, Regularly = 1, Often = 1, and Very Often = 1. These values were chosen because although many people with and without disorders may exhibit similar behaviours, it is the frequency of the behaviour that determines whether it is of clinical significance. A small number of exceptions to these scoring rules apply where some of the behaviours (e.g., fighting with a weapon, stealing) are considered to be of sufficient severity that 'Sometimes' is also awarded a score of 1. Therefore, the summation of the items within each disorder produces a screening score for that disorder, which if exceeding the screening cutoff score, designates that the individual has been awarded a positive screen for that disorder. In order to ensure its validity and reliability, the first version of the psychprofiler was subjected to a series of rigorous psychometric analyses over a number of years. This process has involved validation against a large mainstream sample (n>1000) as well as clinical calibration against individuals with formal diagnoses. These analyses found the psychprofiler to be a highly reliable and valid screening instrument. The CAPP is primarily administered in order to provide an objective indication of whether the individual exhibits behaviours characteristic of a suspected disorder, possible comorbid disorders, and issues pertaining to differential diagnosis. The psychprofiler has been the most widely used Australian psychiatric / psychological / educational global screening instrument since 2004. For further information regarding the CAPP, please visit www.psychprofiler.com or contact Dr Shane Langsford on (08) 9388 8044. Please note that any indication of a positive screen on the CAPP does not constitute a formal diagnosis. A positive screen merely indicates that the individual has met sufficient criteria for a disorder to warrant further investigation.
24
Global Behavioural Assessment Results: John’ mother reported positive screens for:
• Generalised Anxiety Disorder • Separation Anxiety Disorder • Attention-Deficit/Hyperactivity Disorder: Combined Presentation • Language Disorder • Persistent Depressive Disorder • Conduct Disorder • Specific Learning Disorder – with Impairment in Written Expression
John’ teacher reported positive screens for:
• Generalised Anxiety Disorder • Attention-Deficit/Hyperactivity Disorder: Combined Presentation • Autism Spectrum Disorder • Language Disorder • Persistent Depressive Disorder • Conduct Disorder • Posttraumatic Stress Disorder
A copy of the CAPP Report is included as an Appendix, as are the completed CAPP Forms. Please refer to the CAPP Report for the individual behaviours which were responsible for the positive screens elicited.
25
ADHD BEHAVIOURAL ASSESSMENT
Checklists Administered:
Date of Checklists Administration
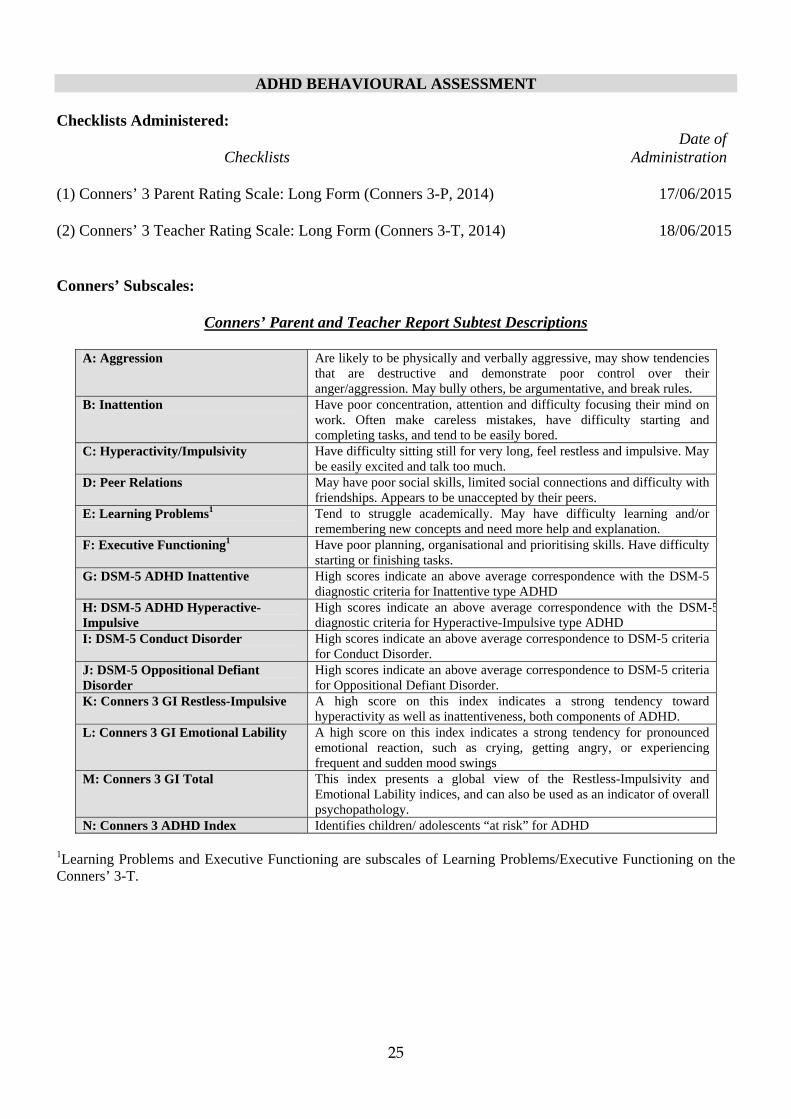
(1) Conners’ 3 Parent Rating Scale: Long Form (Conners 3-P, 2014) 17/06/2015 (2) Conners’ 3 Teacher Rating Scale: Long Form (Conners 3-T, 2014) 18/06/2015 Conners’ Subscales:
Conners’ Parent and Teacher Report Subtest Descriptions
A: Aggression Are likely to be physically and verbally aggressive, may show tendencies
that are destructive and demonstrate poor control over their anger/aggression. May bully others, be argumentative, and break rules.
B: Inattention Have poor concentration, attention and difficulty focusing their mind on work. Often make careless mistakes, have difficulty starting and completing tasks, and tend to be easily bored.
C: Hyperactivity/Impulsivity Have difficulty sitting still for very long, feel restless and impulsive. May be easily excited and talk too much.
D: Peer Relations May have poor social skills, limited social connections and difficulty with friendships. Appears to be unaccepted by their peers.
E: Learning Problems1 Tend to struggle academically. May have difficulty learning and/or remembering new concepts and need more help and explanation.
F: Executive Functioning1 Have poor planning, organisational and prioritising skills. Have difficulty starting or finishing tasks.
G: DSM-5 ADHD Inattentive High scores indicate an above average correspondence with the DSM-5 diagnostic criteria for Inattentive type ADHD
H: DSM-5 ADHD Hyperactive-Impulsive
High scores indicate an above average correspondence with the DSM-5diagnostic criteria for Hyperactive-Impulsive type ADHD
I: DSM-5 Conduct Disorder High scores indicate an above average correspondence to DSM-5 criteria for Conduct Disorder.
J: DSM-5 Oppositional Defiant Disorder
High scores indicate an above average correspondence to DSM-5 criteria for Oppositional Defiant Disorder.
K: Conners 3 GI Restless-Impulsive A high score on this index indicates a strong tendency toward hyperactivity as well as inattentiveness, both components of ADHD.
L: Conners 3 GI Emotional Lability A high score on this index indicates a strong tendency for pronounced emotional reaction, such as crying, getting angry, or experiencing frequent and sudden mood swings
M: Conners 3 GI Total This index presents a global view of the Restless-Impulsivity and Emotional Lability indices, and can also be used as an indicator of overall psychopathology.
N: Conners 3 ADHD Index Identifies children/ adolescents “at risk” for ADHD
1Learning Problems and Executive Functioning are subscales of Learning Problems/Executive Functioning on the Conners’ 3-T.

26
Conners’ 3 Interpretive Guidelines: The authors of the Conners’ 3 Rating Scales (Conners’ 3) state that T-Scores greater than 60 are usually taken to indicate a clinically significant problem.
Interpretive Guidelines for Conners’ T-Scores and Percentiles
T-Score
Percentile
Interpretive Guidelines
<30 <2 Markedly Atypical (Low Scores are Good: Not a Concern) 30-34 2-5 Moderately Atypical (Low Scores are Good: Not a Concern) 35-39 6-15 Mildly Atypical (Low Scores are Good: Not a Concern) 40-44 16-26 Slightly Atypical (Low Scores are Good: Not a Concern) 45-55 27-73 Average (Typical Score: Should Not Raise a Concern) 56-60 74-85 Slightly Atypical (Borderline: Should Raise a Concern) 61-65 86-94 Mildly Atypical (Possibly Significant Problem) 66-70 95-98 Moderately Atypical (Indicates Significant Problem) >70 >98 Markedly Atypical (Indicates Significant Problem)
Furthermore, the greater number of subscales that show clinically relevant elevation (i.e T-Scores above 60), the greater likelihood that the Conners 3 scores indicate a moderate to severe problem. High scores on the ADHD Index are considered by the checklist authors to be useful for differentiating clinical ADHD individuals from non-clinical individuals. Please note, that the ADHD Index score reported is a probability % figure, not a T-score like the other Indexes.
27
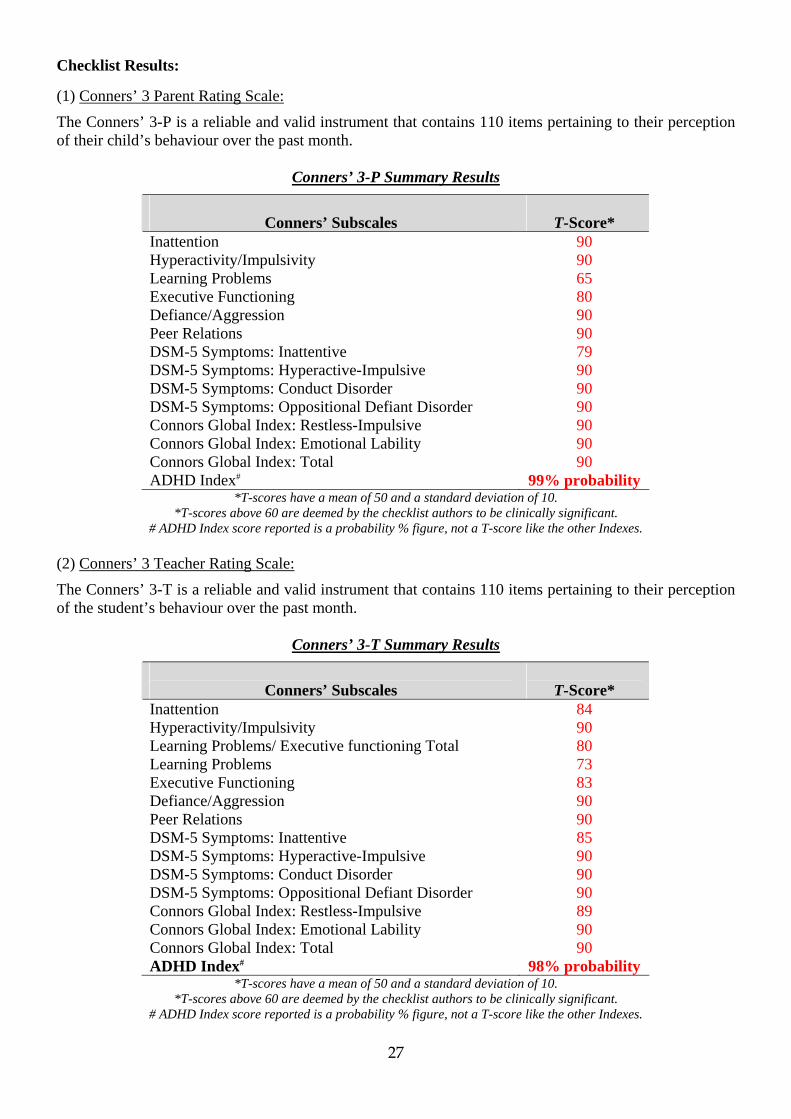
Checklist Results: (1) Conners’ 3 Parent Rating Scale:
The Conners’ 3-P is a reliable and valid instrument that contains 110 items pertaining to their perception of their child’s behaviour over the past month.
Conners’ 3-P Summary Results
Conners’ Subscales
T-Score*
Inattention 90 Hyperactivity/Impulsivity 90 Learning Problems 65 Executive Functioning 80 Defiance/Aggression 90 Peer Relations 90 DSM-5 Symptoms: Inattentive 79 DSM-5 Symptoms: Hyperactive-Impulsive 90 DSM-5 Symptoms: Conduct Disorder 90 DSM-5 Symptoms: Oppositional Defiant Disorder 90 Connors Global Index: Restless-Impulsive 90 Connors Global Index: Emotional Lability 90 Connors Global Index: Total 90 ADHD Index# 99% probability
*T-scores have a mean of 50 and a standard deviation of 10. *T-scores above 60 are deemed by the checklist authors to be clinically significant.
# ADHD Index score reported is a probability % figure, not a T-score like the other Indexes. (2) Conners’ 3 Teacher Rating Scale:
The Conners’ 3-T is a reliable and valid instrument that contains 110 items pertaining to their perception of the student’s behaviour over the past month.
Conners’ 3-T Summary Results
Conners’ Subscales
T-Score*
Inattention 84 Hyperactivity/Impulsivity 90 Learning Problems/ Executive functioning Total 80 Learning Problems 73 Executive Functioning 83 Defiance/Aggression 90 Peer Relations 90 DSM-5 Symptoms: Inattentive 85 DSM-5 Symptoms: Hyperactive-Impulsive 90 DSM-5 Symptoms: Conduct Disorder 90 DSM-5 Symptoms: Oppositional Defiant Disorder 90 Connors Global Index: Restless-Impulsive 89 Connors Global Index: Emotional Lability 90 Connors Global Index: Total 90 ADHD Index# 98% probability
*T-scores have a mean of 50 and a standard deviation of 10. *T-scores above 60 are deemed by the checklist authors to be clinically significant.
# ADHD Index score reported is a probability % figure, not a T-score like the other Indexes.
28
Summary of Conners’ results: The authors of the Conners’ 3 state that T-Scores greater than 60 are usually taken to indicate a clinically significant problem. Furthermore, the greater number of subscales that show clinically relevant elevation (i.e T-Scores above 60), the greater likelihood that the Conners’ 3 scores indicate a moderate to severe problem. John’ scores exceeded the cut-off for 14 on the Parent-report and 15 subscales on the Teacher-report. John’ parent-report score on the ADHD Index indicates that there is a 99% probability that he has ADHD, (unless another factor/diagnosis better explains the behaviours reported). John’ teacher-report score on the ADHD Index indicates that there is a 98% probability that he has ADHD, (unless another factor/diagnosis better explains the behaviours reported).

29
SUMMARY Reason for Referral: John was referred to Psychological and Educational Consultancy Services (PECS) by Dr Greg White (General Practitioner) for a Comprehensive Psychological Assessment and indication of whether the results are reflective of an individual with Autism Spectrum Disorder (ASD). Current Concerns: From a presented list, John’ parents identified concerns in the following areas:
• Academic problems • Attention problems • Learning problems • Written language problems • Receptive language problems • Expressive language problems • Behaviour problems • Anxiety problems • Bullying issues • Memory problems • Suspected hyperactivity • Possible education support placement • Social skills problems
Autism Spectrum Disorder DSM-5 Criteria: John meets sufficient DSM-5 criteria for a diagnosis of Autism Spectrum Disorder; requiring substantial support for deficits in social communication, and moderate support for restricted, repetitive behaviours. Cognitive Assessment: Because of John’ unusually diverse cognitive abilities, the combined WAIS-IV Full Scale IQ score is not a valid representation of his general cognitive ability, and therefore was not calculated. Instead, the PRI was deemed the most appropriate measure of his true cognitive ability. John achieved index scores at the following levels:
• Verbal Comprehension Index (VCI) = 13th percentile • Perceptual Reasoning Index (PRI) = 55th percentile • Working Memory Index (WMI) = 27th percentile • Processing Speed Index (PSI) = 27th percentile

30
Adaptive Behaviour: John’ parent-report ABAS score for the Social Domain was found to be at the 0.1st percentile (Extremely Low). Parent ABAS scores for the Conceptual Domain, Practical Domain and General Ability Composite could not be calculated due to insufficient responses. John’ teacher-report ABAS scores for the Conceptual Domain, Social Domain, and Practical Domain all fell in the Extremely Low category, culminating in a General Ability Composite at the 0.5th percentile (Extremely Low). Comorbidity and Differential Diagnosis Behavioural Assessment: John’ mother reported positive screens for:
• Generalised Anxiety Disorder • Separation Anxiety Disorder • Attention-Deficit/Hyperactivity Disorder: Combined Presentation • Language Disorder • Persistent Depressive Disorder • Conduct Disorder • Specific Learning Disorder – with Impairment in Written Expression
John’ teacher reported positive screens for:
• Generalised Anxiety Disorder • Attention-Deficit/Hyperactivity Disorder: Combined Presentation • Autism Spectrum Disorder • Language Disorder • Persistent Depressive Disorder • Conduct Disorder • Posttraumatic Stress Disorder
ADHD Behavioural Assessment: John’ parent-report score on the ADHD Index indicates that there is a 99% probability that he has ADHD, (unless another factor/diagnosis better explains the behaviours reported). John’ teacher-report score on the ADHD Index indicates that there is a 98% probability that he has ADHD, (unless another factor/diagnosis better explains the behaviours reported).
31
CONCLUSION AND STATEMENT OF DIAGNOSIS
Please note, this conclusion is based on the assessment results and background information currently available. Often, it is necessary/wise to perform follow-up confirmationary testing before definitive conclusive statements are made. John meets sufficient DSM-5 criteria for a provisional diagnosis of Autism Spectrum Disorder; requiring substantial support for deficits in social communication, and moderate support for restricted, repetitive behaviours. A formal diagnosis requires both a Child Psychiatrist/Paediatrician and a Speech Pathologist to concur with the findings of this assessment report. John’ cognitive profile confirms that an Intellectual Disability/Global Developmental Delay is not responsible for his difficulties/behaviours. John’ teacher-report ABAS scores for the Conceptual Domain, Social Domain, and Practical Domain all fell in the Extremely Low category, culminating in a General Ability Composite at the 0.5th percentile (Extremely Low). In addition to the Autism Spectrum Disorder, numerous possible comorbid disorders have been identified that require further assessment/intervention. The diagnosis of ADHD carries both comorbidity and differential diagnosis implications and requires consideration by the Child Psychiatrist/Paediatrician.
32
RECOMMENDATIONS
Please note, PECS does not provide micro-strategies (e.g., sit student at front of classroom, etc) as part of their recommendations. PECS provides recommendations on what further assessment is required, what intervention is necessary, and who is the most appropriate to provide the assessment/intervention recommended. GP Involvement (1) John should once again be seen by Dr Nnaji Nwoko (General Practitioner) now that this new
information is available for incorporation into his overall assessment. (2) Due to the large degree of information supporting possible ASD, it is recommended that John be
seen by a Paediatrician / Child Psychiatrist for the purpose of a formal decision on the presence of ASD.
Please note that a GP referral is required to see a Medical Specialist.
Speech Pathologist Involvement: (1) John should undergo an ASD assessment with a Speech Pathologist, prior to going to the
Paediatrician/Child Psychiatrist. (2) A copy of this report should be provided to Speech Pathologist prior to the assessment. (3) John should continue Speech Pathology to further develop his receptive and expressive language
skills. Child Psychiatrist/Paediatric Involvement: (1) John should be seen by a Child Psychiatrist/Paediatrician for the purpose of a formal decision of a
diagnosis of Autism Spectrum Disorder, and consideration of the comorbidity and differential diagnosis implications identified.
Both this report, and the Speech pathologist’s report should be forwarded to the Child
Psychiatrist/Paediatrician prior to the first appointment. Occupational Therapist Involvement: (1) John should continue Occupational Therapy to assist with the building of fine and gross motor
skills.
33
School Involvement: (1) A case-conference involving John’ parents, the school psychologist, and the classroom teacher
should be held to discuss John’ individual learning requirements.
(2) In light of these new assessment results, an Individual Education Plan (IEP) / Curriculum Adjustment Plan (CAP) should be initiated / amended by John’ teachers in an attempt to maximise John’ access to the curriculum.
(3) The Speech and Language Consultant at the local District Education Office should be contacted to
assist with further speech and language assessment and the implementation of language intervention services.
Dr Shane Langsford
Date of Report Managing Director -PECS
Registered Psychologist APS College of Educational & Developmental Psychologists Academic Member