Embed Size (px)
DESCRIPTION
very good
Citation preview

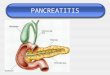
PANCREATITIS
When did the pain start?Pancreatitis is characterized by abdominal pain. It may be acute, chronic, or acute on chronic. The majority of patients will present with an acute episode. Episodes vary from mild to a severe life-threatening attack. Some will suffer multiple acute attacks while the occasional patient will have ongoing persistent pain.
Where is the pain worst? As the pain is frequently excruciating you must ask the patient to point with only one finger, this helps to localize the area. Visceral pain may be difficult to localize, but in pancreatitis it tends to be in the epigastrium.
Does the pain move anywhere?Patients will describe pain “gnawing” through to their back, a leaking abdominal aortic aneurysm must be considered in the older person. Also an erosive peptic ulcer should be included in the differential.
Does the pain come and go?Pain from solid organs tends to be constant “non stop”, whereas pain originating from a hollow viscus, such as the ureter and bowel, it comes and goes in waves due to the peristaltic action of the mural muscles against an obstruction. In persistent chronic severe pain, a pancreatic neoplasm should always be considered.
Does anything make it better or worse?Cholecystitis is aggravated following a fatty meal. Ureteric colic may worsen on micturition, with no improvement with postural change. Pancreatic pain may be somewhat relieved by sitting forward “the pancreatic position”. Patients tend to stay in one position with pancreatitis, unlike those with colicky pain who roll around relentlessly. Hot drinks and spicy foods aggravate peptic ulceration and gastritis. Eating may precipitate ischaemic pain in the gut, due to preferential blood flow to the stomach during meals.
Have you any nausea or vomiting?Timing can be helpful; delayed vomiting following a meal is typical of gastric outlet obstruction usually containing obvious food. Bilious vomiting suggests communication between the duodenum and the stomach although can occur from any cause of persistent vomiting. Blood in the vomitus can be from persistent vomiting leading to a Mallory Weiss tear of the oesphageal mucosa, or from gastritis and peptic ulceration. Vomiting is an almost consistent aspect to pancreatitis and will exacerbate the already volume depleted patient.
Do you have any medical problems? Do you drink?Questions relating to the potential causes of pancreatitis should be asked now. Causes: Gallstones (50-60% acute attacks), alcohol, metabolic causes such as hypercalcaemia of any cause ( 2%) and hyperlipidaemia, medications such as thiazide diuretics, steroid and azathioprine, Post – operative pancreatitis (third most common cause), and also unknown or idiopathic.The vast majority of those with pancreatitis in Ireland are due to alcohol and gallstones.
1

Investigations:
FBC WCC, Hb U+E UreaLFT’s , especially ASTSerum Amylase 2-3 fold rise usually diagnostic, >90% sensitivityUrinary Amylase Increased levels found for a longer durationCalcium Glucose LDH Coag Screen Check for coagulopathy, DICABG base excess
Ranson’s Criteria: 11 early objective signs which correlate well with overall morbidity and mortality.
ADMISSION 48 HOURS
INDICATED MORTALITY
2 or less signs 9%3 or 4 signs 16%5 or 6 signs 40%> 7 signs 100%
Radiology:PFA- To exclude other abdominal pathology such as a small bowel ileus.
CXR- Abnormal in up to 40% of patients, pleural effusions may be evident Left sided > than Right.
Ultrasound – Check for abscess, cyst or pseudocyst formation Associated cholelithiasis and common bile duct stones or obstruction in 80% of patients with biliary pancreatitis.
CT abdomen – Enlarged pancreas in 60-70% patients Contrast enhanced CT highlights areas of underperfusion, ie necrosis/abscess in > 80% of patients Used to guide fine needle aspiration of the pancreas for histology/culture.
Differential Diagnosis: Perforated duodenal ulcer Acute Cholecystitis Myocardial infarction Mesenteric arterial occlusion Acute hepatitis Abdominal aortic aneurysm Splenic rupture/ Ectopic pregnancy.
Age> 55yrs HCT > 10%
Serum Glucose > 11mmol/L Serum Calcium < 2 mmol/LWCC > 16 PaO2 < 8 Kpa
AST > 250 Urea > 1.8mmol/LLDH > 350 Base excess > -4 mmol/L
Fluid Replacement > 6L
2