Embed Size (px)
Citation preview

SBINewsThe Member Newsletter of the Society of Breast Imaging 2015 ISSUE 1
Society of Breast Imaging • 1891 Preston White Drive • Reston, VA 20191
Click here to read this issue!

www.SBI-online.orgii 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 1
Editor’s Note
Gary J. Whitman, MD, FACR, FSBI
Newsletter Editor: Gary J. Whitman, MD, FACR, FSBI, Chair
SBI Newsletter Committee: Shadi A. Shakeri, MD
Jay A. Baker, MD, FSBI
Jade de Guzman, MD
Wendy DeMartini, MD, FSBI
Stamatia V. Destounis, MD, FACR, FSBI
Peter R. Eby, MD, FSBI
Jessica W. Leung, MD
John M. Lewin, MD, FACR, FSBI
Ann M. Leylek, MD
Michael N. Linver, MD, FACR, FSBI
Louise C. Miller, RTRM
Robert Nishikawa, PhD, FSBI
Liane E. Philpotts, MD, FSBI
Murray Rebner, MD, FACR, FSBI
Layout & Design:
Graphic Design Associates, Inc.
Table of Contents2 | President’s Column: 2015: A Look To The Past And To The FutureBy Murray Rebner, MD, FACR, FSBI
4 | Technology Changes: Positioning ChallengesBy Louise C. Miller, RTRM
6 | Breast Imaging Fellowships Update By Jade de Guzman, MD
7 | Breast Cancer Screening with TomosynthesisBy Stamatia V. Destounis, MD, FACR, FSBI
8 | Upcoming Events & Activities
9 | The Value of Screening MammographyBy Ana C. Nelson, MSN, RN, FNP-BC and Therese B. Bevers, MD
11 | My Breast Cancer JourneyBy Oliver Bogler, PhD
12 | Updates in Radiation Therapy for Breast ConservationBy Jyoti Mayadev, MD
15 | My First RSNA – What I Would Do Differently Next TimeBy Ann M. Leylek, MD
17 | ACR 2015 Meeting Preview By Murray Rebner, MD, FACR, FSBI
18 | 2014 RSNA Synopsis: Digital Breast TomosynthesisBy Liane E. Philpotts, MD, FSBI
21 | 2014 RSNA MRI ReviewBy Stamatia V. Destounis, MD, FACR, FSBI
23 | 2014 RSNA Breast Ultrasound SummaryBy Paula Gordon, OBC, MD, FRCPC, FSBI
24 | 2014 RSNA Breast Density Legislation UpdateBy Shadi A. Shakeri, MD
27 | Radioactive Seed Localization: Experiences and ConcernsBy Laurie Margolies, MD, FACR
29 | SBI/ACR Breast Imaging Symposium PreviewBy Yasmeen Fields, CAE
The numbers are looking great!” I heard that phrase twice last week from administrators – the first time from a financial officer and
the second time from a doctor who became a bean counter.
What numbers really look great to us? Is it JUST the number of images read or the revenue captured? What about the number of subtle architectural distortions on mammography that you identified and they turned out to be cancers? What about the number of times that you sat down with a patient and her family and discussed the imaging findings in a humane, compassionate, professional manner? What about the number of times that you stopped and listened attentively as a colleague discussed some troubling issues with you? What about the number of times that you went out of your way to solidify a concept with a trainee just to make sure that he or she would retain the information?
On the Society of Breast Imaging (SBI) Newsletter team, we are blessed with a number of amazing contributors. Lisa Arnall, RDMS, a sonographer, is completing her term on the editorial board. Lisa did a great job, editing, writing, and contributing ideas. Lisa: THANK YOU!
John Boone, PhD, a physicist, is also finishing his term. John wrote articles, edited articles,
recruited people to write articles, and even recruited a member of our editorial board (Shadi A. Shakeri, who contributed an article on breast density legislation on page 24-26). John: THANKS for all your help.
Our new physicist on the editorial team is Robert Nishikawa, PhD from the University of Pittsburgh. We are looking forward to working with Robert.
Recently, Peter Eby, MD was named as the vice-chair of the SBI Newsletter committee. Peter is a talented writer, and he has been active in all facets of the newsletter, especially planning and editing. Peter will become the newsletter editor following the SBI/American College of Radiology (ACR) Breast Imaging Symposium in Orlando, April 25-28, 2015 (see page 29 for Yasmeen Fields’ article on the symposium). We thank Peter for his hard work and we look forward to his leadership.
Copyright 2015. Society of Breast Imaging.
April 25-28, 2015
Hilton Bonnet Creek Orlando, Florida
AC
R
Breast Imaging Symposium2 0 1 5
REGISTER TODAY!

www.SBI-online.org2 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 3
President’s Column: 2015: A Look To The Past And To The Future
It is early January as I write this column. I wish all of you a healthy and happy new year!
To quote Charles Dickens, “It was the best of times, it was the worst of times.” 2014 had its positives and negatives for breast imagers. On the plus side, data for digital breast tomosynthesis (DBT) continued to show improved cancer detection and lower patient recall rates compared to standard two-dimensional (2D) digital technology (1). As a result, the Centers for Medicare and Medicaid Services (CMS) approved DBT as a reimbursable, add-on G code to standard digital mammography. In addition, the cuts in reimbursement for image-guided breast procedures, which affected us in 2014, were reversed for 2015. However, as a friend of mine who is a member of the Relative Value Scale Update Committee (RUC), which suggests fee codes and reimbursements to CMS, said to me “The RUC giveth with one hand and taketh away with the other.” We need to be vigilant.
Dr. Christiane Kuhl demonstrated that an abbreviated breast magnetic resonance imaging (MRI) scan could be as accurate as a complete scan in the screening setting (2). This has major implications for screening the high-risk population: the potential for shorter scan times, increased throughput and lower cost. More extensive research is being planned.
A population-based mammography service screening study, which included 2.7 million women across Canada, demonstrated a mortality benefit for women who participated. Although this was not a randomized controlled trial, it showed an average mortality reduction of 40% for those who took part (3). Contrast these results with the flawed Canadian National Breast
Screening Study that showed no benefit from screening (4).
Unfortunately, there was a continued assault on screening mammography. The misrepresented topic of overdiagnosis remained in the forefront. In February 2014, Dr. Archie Bleyer attempted to defend his original New England Journal of Medicine article with a series of complex, unconvincing explanations and continued “guesstimates” in the journal The Oncologist (5). Dr. Daniel Kopans, our tireless expert supporter of screening, wrote an outstanding rebuttal in the same issue (6). Also, Drs. Mark Helvie and Edward Hendrick took the same Surveillance Epidemiology and End Results (SEER) data that Drs. Bleyer and H. Gilbert Welch used and demonstrated that, in the mammography era, late stage disease decreased by 37% and, more importantly, the incidence of invasive breast cancers decreased by 9% (7).
In 2014, the Unites States Preventive Services Task Force (USPSTF) began its work formulating recommendations for breast cancer screening. Multiple letters objecting to the methodology of the task force were written by the Society of Breast Imaging (SBI)/American College of Radiology (ACR) leadership and sent to the task force’s parent and overseeing organization, the Agency for Healthcare Research and Quality (AHRQ). SBI/ACR leaders also met in person with members from AHRQ and discussed the same problems. However, it appears that no significant changes were made to the task force that would improve the process.
What can we expect this new year? The good news is that the SBI will continue to focus on its education mission. Dr. Elizabeth Morris and her planning committee have put together an outstanding innovative program for the spring SBI/ACR Breast Imaging Symposium.
For the first time, the SBI will offer educational content for the annual ACR meeting to be held in May in Washington, DC. Four and one half hours of informative material dealing with breast cancer epidemiology, screening, technology, economics, and Breast Imaging Reporting and Data System (BI-RADS®), as well as challenging interactive cases, will be presented by SBI experts (see the accompanying article in this edition of the SBI Newsletter on page 17).
Our popular weekend courses will continue. Since DBT utilization continues to increase, the focus of these meetings will be on this new technology.
Our e-learning products continue to evolve. This year, we continue to offer our members the opportunity to obtain their Maintenance of Certification requirements online with the SBI. We are also making it easier to become a member and renew annual dues online.
There are also unknowns in 2015 which may damage our specialty. The most concerning one again relates to the USPSTF’s final screening guidelines. If the task force decides to recommend against annual screening mammography starting at age 40 years, there likely will be a cascade of negative effects. Fewer health care providers will recommend annual screening to begin at age 40, reimbursement restrictions may be instituted, fewer women will undergo screening, and most important, lives will be lost unnecessarily.
It should be noted that the American Cancer Society will also be issuing new mammography screening guidelines this spring. Their
recommendations will also have a major impact on screening coverage and utilization.
This year will not be a dull one. Rest assured that the SBI is committed to provide our members with the best educational tools to practice our specialty, which in turn will help them offer the highest level of care to their patients.
Murray Rebner, MD, FACR, FSBI
President, Society of Breast Imaging
REFERENCES 1. Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 2014;311:2499-2507.
2. Kuhl CK, Schrading S, Strobel K, Schild HH, Hilgers RD, Bieling HB. Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J Clin Oncol 2014;32:2304-2310.
3. Coldman A, Phillips N, Wilson C, et al. Pan-Canadian study of mammography screening and mortality from breast cancer. J Natl Cancer Inst Oct 1, 2014;106.
4. Miller AB, Wall C, Baines CJ, Sun P, To T, Narod S A. Twenty five year follow-up for breast cancer incidence and mortality of the Canadian National Breast Screening Study: randomised screening trial. BMJ Feb 11, 2014.
5. Bleyer A. Were our estimates of overdiagnosis with mammography screening in the United States “based on faulty science”? Oncologist 2014;19113-126.
6. Kopans DB. Arguments against mammography screening continue to be based on faulty science. Oncologist 2014; 19107-112.
7. Helvie MA, Chang JT, Hendrick RE, Banerjee M. Reduction in late-stage breast cancer incidence in the mammography era: implications for overdiagnosis of invasive cancer. Cancer 2014;120:2649-2656.
President’s Column, continued from previous page
Murray Rebner, MD, FACR, FSBI

www.SBI-online.org4 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 5
tomosynthesis and tomosynthesis upgradeable units arrived with an increase in length of the IR once again. Within most of our careers, we have experienced an increased length in Bucky/IR of up to 49% and an increased thickness of the Bucky/IR of up to 80%.
Face ShieldWhile face shield measurements remained fairly consistent from film-screen to digital imaging, modifications were made for tomosynthesis units to accommodate the tube movement. This required an increased width of the shield up to 50% when compared to non-tomosynthesis units.
Possible, And Often Correctable, Changes In Clinical Images1. Inadequate length of the pectoralis muscle on
the mediolateral oblique (MLO) view, optimally visualized down to the posterior nipple line (PNL), and/or inadequate imaging of the inframammary fold (IMF): The increased length of the IR requires an adjustment of the patient. Patient positioning and selection of the proper degree of angulation are also essential.
2. Inadequate width of the muscle at the axilla on the MLO view: Due to the increased width of the IR, the technologist should ensure that the corner of the IR is placed properly in the axilla.
3. Inadequate visualization of the deep medial breast tissue on the craniocaudal (CC) view: The increased width of the face shield may prohibit the patient’s head from coming forward and around the shield and could lead to the exclusion of medial breast tissue and poor visualization of the cleavage area. Careful attention must be given to positioning techniques in order to avoid this potential error.
4. Visualization of the latissimus dorsi muscle, many times identified as the pectoralis minor muscle on the MLO view: Some patients’ axillae are too “narrow” to accommodate the
increased thickness of the IR. It therefore may be necessary to place the IR behind the latissimus dorsi muscle.
5. Increase in skin and fat folds: Skin and fat folds, while often “burned out” on film-screen images, are enhanced with digital imaging. This is due to differences in imaging techniques. Attenuation of the beam, caused when the digital algorithm is applied to the thicker skin, is most common in the posterior breast and nipple area on the CC view, and in the IMF and the axilla on the MLO view. While proper positioning can reduce the presence of skin and fat folds, these folds cannot be entirely eliminated. Breast tissue should never be sacrificed to exclude a fold. An additional image should only be taken if the skin or fat folds impede adequate visualization of the breast tissue. Fortunately, tomosynthesis eliminates this need altogether.
6. Motion artifact: Many facilities have seen an increase in call backs due to motion artifact. Unfortunately, technologists cannot see the motion on their workstations, so motion may go undetected until seen by the radiologist and a call back may be required. Many times having the patient stop breathing during the exposure can be helpful.
While there are no current data published on the above observations, my experience is that the evolution in technology has also produced some changes in our clinical images. Ideally, each technologist and each radiologist must be aware of the differences and do their best to adjust to the technological changes so that we can produce optimal image quality for our patients. However, even while taking these factors into consideration, technically ‘perfect’ images are very difficult to obtain. Further studies should be conducted to quantify reasonable expectations based on the numerous variables that mammographers face.
Technology Changes: Positioning Challenges By Louise C. Miller, RTRM
Mammographers have seen many changes in mammographic technology and equipment over the course of their careers. Yet many of
us have not been given the skills and tools needed to make the transition smoothly. As things evolved, we did our best to adapt with very few resources available. Most manuals and videos for positioning techniques were created for film-screen equipment. Even with mandated initial and continuing education requirements, most of us were not taught consistent, reproducible and ergonomically sound positioning methods. Variations in styles were passed from one generation of mammographers to the next. As technology changed and improved, most of us were not aware that our positioning techniques needed to change and improve also.
If, like me, you remember Xerography, you are most likely ready for retirement. Younger mammographers have no understanding of table-top imaging, blue toner, charged plates, compression balloons, curved paddles or sponges. We learned to position by the “see one, do one, teach one” method. We figured it out. Then it was on to film-screen equipment. No more sponges, no more ribs…and what about the skin line? The pectoralis muscle suddenly became a major focal point and compression changed dramatically: straight paddles instead of curved paddles, “rigid” compression instead of soft sponges. Clinical image evaluation standards were set. There were seminars and application specialists to help us make the transition…barely.
Just when we were getting comfortable, digital imaging arrived. Most of us have direct experience with that transition, perhaps the most significant change that mammographers have experienced. Now technologists of all ages are wrestling with the transition from digital mammography to tomosynthesis. While each new modality requires eight hours of specialized training, most often
offered and obtained from the equipment manufacturer, none includes specific positioning training or hands-on experience with actual patients. So we are left to try to figure it out…again…and most of us struggle a bit at first. In retrospect, we ask ourselves: if the technology and equipment change, do the positions change? Will our images change? A new way of “looking at things” is essential to answer those questions. The real question is: why would it not change?
Equipment ChangesThe biggest positioning challenges are related to the increased length and thickness of the image receptor (IR). The increased width of the face shield can prove to be an additional problem. These differences can frequently be a challenge for the technologist when transitioning to each new modality. How can the technologist compensate for this and how can this affect our clinical images? A complete understanding of the equipment differences, proper positioning and patient anatomy is essential.
Image ReceptorStandards for film-screen units in the United States are based on two sizes of imaging platforms: 18 x 24 cm and 24 x 30 cm. As digital technology was developed, the 18 x 24 detector was initially adapted. However, according to demographics at that time, up to 30% of patients could not be accommodated on the smaller platform, resulting in sub-optimal “tiling” or “mosaic” image acquisition. Both manufacturers of digital equipment in the United States (General Electric and Hologic) then chose a larger option of 24 x 29-31 cm with various sized compression paddles. While the interchangeable and movable paddles were helpful for positioning, the increased size of the image receptor often pushed back against the patients and mammographers. The next generation of
Technology Changes: Positioning Challenges, continued from previous page

www.SBI-online.org6 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 7
Breast Imaging Fellowships UpdateBy Jade de Guzman, MD
In recent years, breast imaging fellowships have become increasingly popular and more competitive to obtain (1). In a recent survey
conducted by the Society of Breast Imaging (SBI) and the Education Committee of the American College of Radiology (ACR) Breast Commission, two-thirds of responding programs reported an increase in fellowship applicants with three-quarters having three or more applicants per position (2). The purpose of this article is to review the application experience from both the applicant and the program perspective.
Because breast imaging fellowships are not accredited by the Accreditation Council for Graduate Medical Education (ACGME), applicants and programs do not participate in the match. For this reason, most programs recruit and start accepting applications earlier in the year, many of which start offering positions on a “rolling” basis. This forces the applicants to start preparing their applications late in the second year or early in the third year of radiology residency. This can be extremely stressful on the part of the applicants who may not rotate on breast imaging until late into their second year of residency.
Upon deciding to pursue a career in breast imaging, most applicants use word-of-mouth information from colleagues and their breast imaging attendings in order to decide where to apply and how many programs they should apply to. Most applicants indicate that location, reputation of the program and specific training experience (i.e., number of months of dedicated breast imaging, volume including diagnostic breast magnetic resonance imaging (MRI) and interventional procedures, exposure to body MRI if dual body/breast women’s imaging program) as the most important factors in deciding where to accept a position.
Apart from the SBI Fellowship and Curriculum website (3), which includes a listing of most programs in the United States and Canada, there is no central source to search for programs. The listing on the SBI website does not include all of the programs and does not indicate how many positions are actually still available in real-time (3). Many applicants find this experience frustrating since a lot of time may be spent preparing an application for positions that have already filled. A majority of spots fill internally which makes it more difficult to pursue a career in breast imaging if one’s home institution does not offer a breast imaging fellowship or if only a limited number of positions are available.
To add to the stressful nature of the application process, many residents report the experience of having to accept a position without even having interviewed or heard from other institutions they were interested in. Some programs are more flexible in this regard, allowing the applicants to interview elsewhere before deciding, but usually offering a short period of time to respond.
From the program perspective, there is also much pressure to secure desirable candidates earlier in the year. For this reason, many programs have progressively started to interview and accept earlier in the year as early as July 1st. The application usually consists of a curriculum vitae, a personal statement, United States Medical Licensing Examination scores and three letters of recommendation. Programs have also reported difficulty maintaining or obtaining funding for fellowship positions either internally from their departments or externally from charitable organizations. This is concerning in light of the fact that breast imaging fellowships have become increasingly competitive in recent years.
I personally was fortunate enough to train at an institution where I was able to stay for a breast imaging fellowship as one of several internal candidates. It is disheartening to hear how difficult it is for radiology residents who train at institutions that do not offer breast imaging fellowships. At the very least, I encourage all breast imaging fellowship directors to list their programs and positions available on the SBI website.
REFERENCES 1. Bassett LW, Bent C, Sayre JW, Marzan R, Verma A, Porter C. Breast imaging training and attitudes: update survey of senior radiology residents. AJR Am J Roentgenol 2011;197:263-269.
2. Farria DM, Salcman, Monticciolo DL, Monsees BS, Rebner M, Bassett LW. A survey of breast imaging fellowship programs: current status of curriculum and training in the United States and Canada. J Am Coll Radiol 2014;11:894-898.
3. http://www.sbi-online.org/RESOURCES/BreastImagingFellowshipsandCurriculum.aspx Acccessed November 11, 2014.
Breast Imaging Fellowships Update, continued from previous page
Breast Cancer Screening with TomosynthesisBy Stamatia V. Destounis, MD, FACR, FSBI
In the Journal of the American Medical Association (JAMA) on June 24, 2014, Dr. Sarah Friedewald of Advocate Lutheran General
Hospital in Park Ridge, IL and other researchers found that adding digital breast tomosynthesis (DBT) to standard mammography increased invasive cancer detection by more than a third compared to mammography alone, while reducing false positives by 15% (1).
The lead author, Dr. Friedewald, was excited by the study’s results and shared some of her thoughts with me via telephone shortly after publication of the article in JAMA. Mammography has been criticized for overdiagnosis and excessive false positives that create anxiety among women and their families. This study, Dr. Friedewald said, addresses the criticisms of mammography related overdiagnosis and false alarms. She also shared that women she encounters in her daily practice are very willing to undergo extra testing in order to know for certain that they are healthy.
Friedewald and the team of researchers from 13 facilities assessed breast cancer detection rates, recall rates, and positive predictive values for recall
and biopsy from March 2010 to December 2012. For the DBT exams, all 13 sites used Hologic Selenia Dimensions units. The sites were diverse in geographic location and academic versus nonacademic settings, and subspecialized breast imagers versus general radiologists participated in the study. The lead author felt that these were some of the strengths of this study. Most of the sites partially adapted DBT technology and a few converted entirely to DBT.
The study included 454,850 examinations, of which 281,187 were digital mammography and 173,663 were digital mammography plus DBT. Of the patients undergoing digital mammography alone, 29,726 (10.7%) were recalled; 5,056 biopsies were performed and cancer was diagnosed in 1,207 (23.9%) of which 815 were invasive and 392 were in situ.
The following year with the combination of digital mammography and tomosynthesis 15,541 (9.1%) patients were recalled; 3,285 biopsies were performed and cancer was diagnosed in 950 (28.9%) with 707 invasive and 243 in situ.

www.SBI-online.org8 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 9
Upcoming Events & Activities2015
April 25-28 – Orlando, FL SBI/ACR Breast Imaging Symposium
May 17 -21- Washington, DC ACR 2015 — The Crossroads of Radiology
September 26 - 27- San Diego, CACase-Based Review & Advanced Breast Imaging Course: Digital Breast Tomosynthesis
November 29 - December 4 – Chicago, IL Radiological Society of North America (RSNA)
For a listing of other society events please check out the SBI Calendar of Events at www.sbi-online.org
Friedewald and colleagues found that the combination of digital mammography and DBT not only reduced recalls but also increased overall and invasive cancer detection rates while ductal carcinoma in situ rates remained the same. The overall cancer detection rate increased from 4.2 per 1000 with digital mammography alone, to 5.4 per 1000 when mammography was combined with DBT and recalls were reduced by 15%.
Eleven of the thirteen sites observed a decrease in recall rate when screening with digital mammography and DBT. Two of the sites had an increase in recall rates when implementing DBT. Twelve sites had an increase in overall and invasive cancer detection rate. The single site with a decrease in overall and invasive cancer detection also reported the lowest volume of DBT. The study did find that DBT plus mammography increased the biopsy rate over mammography alone by 7%, from 18.1 biopsies per 1,000 cases to 19.3 biopsies per 1,000 cases. But there was a corresponding increase of 1.2 cancers detected per 1000 cases.
The study does have limitations. The design was not randomized and selection bias could be present because most of the facilities did not completely convert to DBT. No follow-up
examination data are available and the statistics were calculated at the population level rather than patient level from each site.
Overall, the study supports recent prospective research performed in Europe and the United States. Skaane reported a 40% increase in invasive cancer detection rate and a decrease in recall rate (2). Similarly, other studies by Ciatto and Rose reported similar reductions in the recall rate and an increase in cancer detection (3, 4).
REFERENCES 1. Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA.2014;311: 2499-2507.
2. Skaane P, Bandos AI, Gullien R, et al. Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology.2013;267:47-56.
3. Ciatto S, Houssami N, Bernardi D, et al. Integration of 3D digital mammography with tomosynthesis for population breast cancer screening (STORM): a prospective comparison study. Lancet Oncol. 2013;14:583-589.
4. Rose SL, Tidwell AL, Bujnoch LJ, Kushwaha AC, Nordmann AS, Sexton R Jr. Implementation of breast tomosynthesis in a routine screening practice: an observational study. AJR. 2013;200:1401-1408.
Breast Cancer Screening with Tomosynthesis, continued from previous page The Value of Screening MammographyBy Ana C. Nelson, MSN, RN, FNP-BC and Therese B. Bevers, MD
While the evidence proves that fewer women die of breast cancer as a result of screening mammography, there have
been numerous attempts since the 1990s to cast doubt on the value of this test. The controversy escalated in 2009 when the United States Preventive Services Task Force (USPSTF) issued their recommendations on this topic (1). The USPSTF, considering the overall benefits and harms of the test, recommended biennial screening mammography for women aged 50 to 74 years and an individualized decision to start screening mammography for women in their 40s. The task force also concluded that there was insufficient evidence to assess the benefits and harms of screening mammography for women aged 75 years or older (1).
The USPSTF 2009 recommendations were informed by a systematic review of the randomized controlled trials of screening mammography (2) which showed a relative risk (RR) reduction of 15% for women aged 40 to 49 years (95% confidence interval [CI] 0.75-0.96) and 14% for women aged 50 to 59 years (95% CI: 0.75-0.99).
The USPSTF recommendation was also informed by Cancer Intervention and Surveillance Modeling Network (CISNET) modeling (3) which showed that biennial screening mammography retained 81% of the benefit of annual screening mammography with almost half the number of false-positive results.
For all women undergoing screening mammography, it is important to weigh the benefits and harms of screening. Benefits include mortality reduction and, possibly, the need for less intensive treatment (e.g., some women with early stage disease do not require chemotherapy). The primary harms include false-positive results and overdiagnosis (4).
The USPSTF recommended against routine screening mammography for women aged 40 to 49 years, citing uncertainty that the benefits of screening for this population outweigh the harms. However, the CISNET analysis noted that if program benefits are to be measured in life-years, the metric most commonly used in cost-effectiveness analysis, initiating screening at age 40 saves more life-years, albeit at the cost of an increase in the number of false-positive mammograms (3). Overall, 40% of years of life lost to breast cancer are exacted from women diagnosed in their 40s (4). Many women, especially those in their 40s, find that the value of a reduced risk of dying from breast cancer, potentially less intensive treatment and being available in the long-term to take care of their families, outweigh the associated harms.
For women aged 50-74 years, the USPSTF reported that the lower rate of false-positive results of biennial screening for this population justified a compromise in breast cancer mortality reduction (1). Not all women, or their clinicians, agree with this conclusion.
False-positive results occur when a screening test is positive but no cancer is found on additional evaluation. About 10% of women in each round of screening will be recalled for additional evaluation and more than 80% of these women will have a normal or benign result after undergoing additional mammography, ultrasound or needle biopsy (5). For most women, false-positive results that require
additional testing, while anxiety-provoking, do not seem to interfere with future screening participation (5). Recently, tomosynthesis, or 3D mammography, a new technology that obtains a series of images of the breast that can be

www.SBI-online.org10 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 11
reconstructed into slices, has been shown to increase the detection of breast cancer, decrease the number of recalls and improve the positive predictive value (PPV) of mammography (i.e., decrease false-positives). A recent study by Friedewald et al has shown an increase in the PPV for mammography from 4.3% to 6.4% [difference, 2.1%; 95% CI, 1.7%-2.5%; P < .001] when incorporating tomosynthesis (6). Reducing false-positives and improving the PPV of recalls improves the efficacy of screening mammography.
Overdiagnosis occurs when a breast cancer is discovered that would not become clinically relevant in a woman’s lifetime. However, the real concern is not overdiagnosis but the over-treatment of a breast cancer. Over-treatment happens when women undergo unnecessary interventions, such as mastectomy, for a clinically irrelevant breast cancer. It does not seem reasonable to abandon mammographic screening based on our incomplete understanding of which breast cancers do or do not require aggressive intervention. Studies to define such characteristics are currently underway (7).
At this time, mammography is the only screening modality that has been shown in randomized controlled trials to reduce breast cancer mortality. While the USPSTF recommendations provide a framework for counseling women regarding the benefits and harms of breast cancer screening, it is important to appreciate that fewer women die from breast cancer as a result of the test. Since
many women do not have the same concerns as the USPSTF about the harms of screening, they should be allowed to make an informed, personal decision about screening mammography.
REFERENCES 1. U.S. Preventive Services Task Force Screening for breast cancer: recommendation statement. Annals of Internal Medicine.2009;151:716-726.
2. Nelson HD, Tyne K, Naik A, Bougatsos C, Chan BK, Humphrey L. Screening for breast cancer: systematic evidence review update for the U.S. Preventive Services Task Force. Annals of Internal Medicine. 2009;151:727-737.
3. Mandelblatt JS, Cronin KA, Bailey S, et al. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Annals of Internal Medicine.2009:151738-747.
4. Smith, RA, Cokkinides V, Brooks D, Saslow D, Brawley OW. Cancer screening in the United States, 2010: a review of current American Cancer Society guidelines and issues in cancer screening. CA Cancer Journal for Clinicians.2010: 60: 99-119.
5. Brewer NT, Salz T, Lillie SE. Systematic review: the long-term effects of false-positive mammograms. Annals of Internal Medicine.2007:146: 502-510.
6. Friedewald SM, Rafferty EA, Rose SL, et al. Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA. 2014:311:2499-2507.
7. Francis A, Bartlett J, Billingham L, et al, HTA – 11/36/16: The Low Risk DCIS (ductal carcinoma in situ) Trial.(2014-2025) University of Birmingham, United Kingdom. Retrieved from http://www.nets.nihr.ac.uk/projects/hta/113616. Accessed on October 25, 2014.
The Value of Screening Mammography, continued from previous page
I t started in the classical way: I felt a lump in my right breast just behind the nipple. It couldn’t be cancer – after all, it was slightly painful and
cancer lumps don’t hurt and it felt larger some days than others. It couldn’t be – the coincidence that this disease would strike our family again, five years after my wife’s diagnosis, was just too unlikely. And so it took several months for me, a 20-year cancer scientist, to go to a doctor. After I did, things moved fast. First, I saw my primary care physician for a sanity check. Then I went to a breast cancer surgeon who quickly referred me for a mammogram, which led to an ultrasound and right away a biopsy. The radiologist and the pathologist, looking at the histology, quickly saw what was confirmed a day or two later: breast cancer.
Since my diagnosis, I have met many fellow cancer survivors, and I have learned that every cancer journey is unique. Mine is characterized by the obvious cultural dissonance of being among the 1% of breast cancer patients who are not women. It has led to a new dimension of shared experience with my wife. I benefited immeasurably from having seen her bravely navigate her therapy, and from her support and love. My journey is also unusual in that I am receiving my care at the same cancer center where I work, and so the doctors who care for me are also my colleagues. Ideally a journey is an opportunity for learning. So what have I learned?
Perhaps foremost is a new respect and affection for the medical professionals who care for me. My medical oncologist, who orchestrates the overall care and is with me for the long haul, and my surgeon and radiation oncologist, who delivered very important care, are prominent. Then there are many other specialists I met briefly or saw in my
medical record who made critical contributions to my care including radiologists, pathologists anesthesiologists, interventional radiologists, surgeons and genetic counselors. For the trials I joined there are the principal investigators and the research nurses who make them happen. Then there are the many physician assistants, nurses, phlebotomists and technologists who help with the many things that a cancer patient experiences. I thank you all.
I also learned that there remain significant opportunities for progress in understanding breast cancer in men. The treatment I received was essentially identical to my wife’s. On the one hand, this is not surprising as we had similar diagnoses: hormone receptor positive, HER2 negative ductal carcinoma. On the other hand, given that these are hormone driven cancers, I wonder whether we are missing some important biological differences. I do expect that my treatment will be effective, but this confidence is based on limited data, particularly for men like me, diagnosed 20 years younger than the median age. As I have posted on my blog, malebreastcancerblog.org, I was not able to find any NIH grants focused on the biology of male breast cancer, which against the backdrop of the $600 million per year the NCI currently invests in breast cancer research is an opportunity missed. Similarly, a search of clinicaltrials.gov showed that men were only eligible for one third of the breast cancer clinical trials, including many studies where the biology of their tumors would make them eligible, suggesting that the issue of equal access needs to be considered. I guess another thing I have learned from cancer is to find my advocate’s voice, and so I thank you for the opportunity to share my thoughts with you.
My Breast Cancer JourneyBy Oliver Bogler, PhD
Like, Follow, and Join SBI on Social Media

www.SBI-online.org12 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 13
Updates in Radiation Therapy for Breast ConservationBy Jyoti Mayadev, MD
Through the advent of more sophisticated imaging techniques, results of large randomized phase 3 trials looking at dose
and schedules, brachytherapy, and intraoperative radiation, the field of breast radiation therapy has evolved tremendously over the last decade. This article provides an update on radiation therapy for early stage breast cancer following breast conservation.
HypofractionationRadiotherapy is the standard treatment after breast conserving surgery, reducing the risk of local failure and improving overall survival in patients with early stage breast cancer. Recently, several large randomized trials have been published to suggest that women can be treated with a shorter course than the standard fractionation (1-5). The most common fractionation schedule is 50 Gy in 25 fractions delivered over five weeks. The four large randomized hypofractionation trials with up
to 10 years follow-up data showed equal results in terms of outcome and toxicity compared to the standard regimen, as shown in Table 1 (1-5).
Accelerated Partial Breast Irradiation Accelerated partial breast irradiation (APBI) is a localized form of radiation treatment (brachytherapy) that involves the insertion of a single multichannel catheter or multiple catheters for breast conservation therapy. The program is truly multidisciplinary in its formation, execution, and delivery of patient care. APBI programs rely on strong communication and team effort involving surgical oncology, medical oncology, and radiation oncology, including physicians, medical physicists, medical dosimetrists, and radiation therapists to provide this treatment option to early stage breast cancer patients. APBI delivers a highly conformal and effective dose of radiation while
greatly reducing treatment time. APBI is usually performed about one to four weeks after a lumpectomy. In addition to the multichannel brachytherapy option, there are three types of single-entry breast brachytherapy devices. The surgeon and radiation oncologist choose which one to use for the given patient based on the size and the shape of the lumpectomy cavity: The Strut Assisted Volume Implant (SAVITM) device has
7-11 “struts” or catheters through which the iridium seed travels. The struts are expanded after the device is inserted into the lumpectomy cavity. The Mammosite® consists of a balloon that is inserted into the lumpectomy cavity and inflated. The original Mammosite balloon had a single lumen catheter. The Mammosite ML has four lumens through which the iridium seed travels. The ConturaTM Multi-Lumen Balloon (MLB) is also a
Table 1: Hypofractionation trials and results
Updates in Radiation Therapy, continued from previous page
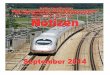
Figure 1. Prone positioning of a left sided breast cancer patient with the red arrow depicting the posterior border of the beam to spare the heart.

www.SBI-online.org14 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 15
balloon device with five lumens (catheters) through which the iridium seed travels. The Contura™ MLB also has vacuum ports on either end of the balloon to remove air or fluid between the balloon and the targeted breast tissue.
Intraoperative Breast RadiationIntraoperative radiation therapy (IORT) is radiation that is delivered during surgery, directly into the cavity where the tumor has just been removed. Most eligible patients will not need additional radiation, except for patients with adverse features when the final pathology report returns. Data continues to develop from IORT with various applicators available. The usual eligibility criteria include small tumors, age over 50 years, and invasive ductal carcinoma. After the lumpectomy, a spherical applicator on the IORT device is placed directly into the tumor bed. A radiation dose that is smaller than standard radiation therapy is delivered directly to the tumor bed over about 30 minutes. The major study of IORT in breast cancer was the TARGIT-A trial (6). In this study, breast cancer patients were given either IORT or standard external beam radiotherapy (EBRT) (6). The results showed that after four years, both therapies were almost equally effective in selected patients (6).
Prone Breast TreatmentsThe heart can be particularly vulnerable to the late effects of radiation when the left breast is treated in the supine position. Positioning women with early stage breast cancer in the prone position while undergoing radiation treatments can substantially decrease the radiation dose that reaches the heart, the lungs, and the skin. A
customizable positioning device allows the woman to lie comfortably in the prone position for radiation treatment, and the affected breast falls away from the chest wall. In selected patients, prone positioning can reduce normal tissue dosing and potential toxicity. Several studies have shown that prone breast irradiation decreases the dose to the lungs and the heart. Figure 1 represents a prone positioned breast with the subsequent beam placed to spare the heart in a patient with left sided breast cancer.
REFERENCES 1. Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med 2010; 362:513-520.
2. Haviland JS, Owen JR, Dewar JA, et al. The UK Standardisation of Breast Radiotherapy (START) trials of radiotherapy hypofractionation for treatment of early breast cancer: 10-year follow-up results of two randomised controlled trials. Lancet Oncol 2013; 14:1086-1094.
3. Owen JR, Ashton A, Bliss JM, et al. Effect of radiotherapy fraction size on tumour control in patients with early-stage breast cancer after local tumour excision: long-term results of a randomised trial. Lancet Oncol 2006; 7:467-471.
4. Kim JY, Jung SY, Lee S, et al. Phase 2 trial of accelerated, hypofractionated whole-breast irradiation of 39 Gy in 13 fractions followed by a tumor bed boost sequentially delivering 9 Gy in 3 fractions in early-stage breast cancer. Int J Radiat Oncol Biol Phys 2013;87:1037-1042.
5. Bentzen SM, Agrawal RK, Aird EG, et al. The UK Standardisation of Breast Radiotherapy (START) Trial A of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet Oncol 2008; 9:331-341.
6. Vaidya JS, Joseph DJ, Tobias JS, et al. Targeted intraoperative radiotherapy versus whole breast radiotherapy for breast cancer (TARGIT-A trial): an international, prospective, randomized, non-inferiority phase 3 trial. Lancet 2010; 376:91-102.
Updates in Radiation Therapy, continued from previous page My First RSNA – What I Would Do Differently Next TimeBy Ann M. Leylek, MD
As a first-time attendee of the Radiological Society of North America (RSNA) meeting in 2014, I planned not to have a plan. I
planned to wing it. However, from the first moment I arrived at McCormick Place, I realized that I needed an actual plan. Ironically, the epiphany struck me as I ran back and forth across the entire conference center to find the editorial board meeting for the Society of Breast Imaging (SBI) Newsletter!
Whether you are a trainee, a practicing radiologist, a medical physicist or an industry professional, RSNA is unlike any other conference. The Healthcare Convention and Exhibitors Association ranked it the third largest medical meeting in the United States in 2013 (1). More than 56,000 people attended the 2014 RSNA Scientific Assembly and Annual Meeting, including nearly 29,000 professionals from over 100
countries (2). This past meeting featured greater than 2,100 educational exhibits and 2,700 scientific presentations from 16 subspecialties (3). Concordantly, the venue is enormous. Chicago’s McCormick Place comprises four buildings that span 2.6 million square feet (4).
The following pearls of wisdom are those that I found most valuable during my maiden voyage to Chicago for RSNA:
Arrive with a game plan. Know what you want to get out of the meeting ahead of time. Whether you are most interested in attending scientific talks, meeting with vendors, networking, or a combination thereof, decide this before you arrive. The sheer size of RSNA can overwhelm even a seasoned conference-goer, so plan your schedule for each day.
Wear comfortable shoes. You will walk a lot. The daily mileage can easily double when you get lost (and you will get lost) so keep your RSNA pocket guide map on hand. The information booths are also a convenient resource to help you reach your destination.
Capitalize on networking opportunities. RSNA is a massive conference so odds are good that someone you want to meet will be there, but odds are slim that you will serendipitously bump into that person. Before RSNA, take advantage of the opportunity to set up any meetings with friends, former colleagues, and future job prospects. Improve your networking potential by attending any of the many social events happening (i.e., vendor parties, alumni reunions, resident and fellow section events, etc).
Follow your interests. Pick up the subspecialty brochures (one even caters to trainees) available in the main concourses to help you identify

www.SBI-online.org16 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 17
pertinent offerings. You may not have pre-registered for an interesting session, but if you hang around as it begins, you can often sneak into an empty seat or find standing room.
Take advantage of being a trainee. Find the RSNA Resident and Fellow Lounge for free lunch and refreshments all week. Check out the “Essentials” series for a good review of the basics in many areas. Attend Monday’s RSNA/American College of Radiology (ACR) Resident and Fellow reception to meet trainees from around the world and do not miss Wednesday’s RSNA Resident and Fellow symposium, which offers career advice and strategies for focusing on advocacy, marketing yourself, evaluating job offers and succeeding in radiology.
Realize you cannot do it all. Do not overwhelm yourself with 100 lectures. Instead, catch up on the highlights from each day in the Daily Bulletin available in print, online, or via the RSNA app. Other popular attractions from the annual meeting,
including the case of the day – image-based case scenarios spanning 14 radiology subspecialties – and educational materials are available online. Let your fingers do some of the walking.
Try the Chicago style pizza. Locals hotly debate which of Chicago’s cheesy deep-dish wonders is the best, but a few of the top contenders are Gino’s East, Lou Malnati’s, and Giordano’s. You know what they say: “When in Rome…!”
REFERENCES 1. ttp://www.hcca.org/?page=research_top%2050 (accessed on February 7, 2015)
2. http://rsna2014.rsna.org/information/attendancefigures.cfm (accessed on February 7, 2015)
3. http://rsna.org/NewsDetail.aspx?id=13568 (accessed on February 7, 2015)
4. http://www.mccormickplace.com/about-us/about-us.php (accessed on February 7, 2015)
My First RSNA, continued from previous page
Case-Based Review & Advanced Breast Imaging Course: DIGITAL BREAST TOMOSYNTHESIS
2015
September 26-27, 2015San Diego, CA
ACR 2015 Meeting PreviewBy Murray Rebner, MD, FACR, FSBI
ACR 2015 – The Crossroads of Radiology - will take place at the Marriott Wardman Park Hotel in Washington, DC from May 17 through May 21, 2015. This upcoming inaugural meeting will be different from prior ones in that it will educate not only ACR members, but also professionals involved in all aspects of radiology. The attendees will convene to improve their clinical skills, business practices, government relations and patient care. ACR members and non-members will also leave with a better understanding of what role the College plays in these important areas. This format will be continued annually after the 2015 event. This is also the first time that the Society of Breast Imaging (SBI) has provided content for an annual ACR meeting.
The SBI portion of the program will take place from Monday, May 18 through Wednesday, May 20. There will be 4.5 hours of content, divided into three 1.5 hour blocks.
On Monday, May 18, Dr. Carol Lee will speak on preoperative magnetic resonance imaging (MRI) and supplemental screening. Dr.
Robert Smith will discuss breast cancer as a worldwide problem, and Dr. Michael Linver will lecture on the economics of breast imaging.
On Tuesday, May 19, Dr. Margarita Zuley will address the “hot topic” of digital breast tomosynthesis. The following 60 minutes will be an interactive session, dealing with the appropriate use of the new Breast Imaging Reporting and Data System (BI-RADS®) Fifth Edition. Dr. Ellen Mendelson, (ultrasound) Dr. Elizabeth Morris (MRI) and Dr. Edward Sickles (mammography) will discuss the critical changes in the atlas.
The presentations on Wednesday, May 20 include a half hour talk by Dr. Daniel Kopans on why breast cancer screening works. The final 60 minute session will be a multimodality case review given by Drs. Christopher Comstock and Linver.
The SBI hopes that the new content will be well received. I plan on attending and I hope to see you there!

www.SBI-online.org18 2015 Issue 1 SBINews
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
This year, digital breast tomosynthesis (DBT) received a great deal of attention at the Radiological Society of North America (RSNA)
annual meeting during dedicated sessions (Screening and Diagnostic) and additional papers interspersed in other modality sessions. It is both exciting and encouraging to see the spectrum of work that is being done with this new technology. The news is uniformly positive as improvements are being noted in both screening and diagnostic utilization as well as with its integration with other imaging modalities.
On Monday afternoon, 3:00-4:00 PM, a session was devoted to diagnostic tomosynthesis. A few studies compared the performance of DBT to breast magnetic resonance imaging (MRI) and ultrasound (US). Two studies, one from the United States (M. W. Yamashita, MD) and another from Italy (G. Mariscotti, MD) showed that DBT improved cancer detection over two-dimensional (2D) mammography and 2D mammography and US but did not achieve the high sensitivity of MRI. Yet 2D mammography and DBT had better specificities than MRI. A paper from the University of Pennsylvania, for which Amy Chudgar, MD, was awarded the trainee research prize, examined the utility of breast MRI in cancer diagnosed by 2D mammography compared with DBT and found that while MRI detects cancers not identified by either technique, its supplemental value after DBT is not as great as it is after 2D mammography, reflecting that some of those additional cancers are detected by DBT. Two studies from Yale presented by Madhavi Raghu, MD looked at the effect of DBT in the diagnostic setting and how the rates of Breast Imaging Reporting and Data System (BI-RADS®) final assessment categories
change over time with more definitive separation of benign and malignant lesions. DBT resulted in a larger percentage of BI-RADS® 1 and 2 assessments, fewer BI-RADS® 3 assessments, and an increase in the positive predictive value (PPV) of BI-RADS® 4 and 5 assessments. A second study of BI-RADS® 3 lesions found no malignancies in the asymmetry category, suggesting that these findings may not need follow-up. Another study from the Republic of Korea (W. H. Kim, MD, PhD) showed the continued importance of US as digital mammography (DM) and US combined had superior diagnostic performance compared to DM or DBT alone, with higher cancer detection rates, but at the cost of lower specificity.
Tuesday morning 8:30-12:00 showcased a large number of DBT-related papers in the Emerging Technologies in Breast Imaging session. One paper from Taiwan (C.-P. Chou, MD) showed similar performance of contrast-enhanced breast tomosynthesis (CEBT) and MRI for assessing mammographic abnormalities but higher sensitivity for CEBT. A study from Egypt (M. H. Helal, MD) showed that contrast-enhanced spectral mammography provides similar size assessments to pathology and better detection of multifocal cancer. A study of dosimetric properties of DBT (L. L. Fajardo, MD, MBA) reported greater than 3 mGy in the majority of exposures, encouraging retrograde synthesis of 2D mammograms to reduce radiation dose. And another study from Boston (F. Proulx, MD) examining DBT dose found a stronger correlation between dose and thickness than patient age or breast density. An interesting study from Japan (N. Uchiyama MD) discussed a novel combined three-
www.SBI-online.org
The Member Newsletter of the Society of Breast Imaging
2014 Issue 3 19
2014 RSNA Synopsis: Digital Breast TomosynthesisBy Liane E. Philpotts, MD, FSBI
April 25-28, 2015
Hilton Bonnet Creek Orlando, Florida
AC
R
Breast Imaging Symposium2 0 1 5
REGISTER TODAY!
SBINews
dimensional (3D) rotating mammogram (RM). The authors reported significantly better visualization of microcalcifications on RM than DBT, which could result in better calcification detection and improved interpretation times.
A few studies from the Tuesday session examined synthesized 2D mammograms in conjunction with DBT. One study (J. Choi, MD, Seoul) regarding T1 (small invasive) cancers reported no difference in performance of synthesized mammography and DBT versus DM and DBT. While calcification cases were not assessed, this result adds confidence that synthesized mammography with DBT can be used in practice to reduce radiation dose. An update on the Screening with Tomosynthesis or Mammography (STORM) II trial (D. Bernardi, MD) also showed that synthesized 2D mammography functioned slightly better than DM in cancer
detection and that the combination of synthesized 2D images with DBT was superior to DM plus DBT. Another study (N. Salem, MD) showed lower rates of interval cancers with the use of DBT. A study from Brown assessing architectural distortion detected on DBT (K. Damico, MD) demonstrated a 27% cancer yield, suggesting that this important mammographic finding should be carefully assessed and managed. Per Skaane, MD, PhD discussed an update of the Oslo DBT screening trial, showing higher rates of cancer detection for breast densities 2-4 (also known as B-D in the BI-RADS® 5th edition). Finally, another study from Yale (J. L. Geisel, MD) assessed the utility of tomographic spot compression views in non-calcification BI-RADS® 0 recall cases. All malignant lesions were correctly identified on the ‘routine’ CC and MLO DBT views alone, suggesting that many patients can forego additional mammographic
2014 RSNA Synopsis: Digital Breast Tomosynthesis, continued from previous page

www.SBI-online.org20 2015 Issue 1 SBINews
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
www.SBI-online.org
The Member Newsletter of the Society of Breast Imaging
SBINews 2014 Issue 3 21
2014 RSNA Synopsis: Digital Breast Tomosynthesis, continued from previous page
imaging and proceed to US for further assessment.
Wednesday morning 10:30-12:00 was devoted to tomosynthesis screening. One study (R. E. Sharpe, Jr., MD, MBA) reported that for many cases of non-calcified findings recalled from DBT screening, additional views may not be helpful. Two papers looked at recalls from DBT screening and the importance of architectural distortion. A study from Yale (M. Durand, MD) examined DBT recall rates over a three-year period and found that the incidence of architectural distortion rose significantly in the second year and then decreased, but remained slightly higher than pre-DBT levels, reflecting a persistently increased sensitivity of DBT to detecting this finding. Architectural distortion was the mammographic finding with the highest PPV for malignancy, indicating that its detection is critical. A separate study (N. Ibrahim, MD) also showed an increase in the rate of architectural distortions recalled, resulting in similar cancer detection rates but an increase in radial scar diagnoses. Another interesting study (C. M. Hakim, MD) reported that DBT technology and the availability of prior exams are independent factors in reducing recall rates. The sensitivity for cancer detection was most affected by DBT, regardless of prior exams, but the addition of prior studies improved the specificity. Another paper (A. Chudgar, MD) looking at MRI as a problem-solving tool after 2D mammography versus DBT showed that although the overall utilization for problem solving did not change, the types of lesions did change, with fewer masses and more architectural distortions in the DBT group. An analysis from the University of Pittsburgh Medical Center (UPMC) (presented by J. Koo, MD) found that cancers missed on DBT often appeared as areas of normal tissue. Interestingly, their data showed that the CC view was more helpful than the MLO view in cancer detection. A cost analysis of DBT from Yale (presented by
V. Kalra, MD) demonstrated that age, grouped by decade, was more than twice as significant as mammographic density in recall cost benefits, with greater savings in the 40-49 years age group compared to the 70 years and older group. Finally, Jules Sumkin presented data from the UPMC group showing significantly reduced recall rates for baseline DBT exams compared with 2D studies.
DBT papers interspersed in other sessions included a few studies comparing the additional cancer yield of DBT to whole breast US. These generally showed that DBT detected most cancers with a small additional yield from whole breast US. However, DBT resulted in fewer false positive biopsies. In the Quantitative Imaging session, A. J. Chu, MD from Seoul, Korea, discussed promising results for the detection of the majority of malignant calcifications with 3D computer-aided detection (CAD) for DBT. An automated volumetric density assessment tool that segments tissue from DBT images (S Pertuz, PhD from the University of Pennsylvania) reported estimations in concordance with those from digital mammography and MRI. Another study from the UK, presented in the Breast Density and Risk Assessment session (S. W. Duffy, MSc), showed that DBT significantly increased the sensitivity for cancer in women with densities >50%, while specificity was increased for all breast densities, as judged by visual assessment and quantitative methods.
The diversity of presentations discussing DBT demonstrates its benefits in all aspects of breast imaging and how it is helping radiologists to provide a superior form of breast imaging to their patients. This was an exciting RSNA meeting, and next year is sure to bring even more interesting studies as this technology takes off.
A t the 2014 annual meeting of the Radiological Society of North America (RSNA), hundreds of presentations were
made on breast magnetic resonance imaging (MRI), including refresher courses, workshops and scientific abstracts. There was so much to see and hear that my greatest challenge was deciding which session to attend. The electronic and educational exhibits had many interesting and timely breast MRI topics and subjects as well. From the scientific sessions, presentations and categorical courses, anyone attending could discover all the latest in breast MRI, how MRI may relate to personalized breast care, current screening recommendations and get a refresher on standard applications.
A scientific paper session presentation by Dr. Pertuz and co-authors embraced accurate breast density measurement estimation and its importance for cancer risk assessment. The authors reviewed bilateral digital breast tomosynthesis (DBT) images, digital mammography (DM) images and sagittal MRI scans. An algorithm was developed to segment the fibroglandular tissue and measure volumetric breast density, utilizing the DBT projection images and reconstructed slices for analysis. Volumetric breast density (VBD) estimates were made for DM images using United States Food and Drug Administration (FDA) approved software and for MRI with another automated software program. The authors concluded that estimating VBD can be highly accurate by DBT and correlates well to MRI and DM estimates.
Review and didactic presentations were given on topics such as MRI acquisition by Dr. Schnall, who described the technical elements, pulse sequences and high in-plane spatial resolution needed to perform high quality breast MRI. Many
other presentations reviewed current applications and methodology for breast MRI. Along with the didactic and refresher courses, there were presentations on exciting, new research and experimental techniques.
Several presenters described their investigations on enhancement parameters with dynamic contrast enhanced (DCE) MRI, such as the one by Dr. Moon Yang and co-authors, correlating enhancement patterns with prognostic factors and immunohistochemical subtypes of breast cancer. These authors revealed that background parenchymal enhancement (BPE) correlated significantly with epidermal growth factor receptor (EGFR) expression and that these parameters may predict prognosis and subtypes of breast cancer. Several scientific abstracts discussed the importance of pre-operative breast MRI for newly diagnosed breast cancer patients while others found no difference in outcomes by performing pre-operative MRI. On a similar note, my abstract, consisting of a retrospective review of data from Elizabeth Wende Breast Care on premenopausal women with a personal history of breast cancer, revealed recurrence rates similar to women with a strong family history of breast cancer and concluded that consideration should be given to yearly breast MRI for this subgroup of patients.
Dr. Partridge, in the Diffusion Weighted Imaging (DWI) session, presented the physical basis of DWI and the methods used to acquire diffusion weighted data. This was one of many didactic sessions for those needing a refresher or hearing about this technology for the first time and its uses for diagnosing cancer and assessing response to treatment. A presentation on 7 Tesla (T) breast MRI for pre-operative characterization of breast cancer utilizing DWI and phosphorus
2014 RSNA MRI ReviewBy Stamatia V. Destounis, MD, FACR, FSBI

www.SBI-online.org22 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 23
SAVE THE DATES!
Case-Based Review & Advanced Breast Imaging Course: DIGITAL BREAST TOMOSYNTHESIS
2016
September 17-18, 2016San Diego, CA
January 16-17, 2016Orlando, FL
spectroscopy was given in the Arie Crown Theater by Dr. Schmitz as an investigative method to stratify tumor proliferation and as a predictive marker for therapy selection.
The many unique and timely MRI topics had the common theme of addressing early detection, possible overtreatment concerns and controversies, and treatment failures for some patients versus others. The common thread in many of these very different scientific works was the large amount of effort by the scientists to identify or develop prognostic models tailored to the individual patient and their specific needs at the time of diagnosis. An abstract on detecting patterns of recurrence according to breast cancer subtype in patients treated with breast conserving therapy, presented by Dr. Min Sun Bae and co-authors, revealed that multifocal or multicentric disease was
more frequently found in human epidermal growth factor receptor 2 (HER2) positive breast cancer. They also reported that increased fibroglandular tissue on MRI was more likely to be associated with estrogen receptor (ER) positive, progesterone receptor (PR) positive tumors. Many other abstracts discussed the importance of BPE versus fibroglandular tissue with contradictory although interesting findings.
As I sat and listened to the refresher and review courses and the scientific presentations on new technology and clinical research, I was very proud to be present, in the moment, watching our peers working on the many advances in breast MRI, and appreciating the transition of MRI from a tool for early detection and diagnosis to a vehicle for improving treatment opportunities and options.
2014 RSNA MRI Review, continued from previous page 2014 RSNA Breast Ultrasound SummaryBy Paula Gordon, OBC, MD, FRCPC, FSBI
This year’s Radiological Society of North America (RSNA) breast ultrasound (US) scientific sessions covered screening and
technologies aimed at improving positive predictive value (PPV).
The excellent introductory talk by Regina Hooley in the Sunday session summarized the evolution of US for breast screening from the automated scanners trialed in the 1960s and 1970s to the ACRIN 6666 trial in 2008 and a Korean publication in 2014.
Breast density legislation in the United States began in Connecticut in 2009 and included 20 states at the time of this writing. Screening can be performed by automated units available from several vendors, or by either radiologists or sonographers using hand-held transducers. Screening US can be done at the same time as mammography or at alternating six-month intervals. Better methods of triaging Breast Imaging Reporting and Data System (BI-RADS®) 3 lesions, or down-staging 4A lesions would be helpful. If digital breast tomosynthesis (DBT) screening becomes the standard-of-care, we can expect the yield of screening US to decrease, as shown in the presentations by Vera Aguillar and Jin Chung.
Jean Weigert presented the 3rd and 4th year updates regarding the Connecticut experience showing new cancer detection rates remained stable at three per 1000 as in the first two years. The PPV increased from 8.1% in year 3 to 16.1% in year 4.
Islamiat Ego-Osuala presented her group’s experience using US
screening in the first 15 months, finding only two cancers per thousand; a much lower rate than previously reported.
Kyung Jin Nam used US-detected cancers as a starting point to compare full-field digital mammography (FFDM) to DBT. That group retrospectively reviewed 41 cancers detected on screening US. In these cases, mammography was prospectively read as negative. As would be expected, significantly more cancers were visible with DBT compared to FFDM.
Sung Eun Song presented an analysis of cancers missed on screening US. In one third of cases, visible findings were seen at the site of the cancer diagnosis, and of these, about one half were actionable and one half were not. The most frequent reasons for misdiagnosis were misinterpretation (41%), benign appearance (30%), small size < 5 mm (9%), or multiple distracting lesions (8%).
Find thepeople and careers driving innovation.Visit the Society of Breast Imaging
Career Center, where we’re bringing
professionals and employers
together in the radiology community.
Recruit top talent, find jobs and get
connected.
Visit theSBI Career Center
today!
sbi-online.org
Since 1985

www.SBI-online.org24 2015 Issue 1 SBINews
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
www.SBI-online.org
The Member Newsletter of the Society of Breast Imaging
SBINews 2014 Issue 3 25
2014 RSNA Breast Ultrasound Summary, continued from previous page 2014 RSNA Breast Density Legislation Update, continued from previous pageEllen Mendelson’s presentation compared hand-held to automated breast US and showed discrepancies in the BI-RADS® assessment category in 18% of cases, but no cancers were miscast as benign. This emphasizes the need for familiarity with artifacts on automated examinations.
Maha Helal’s group compared FFDM, DBT, contrast-enhanced mammography and three-dimensional (3D) US for staging. They found DBT and US best at size determination, but contrast-enhanced mammography best at diagnosing multifocality.
An interesting study by Neb Duric on US tomography used quantitative parameters of sound speed and attenuation to characterize lesions, and showed the potential to increase the PPV of US compared to BI-RADS® criteria.
Betty Tuong presented a low cancer yield (10/1860, 0.5%), for US to evaluate screening mammography-detected findings when spot views were negative.
Adrienne Newburg’s group looked at US of cases where magnetic resonance imaging (MRI) showed non-mass enhancement (NME), and found that an US correlate was seen in only 23% of cases, of which 18% showed malignancy on biopsy. In the 77% of cases where there was no US correlate, MRI-guided biopsy yielded cancer in 12% of the cases, indicating that a negative US should not preclude biopsy of suspicious NME lesions.
Elastography papers showed promise in both upgrading and downgrading lesions.
Ellen Sun discussed the use of shear wave elastography to demonstrate stiffness in masses and surrounding tissue, which should prompt biopsy of masses that might otherwise have been assessed as probably benign or low-suspicion. Alice Carboni’s presentation of the use of strain ratio in elastography showed promise in downgrading BI-RADS® 3 and 4 lesions.
In summary, many interesting presentations reinforced current uses of US in breast, and show continuing promise for new applications.
Breast density and breast density notification laws remained a topic of interest at the 2014 meeting of the Radiological Society of North
America (RSNA). The pinnacle of the density legislation discussions took place on Wednesday morning when Dr. Barbara Monsees, the Ronald and Hanna Evens Professor of Women’s Health at Washington University in St. Louis and Dr. Stephen Feig, professor of clinical radiology and radiological sciences from the University of California, Irvine led the lively and well attended
Controversy Session: Breast Density Notification Legislation: Pros and Cons (1).
Drs. Monsees and Feig discussed the classic definition of breast parenchymal density quantification by quartiles and the newer subjective determinations per the Breast Imaging Reporting and Data System (BI-RADS®) 5th edition. They discussed breast density as an independent risk factor for breast cancer and its “masking” effect that decreases the sensitivity of
2014 RSNA Breast Density Legislation UpdateBy Shadi A. Shakeri, MD
screening mammography.
Dr. Monsees summarized the relevant studies, including the Digital Mammographic Imaging Screening Trial (DMIST), describing the percentages of the population with different grades of breast density and the associated relative risk (RR). Considering the RRs of the four breast density categories and their frequency of occurrence in the population, Dr. Feig reminded us that while women with extremely dense breasts have a RR 4 times that of women with fatty breasts, the RR of extremely dense breasts compared to average density is only 1.6. Women with heterogeneously dense breasts have a RR of only 1.2. This places density at the lower cusp of risk factors compared to positive family history, personal history of breast cancer or benign proliferative lesions (atypical ductal and lobular hyperplasias), with a RR ranging from 2.0 to 4.0.
Dr. Monsees reviewed data from studies of supplemental screening with ultrasound (US) showing an incremental increase in cancer detection. She emphasized the importance of data from American College of Radiology Imaging Network (ACRIN) 6666 trial regarding additional cancers detected by magnetic resonance imaging (MRI) after three rounds of negative screening mammography and ultrasound, possibly eliminating the need for screening ultrasound if MRI is chosen as the supplemental study (2). Referring to data presented earlier in the week by Dr. Christiane Kuhl from Germany on fast breast MRI sequences, Dr. Monsees suggested that MRI may be the better choice if supplemental screening is needed for women with dense breasts, stating that “US works, MRI works better.”
In support of breast density notification, Dr. Monsees made the argument that women deserve to know the limitations of the tests they undergo. More importantly, patients should be informed of their breast density to facilitate discussions with
their physicians, stating that many patients are unaware of their family history and other risk factors. With a federal bill under consideration in the House of Representatives and another in the Senate, our patients and colleagues are likely to request further information on this topic. Adding that our medical colleagues are likely struggling with how to proceed, Dr. Monsees advised the audience to seek and share the information regarding breast density in American College of Radiology (ACR) brochures or websites from the following groups: California Breast Density Interest Group (CBDIG), The New England Comparative Effectiveness Public Advisory Council (CEPAC) and the California Technology Assessment Forum (CTAF). She also pointed out that density alone is not the only factor informing the decision to have extra screening and that not every woman with dense breasts may need supplemental screening. She re-emphasized that any federal bill should include research funding to explore the complexities of this issue.
In addition to discussing the limitations of density determination due to inter- and intra-observer variability, Dr. Feig made it clear that we do not have enough evidence to screen anyone less frequently. He added that personalized screening to radiologists means annual screening exams for every woman starting at age 40 years, supplemented by MRI for high-risk patients, or possibly US for dense breasts. However, to others it means screening less frequently than annually because younger women are presumed to have lower risk. “For these anti-screening advocates,” he added, “personalized screening is a euphemism for health care rationing.”
Dr. Feig went on to summarize preliminary data on automated breast ultrasound and digital breast tomosynthesis for supplemental screening in women with dense breasts. He reiterated some of the main concerns raised by the ACR on reporting

www.SBI-online.org26 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 27
R adioactive seed localization (RSL), introducing an Iodine (I)-125 seed by mammographic or ultrasound guidance into a lesion that is to be
excised – as opposed to wire localization, is becoming increasingly popular. As experience grows and more surgeons, radiologists and pathologists have trained in facilities using RSL, there will be an increasing number of facilities implementing RSL programs.
Initiating a RSL program can appear to be a daunting task. There are many who need to cooperate; having a point person and champions among the key stake holders facilitates the process. Once properly implemented, the benefits are apparent and the issues are few. Pragmatic benefits include uncoupling of the radiology localization and the surgery schedules. Gone are the sometimes irate phone calls from the operating suite looking for the localization patient. Administration appreciates the lack of operating room downtime. Within the radiology department, many fewer episodes of syncope can be expected as typically the procedure is done days prior to surgery; the patients are not fasting and not nearly as anxious as they might be on the day of the operation. Some report fewer positive margins and, therefore, less return trips to the operating room, resulting in improved, cost-effective care and happier patients (1-3).
The potential problems associated with RSL are many, but all can be addressed in an appropriate manner. The surgeons and pathologists must agree to change some of their techniques. Scissors and suction, for example, cannot be used until the seed is isolated and safe from being transected. If a surgeon, for example, will not change techniques, his or her patients cannot participate in the RSL program
and must have wire localizations. Concerns regarding radiation exposure have been shown to be unfounded (4). Yearly radiation safety education of the entire staff involved in the RSL program is necessary.
The largest obstacle to a RSL program is the set up. The radioactive nature of the seed mandates that the radiation safety officer assume a key role in the program. The seeds must be ordered, accepted, stored, dispensed, retrieved and disposed of in accordance with Nuclear Regulatory Commission (NRC) or local regulations as appropriate. Loss of a seed is a real concern. There are many pragmatic steps that one can take to limit the possibility of seed loss. These include patient selection. If, for example, a patient has social, medical, or insurance related challenges that place her at a higher risk of not returning for a scheduled surgery, it is wise not to place a seed until the day of the operation or revert to wire localization. Despite all precautions , a patient may not have surgery as planned. The patient might eat or be in an accident or become ill and spend the next few weeks dealing with other medical issues and not be able to have the planned breast surgery. Procedures must be in place to track the patient and document follow-up.
Implanting a radioactive seed is a simple procedure, analogous to placing a tissue marker. Theoretically, if one used an inferior approach for placement under mammographic guidance, the seed could fall out through the track and, therefore, the inferior approach is not used. Whether the seed is placed under mammographic or ultrasound guidance, the sterile tray is kept intact with no personnel leaving the room until the seed is documented in appropriate position by
Radioactive Seed Localization: Experiences and Concerns By Laurie Margolies, MD, FACR
2014 RSNA Breast Density Legislation Update, continued from previous page
breast density to physicians and patients. Namely, that this may create anxiety about risk, and also create confusion with year-to-year reporting variability of breast density, which could be interpreted by some as unreliability. A lack of reimbursement, and not having enough technologists and radiologists to perform and interpret the exams were some of the other concerns Dr. Feig raised regarding breast density legislation. He also added that primary care providers have insufficient time and knowledge to discuss these complex issues with patients.
Potential positive points that Dr. Feig mentioned in support of breast density legislation were that more cancers would be detected earlier and women will be encouraged to personally consider the benefits and risks of supplementary screening. Legislation may promote future reimbursement for screening ultrasound and encourage advancement of new technology.
Apropos the issues raised by Drs. Monsees and Feig were several interesting studies presented at the Thursday morning session on Breast Density and Risk Assessment. Regarding the need for primary care provider education, Dr. Kathleen Khong from the University of California, Davis reported that 10 months after the state breast density law went into effect, 49% of 174 physicians surveyed from a single institution primary care network were not aware of the breast density legislation. Moreover, 5% of the surveyed physicians reported being “completely comfortable” answering patients’ questions about breast density (3).
Also in the Thursday morning session, vis-à-vis Dr. Feig’s comments about personalized screening, Dr. Elissa Price from University of California, San Francisco reported that of the 194 cases of breast
cancer diagnosed in 40-49 year old women over a 15 year period, 78% of the patients had neither very strong family history nor extremely dense breasts. The results of this retrospective study suggest that using a risk-based approach to screening mammography could miss up to 75% of screen-detected cancers in 40-49 year old women (4).
There are now at least 20 states with breast density notification legislation. With other states working on similar laws and a federal bill under consideration, there is a need for greater radiologist involvement in breast density research and education of our patients and colleagues about this very complex issue.
REFERENCES 1. Comstock C, Monsees B, Feig S. Controversy session: breast density notification legislation: pros and cons. Radiological Society of North America 2014 Scientific Assembly and Annual Meeting, November 30 - December 5, 2014, Chicago IL. rsna2014.rsna.org/program/details/?emID=14002732 Accessed January 8, 2015
2. Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 2012;307:1394-1404.
3. Khong K, Hargreaves J, Aminololama-Shakeri S, Lindfors K. Impact of state breast density legislation on primary care physicians. Radiological Society of North America 2014 Scientific Assembly and Annual Meeting, November 30 – December 5, 2014, Chicago IL. rsna2014.rsna.org/program/details/?emID=14008249 Accessed January 12, 2015
4. Price E, Keedy A, Gidwaney R, Sickles E, Joe B. The potential impact of risk-based screening mammography in women age 40-49 years. Radiological Society of North America 2014 Scientific Assembly and Annual Meeting, November 30 – December 5, 2014, Chicago IL. rsna2014.rsna.org/program/details/?emID=14004920 Accessed January 12, 2015

www.SBI-online.org28 2015 Issue 1 SBINews www.SBI-online.org
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
The Member Newsletter of the Society of Breast ImagingClick on this bar to return to Table of Contents
SBINews 2015 Issue 1 29
Radiation-Induced Breast Cancer Risks, continued from previous page
mammography or by Geiger counter. Specimen radiographs are obtained to document that the entire seed has been retrieved. In the unlikely event that the seed is not in the initial specimen, it must be located either within the patient or within the room. Seeds cannot be repositioned. Once deployed, the seed must be retrieved. This is rarely an issue because the seeds do not appear to migrate. If, however, there is a large hematoma or if the seed lies in a capacious tract, it could be malpositioned and require more extensive surgery than anticipated.
As with wires, pre-loaded seeds can be ordered in different lengths. Most lesions can be reached with a 7 cm needle, but if a longer or a shorter needle is necessary it can be procured. We have elected to only stock one size and special order in the rare case that another size is needed. This implies and mandates that we review all cases ahead of time before the seed is dispensed from nuclear medicine to the breast imaging section. From the patient’s perspective, the most serious risk is that of seed rupture (i.e., it being cut while in the patient), which would require that the patient be given iodine to saturate the thyroid gland.
Cost of the radioactive seeds compared to localization wires is a potential barrier to adoption. A recent analysis has shown that the overall cost to a healthcare system is decreased when RSL is adopted,
but in a fee for service environment, the cost of RSL is greater (5).
RSL is not appropriate for all facilities. If there is not a sufficient volume of cases to warrant the time and the cost of implementing and maintaining a RSL program, wire localization remains a very safe and proven method. However, for larger programs with higher volumes of cases, the benefits are substantial and lead to better patient experiences.
REFERENCES 1. Gray RJ, Pockaj BA, Karstaedt PJ, Roarke MC. Radioactive seed localization of nonpalpable breast lesions is better than wire localization. Am J Surg 2004;188:377-380.
2. Hughes JH, Mason MC, Gray RJ, et al. A multi-site validation trial of radioactive seed localization as an alternative to wire localization. Breast J 2008;14:153-157.
3. Jakub JW, Gray RJ, Degnim AC, Boughey JC, Gardner M, Cox CE. Current status of radioactive seed for localization of non palpable breast lesions. Am J Surg 2010;199:522-528.
4. Pavlicek W, Walton HA, Karstaedt PJ, Gray RJ. Radiation safety with use of I-125 seeds for localization of nonpalpable breast lesions. Acad Radiol 2006;13:909-915.
5. Loving VA, Edwards DB, Roche KT, et al. Monte Carlo simulation to analyze the cost-benefit of radioactive seed localization versus wire localization for breast-conserving surgery in fee-for-service health care systems compared with accountable care organizations. AJR Am J Roentgenol 2014;202:1383-1388.
SBI/ACR Breast Imaging Symposium PreviewBy Yasmeen Fields, CAE
T he Society of Breast Imaging (SBI)/American College of Radiology (ACR) Breast Imaging Symposium promises to
give attendees an experience like never before. Under the leadership of Dr. Elizabeth Morris, the SBI vice president, and with the assistance of the 2015 Symposium Planning Committee, we are pleased to bring you a robust program. Topics include: the biology of breast cancer, population-based screening and beyond, overdiagnosis, breast density legislation, and an update on emerging technologies. For the first time, the program is offering three scientific sessions where original research related to breast imaging will be presented. Two research prizes, consisting of a plaque and $1,000, will be awarded based on scientific merit, one to a medical student or resident and one to a fellow.
For the first time the SBI is providing attendees the opportunity to participate in the United Kingdom’s national PERFORMS mammography self-assessment program. Participants will read sets of recent challenging screening cases on clinical workstations and report their decisions about each case into the PERFORMS reporting application. At the conclusion of the meeting, participants will receive a report comparing how they scored against their peers. PERFORMS sessions will run concurrently with the plenary and breakout sessions throughout the first three
days of the meeting. Class size is very limited and on a first-come basis. There is no additional fee to participate but pre-registration is required in order to attend this session. Sign up early!
On Monday, April 27, 2015, from 12:30 – 1:20 pm in the general session room, the SBI invites you to an award-winning play, “The Actual Dance”, written and performed by Sam Simon. The performance is a moving account of the experiences of a husband dealing with his beloved wife’s diagnosis and treatment of breast cancer. Don’t miss this unique and special performance that is sure to warm your heart.
Finally, we cannot forget our past. In honor of the SBI’s 30thAnniversary, and with the help of Dr. Marc Homer, Dr. Edward Sickles, Dr. Bonnie Joe, and Dr. Murray Rebner, we have special presentations depicting the rich history of breast imaging through technological advances in the field and notable events throughout the history of the society.
I sincerely hope you will join us for the first ever SBI/ACR Breast Imaging Symposium on April 25 – 28, 2015 at the Hilton Bonnet Creek in Orlando, Florida. To view the entire program, please go to www.sbi-online.org for more information.