Embed Size (px)
Citation preview

Vasanti Malik, ScD Research Scientist
Department of Nutrition
Harvard School of Public Health
Saturated Fatty Acids and Risk of
CHD: Modulation by Replacement
Nutrients
Cardiovascular Disease Prevention International Symposium,
Baptist Health South Florida
Thursday February 19, 2015
No conflicts of interest or disclosures
Conclusion from Chowdhury Abstract
“Current evidence does not clearly
support cardiovascular guidelines that
encourage high consumption of polyunsaturated fatty acids and low
consumption of total saturated fats.”
(Chowdhury R. et al. Ann Intern Med 2014:160:398-406)
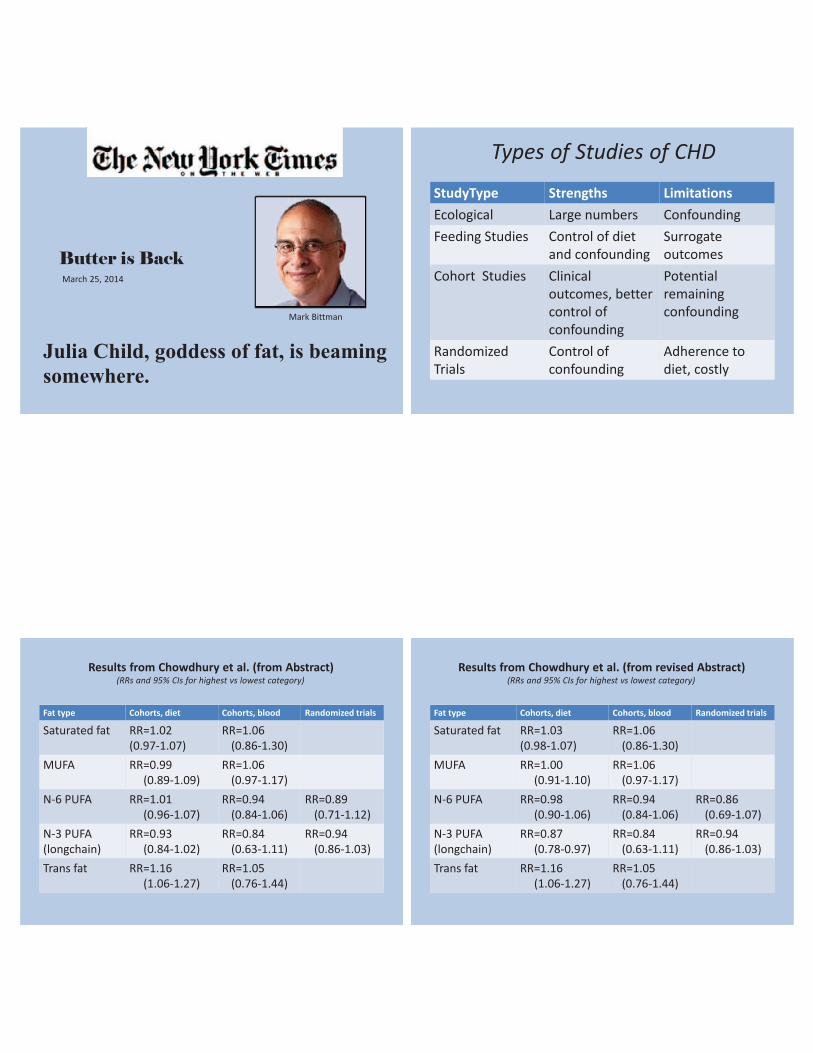
Mark Bittman
Butter is Back
March 25, 2014
Julia Child, goddess of fat, is beaming
somewhere.
StudyType Strengths Limitations
Ecological Large numbers Confounding
Feeding Studies Control of diet
and confounding
Surrogate
outcomes
Cohort Studies Clinical
outcomes, better
control of
confounding
Potential
remaining
confounding
Randomized
Trials
Control of
confounding
Adherence to
diet, costly
Types of Studies of CHD
Fat type Cohorts, diet Cohorts, blood Randomized trials
Saturated fat RR=1.02
(0.97-1.07)
RR=1.06
(0.86-1.30)
MUFA RR=0.99
(0.89-1.09)
RR=1.06
(0.97-1.17)
N-6 PUFA RR=1.01
(0.96-1.07)
RR=0.94
(0.84-1.06)
RR=0.89
(0.71-1.12)
N-3 PUFA
(longchain)
RR=0.93
(0.84-1.02)
RR=0.84
(0.63-1.11)
RR=0.94
(0.86-1.03)
Trans fat RR=1.16
(1.06-1.27)
RR=1.05
(0.76-1.44)
Results from Chowdhury et al. (from Abstract) (RRs and 95% CIs for highest vs lowest category)
Fat type Cohorts, diet Cohorts, blood Randomized trials
Saturated fat RR=1.03
(0.98-1.07)
RR=1.06
(0.86-1.30)
MUFA RR=1.00
(0.91-1.10)
RR=1.06
(0.97-1.17)
N-6 PUFA RR=0.98
(0.90-1.06)
RR=0.94
(0.84-1.06)
RR=0.86
(0.69-1.07)
N-3 PUFA
(longchain)
RR=0.87
(0.78-0.97)
RR=0.84
(0.63-1.11)
RR=0.94
(0.86-1.03)
Trans fat RR=1.16
(1.06-1.27)
RR=1.05
(0.76-1.44)
Results from Chowdhury et al. (from revised Abstract) (RRs and 95% CIs for highest vs lowest category)
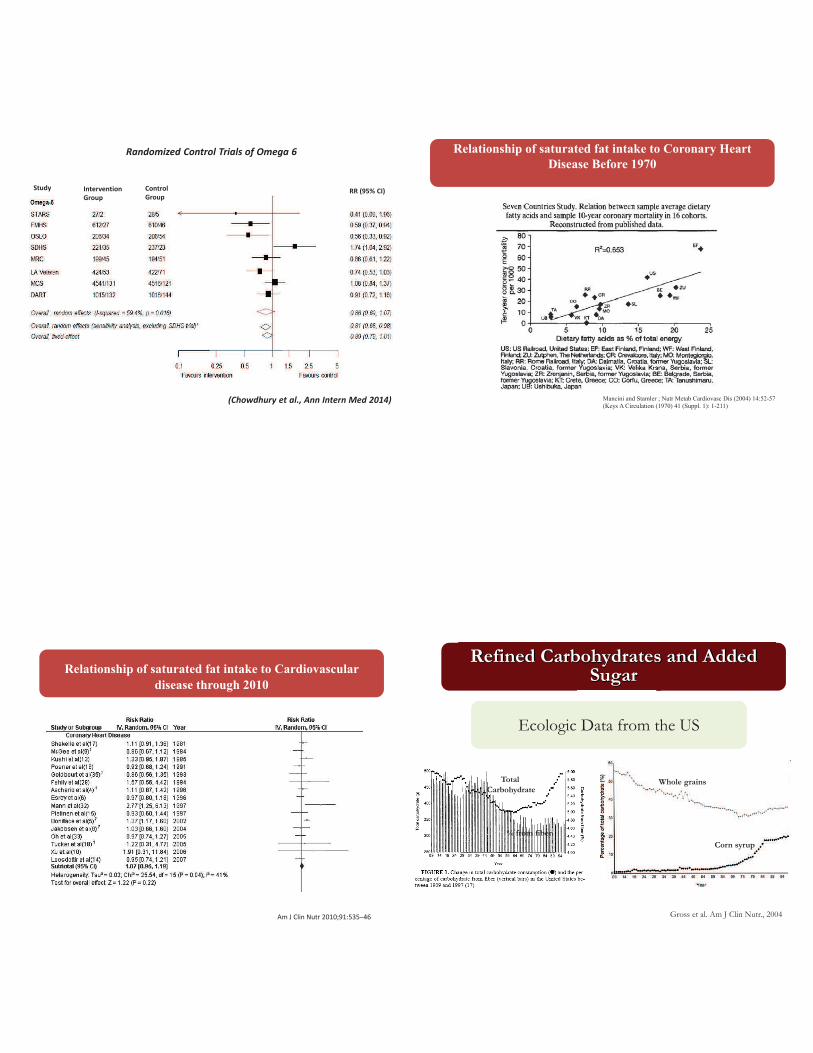
Randomized Control Trials of Omega 6
Study Intervention
Group
Control
Group RR (95% CI)
(Chowdhury et al., Ann Intern Med 2014)
Relationship of saturated fat intake to Coronary Heart
Disease Before 1970
Mancini and Stamler ; Nutr Metab Cardiovasc Dis (2004) 14:52-57
(Keys A Circulation (1970) 41 (Suppl. 1): 1-211)
Relationship of saturated fat intake to Cardiovascular
disease through 2010
Am J Clin Nutr 2010;91:535–46
HFCS
Whole grains
Whole grains
Corn syrup
% from fiber
Total
Carbohydrate
Gross et al. Am J Clin Nutr., 2004
Refined Carbohydrates and Added Sugar
Ecologic Data from the US
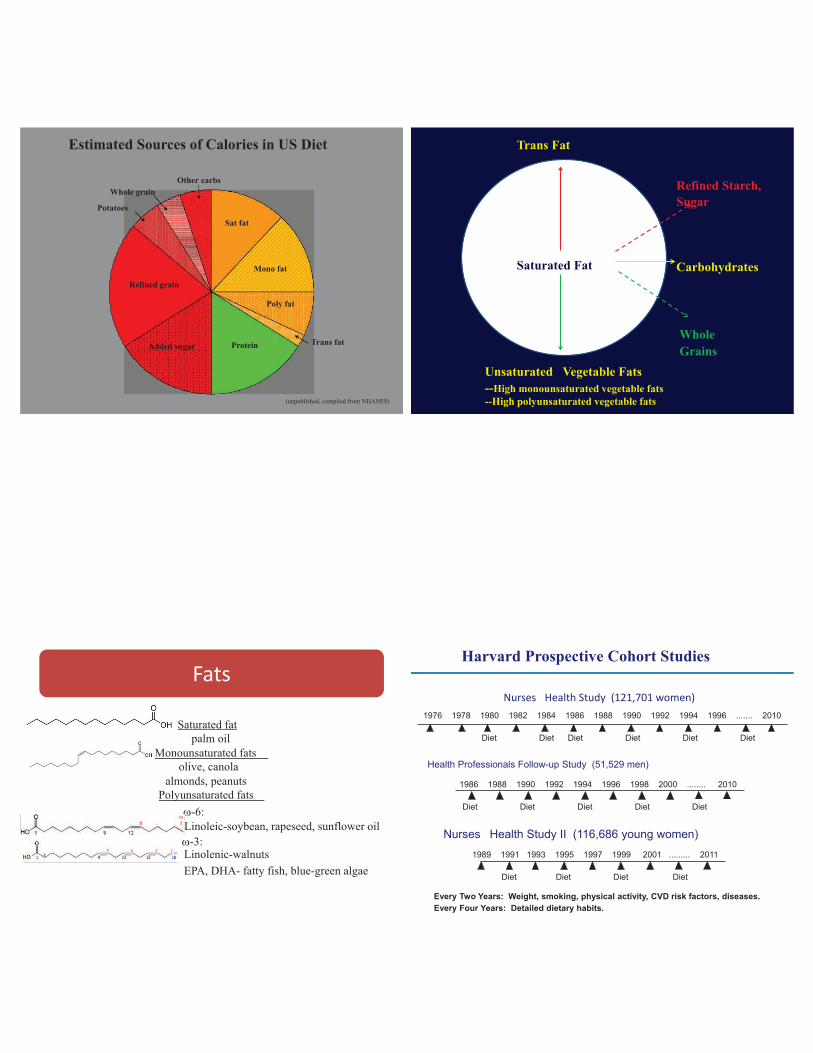
Mono fat
Poly fat
Trans fat Protein
Estimated Sources of Calories in US Diet Other carbs
Whole grain Potatoes Sat fat
Refined grain
Added sugar
(unpublished, compiled from NHANES)
Trans Fat
Saturated Fat
Unsaturated Vegetable Fats
--High monounsaturated vegetable fats
--High polyunsaturated vegetable fats
Refined Starch,
Sugar
Carbohydrates
Whole
Grains
Saturated fat
palm oil
Monounsaturated fats
olive, canola
almonds, peanuts
Polyunsaturated fats
w-6:
w-3: Linolenic-walnuts EPA, DHA- fatty fish, blue-green algae
Fats
Linoleic-soybean, rapeseed, sunflower oil
Nurses Health Study (121,701 women)
Health Professionals Follow-up Study (51,529 men)
Nurses Health Study II (116,686 young women)
1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 ....... 2010
Diet
Every Two Years: Weight, smoking, physical activity, CVD risk factors, diseases.
Every Four Years: Detailed dietary habits.
Diet Diet Diet Diet Diet
1986 1988 1990 1992 1994 1996 1998 2000 ........ 2010
Diet Diet Diet Diet
1989 1991 1993 1995 1997 1999 2001 ......... 2011
Diet Diet Diet
Diet
Diet
Harvard Prospective Cohort Studies

% C
ha
ng
e i
n C
HD
20
0 -20 -40
1%E 2%E 3%E 4%E 5%E
Sat
Mono Poly
Hu FB, et al. N Engl J Med 1997;337:1491-9
Type of Dietary Fat and Risk of Coronary Heart Disease
The Nurses' Health Study
14-Year Follow-up 100
Trans 80 60 40
-80 -60 -40 -20 0 20 40 60 80
Nurses’ Health Study
Dietary Fats and Risk of CHD Sat -->Carbo (5%E) Mono -->Carbo (5%E) Poly --> Carbo (5%E) Sat--> Mono (5%E) Sat--> Poly (5%E) Sat-->Unsat (5%E) Trans--> Mono (2%E) Trans --> Poly (2%E) Trans --> Unsat (2%E)
Change in CHD Risk (%)
Hu FB, et al. N Engl J Med 1997;337:1491-9
Coronary events per 5 E% increments: Pooled analysis of 11 cohorts
The model included intake of MUFA, PUFA, trans-fatty acids, CHs, protein expressed as percentage, TEI,
smoking, BMI, physical activity, highest attained educational level, alcohol intake, history of
hypertension, and energy-adjusted quintiles of fiber intake (g/d) and cholesterol intake (mg/d)
Am J Clin Nutr 2009;89:1425–32
Meta-analysis of RCTs evaluating effects of increasing PUFA consumption in place of SFA and occurrence of CHD events
PLoS Med 2010:7(3): e1000252. doi:10.1371

Ha
zard
Ra
tio
fo
r m
yo
card
ial
infa
rcti
on
1.08
1.64 1.33
0.6
0.8
1
1.2
1.6 1.4
Low-GI High-GI Medium-GI
Tertile of Glycemic Index
1.21
0.98
0.80
1.07
0.88
0.72
HR=1
Am J Clin Nutr 2010;91:1764–68
Substitution effect (5% of energy from carbohydrates for
saturated fatty acids differs by Glycemic Index
Danish prospective cohort study of Diet, Cancer and Health
Hazard ratios for CHD by intake of fatty acids and carbohydrates of
different quality as a percentage of total energy intake: Pooled results from
the NHS and HPFS
Unpublished
Two-to-4-year changes in percentage of energy intake from different fatty
acids and carbohydrate sources according to deciles of changes in saturated
fat as a percentage of energy intake: Pooled results from the NHS and HPFS
Unpublished
Multivariable hazard ratios for CHD with isocaloric (% of energy)
substitution of Saturated fat for other fats and different quality
carbohydrates: Pooled results from the NHS and HPFS
Unpublished
• A focus of dietary recommendations for CVD prevention and treatment has been a
reduction in saturated fat intake, primarily as a means of lowering LDL- cholesterol.
• The evidence that supports a reduction in saturated fat intake must be evaluated in the
context of replacement by other macronutrients.
• Based on prospective studies, replacement of saturated fat with carbohydrate is unlikely
to have an important effect on risk of CHD, but this depends on type of carbohydrate.
• Based on prospective studies and few RCTs, replacement of saturated fat with PUFA,
including a mix of N-6 and N-3 PUFA, will reduce risk of CHD.
• Data from prospective studies support an adverse effect of trans fat on
risk of CHD, which is consistent with feeding studies with intermediate endpoints.
• Findings for MUFA are complicated because main sources have been animal fats and
partially hydrogenated oils in the populations studied. Results of RCTs involving canola and
olive oil suggest likely benefits.
Conclusions
Acknowledgements:
Walter Willett
David Jenkins
Frank Hu
Yanping Li
Thank You























![[LEC_OLESON] CHD](https://img.pdfslide.us/doc/110x75/577d2e911a28ab4e1eaf66e8/lecoleson-chd.jpg)


