Embed Size (px)
Citation preview
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
COMMUNITY HEALTH DEVELOPMENT
Concept of Health Promotion/Disease Prevention
A. HEALTH PROMOTION/DISEASE PREVENTION
Ottawa Charter for Health Promotionv created through the organization of International Conference on Health Promotion in 1986
by the World Health Organization (WHO), Health and Welfare Canada, and the Canadian Public Health Association.
v adopted by 212 participants from 318 countriesv remains to be the guiding principle in health promotion efforts currently despite
various charters have been issued on health promotion
Health Promotionv The term was first used in 1945 when Henry E. Sigerist, the great medical historian,
defined the four major tasks of medicine [(1.) the promotion of health, (2.) the prevention of illness, (3.) the restoration of the sick and (4) rehabilitation]
v “the process of enabling people to increase control over and to improve their health” (Ottawa Charter)
v activities that, by accentuating the positive, assist the person to develop those resources that will maintain and enhance well-being and improve the quality of life.
v activities that a person does for himself in the absence of symptoms in an attempt to remain healthy
v any endeavour directed at enhancing the quality of health and well-being of individuals, families, groups, communities and nations through strategies involving supportive environments, coordination of resources, and respect for personal choice and values
Disease Preventionv activities designed to protect patients or other members of the public from actual
or potential health threats and their harmful consequences.
Action Areas recommended by the Charter to operationalize the concept of health promotion:
1. Reorient Health Services2. Develop Personal Skills3. Build Healthy Public Policy 4. Create Supportive Environments5. Strengthen Community Action
Principles of Health Promotion cited by WHO:1. Health promotion involves the population as a whole in the context of their everyday
life.2. Health promotion is directed towards action on the determinants of health.3. Health promotion combines diverse but complementary methods or approaches.4. Health promotion aims particularly at effective and concrete public participation.5. Health promotion is primarily a societal and political venture and not a medical service.
Community Health Nursing by Caesar G. Balatero, RN | 1
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
------------------ SSSSS ------------------
B. HEALTH AS A MULTIFACTORIAL PHENOMENON
Healthv “a state of complete physical, mental and social well-being, and not merely the
absence of disease or infirmity.” (WHO, 1947)
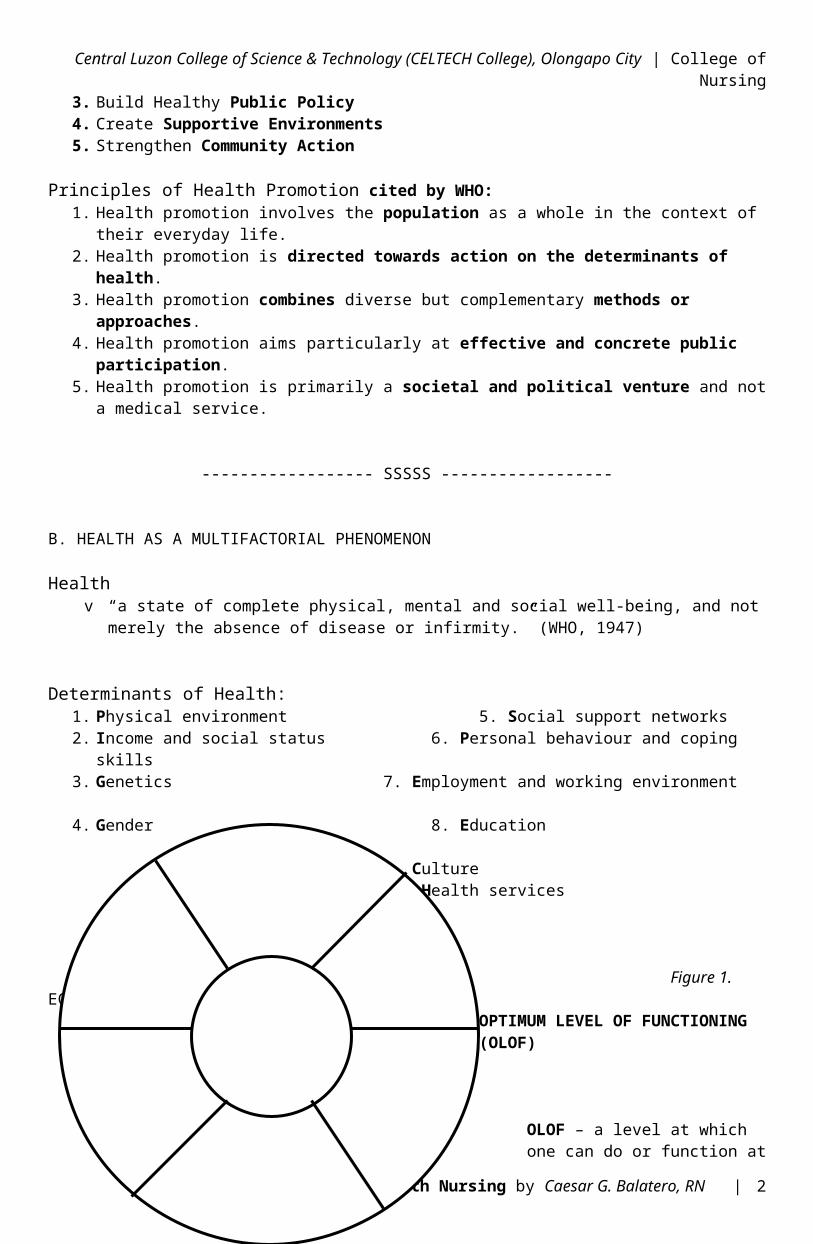
Determinants of Health:1. Physical environment 5. Social support networks2. Income and social status 6. Personal behaviour and coping skills3. Genetics 7. Employment and working environment4. Gender 8. Education
9. Culture10. Health services
Figure 1. ECOSYSTEM INFLUENCES ON
OPTIMUM LEVEL OF FUNCTIONING
(OLOF)
OLOF – a level at which one can do or function at his best out of a number of possible options and outcomes
------------------ SSSSS ------------------
C. LEVELS OF PREVENTION
LEVEL DEFINITION EXAMPLES
1. Primary Prevention specific protection for diseases improving general well-being
maintenance of diet & body weight, safe sex, cessation of
Community Health Nursing by Caesar G. Balatero, RN | 2
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
prevention or delay of the actual occurrence of a specific illness or disease
smoking, limiting alcohol intake, immunization, handwashing, fluoride application
2. Secondary Prevention early detection/diagnosis (case
finding and screening) use of referral services early treatment of disease
BSE; TB screening; newborn screening; cancer screening; genetic counselling
3. Tertiary Prevention prevention of complications rehabilitation after the disease
vocational training, physical therapy, occupational therapy, speech therapy, chronic pain clinics, remedial reading
------------------ SSSSS ------------------
D. THEORIES/MODEL OF HEALTH PROMOTION
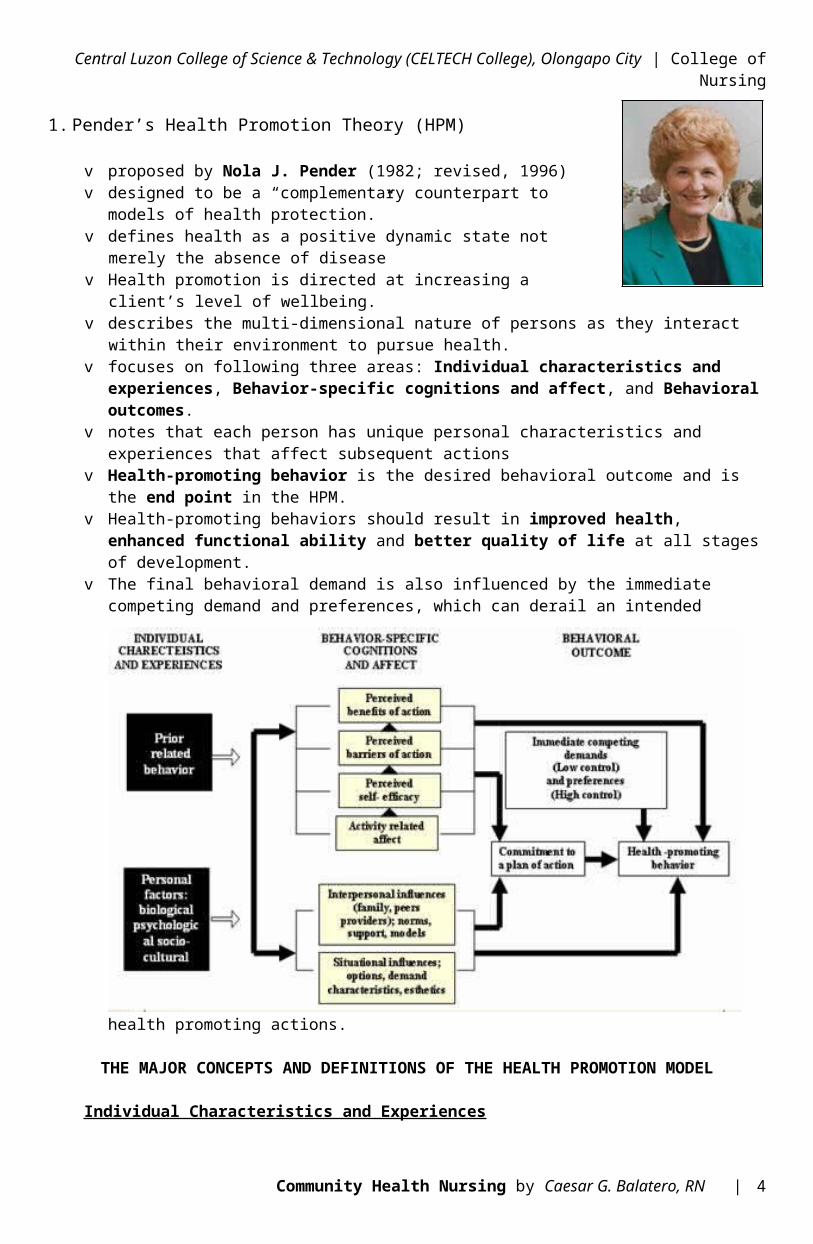
1. Pender’s Health Promotion Theory (HPM)
v proposed by Nola J. Pender (1982; revised, 1996) v designed to be a “complementary counterpart to models of
health protection.”v defines health as a positive dynamic state not merely the
absence of diseasev Health promotion is directed at increasing a client’s level of
wellbeing.v describes the multi-dimensional nature of persons as they
interact within their environment to pursue health.v focuses on following three areas: Individual characteristics and experiences, Behavior-specific
cognitions and affect, and Behavioral outcomes.v notes that each person has unique personal characteristics and experiences that
affect subsequent actionsv Health-promoting behavior is the desired behavioral outcome and is the end point in
the HPM.v Health-promoting behaviors should result in improved health, enhanced functional ability
and better quality of life at all stages of development.v The final behavioral demand is also influenced by the immediate competing
demand and preferences, which can derail an intended health promoting actions.
Community Health Nursing by Caesar G. Balatero, RN | 3
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
THE MAJOR CONCEPTS AND DEFINITIONS OF THE HEALTH PROMOTION MODEL
Individual Characteristics and Experiences
PRIOR RELATED BEHAVIOR – Frequency of the similar behavior in the past. Direct and indirect effects on the likelihood of engaging in health-promoting behaviors.
PERSONAL FACTORS – Personal factors categorized as biological, psychological and socio-cultural. These factors are predictive of a given behavior and shaped by the nature of the target behavior being considered.
Personal biological factors – Include variable such as age, gender, body mass index, pubertal status, aerobic capacity, strength, agility, or balance.
Personal psychological factors – Include variables such as self-esteem, self-motivation personal competence, perceived health status and definition of health.
Personal socio-cultural factors - Include variables such as race ethnicity, acculturation, education and socioeconomic status.
Behavior-Specific Cognition and Affect
PERCEIVED BENEFITS OF ACTION – Anticipated positive outcomes that will occur from health behavior.
PERCEIVED BARRIERS TO ACTION – Anticipated, imagined or real blocks and personal costs of understanding a given behavior.
PERCEIVED SELF-EFFICACY – Judgment of personal capability to organize and execute a health-promoting behavior. Perceived self-efficacy influences perceived barriers to action so higher efficacy result in lowered perceptions of barriers to the performance of the behavior.
ACTIVITY-RELATED AFFECT– Subjective positive or negative feeling that occur before, during and following behavior based on the stimulus properties of the behavior itself. Activity-related affect influences perceived self-efficacy, which means the more positive the subjective feeling, the greater the feeling of efficacy. In turn, increased feelings of efficacy can generate further positive affect.
INTERPERSONAL INFLUENCES – Cognition concerning behaviors, beliefs, or attitudes of the others. Interpersonal influences include: norms (expectations of significant others), social support (instrumental and emotional encouragement) and modeling (vicarious learning through observing others engaged in a particular behavior). Primary sources of interpersonal influences are families, peers, and healthcare providers.
SITUATIONAL INFLUENCES – Personal perceptions and cognitions of any given situation or context that can facilitate or impede behavior. Include perceptions of options available, demand characteristics and aesthetic features of the environment in which given health promoting is proposed to take place. Situational influences may have direct or indirect influences on health behavior.
Community Health Nursing by Caesar G. Balatero, RN | 4
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
Behavioral Outcome
COMMITMENT TO PLAN OF ACTION – The concept of intention and identification of a planned strategy leads to implementation of health behavior.
IMMEDIATE COMPETING DEMANDS AND PREFERENCES – Competing demands are those alternative behavior over which individuals have low control because there are environmental contingencies such as work or family care responsibilities. Competing preferences are alternative behavior over which individuals exert relatively high control, such as choice of ice cream or apple for a snack
HEALTH-PROMOTING BEHAVIOR – Endpoint or action outcome directed toward attaining positive health outcome such as optimal well-being, personal fulfillment, and productive living.
2. Bandura’s Self-Efficacy Theoryv A theory of situation-specific self-confidence that proposes that self-efficacy is fundamental
to initiating certain behavior necessary for competent performance.
v According to the theory, self-efficacy is enhanced by four factors: successful performances, vicarious experiences, verbal persuasion, and emotional arousal.
v Successful performance, which can be achieved by participatory modeling, is regarded as the most important factor.
People with weak belief in their self efficacy
shy away from difficult tasks (personal threats) have low aspirations and weak commitment to the goals they choose maintain a self diagnostic focus (rather than how to perform) dwell on personal deficiencies, obstacles & adverse outcomes attribute failures to deficient capabilities slacken their efforts or give up quickly in face of difficulty slow to recover their sense of efficacy after failures or setbacks prone to stress & depression
People with strong belief in their efficacy
set challenging goals & sustain strong commitments to their goals approach difficult tasks as challenges rather than as threats maintain a task diagnostic focus attribute failures to insufficient effort heighten effort in face of difficulties quickly recover their sense of efficacy after failure or setback display low vulnerability to stress & depression
3. Health Belief Model (HBM)vdeveloped by Hochbaum, Rosenstock and Kegels
Core Assumptions and Statements
The HBM is based on the understanding that a person will take a health-related action (e.g.., use condoms) if that person:
1. feels that a negative health condition (e.g., HIV) can be avoided,2. has a positive expectation that by taking a recommended action, he/she will
avoid a negative health condition (e.g., using condoms will be effective at preventing HIV), and
3. believes that he/she can successfully take a recommended health action (e.g., he/she can use condoms comfortably and with confidence).
Community Health Nursing by Caesar G. Balatero, RN | 5
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
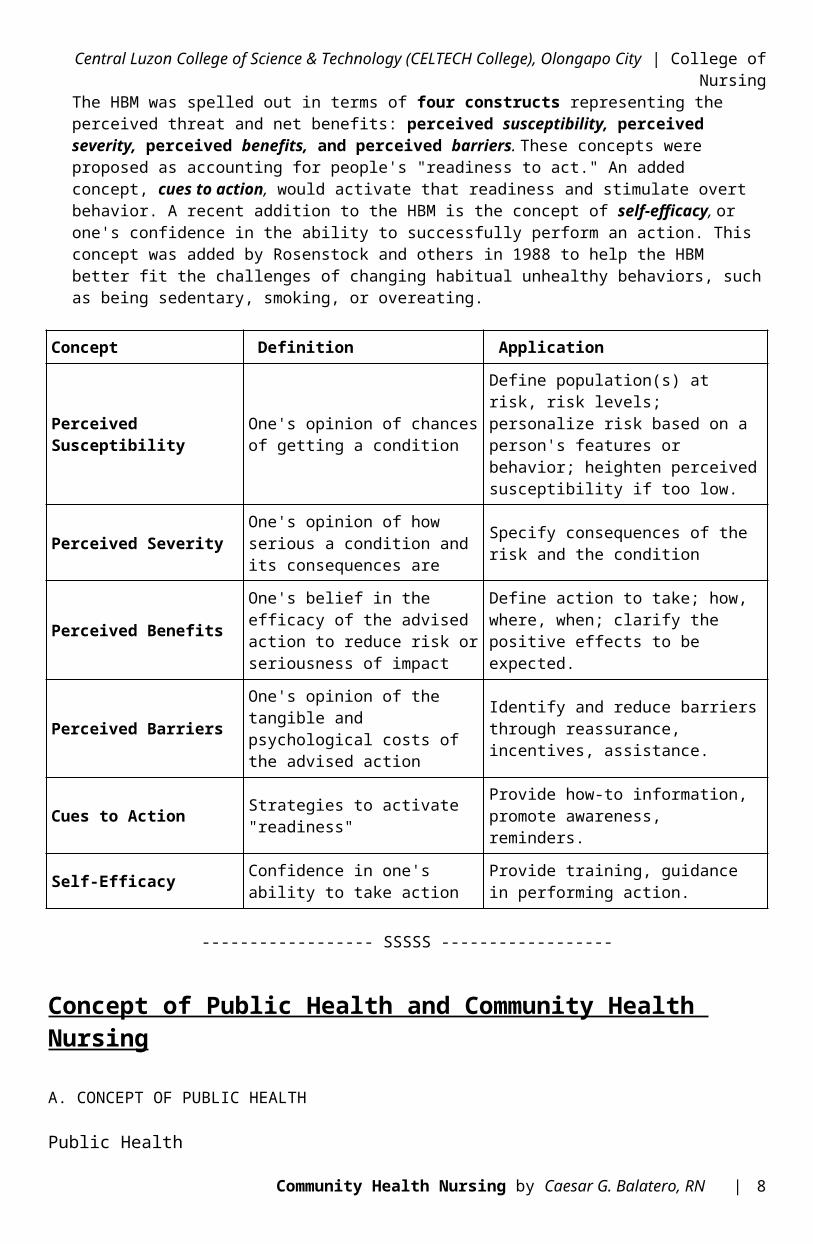
The HBM was spelled out in terms of four constructs representing the perceived threat and net benefits: perceived susceptibility, perceived severity, perceived benefits, and perceived barriers. These concepts were proposed as accounting for people's "readiness to act." An added concept, cues to action, would activate that readiness and stimulate overt behavior. A recent addition to the HBM is the concept of self-efficacy, or one's confidence in the ability to successfully perform an action. This concept was added by Rosenstock and others in 1988 to help the HBM better fit the challenges of changing habitual unhealthy behaviors, such as being sedentary, smoking, or overeating.
Concept Definition Application
Perceived Susceptibility One's opinion of chances of getting a condition
Define population(s) at risk, risk levels; personalize risk based on a person's features or behavior; heighten perceived susceptibility if too low.
Perceived SeverityOne's opinion of how serious a condition and its consequences are
Specify consequences of the risk and the condition
Perceived Benefits
One's belief in the efficacy of the advised action to reduce risk or seriousness of impact
Define action to take; how, where, when; clarify the positive effects to be expected.
Perceived BarriersOne's opinion of the tangible and psychological costs of the advised action
Identify and reduce barriers through reassurance, incentives, assistance.
Cues to Action Strategies to activate "readiness"
Provide how-to information, promote awareness, reminders.
Self-Efficacy Confidence in one's ability to take action
Provide training, guidance in performing action.
------------------ SSSSS ------------------
Concept of Public Health and Community Health Nursing
A. CONCEPT OF PUBLIC HEALTH
Public Healthv Dr. C.E. Winslow: “science and art of preventing disease, prolonging life, promoting
health and efficiency through organized community effort for the sanitation of the environment, control of communicable diseases, the education of individuals in personal hygiene, the organization of medical and nursing services for the early diagnosis and preventive treatment of disease, and the development of the social machinery to ensure everyone a standard of living adequate for the maintenance of health, so organizing these benefits as to enable every citizen to realize his birthright of health and longevity.”
In diagram:
science and art of → 1. preventing disease → through organized community effort
Community Health Nursing by Caesar G. Balatero, RN | 6
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
2. prolonging life 3. promoting health and efficiency
↓
for the: to ensure everyone 1. sanitation of the environment a standard of living ← 2. control of communicable diseases 3. education of individuals in personal hygiene ↓ 4. organization of medical and nursing services adequate for the maintenance of health for the early dx and preventive tx of disease 5. development of social machinery
↓
so organizing these benefits as to
↓
Enable every citizen to realize his birthright of health and longevity
In short: Public health is a science and art of preventing disease, prolonging life and efficiency to enable every citizen to realize his birthright of health and longevity.
vHanlon: “Public health is dedicated to the common attainment of the highest level of physical, mental, and social well-being and longevity.”
4 GOAL: contribute to the most effective total development and life of the individual and his society
vWHO: “art of applying science in the context of politics so as to reduce inequalities in health while ensuring the best health for the greatest number.”
4 further presented the core business of public health as:
1. disease control2. injury prevention3. health protection4. healthy public policy5. promotion of health and
equitable health gain
Essential public health functions1. health situation monitoring and analysis2. epidemiological surveillance3. development of policies and planning
Community Health Nursing by Caesar G. Balatero, RN | 7
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
4. strategic management of health systems and services5. regulation and enforcement to protect public health6. HR dev’t and planning7. health promotion, social participation, and empowerment8. ensuring quality or health services9. research, development and implementation of innovative solutions
Public Health Nursing
v a term coined by Lillian Wald to denote a service available to all people.v refers to the practice of nursing in the national and local government health departments.
It is community health nursing practiced in the public sector.v WHO Expert Committee on Nursing: “a special field of nursing that combines the skills
of nursing, public health and some phases of social assistance and functions as part of the total public health program for the promotion of health, improvement of the conditions in the social and physical environment, rehab of illness and disability.”
National League of Philippine Government Nurses came up with the Standards of Public Health Nursing in the Philippines 2005
↓ Differentiated PHN and CHN only in one area: setting of work as dictated by
funding.
HISTORICAL BACKGROUND OF PUBLIC HEALTH NURSING IN THE PHILIPPINES
1898 – start of PHN as embedded in history of the DOH which was first established as the Department of Public Works, Education and Hygiene
1912 – the Fajardo Act created Sanitary Divisions1914 – school nursing was rendered by a nurse employed by the Bureau of Health in Leyte1916-1918 – Miss Perlita Clark took charge of the PHN work1919 – the first Filipino nurse supervisor under Bureau of Health, Miss Carmen del
Rosario, was appointed.1928 – first convention of nurse was held1986 – reorganization of Department of Health1987-1989 – E.O. No. 119 reorganization of Department of Health, created several offices and services2005-2006 – development of the Rationalization Plan
Functions of Public Health Nurse
1. Management function2. Supervisory function3. Nursing care function4. Collaborating and coordinating function5. Health promotion and education function6. Training function7. Research function
------------------ SSSSS ------------------
Community Health Nursing by Caesar G. Balatero, RN | 8
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
B. CONCEPT OF COMMUNITY HEALTH NURSING
Community Health Nursing
v Jacobson: CHN is a learned practice discipline4 Ultimate goal: contribute to the promotion of client’s OLOF
v Ruth B. Freeman: CHN is a service rendered by a professional nurse with the community, groups, families, and individuals at home, in health centers, in clinics, in school, in places of work for the promotion of health, prevention, of illness, care of the sick at home and rehabilitation.
Philosophy CHN is based on the worth and dignity of man (Dr. Margaret Shetland)
Concepts1. Health promotion – primary focus2. Practice is extended to benefit not only the individual but the whole family and
community3. Community health nurses are generalists4. Contact with client/s may be over a long period of time and include all ages and
all types of health care5. Utilizes current knowledge6. Using the nursing process for periodic measurements of progress
Goal help communities and families to cope with the discontinuities in health and threats
Ultimate Goal raise the level of health of the citizenry
Objectives1. participate in the development of over-all health plan2. provide quality nursing services3. coordinate nursing services4. participate/conduct researches5. provide staff development
Principles (adapted from those of Mary S. Gardner, Leahy, Cobb and Jones)1. is based on recognized needs of clients2. CH nurse must understand objectives and policies of his agency3. family is the unit of service4. CHN must be equitable5. Health teaching is a primary responsibility6. CH nurse works as a member of the health team7. periodic evaluation of CHN services8. continuing staff education programs be provided9. resourcefulness10. utilize existing active organized groups in
the community11. educative supervision12. accurate recording and reporting
Roles of a CH (even PH) Nurse1. Planner/Programmer 6. Trainer/Health Educator/
Counsellor
Community Health Nursing by Caesar G. Balatero, RN | 9
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
2. Provider of Nursing Care 7. Health Monitor3. Manager/Supervisor 8. Role Model4. Community Organizer 9. Change agent5. Coordinator of Services 10.
Recorder/Reporter/Statistician/Researcher
Theories and Models related to CHNThe commonly used theories are:
1. Nightingale’s theory of environment 2. Orem’s Self care model 3. Neuman’s health care system model 4. Roger’s model of the science and
unitary man 5. Pender’s health promotion model 6. Roy’s adaptation model 7. Milio’s Framework of prevention 8. Salmon White’s Construct for Public health nursing 9. Block and Josten’s Ethical Theory of population focused nursing 10. Canadian Model
S Milio’s Framework of Prevention
Nancy Milio v a nurse and leader in public health policy and public health education v developed a framework for prevention that includes concepts of
community-oriented, population-focused carev The basic treatise is that behavioral patterns of populations and individuals
who make up populations are a result of habitual selection from limited choices. v She challenged the common notion that a main determinant for
unhealthful behavioral choice is lack of knowledge.
S Salmon White’s Construct for Public Health Nursing
Mark Salmon Whitev describes a public health as an organized societal effort to protect, promote
and restore the health of people and public health nursing as focused on achieving and maintaining public health.
v gave 3 practice priorities i.e.; (1) prevention of disease and poor health, (2) protection against disease and external agents and (3) promotion of health. For these 3 general categories of nursing intervention have also been put forward, they are:
1. education directed toward voluntary change in the attitude and behaviour of the subjects
2. engineering directed at managing risk-related variables 3. enforcement directed at mandatory regulation to achieve better
health. v Intervention target is in 4 categories
1. Human/Biological 2. Environmental 3. Medical/technological/organizational 4. Social
S Block and Josten’s Ethical Theory of Population-Focused Nursing
Derryl Block and Lavohn Josten (public health educators)
Community Health Nursing by Caesar G. Balatero, RN | 10
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
v proposed this theory based on intersecting fields of public health and nursing. They have given 3 essential elements of population-focused nursing that stem from these 2 fields:
1. the primacy of prevention2. an obligation to population3. centrality of relationship-based care
the first two are from public health and the third element from nursing. Hence it implies to nursing that relation-based care is very important in population focused care.
S Canadian Model for Community
The community health nurse works with individuals, families, groups, communities, populations, systems and/or society, but at all times the health of the person or community is the focus and motivation from which nursing actions flow.
------------------ SSSSS ------------------
C. SPECIALIZED FIELDS IN COMMUNITY & PUBLIC HEALTH NURSING
School Nursingv a type of public health nursing that focuses on the promotion of health and
wellness of the pupils/students, teaching and non-teaching personnel of the schools.
v the primary role of the school nurse is to support student learning and ensure that educational potential is not hampered by unmet health needs.
HEALTH and NUTRITION CENTER (HNC) of the Department of Education (DepEd)v is mandated to safeguard the health and nutritional well-being of the total
school populationv has two divisions:
1. Health1.a. Medical1.b. Dental1.c. Nursing1.d. Health Education
2. Nutrition
Objectives of School Nursing
General: To promote and maintain the health of the school populace by providing comprehensive and quality nursing care.
Specific: 1. Provide quality nursing service to the school population.2. Create awareness among school children, personnel and administrators on
the importance of the promotive and preventive aspects of health through health education.
3. Encourage the provision of standard functional facilities.4. Provide nursing personnel with opportunities for continuing education and
training.5. Conduct and participate in researches related to nursing care; and6. Establish/strengthen linkages with government and non-government
organizations/agencies for school community health work.
Community Health Nursing by Caesar G. Balatero, RN | 11
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
Duties and Responsibilities of School Nurses1. Health advocacy2. Health and nutrition assessment (including other screening procedures such
as vision and hearing.)3. Supervision of the health and safety of the school plant4. Treatment of common ailments and attending to emergency cases5. Referrals and follow-up of pupils and personnel6. Home visits7. Community outreach like attending community assemblies and organizing
school community health councils8. Recording and reporting of
accomplishments9. Monitoring and evaluation of programs and
projects
Skills Needed by a School Nurse 1. Assessment and screening skills2. Health counselling skills3. Social mobilization skills4. Good oral and written communication skills5. Basic management skills6. Life skills
Functions of the School Nurse1. School health and nutrition survey2. Putting up a functional school clinic
S R.A. 124 – mandates that all schools are to provide school clinics for the treatment of minor ailments and attendance to emergency cases.
3. Health assessment4. Standard vision testing for children5. Ear examination6. Height and weight measurement and nutritional status determination
S children 10 yrs. old – weight-for-age and height-for-age indicators are used
S children 10 yrs. old – body mass index (BMI) is usedS deworming – 120 days, parental consent is a must
7. Medical referrals8. Attendance to emergency cases9. Student health counselling10. Health and nutrition education activities11. Organization of school-community health and nutrition
councils12. Communicable disease control13. Establishment of data bank on school health and nutrition
activities14. School plant inspection for healthy environment15. Rapid classroom inspection16. Home visitation
Occupational Health Nursingv an autonomous practice requiring independent decisions and creative solutions
to complex occupational and environmental health and safety problemsv focus: preservation and restoration of the health of workers and working
populationsv mission: to assure so far as possible every working man and woman in the country
is safe and in healthful working conditions.
Issues in Occupational Health Nursing
Community Health Nursing by Caesar G. Balatero, RN | 12
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
A. Physical hazards – radiation, temperature extremes, noise, electric and magnetic fields, lasers, microwaves, vibration
B. Chemical hazards – solution, mists, vapors, aerosols, gases, medications, particulate matter (fumes and dust), solvents, metals, oils, synthetic textiles, pesticides, explosives, and pharmaceuticals
C. Biological hazards – viruses, bacteria, fungi, mold, parasitesD. Mechanical hazards – inadequate work-station and tool design, frequent repetition
of a limited movement, repeated awkward movements with handheld tools, local vibrations
E. Psychosocial hazards – interpersonal conflict, unsafe working conditions, overtime, sexual harassment, racial inequality, role conflict, shift work, limited autonomy, poorly defined expectations and work instructions, absent or limited hob reward
Work-Related Injury and Illness
: Occupational injury – any injury such as a cut, fracture, sprain, or amputation that results from a single incident in the work environment
: Occupational illness – any abnormal condition or disorder, other than one resulting from an occupational injury, caused by exposure to environmental factors associated with employment.
The Worker’s Compensation
S P.D. 626 – promotes and develops a tax exempt employees’ compensation whereby employees and their dependents, in the event of work-connected disability or death, may promptly secure adequate income benefit, and medical or related benefits.
------------------ SSSSS ------------------
The Philippine Health Care Delivery System
A. RESTRUCTURED HEALTH CARE DELIVERY SYSTEM
Philippine Health Care Delivery Systemv composed of two sectors:
1. public sector – largely financed through a tax-based budgeting system at both national and local levels and where health care is generally given free at the point of service (although socialized user fees have been introduced in recent years for certain types of services)
2. private sector – largely market-oriented and where health care is paid through user fees at the point of service
PUBLIC SECTOR(at the national level)
Department of Health (DOH)
(at the local level)Local Government Units (LGUs)v runs the local health system with the devolution of health servicesv provincial government manages:
provincial hospitals district hospitals
Community Health Nursing by Caesar G. Balatero, RN | 13
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
v city/municipal government manages: health centers rural health units (RHUs) barangay health stations (BHSs)
PRIVATE SECTORv includes for-profit and non-profit health providersv includes providing health services in clinics and hospitals, health insurance,
manufacture of medicines, vaccines, medical supplies, equipment, and other health and nutrition products, research and development, human resource development and other health-related services.
------------------ SSSSS ------------------
B. THE DEPARTMENT OF HEALTH
Department of Health (DOH)v mandated as the lead agency in healthv has a regional field office in every regionv maintains specialty hospitals, regional hospitals and
medical centersv also maintains provincial health teams made up of DOH representatives to the
local health boards and personnel involved in communicable disease control
HISTORICAL BACKGROUNDYEAR NAME LAW1888 Superior Board of Health and Charity -------1898 Department of Public Works, Education and
Hygiene-------
(July) 1901
Board of Health Act No. 157
(Dec.) 1901
Insular Board of Health Act Nos. 307, 308
1905 Bureau of Health Act No. 14071915 Philippine Health Service Act No. 24681932 Bureau of Health Act No. 40071939 Department of Health and Public Welfare Act No. 4301947 Department of Health and Public Welfare
(reorg)E.O. No. 94
1978 Ministry of Health P.D. 13971987 Department of Health (through Pres.
Corazon Aquino)E.O. No. 119
Roles and Functions
1. ADMINistrator of Specific Servicesv Manage selected national health facilities and hospitals with modern
and advanced facilities that shall serve as national referral centers and selected health facilities at sub-national levels that are referral centers for local health systems
v Administer direct services for emergent health concerns that require new complicated technologies; administer special components of specific programs (TB, schistosomiasis, HIV-AIDS, etc.)
v Administer health emergency response services, including referral and networking system for trauma, injuries and catastrophic events, in cases of epidemic and other widespread public danger
2. LEADership in Health
Community Health Nursing by Caesar G. Balatero, RN | 14
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
v Serve as the national policy and regulatory institution.v Provide leadership in the formulation, monitoring and evaluation of
national health policies, plans, and programs.v Serve as advocate in the adoption of health policies, plans and
programs to address national and sectoral concerns.3. CAPAcity Builder and Enabler
v Innovate new strategies in health to improve the effectiveness of health programs, initiate public discussion on health issues and undertaking, and disseminate policy research outputs to ensure informed public participation in policy decision-making.
v Exercise oversight functions, and monitoring and evaluation of national health plans, programs and policies
v Ensure the highest achievable standards of quality health care, health promotion and health protection.
Vision:The DOH is the leader, staunch advocate and model in promoting Health for All in the
Philippines.
Mission:Guarantee, equitable, sustainable and quality health for all Filipinos, especially the poor and shall lead the quest for excellence in health.
The DOH shall do this by seeking all ways to establish performance standards for health human resources; health facilities and institutions; health products and health services that will produce the best health systems for the country.
Goal: Health Sector Reform Agenda (HSRA)v the overriding goal of the DOHv support mechanisms will be through sound organizational development,
strong policies, systems and procedures, capable human resources, and adequate financial resources.
Rationale for Health Sector ReformAlthough there has been a significant improvement in the health status of Filipinos for the last 50 years, the following conditions are still seen among the population:
slowing down in the reduction in the Infant Mortality Rate (IMR) and the Maternal Mortality Rate (MMR)
persistence of large variations in health status across population groups and geographic areas
high burden from infectious diseases rising burden from chronic and degenerative diseases unattended emerging health risks from environmental and work-
related factors burden of disease is heaviest on the poor
The reasons why the above conditions are still seen among the population can be explained by the following factors:
1. inappropriate health delivery system2. inadequate regulatory mechanisms for health services3. poor health care financing and inefficient sourcing or generation of
funds
FRAMEWORK FOR IMPLEMENTATION OF HSRA: FOURmula ONE for Health
Community Health Nursing by Caesar G. Balatero, RN | 15
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
v intends to implement critical interventions as a single package backed by effective management infrastructure and financing arrangements following a sector-wide approach
Goals of FOURmula ONE for Health
1. Better health outcomes2. More responsive health
systems3. Equitable health care
financing
Four Elements of the Strategy
1. Health financingv The goal of this heath reform area is to foster greater, better
and sustained investments in health.v The Philippine Health Insurance Corporation (PHIC) through
the National Health Insurance Program and the Department of Health through sector-wide policy support will lead this component jointly.
2. Health regulationv the goal is to ensure the quality and affordability of health
goods and services3. Health service delivery
v the goal is to improve and ensure the accessibility and availability of basic and essential health care in both public and private facilities and services
4. Good governancev the goal is to enhance health system performance at the
national and local levels
National Health Insurance Program (NHIP)
v a key feature of the FOURmula ONE for Healthv supports each of the elements in terms of:
financing – as it reduces the financial burden placed on Filipinos by health care costs
regulation – as the NHIP’s role in accreditation and payments based on quality acts as driver for improved performance in the health care
service delivery – as the NHIP demands fair compensation for the costs of care directed at providing essential goods and services in health.
governance – as it is a prudent purchaser of health care thereby influencing the health care market and related institutions
Objectives of the Health Sector Reform Agenda
a. Improve the general health status of the populationb. Reduce morbidity and mortality from certain diseasesc. Eliminate certain diseases as public health problemsd. Promote healthy lifestyle and environmental healthe. Protect vulnerable groups with special health and nutrition needsf. Strengthen national and local health systems to ensure better health
service deliveryg. Pursue public health and hospital reformsh. Reduce the cost and ensure the quality of essential drugs
Community Health Nursing by Caesar G. Balatero, RN | 16
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
i. Institute health regulatory reforms to ensure quality and safety of health goods and services
j. Strengthen health governance and management support systemsk. Institute safety nets for the vulnerable and marginalized groupsl. Expand the coverage of social health insurancem. Mobilize more resources for healthn. Improve efficiency in the allocation, production and utilization or
resources for health
Roadmap for All Stakeholders in Health:National Objectives for Health 2005 to 2010
v provides the road map for stakeholders in health and health-related sectors to intensify and harmonize their efforts to attain its time-honored vision of health for all Filipinos and continue its avowed mission to ensure accessibility and quality of health care to improve the quality of life of all Filipinos, especially the poor.
v sets the targets and the critical indicators, current strategies based on field experiences, and laying down new avenues for improved interventions.
v provides concrete handle that would guide policy makers. Program managers, local government executives, development partners, civil society and the communities in making crucial decisions for health
Global and National Health Imperatives
Public health systems are operating within a context of ongoing changes, which exert a number of pressures on the public health system. These changes include:
1. Shifts in demographic and epidemiological trends in diseases, including the emergence and re-emergence of new diseases and in the prevalence of risk and protective factors;
2. New technologies for health care, communication and information;3. Existing and emerging environmental hazards some associated with
globalization;4. Health reforms.
In response to above trends, the global community, represented by the United Nations General Assembly, decided to adopt a common vision of poverty reduction and sustainable development in September 2000.
MILLENNIUM DEVELOPMENT GOALS (MDGs)v exemplifies the vision of poverty reduction and sustainable developmentv are based on the fundamental values of solidarity, shared responsibility, respect
for nature, freedom, tolerance, health, and equality.
The 8 Millennium Development Goals (MDGs)1. Eradicate extreme poverty and hunger2. Achieve universal primary education3. Promote gender equality and empower women4. Reduce child mortality5. Improve mental health6. Combat HIV/AIDS, malaria and other diseases7. Ensure environmental sustainability8. Develop a global partnership for development
Community Health Nursing by Caesar G. Balatero, RN | 17
Central Luzon College of Science & Technology (CELTECH College), Olongapo City | College of Nursing
Except for goals 2 and 3, all the MDGs are health or health-related.
In order to achieve these goals, the participation of all members of the society from both developing and developed countries is required.
Levels of Health Care and Referral System
1. PRIMARY LEVEL OF CAREv devolved to the cities and the municipalitiesv health care provided by center physicians, public health nurses, rural health
midwives, barangay health workers, traditional healers, and others at the barangay health stations and rural health units.
2. SECONDARY LEVEL OF CAREv given by physicians with basic health trainingv usually given in health facilities either privately owned or government-
operated such as infirmaries, municipal and district hospitals, and out-patient departments of provincial hospitals.
3. TERTIARY LEVEL OF CAREv rendered by specialists in health facilities including medical centers as well as
regional and provincial hospitals, and specialized hospitals such as the Philippine Heart Center.
v referral center for the secondary care facilities
------------------ SSSSS ------------------
C. DEVOLUTION OF HEALTH SERVICES (RA 7160)
Republic Act 7160v took place in 1991v all structures, personnel and budgetary allocations from the provincial health
level down to the barangays were devolved to the local government units to facilitate health service delivery.
Devolutionv made local government executives responsible to operate local health care
services.
Provincial governmentsv operate the hospital system, provincial and district hospitals
City/municipal governmentsv operate the health centers (HC), rural health units (RHU), and barangay
health stations (BHS)
Community Health Nursing by Caesar G. Balatero, RN | 18




















![[LEC_OLESON] CHD](https://img.pdfslide.us/doc/110x75/577d2e911a28ab4e1eaf66e8/lecoleson-chd.jpg)