Embed Size (px)
Citation preview

Erasmo Miele
Centro di Riferimento Regionale per le Malattie
Infiammatorie Croniche Intestinali dell’Età
Evolutiva Dipartimento di Scienze Mediche Traslazionali,
Sezione di Pediatria
Università di Napoli “Federico II”
Sanguinamento dal Tratto
Intestinale Alto:
Approccio Clinico ed
Endoscopico

Upper GI Bleeding in Children
Upper GI bleeding (or haemorrhage) is that originating proximal to
the ligament of Treitz; in practice from the oesophagus, stomach and
duodenum.
• Haematemesis (and coffee-ground vomitus) is vomiting of blood
from the upper GI tract or occasionally after swallowing blood
from a source in the nasopharynx.
• Melaena is the passage of black tarry stools usually due to acute
upper GI bleeding but occasionally from bleeding within the small
bowel or right side of the colon.
• Hematochezia is the passage of fresh or altered blood per
rectum usually due to colonic bleeding. Occasionally profuse
upper GI or small bowel bleeding can be responsible.

Upper GI Bleeding in Children
Epidemiology
• Severe GI bleeds are rare in the general pediatric population and are
therefore not well documented.
• Upper gastrointestinal bleeding (UGIB) accounts for about 20% of all
gastrointestinal bleedings in childhood.
• In the pediatric ICU population, 6-20% of the general pediatric
population has UGIB .
• The estimated incidence of peptic-ulcer bleeding in the US pediatric
population in 2008 ranged from 0.5 to 4.4/100.000 individuals.
J Pediatr 2000;76:135-146 J Pediatr Gastroenterol Nutr 2012; 54: 733–736

• 486 children hospitalised for Upper GI Complications (UGIC) (defined as
endoscopically confirmed gastroduodenal lesions or clinically defined
haematemesis or melena) were enrolled between November 1999 and
November 2010 through the emergency departments (ED) of 8 Italian
paediatric hospitals
• The number of UGIC patients admitted through EDs can be roughly
estimated as 2.4 per 10 000 children with ED visits
• Threefold increased risk of UGIC associated with either NSAID or oral
corticosteroid use
• A twofold increased risk of UGIC was estimated for paracetamol and
antibiotics.
Arch Dis Child Published Online First: 20 Dec 2012 doi:10.1136/ archdischild-2012-302100

World J Pediatr 2012; 8: 123-128
0% 10% 20% 30% 40% 50%
Varices
Erosive Esophagitis
Vomiting-Induced Hematemesis
Peptic Ulcer Disease
Questionable
Other
None
Multiple Present study
Western hemisphere
Eastern hemisphere
Comparison of Etiology of Upper GI Bleeding by Geographic Areas
(1977-2009)
(1976-1983)

Age Wise Distribution of Etiology of
Upper GI Bleeding in Children
Age group Well appearing Ill appearing
Neonates Swallowed maternal blood Hemorrhagic gastritis
Hemorrhagic disease of newborn Necrotizing enterocolitis
Drugs- heparin, indomethacin Gastric stress ulcers
Thrombocytopenia,
platelet dusfunction
Disseminated intravascular
coagulation
Infants Reflux esophagitis Hemorrhagic gastritis
Reactive gastritis Gastric stress ulcers
Arteriovenous malformation
Children Mallory-Weiss tear Esophageal varices (liver disease)
Reflux esophagitis Hemorrhagic gastritis
Reactive gastritis Stress ulcers
Adapted from Boyle JT. Pediatr Rev 2008;29:39–52.

World J Pediatr 2012; 8: 123-128
Hemoglobin and mean corpuscular volume (MCV) are expressed as mean ± SD. *: P<0.001, the mean hemoglobin level was signifi cantly lower in the melena group than in the other two groups; †: no significant difference between the groups; ‡: P<0.001, the need for transfusion was signifi cantly higher in the melena group than in the other two groups; §: P=0.01, a source of bleeding was more commonly found in the melena group than in the other two groups
Presentation of Upper Gastrointestinal Bleeding
• Four % of children seen in a tertiary care pediatric Emegency
Department with hematemesis have clinically significant upper GI
hemorrhage (UGIH).
• Four features detected all of the children with significant UGIH:
Unwell appearance
History of melena
History of hematochezia
Moderate to large volume of fresh blood in the vomitus
• In addition, older age, a significant medical history, and the presence
of tachycardia were independently associated with a clinically
significant UGIH.
JPGN 2012;54: 737–743
Indian J Pediatr 2013; 80 (4):326–333
Initial Assessment and Stabilization

Management of GI Bleeding Before Endoscopic Diagnosis
Nasogastric Tube
• Nasogastric intubation may help confirm, but cannot discount, suspected
upper GI bleeding (strong agreement)
• Suspected rupture of esophageal/gastric varices probably does not
contraindicate nasogastric intubation (strong agreement)
• To ensure emptying of the stomach content before EGD, intravenous
erythromycin should be administered at a dose of 250 mg (5 mg/kg in
children), in the absence of contraindications (strong agreement)
Annals of Intensive Care 2012, 2:46

Management of GI Bleeding Before Endoscopic Diagnosis
Proton Pump Inhibitors:
• Do not offer acid-suppression drugs (proton pump inhibitors or H2-receptor
antagonists) before endoscopy to patients with suspected non-variceal
upper gastrointestinal bleeding.
• Offer proton pump inhibitors to patients with non-variceal upper
gastrointestinal bleeding and stigmata of recent haemorrhage shown at
endoscopy.
Acute Upper Gastrointestinal Bleeding: Management

World J Pediatr 2012; 8: 123-128
Correlation Between Time to Endoscopy and Identification of a Source
*: P>0.05; †: P<0.01
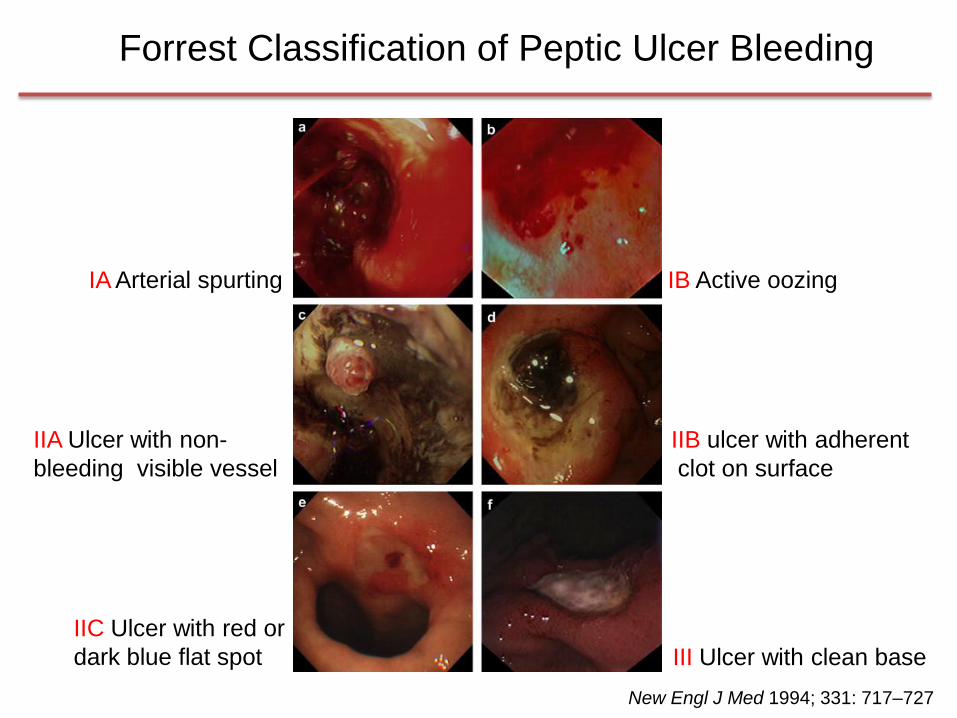
III Ulcer with clean base
IA Arterial spurting IB Active oozing
IIA Ulcer with non-
bleeding visible vessel
IIB ulcer with adherent
clot on surface
IIC Ulcer with red or
dark blue flat spot
New Engl J Med 1994; 331: 717–727
Forrest Classification of Peptic Ulcer Bleeding

Annals of Intensive Care 2012, 2:46
Treatment of Upper GI Bleeding Unrelated To Portal Hypertension
• In the presence of stigmata associated with a low risk of rebleeding
(Forrest type IIc and III), endoscopic hemostasis should not be used
(strong agreement).
• In the presence of stigmata associated with a low risk of rebleeding
(Forrest type IIc and III), PPI treatment at “standard” doses should be
continued (strong agreement).
• In the presence of stigmata associated with a high risk of rebleeding
(Forrest type Ia, Ib, IIa), endoscopic hemostasis should be performed
(strong agreement).

Management of Non-Variceal Bleeding
Endoscopic treatment
• Do not use adrenaline as monotherapy for the endoscopic treatment of
non-variceal upper gastrointestinal bleeding.
• For the endoscopic treatment of non-variceal upper gastrointestinal
bleeding, use one of the following:
mechanical method (for example, clips) with or without adrenaline
thermal coagulation with adrenaline
fibrin or thrombin with adrenaline
Acute Upper Gastrointestinal Bleeding: Management

Annals of Intensive Care 2012, 2:46
Treatment of Upper GI Bleeding Related to Portal Hypertension
• Vasoactive treatment (terlipressin or somatostatin or a somatostatin
derivative) should be administered as soon as possible when portal
hypertension is the suspected cause of GI bleeding (strong agreement).
• Specific vasoactive treatment of the splanchnic area should probably not
be administered when portal hypertension is not the suspected cause of
GI bleeding (weak agreement).
• Vasoactive treatment should be continued for 3 to 5 days after endoscopic
therapy of esophageal/gastric varices rupture (strong agreement).

Management of Variceal Bleeding
Antibiotics:
Offer prophylactic antibiotic therapy at presentation to patients with
suspected or confirmed variceal bleeding
Oesophageal varices
• Use band ligation
• Consider transjugular intrahepatic portosystemic shunts (TIPS) if
bleeding is not controlled.
Gastric varices
• Offer endoscopic injection of N-butyl-2-cyanoacrylate
• Offer TIPS if bleeding is not controlled
Acute Upper Gastrointestinal Bleeding: Management

MG, Female, 15 yrs
• Mental Retardation with Acute Myeloid Leukemia
• Allogeneic Bone Marrow Transplantation from HLA-matched unrelated donor
• Day+11: Hematemesis, Melena and Ematochezia
Plts: <10.000
Somatostain: 6000 mcg /24h x 72 h with GI bleeding stop
Renal Failure
• Day+24: Hemorrhagic cystitis
• Day+67: Hematemesis, Melena and Ematochezia
Severe Anemia (Hb 4,9 g/dl)
Several Red Blood Cells and Platelets Transfusions per day
Somatostin
• Day+71: Wireless Capsule Endoscopy
A Challenging Bleeding Clinical Case

Wireless Capsule Endoscopy

MG, 15 yrs,
• ………….
• Day+75: Angiographic findings: celiac, superior and inferior mesenteric arteriogram shows normal vascular anatomy with no bleeding sites
To be continued……………
A Challenging Bleeding Clinical Case

Key Points
• Upper gastrointestinal bleeding (UGIB) accounts for about
20% of all gastrointestinal bleedings in childhood.
• Mostly the clinical course is benign and approximately
80% of the patients present self limited bleeding
• UGIB is a potentially life threatening medical emergency
requiring an appropriate diagnostic and therapeutic
approach.
• Upper GI endoscopy is the gold standard for diagnosis
and treatment of UGIB.