Embed Size (px)
Citation preview

SALT LAKE CITY

Today’s Speakers:
• Mark Higley, Vice President - Regulatory Affairs• Amy Streeter, Manager, Talent, Acquisition and
Development.• Hans Gullickson, Member Services
Representative

Todays’ Schedule• 8:30 - 9:00 AM Registration
• 9:00 - 10:30 AM Preparing for the Round Two “Recompete”
• 10:30 - 10:45 AM Morning Break
• 10:45 - 12:00 AM Competitive Bidding in 2015 and Beyond
• 12:00 - 12:45 PM Lunch/Introductions
• 12:45 - 2:15 PM Human Resources Management Part 1
• 2:15 – 2:30 PM Afternoon Break
• 2:30 - 3:15 PM Human Resources Management Part 2
• 3:15 - 4:00 PM Options for “Acquiring” a Bid Contract
• 4:00 - 4:30 PM Partnering with VGM - Summary of Our Services
Competitive Bidding:
Part 1 – Preparing for the Round Two“Recompete”
http://vgmncbservices.com/FallSeminarSeries/FSS.asp


Some Introductory Commentsand History…


And as we know…
• On July 15, 2014, CMS announced its plans to recompete thesupplier contracts awarded in Round 2 of the DMEPOSCompetitive Bidding Program and the National Mail-Orderdiabetic testing supplies competition. (It is required by statute todo at least every three years.)
• The current contract period expires June 30, 2016; the newcontracts will begin on July 1, 2016 (which is a contract period oftwo and one half years).
• For the recompete, CMS is making changes to both thecomposition of the product categories (includingaddingnewproducts) and the number of competitive biddingareas (CBAs).

• We will have a question and answer sessionduring the last half hour or so of thispresentation...but please feel free to chime in!
• I’ll do my best to answer your particularconcerns and issues!
• In the meantime, let’s start with some basicsabout the program…

The product categories to be included in the Round2 Recompete are as follows:
• Enteral Nutrients, Equipment and Supplies
• General Home Equipment and Related Supplies andAccessories (includes hospital beds and relatedaccessories, group 1 and 2 support surfaces,commode chairs, patient lifts, and seat lifts)
• Nebulizers and Related Supplies
• Negative Pressure Wound Therapy (NPWT) Pumpsand Related Supplies and Accessories
• And…
• Respiratory Equipment and Related Supplies andAccessories (includes oxygen, oxygen equipment,and supplies; continuous positive airway pressure(CPAP) devices and respiratory assist devices (RADs)and related supplies and accessories)
• Standard Mobility Equipment and RelatedAccessories (includes walkers, standard power andmanual wheelchairs, scooters, and relatedaccessories)
• Transcutaneous Electrical Nerve Stimulation (TENS)Devices and Supplies

• CMS is conducting the Round 2 Recompete in virtually thesame geographic areas that were included in Round 2.
• BUT…Because of changes to the metropolitan statisticalareas and boundary changes to ensure that no CBA isincluded in more than one state, however, there will be117 CBAs in the Round 2 Recompete (compared to 91 inthe current Round 2 competition).
• A list of the ZIP codes included in each CBA is also availableon the CBIC website (dmecompetitivebid.com – click onupper left “Round 2 Recompete tab) .
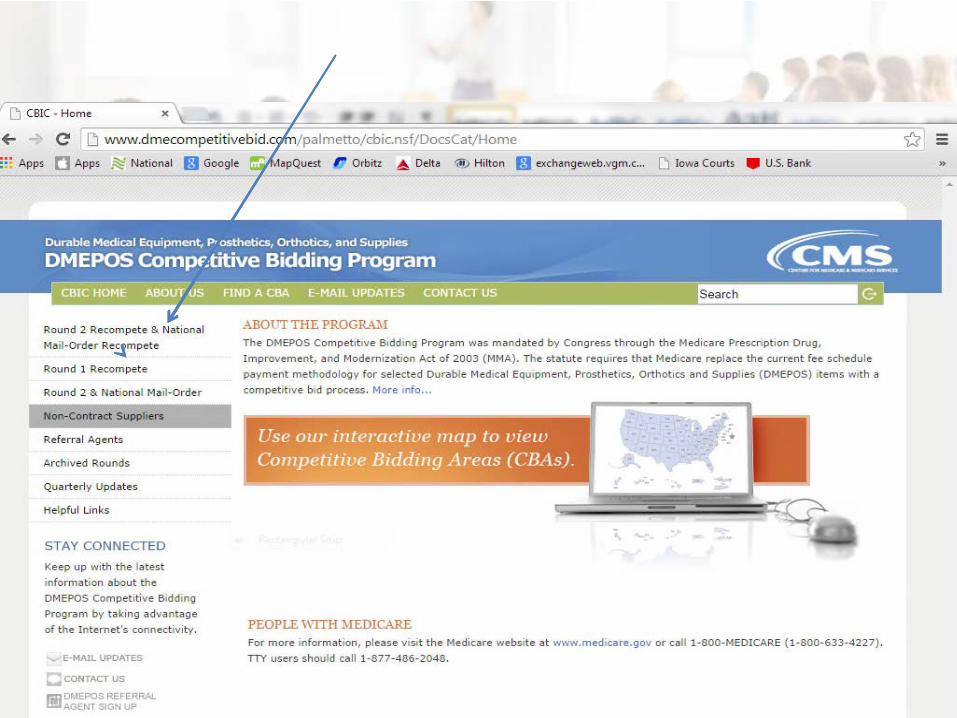

See the left menu tabs for current information andstatus. Registration is NOT yet open…

What you CAN do now – review this page to ensure you areproperly enrolled, licensed, etc. prior to the bid window…
• CMS will also be conducting the National Mail-OrderRecompete for diabetic testing supplies concurrentlywith the Round 2 Recompete.
• As before, this “competition” will include all parts ofthe United States, including the 50 states, the Districtof Columbia, Puerto Rico, the U.S. Virgin Islands,Guam, and American Samoa.
• We saw relatively few contracts (15) awarded for thenational diabetic program.
• You are likely aware the reimbursement amountsaveraged more than a 70% (!!) decrease from the feeschedule

Here is the general timeline for the Round 2 Recompete:
• July 15, 2014: CMS began the “pre-bidding supplierawareness program” and updated dmecompetitivebid.comwith Recompete information.
• “Fall” 2014: CMS will announce the bidding schedule and willbegin a “bidder education program” (Mark will demonstratethe ‘bid worksheets’ and offer some tips shortly…).
• Bidder registration period to obtain user ID and passwordsmay begin in December.
• “Winter” 2015: Bidding begins (we think February).• Once more: DME providers considering bidding should prepare now, including ensuring
that their enrollment files at the National Supplier Clearinghouse are current, and that theyare accredited and hold all necessary state licenses for any products for which they will bid.

So…let’s start with common questions we receive…
• There was already a “Round 1 recompete”that affected, for example, Charlotte andMiami and the rest of the original nine CBAareas. What’s different this time around forproviders considering placing a bid or bids inRound 2 areas?
• The Categories!...the current Oxygen and CPAPDevices/Respiratory Assist Devices product categorieswere combined into a single product category; thecurrent Walkers and Wheelchairs/Scooters categorieswere combined into a single product category
• A new General Home Equipment category wascreated, including the previous Hospital Beds andSupport Surfaces categories in addition to newproducts; and a new TENS devices product categorywas added.
• Suppliers can bid on one or more productcategories, but they must bid on all specifiedHCPCS codes within the category. (A list of thespecific items in each product category isavailable on the Competitive BiddingImplementation Contractor website .
And…
• The external infusion pumps and suppliesproduct category, which was bid in the Round1 Recompete, is not included in the Round 2Recompete.

Lastly…
• The general home equipment categoryremoves transcutaneous electrical nervestimulation (TENS) devices.
• The nebulizers and related supplies are nowseparate category (as compared to the Round1 respiratory equipment category whichincluded these products).

• For some bidding companies, these productcategories combine products not typicallyfurnished by the supplier in the today’smarketplace.
• For example, HMEs furnishing oxygen andoxygen equipment do not necessarily furnishCPAP devices and RADs.

• Most Round 2 Recompete MSAs have one CBA.
• However, the three largest MSAs (Chicago, LosAngeles, and New York) are subdivided into multipleCBAs.
• And the biggest change from previous rounds…CBAsin multi-state MSAs have been re-defined (split up)so that there are no multi-state CBAs.
• There are 117 CBAs in the Round 2 Recompete(versus 91 in Round 2).
• Again…the CBAs with ZIP codes and maps areavailable now at www.dmecompetitivebid.com.
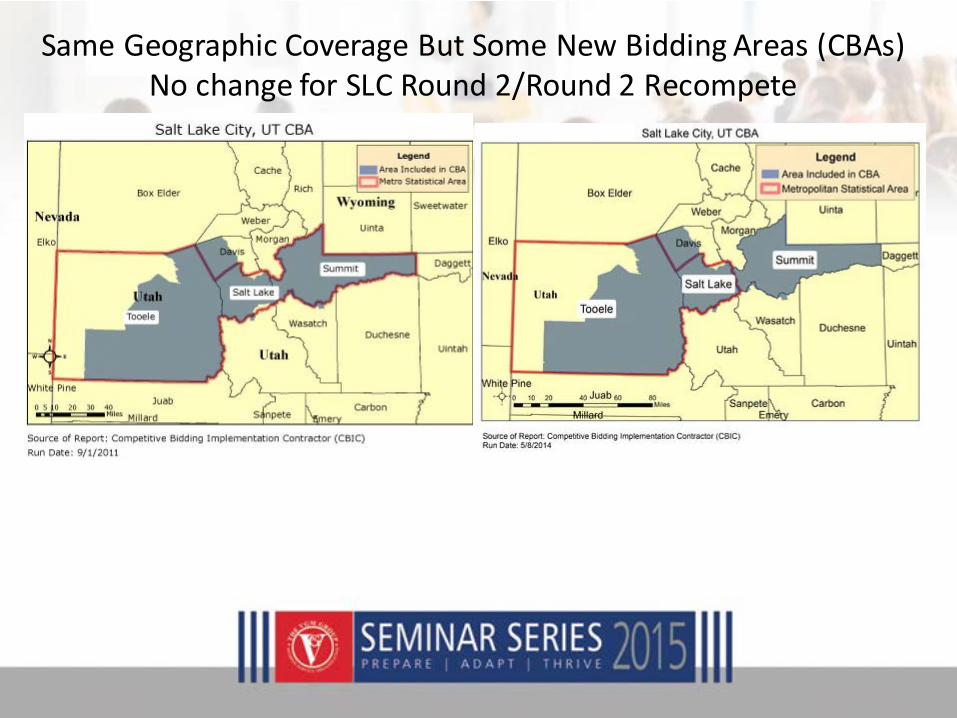
Same Geographic Coverage But Some New Bidding Areas (CBAs)No change for SLC Round 2/Round 2 Recompete

But multi-state MSAs are no longer: LOUISVILLE/JEFFERSON COUNTY, KY-IN
Round 2 CurrentMultiple State CBA
Round 2 Recompete CBALouisville

• So once more….CBAs in multi-state MSAs havebeen defined so that there are no multi-stateCBAs.
• There are 117 CBAs in the Round 2Recompete.
• I believe there is an opportunity with theRecompete to improve the reimbursements(“single payment amounts”) for Round 2products and services.
• The combiningof product categories (e.g., oxygen and CPAP) mightresult in a reduction in the amount of out-of-area bidders, who, inprevious rounds, bid CPAP in virtually all areas of the country.
• Delivery of CPAP supplies have seen, arguably, an increase in drop-shipments. Now that the biddingsupplier must also offer oxygenand oxygen equipment in the same CBAs (requiring comparablymore in-home service), I anticipate a decrease in the number ofout-of-area contracts offered (with a resulting increase inreimbursement/single payment amounts).

• In any case, remember that If you have only one location andare bidding in a CBA that includes more than one state, youmust have all required licenses for every state in that CBA.
• If you have more than one location and are bidding in a CBAthat includes more than one state, your company must haveall required licenses for the product category for every state inthat CBA.
• Make sure that current versions of all required licenses arewith the NSC BEFORE you bid. If any required licenses areexpired or missing from your enrollment file, your bid(s) maybe rejected.
(Most of you here today areaware of – and experienced
with – bidding basics….)
• Considerations for Submitting aBid
Period of Performance
• Suppliers that are awarded a contract mustagree to furnish the competitively bid itemsfor the full duration of the contract periodthroughout the entire CBA.
• The length of the contract period for theround one recompete is two and one halfyears, scheduled to begin July 1, 2016.

Servicing the Entire CBA• A contract supplier must furnish competitively bid
items to any beneficiary who maintains a permanentresidence in or who visits a CBA and who requeststhose items from the contract supplier.
• The only exception to this rule applies to a skillednursing facility (SNF) or nursing facility (NF) that isbidding for enteral nutrients, equipment, and suppliesand is awarded a contract as a specialty supplier thatfurnishes competitively bid items only to its ownresidents to whom it would otherwise furnish Part Bservices.
“Single Payment Amount” (SPA)
• As in previous rounds, existing DMEPOS fee schedulepayment amounts will be replaced with a “singlepayment amount” for selected items.
• The single payment amount for an item furnishedunder the Program is equal to the median amount ofbids submitted and accepted for that item.
• The single payment amount remains in effect for theentire contract period and is not adjusted by anyupdate factor (e.g. CPI Update).

• Most importantly!!! – HME providers must be aware thatthe “bid limits” for all Round 2 recompete items willrevert back to the current Medicare Fee Schedule. Insimpler terms, the upper bidding amount will not “startat” the current reimbursement (single payment amount)in effect now for a Round 2 CBA.
• By way of example, one month’s rental of E1390 oxygenconcentrator in the Salt Lake City, UT CBA is currentlyreimbursed at $90.00. The recompete bid limit for thisitem will be $178.24 (plus any inflation adjustment) andNOT $90.00 (!)

Meet Financial Standards• All bidders must meet certain “financial standards”
• Bidding suppliers are required to submit specifiedfinancial documents for the most recent year inwhich a tax return has been submitted.
• For the Round 2 recompete financial documentswill represent calendar or fiscal year 2013 or 2014.
• See your Fall Series URL for official documents.http://vgmncbservices.com/FallSeminarSeries/FSS.asp
• CMS determines a supplier’s financial viabilitybased on financial ratios calculated from thebidder’s submitted financial information.
• The financial ratios can be found on the CBICwebsite.
• All bidders must meet CMS’ established financialthresholds to be considered for a contract
• Commentary and examples of common HMEratios and other financial metrics are included onyour Fall Series URL.http://vgmncbservices.com/FallSeminarSeries/FSS.asp
Choice of CBAs/Product Categories
• Bidders do not have to submit a bid for allrecompete product categories and CBAs butmay choose to bid for certain productcategories in certain CBAs.
• However, the program (and DBidS software)requires bidders to submit bids for ALL codeswithin the category.

Physical Location Issue
• Contract suppliers must be ready to provide servicesin the CBA on day one of the contract period.
• To ensure that only qualified suppliers becomecontract suppliers, a supplier must have at least onephysical location that meets all requirements toserve a CBA in order to bid in that CBA.
• HOWEVER…Suppliers with physical locations outsideof CBAs may bid on those CBAs IF they meet allrequirements (e.g., state licensure, accreditation) atthe time of bidding.

• Contracts are awarded only to locations listed onForm A in the online DMEPOS Bidding System(DBidS).
• It is important that suppliers identify the PTANs of alllocations that will provide competitively bid items ina CBA; only those locations identified on the bid willbe included in the contract and eligible for Medicarepayment for competitively bid items at the time theprogram begins.
Service Entire Bidding Area• Suppliers should not submit a bid unless they currently
have the ability to furnish items and services throughoutthe entire bidding area.
• For the recompete product categories, suppliers must agreeto furnish competitively bid items to beneficiariesthroughout the entire CBA.
• If a supplier intends to use the services of a subcontractor,the supplier must ensure the subcontractor is accredited asapplicable and complies with the standards in 42 CFR§424.57(c).
• (More information about subcontracting is available at yourFall Series URL)
Commonly Ownedand/or Controlled Locations
• Suppliers may not bid against themselves for the sameproduct category in the same CBA.
• Therefore, commonly owned or commonly controlledsuppliers must submit one bid that includes allcommonly owned and/or controlled locations thatwould furnish competitively bid items in the sameproduct category in the designated CBA.
• Separate bids submitted for the same product categoryin the same CBA by supplier organizations that arecommonly owned or controlled will be disqualified.

• Commonly owned and/or controlled locationsoutside of the CBA that would routinely furnishitems in the product category to beneficiaries inthe CBA must also be identified on Form A underthe location-specific section.
• Only locations identified in the bid are included inthe contract and eligible for Medicare payment atthe time the program begins.

“Bona Fide” Bids• CMS requires that all bid amounts must be bona fide
(rational and feasible for the bidder to furnish at the bidprice) and that “suppliers should not submit a bid for anitem at a loss in order to improve their chances ofwinning a contract”.
• “Suppliers should include all costs related to furnishing anitem to the beneficiary in the bid price. CMS will evaluatebids to ensure that they are bona fide and may requestthat a supplier submit additional information, such asmanufacturers’ invoices, to validate the bid amount.”
• “The supplier will also be required to providea valid and reasonable rationale to support itsbid amount.”
• If a supplier submits a non-bona fide bid forany competitively bid item in a productcategory, the entire bid for that productcategory in that CBA will be disqualified.
• In perhaps a few weeks CMS will release a Round 2recompete “bid preparation worksheet” on the CBICwebsite (http://dmecompetitivebid.com) to assistbidders in determining their bid amount and if theirbid is bona fide.
• Suppliers should NOT mail this worksheet to theCBIC.
• However, if the supplier is asked to validate its bidduring the bona fide bid process, the worksheet canbe submitted along with a rationale to support thevalidity of the bid.

• The Bidding Process
The bidding process includes three steps:
• 1. Register for user ID and password
• 2. Submit bid in the bidding system
• 3. Mail required hardcopy documents
Register!• For an overview, you can start here:
http://vgmncbservices.com/Documents/DMEPOSRoundTwoRecompeteCB.pdf (see screen shots next)....
• As in original Round 2, Suppliers intending to submit a bidmust first obtain a user ID and password to access DBidS byregistering in the Individuals Authorized Access to the CMSComputer Services (IACS) application.
• Bidding suppliers will register in IACS on the CBIC website.Only an individual identified as an authorized official (AO)on the CMS-855S enrollment form can register the companyand approve the registration of the end users and backupauthorized officials (BAOs). A BAO is someone who is alsoidentified as an AO on the 855S and can serve as a backupto the AO.

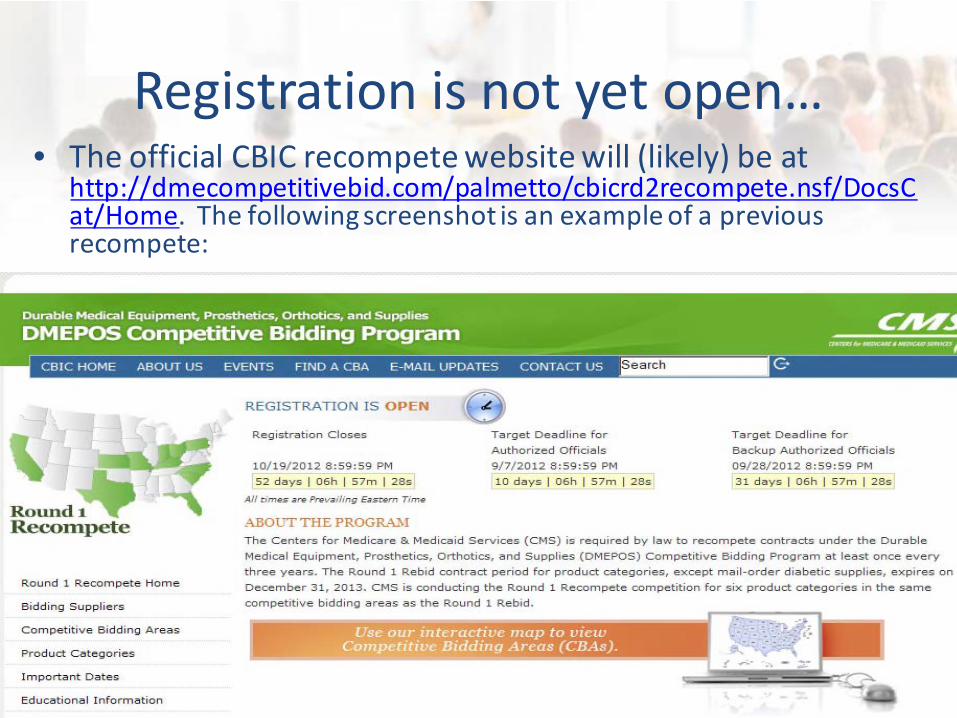
Registration is not yet open…• The official CBIC recompete website will (likely) be at
http://dmecompetitivebid.com/palmetto/cbicrd2recompete.nsf/DocsCat/Home. The following screenshot is an example of a previousrecompete:

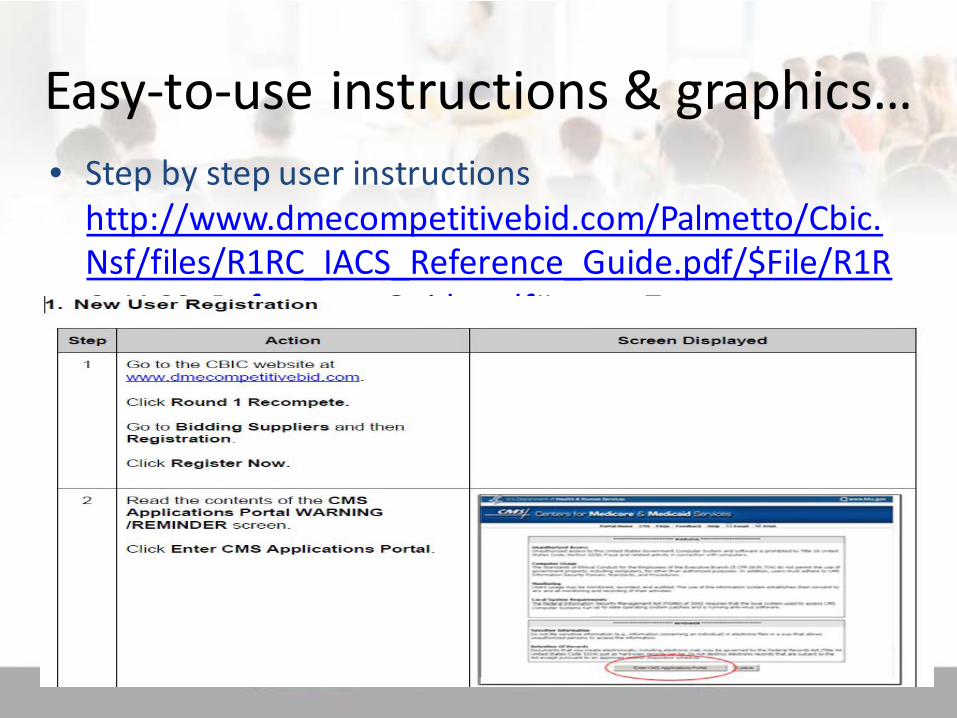
Easy-to-use instructions & graphics…
• Step by step user instructionshttp://www.dmecompetitivebid.com/Palmetto/Cbic.Nsf/files/R1RC_IACS_Reference_Guide.pdf/$File/R1RC_IACS_Reference_Guide.pdf#page=7
Submit Your Bid
• All bidders must submit bids electronically via DBidSwhich is located on the CBIC website.
• Step by step user instructions (example from Round1 recompete may be found here:
http://www.dmecompetitivebid.com/Palmetto/Cbic.Nsf/files/R1RC_IACS_Reference_Guide.pdf/$File/R1RC_IACS_Reference_Guide.pdf#page=7
Submitting a Bid…
• A supplier’s bid must be completed, approved, andcertified by the close of the bid window in order tobe considered.
• You may make changes to a bid after it has beenapproved or certified, but it will likely result in aneed to reapprove or recertify.
• Bidders do not have to submit a bid for all recompeteproduct categories and CBAs but may choose to bidfor certain product categories in certain CBAs.
Changing a Bid Submission
• We anticipate Bidders will again have 60 days tosubmit their bids in DBidS for the Round 2recompete.
• Bidders may amend their bids as many times asnecessary prior to the close of the 60-day bidwindow.
• Hardcopy documents may be amended prior to theclose of the bid window as long as the amendeddocuments are identified as “amended” and receivedby the CBIC by midnight, prevailing Eastern Time, onthe last day of the bid window.
• Once the bid window has closed, no furtherchanges can be made to the electronic bid,and CMS will only accept hardcopy documentsthat it has requested through the “covereddocument review process”.
•The Forms…(Summary & Actual Screen Shots)The bid application consists of two RFB forms approved by theOffice of Management and Budget (OMB): Form 10169A: Bid
Application Form 10169B: Bidding Form. Bidders are required tocomplete Form A and Form B online using the DMEPOS Bidding
System (DBidS), which can be accessed through the CBICwebsite. (BIDDING IS NOT YET OPEN!)
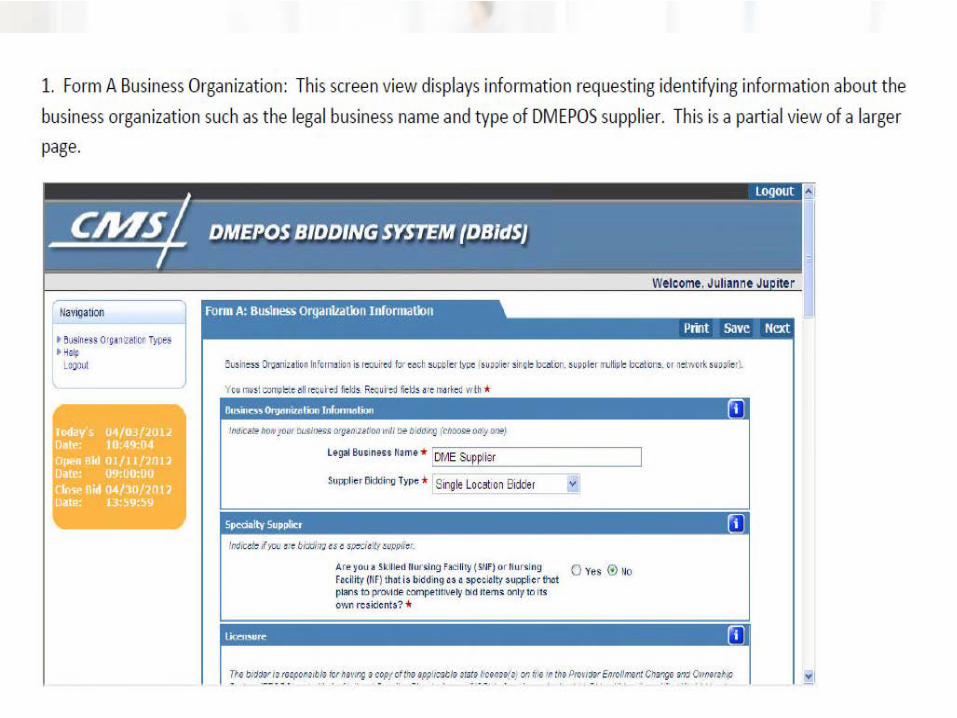
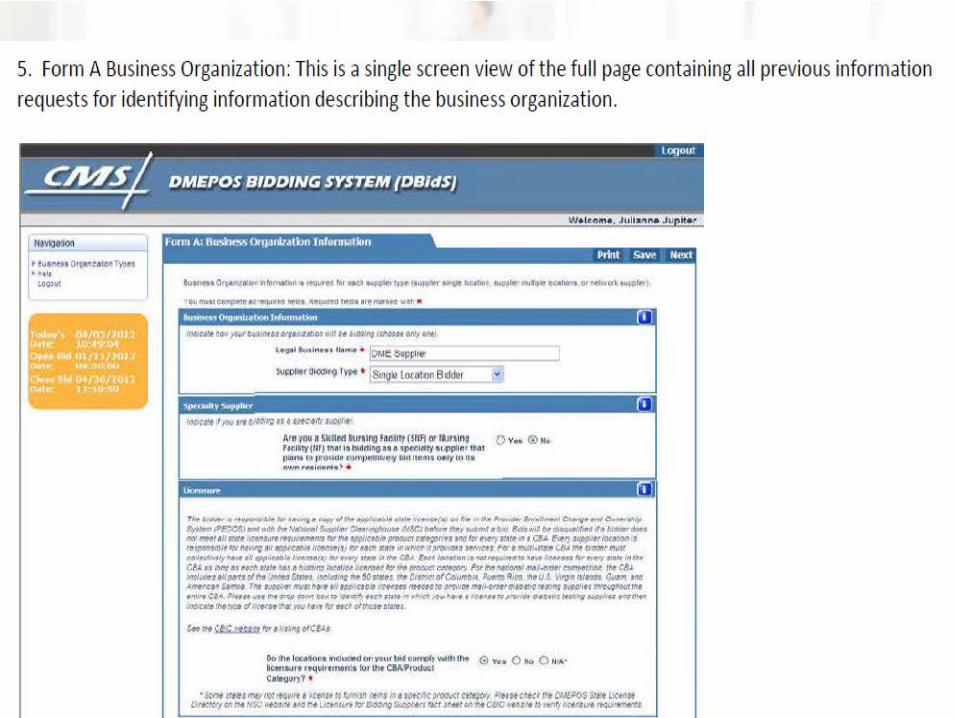
“Form A”• Form A requests information about the
bidder’s organization and the organization’slocations that are included in the bid.
• Suppliers must identify their organizations asone of a specific business organization type(supplier with single location, supplier withmultiple locations, or network).
• (For definitions and additional information,see your Fall Series URL).
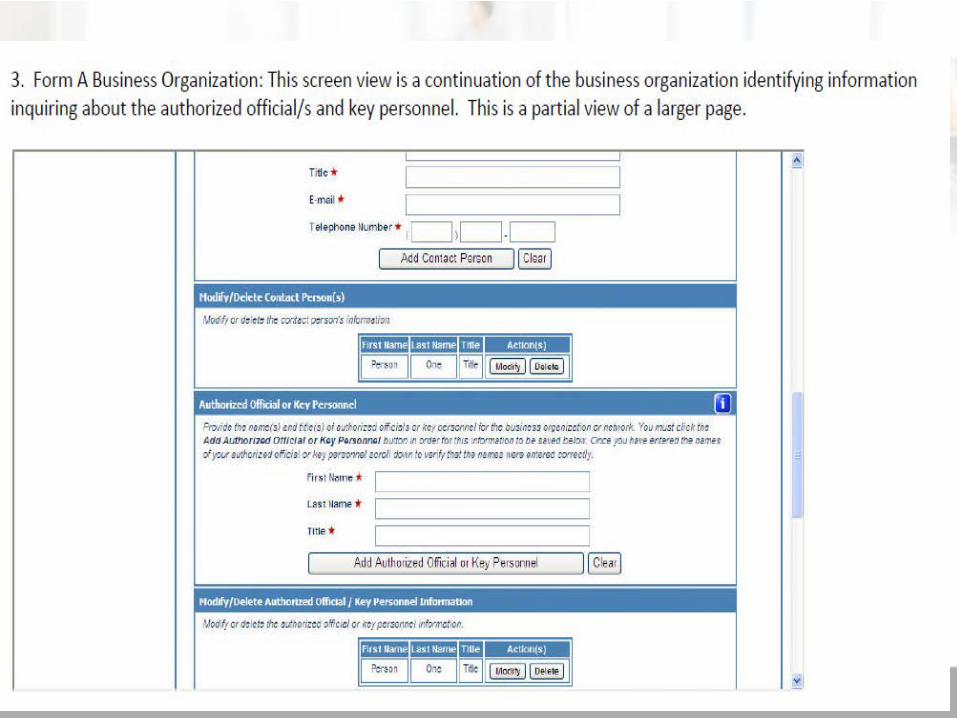
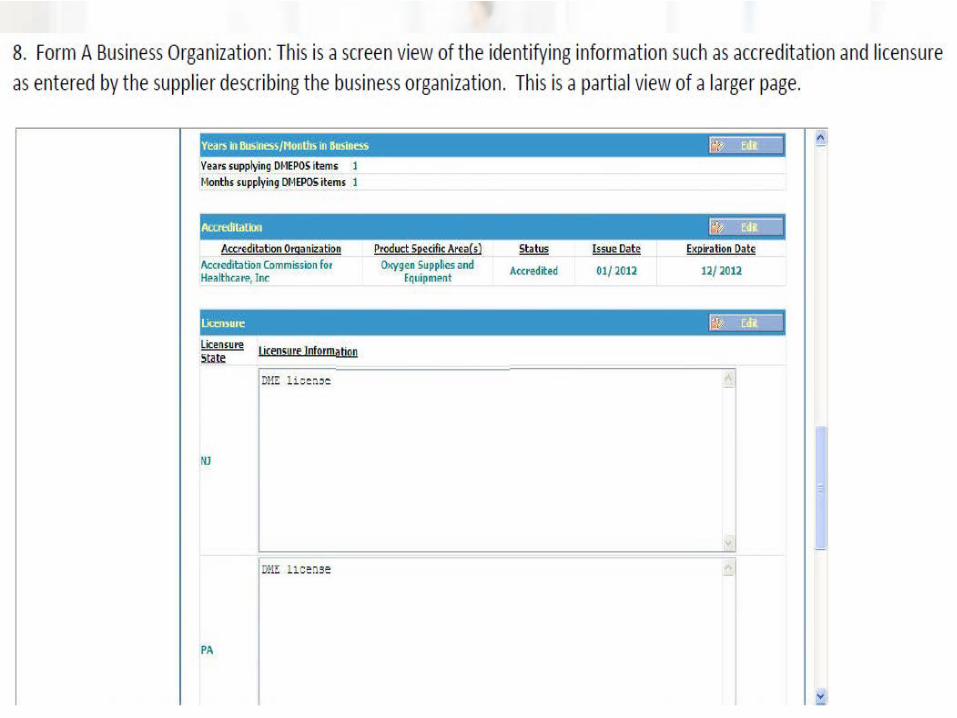
“Form A”• Form A requires the bidder to provide identifying
information, such as the legal business name, doing-business-as name, mailing address, and physicaladdress for both the business organization and foreach location identified by the PTAN.
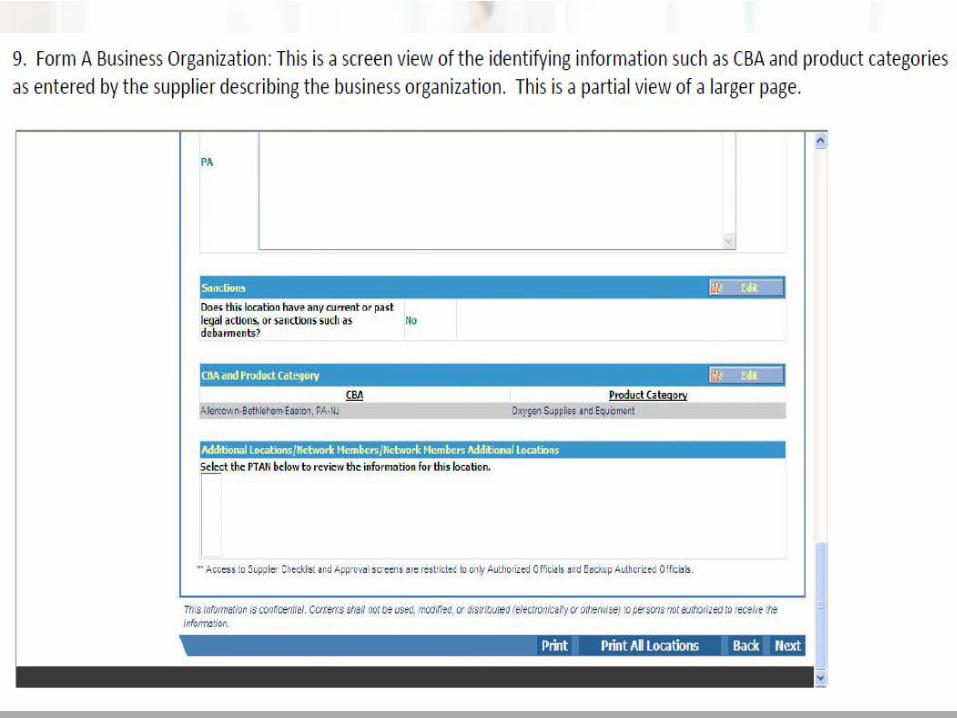
• Bidders will also select the CBA(s)/productcategory(s) for which they are bidding.
• Only the PTANs entered on the bid will be included ina contract award and will be the only PTANs qualifiedto receive payment from Medicare for competitivelybid items

Suppliers are only required tocomplete ONE Form A…
• Suppliers submit ONE Form A, regardless of thenumber of CBAs and product categories being bid.
• Exception: If a supplier has more than one locationwithin the same CBA and one or more of thelocations furnishes a different product line that doesnot compete against the other location(s), thesupplier will have distinct bidder numbers and mustcomplete separate Form As representing each biddernumber.

Bidding Types Identified on Form A
• Single Location: A single location supplier is abidding entity with only one location that has one ormore owners and is represented by a single PTAN.
• Multiple Location: Multiple-location suppliers havetwo or more locations with one or more owners(may be commonly owned or commonly controlled)and each location is identified by a unique PTAN.Multiple-location suppliers may or may not share acommon taxpayer identification number.
Multiple-location suppliers may be oneof the following:
• Subsidiary of a Parent Company/Holding Company:Parent-subsidiaries are separate entities where oneentity has control of the other.
• In general, a parent entity is a company that ownscontrolling interests in one or more companies. Asubsidiary is a company that is controlled by a parentcompany.
• These companies do not have to operate in the samelocations or even in the same business.

“Commonly Owned” or “CommonlyControlled”…
• Commonly owned suppliers are those where one ormore of them has an ownership interest totaling atleast 5 percent in the other(s). The term “ownershipinterest” is defined as “the possession of equity in thecapital, stock, or profits of another supplier,” asdefined in 42 CFR 414.412(e).
• Commonly controlled suppliers are those where oneor more of the supplier’s owners is also an officer,director, or partner in another supplier.

• Commonly owned or commonly controlled suppliersmust submit one bid that includes all commonlyowned or controlled locations that would furnish thesame product category within the designated CBA.
• Separate bids submitted for the same productcategory in the same CBA by commonly owned orcontrolled supplier organizations will be disqualified.
• See the pdf file athttp://vgmncbservices.com/FallSeminarSeries/FSS.asp for step bystep screen shots andinstructions START HERE!DMEPOS Round Two RecompeteCompetitive Bidding in 3 EASYSteps






“Form B”…the Bidding Form
• Includes the bidding forms for each productcategory/CBA.
• A separate Form B is required for each competition.
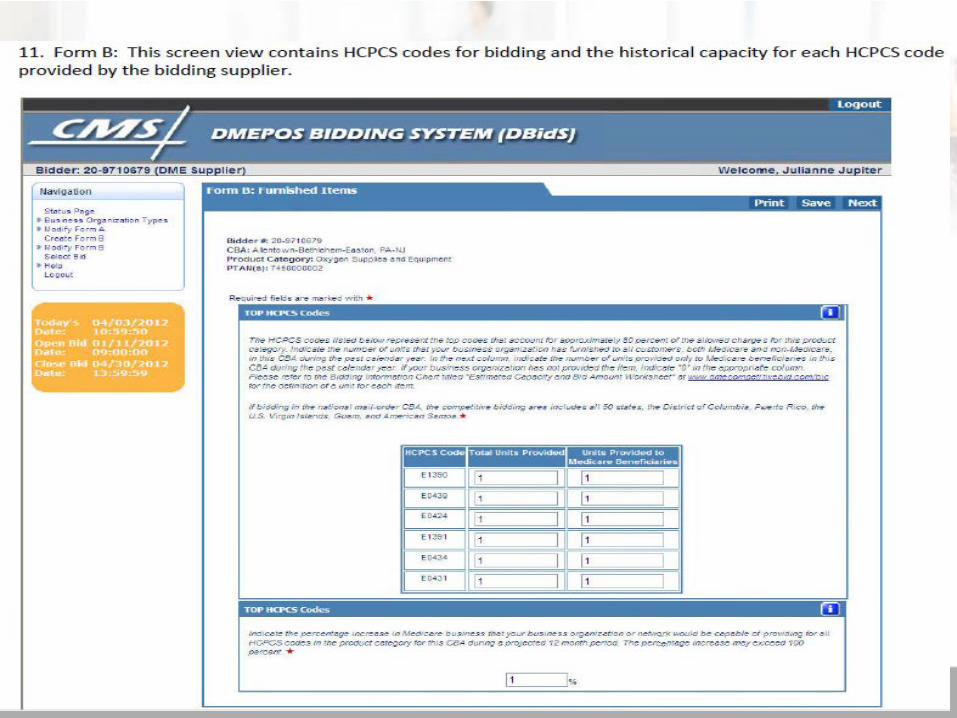
• Requests historic information about the supplier’sexperience in the product category and/or CBA. Thesupplier must provide the number of units it hasfurnished to all customers, Medicare and non-Medicare, for the top 80% of the HCPCS codes in theproduct category during the past calendar year in theCBA.
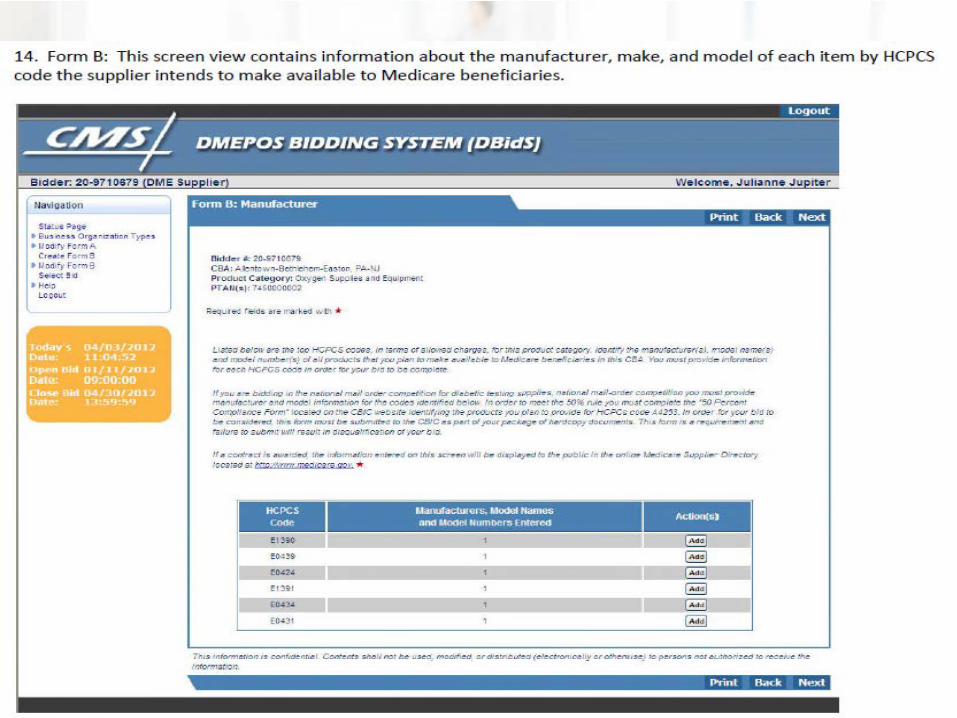
• Form B requires suppliers to identify the manufacturerand model of the products they plan to make available tobeneficiaries in the CBA.
• This information will be used to populate the MedicareSupplier Directory on the Medicare website,http://www.medicare.gov/.
• The supplier directory will list the manufacturerinformation for the top items provided by contractsuppliers to allow beneficiaries to make informed choicesabout the available products.

The Bidding Form:
• Total Estimated Capacity – Requires suppliers toprovide their “expected” capacity.
• The total estimated capacity indicates the number ofunits per HCPCS code you estimate you can furnishthroughout the entire CBA for one (1) year.
• The bid preparation worksheet on the CBIC websitecontains the unit by product category definitions andhistorical utilization.
CMS’ Capacity Instructions…• “To determine your expected capacity, calculate the
number of units you currently furnish in the area ona yearly basis and add units you would be capable ofproviding annually as of the start of the contractperiod. It is anticipated that suppliers can maintainthis level or greater throughout the contract period.”
• HOWEVER…we will discuss the “capacity”issue later on in the program and I willcomment on some pitfalls relative to its effecton your bid, and the industry as a whole…
Bidding Form, continued…
• Bid Price – The amount for which a supplier canfurnish the item, “including all costs associated withfurnishing the item”.
• “The bid price must be rational and feasible andmust indicate the cost of furnishing a new item orthe rental of a new item at the bid price submitted.”
• Item description, bid type, item weight and feeschedule amount will be provided on the bid form.

• After a supplier has completed Form B, the authorizedofficial or backup authorized official must (electronically)certify Form B for consideration of a contract.
• Bids will be evaluated based on the information providedin DBidS and submitted in the package of hardcopydocuments.
• Once the bid window closes, all bids are considered finaland cannot be amended by the bidder. Bidders can checkthe DBidS status page for 45 days after the bid windowcloses to confirm that their online bid is complete,approved, and certified by the authorized official orbackup authorized official, and whether their hardcopydocuments have been received by the CBIC.
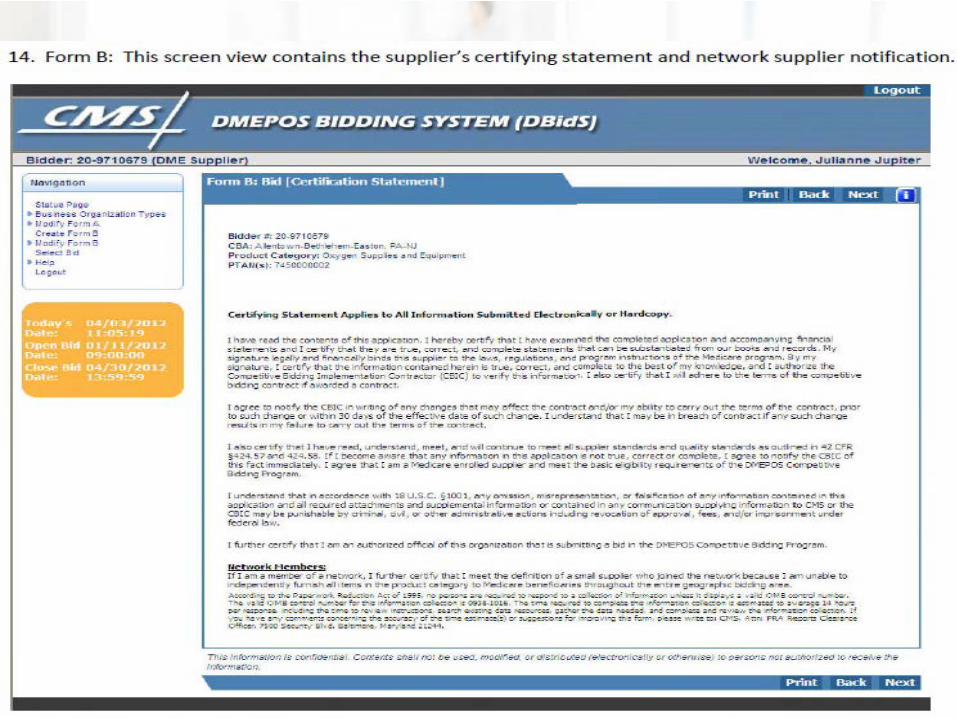
Certification Statement
• After completing Form A and Form B, the AO mustcertify the bid in DBidS. In order for a bid submissionto be complete, an AO or backup AO must approveForm A and certify that the information provided istrue, correct, and complete.
• The certification statement serves as the bidder’selectronic signature.
• Bidders can verify the status of their bid by visiting theDBidS home page.

• Let’s look at some Form Bscreen shots from the Round 1recompete RFB and DBidS…
• Again, a “step-by-step” is athttp://vgmncbservices.com/FallSeminarSeries/FSS.asp



Steps you can take now:• Have a copy of the required state license(s) on file
with the National Supplier Clearinghouse (NSC) andin the Provider Enrollment, Chain and OwnershipSystem (PECOS) for the physical location(s) that willbe on your bid to provide the items in the productcategory(s).
• Make sure your CMS-855S enrollment application isup-to-date with the NSC and in PECOS and indicatesthe products you furnish in the states where youprovide the items.
• For reference purposes, review the NSC DMEPOS StateLicense Directory on its website atwww.palmettogba.com/NSC
• The directory provides general state licensing requirementsand contact information for each state’s licensing board oragency. The directory is only a guide. Licensing requirementschange periodically, and it remains the responsibility of thebiddingsupplier to identify and obtain all required licenses.
• For more information about licensure requirements, consultthe appropriate license issuing agency listed on the guides orcall the NSC at 866-238-9652.
• One more time!http://vgmncbservices.com/FallSeminarSeries/FSS.asp

http://www.palmettogba.com/Palmetto/Providers.nsf/docsCat/National%20Supplier%20Clearinghouse~Resources~Licensure%2
0Information~Licensure%20Information?open

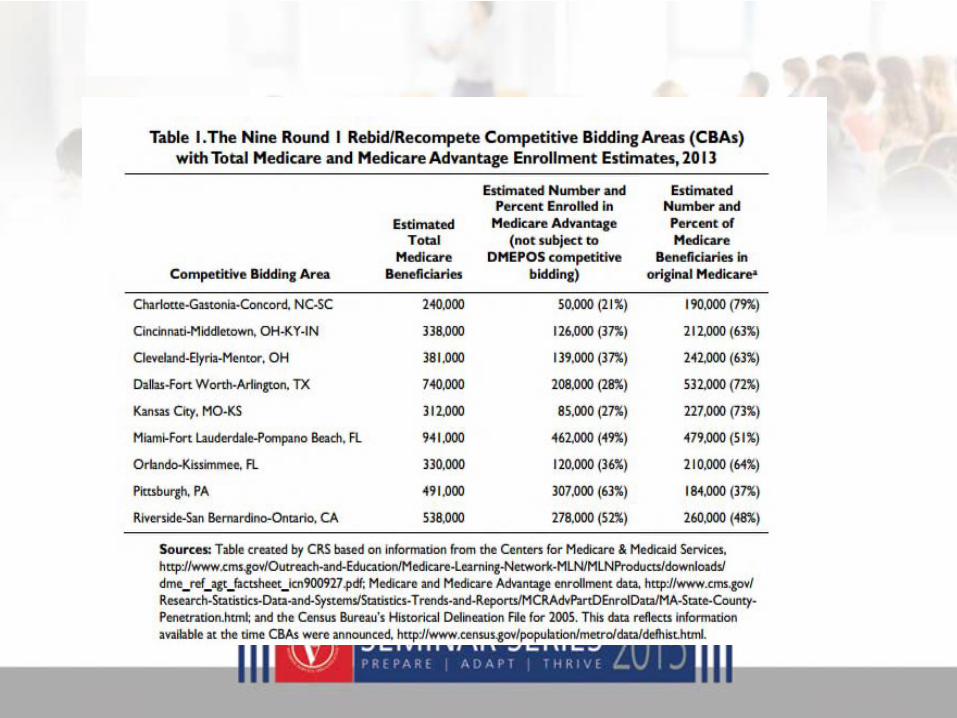
• Also…I’d like to remind providers thatMedicare Advantage beneficiaries are NOTcovered by this bidding program.


Bid Preparation Worksheets
• Not yet released for Round 2 Recompete –watch for email updates from me,
• We can still demo sample worksheets today.
• How is the composite bid is determined?
• Why do just a few HCPC codes affect theoverall composite bid?


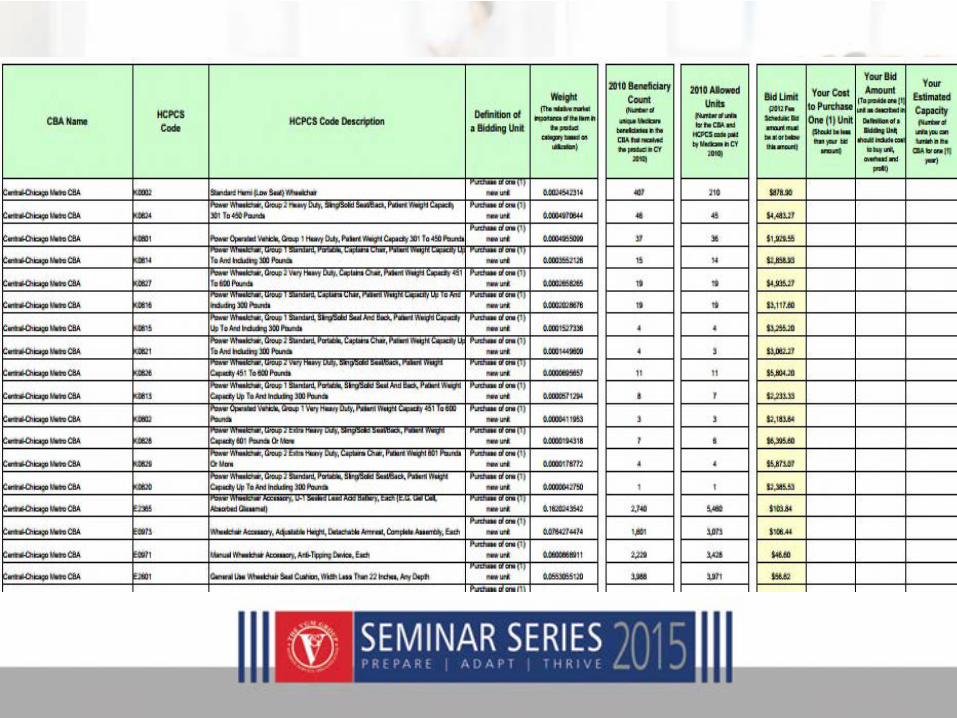
How to Use the Worksheets• The worksheets are divided into columns. Each item is
identified by its Healthcare Common Procedure CodingSystem (HCPCS) code and followed by a description of thatcode.
• The HCPCS code is listed in the first column and a descriptionof that code is provided in the next column.
• Review the code description column to determine the specificnumber of products in a unit.
• In most cases, a unit is described as a single product; however,in a few cases, a unit may be more than one product, such asfor diabetic test strips. In this case, a unit is 50 strips.

The column labeled Definition of a “Bidding Unit”…
• …indicateswhether to submit a bid on a rental or purchasebasis for the item.
• In order to ensure you submit your bid correctly, you will needto look at both the description of the code and the definitionof a biddingunit.
• For example, for enteral nutrients HCPCS code B4150, thecode descriptor indicatesthat 1 unit = 100 calories of enteralformula, and the biddingunit indicatesthat the bid is on apurchase basis. Therefore, you are submitting a purchase bidfor one unit consisting of 100 calories of enteral formula.
• The column labeled Weight provides,according to CMS, “the relative marketimportance of that item to other items in theproduct category. Items with a high numberhave a greater market importance than itemswith a low number.”
• We will debate that interpretation shortly…
• The worksheets provide reference data that shows historicutilization information.
• We anticipate a “2013 Beneficiary Count column” to show thenumber of beneficiaries in the biddingarea who received theitem in 2013, and the 2013 Allowed Units column shows thenumber of units that Medicare paid for in 2013 in the biddingarea.
• Remember: This information detailingthe allowed units andbeneficiary count is background information provided as acourtesy for those bidders that want recent information aboutthe number of items paid for by Medicare in the area and thenumber of beneficiaries in the area who have received theseitems. This background data is provided for informationalpurposes only.

• The Bid Limit column shows the current feeschedule amount for the item.
• Bids must be at or below the fee scheduleamount.
• Once more!! – the bid limit reverts to the2014 fee schedule; HME providers should NOTbe confused with the current Round 2 (orRound 1 recompete) “single paymentamounts”
Key Dynamics of theBidding Process
Strategies & Tactics for Calculating Bid Rates
• It is critical for HME providers contemplatingentering a bid for the 117 MSAs scheduled forthe Round 2 recompete to understand:
– the key dynamics of the bidding process, and;
– develop a strategy for calculating bid rates.
• This section will explain the statisticalmethodology that CMS uses to evaluate thebids.

The Root of the Problem
• We learned from the flawed bidding approaches ofproviders who participated in the failed first round, the re-bid and Round 2.
• These companies may have known their costs before theybid -- but many never completely understood HOW to bid.
• The great majority of these HMEs were not awardedcontracts, and not only because “they bid too high”. Manywere excluded due to preventable miscalculations,omissions, and, in my opinion…just stupid mistakes.
• Let’s get started!

• Unless the auction methodologychanges or there is a delay byCongress, the (flawed) “BidEvaluation Process” for yourrecompete is the same as RoundOne Re-bid and Round 2!

• CMS calculates expected beneficiary demand in the CBAfor the items in the category using past utilizationstatistics.
• CMS calculates total supplier capacity that would meetthe expected demand in CBA
– Supplier-estimated input of capacity (subject toverification/edit) is used to determine this
• CMS establishes a “composite bid” for each supplier thatsubmits bid for product category
What is a “Composite Bid?”
• Here is how the RFB describes it!: “To allow comparisonsamong bidders, CMS will establish a composite bid foreach supplier for each product category”
• “Composite bid is based on the sum of each item’s bidamount times its weight for the entire product category”
• “Weight of an item is based on volume, which isutilization of the individual item compared to other itemswithin the product category”

The Composite Bid
How it’s calculated, and how itshould drive your bidding strategy….
The Bid Evaluation Process
• CMS rationale for the use of a Composite Bid:
– “Composite bids allow CMS to compare allsuppliers bids submitted for the entire productcategory This allows Medicare to select thesuppliers with the lowest expected cost for theentire product category.”
• Array composite bids from low to high
• Calculate “pivotal” bid for category
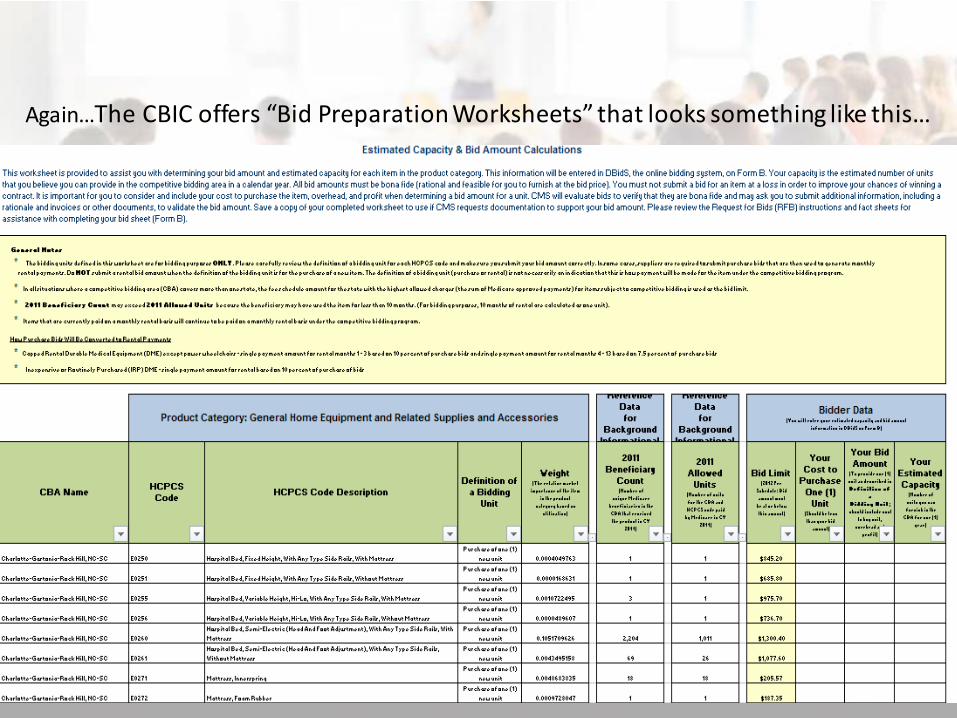
Again…The CBIC offers “Bid Preparation Worksheets” that looks something like this…
• But let’s simplify (and enlarge)the worksheet a bit todemonstrate how the compositebid is determined.
• We will demo CPAP from aprevious round.
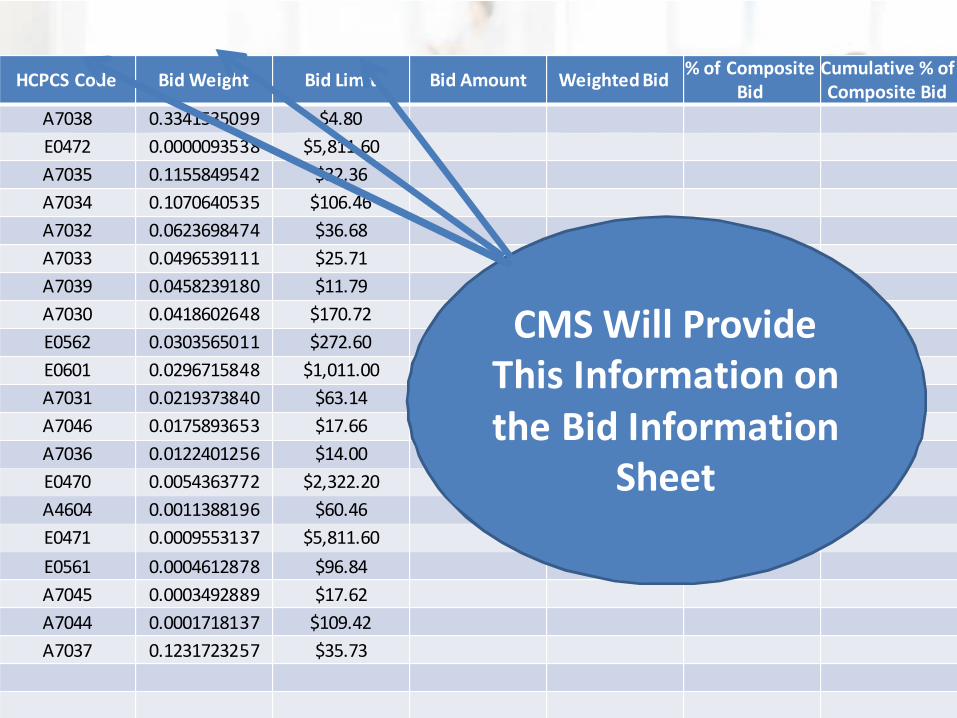
HCPCS Code Bid Weight Bid Limit Bid Amount Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80
E0472 0.0000093538 $5,811.60
A7035 0.1155849542 $32.36
A7034 0.1070640535 $106.46
A7032 0.0623698474 $36.68
A7033 0.0496539111 $25.71
A7039 0.0458239180 $11.79
A7030 0.0418602648 $170.72
E0562 0.0303565011 $272.60
E0601 0.0296715848 $1,011.00
A7031 0.0219373840 $63.14
A7046 0.0175893653 $17.66
A7036 0.0122401256 $14.00
E0470 0.0054363772 $2,322.20
A4604 0.0011388196 $60.46
E0471 0.0009553137 $5,811.60
E0561 0.0004612878 $96.84
A7045 0.0003492889 $17.62
A7044 0.0001718137 $109.42
A7037 0.1231723257 $35.73
CMS Will ProvideThis Information onthe Bid Information
Sheet
HCPCS Code Bid Weight Bid Limit Bid Amount Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80 $3.84
E0472 0.0000093538 $5,811.60 $4,649.28
A7035 0.1155849542 $32.36 $25.89
A7034 0.1070640535 $106.46 $85.17
A7032 0.0623698474 $36.68 $29.34
A7033 0.0496539111 $25.71 $20.57
A7039 0.0458239180 $11.79 $9.43
A7030 0.0418602648 $170.72 $136.58
E0562 0.0303565011 $272.60 $218.08
E0601 0.0296715848 $1,011.00 $808.80
A7031 0.0219373840 $63.14 $50.51
A7046 0.0175893653 $17.66 $14.13
A7036 0.0122401256 $14.00 $11.20
E0470 0.0054363772 $2,322.20 $1,857.76
A4604 0.0011388196 $60.46 $48.37
E0471 0.0009553137 $5,811.60 $4,649.28
E0561 0.0004612878 $96.84 $77.47
A7045 0.0003492889 $17.62 $14.10
A7044 0.0001718137 $109.42 $87.54
A7037 0.1231723257 $35.73 $28.58
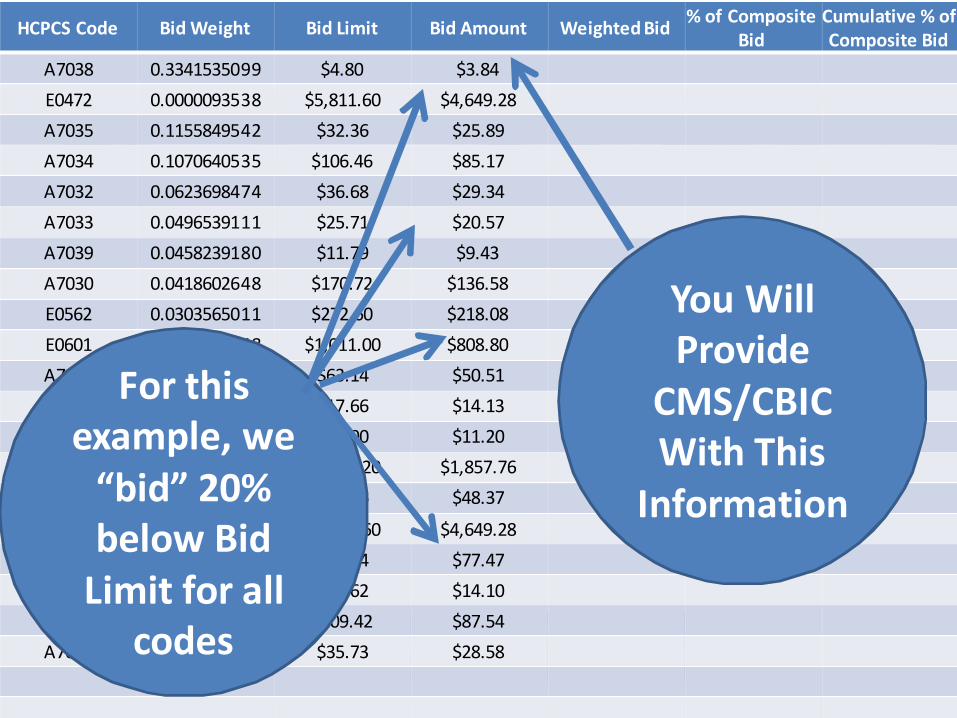
You WillProvide
CMS/CBICWith This
Information
For thisexample, we
“bid” 20%below Bid
Limit for allcodes

HCPCS Code Bid Weight Bid Limit Bid Amount Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80 $3.84 $1.28
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04
A7035 0.1155849542 $32.36 $25.89 $2.99
A7034 0.1070640535 $106.46 $85.17 $9.12
A7032 0.0623698474 $36.68 $29.34 $1.83
A7033 0.0496539111 $25.71 $20.57 $1.02
A7039 0.0458239180 $11.79 $9.43 $0.43
A7030 0.0418602648 $170.72 $136.58 $5.72
E0562 0.0303565011 $272.60 $218.08 $6.62
E0601 0.0296715848 $1,011.00 $808.80 $24.00
A7031 0.0219373840 $63.14 $50.51 $1.11
A7046 0.0175893653 $17.66 $14.13 $0.25
A7036 0.0122401256 $14.00 $11.20 $0.14
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10
A4604 0.0011388196 $60.46 $48.37 $0.06
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44
E0561 0.0004612878 $96.84 $77.47 $0.04
A7045 0.0003492889 $17.62 $14.10 $0.00
A7044 0.0001718137 $109.42 $87.54 $0.02
A7037 0.1231723257 $35.73 $28.58 $3.52
CMS WillCalculateWeighted
BidsBased onYour BidAmount

HCPCS Code Bid Weight Bid Limit Bid Amount Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80 $3.84 $1.28
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04
A7035 0.1155849542 $32.36 $25.89 $2.99
A7034 0.1070640535 $106.46 $85.17 $9.12
A7032 0.0623698474 $36.68 $29.34 $1.83
A7033 0.0496539111 $25.71 $20.57 $1.02
A7039 0.0458239180 $11.79 $9.43 $0.43
A7030 0.0418602648 $170.72 $136.58 $5.72
E0562 0.0303565011 $272.60 $218.08 $6.62
E0601 0.0296715848 $1,011.00 $808.80 $24.00
A7031 0.0219373840 $63.14 $50.51 $1.11
A7046 0.0175893653 $17.66 $14.13 $0.25
A7036 0.0122401256 $14.00 $11.20 $0.14
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10
A4604 0.0011388196 $60.46 $48.37 $0.06
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44
E0561 0.0004612878 $96.84 $77.47 $0.04
A7045 0.0003492889 $17.62 $14.10 $0.00
A7044 0.0001718137 $109.42 $87.54 $0.02
A7037 0.1231723257 $35.73 $28.58 $3.52
WeightedBid=
BidWeight
XBid
Amount
HCPCS Code Bid Weight Bid Limit Bid Amount Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80 $3.84 $1.28
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04
A7035 0.1155849542 $32.36 $25.89 $2.99
A7034 0.1070640535 $106.46 $85.17 $9.12
A7032 0.0623698474 $36.68 $29.34 $1.83
A7033 0.0496539111 $25.71 $20.57 $1.02
A7039 0.0458239180 $11.79 $9.43 $0.43
A7030 0.0418602648 $170.72 $136.58 $5.72
E0562 0.0303565011 $272.60 $218.08 $6.62
E0601 0.0296715848 $1,011.00 $808.80 $24.00
A7031 0.0219373840 $63.14 $50.51 $1.11
A7046 0.0175893653 $17.66 $14.13 $0.25
A7036 0.0122401256 $14.00 $11.20 $0.14
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10
A4604 0.0011388196 $60.46 $48.37 $0.06
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44
E0561 0.0004612878 $96.84 $77.47 $0.04
A7045 0.0003492889 $17.62 $14.10 $0.00
A7044 0.0001718137 $109.42 $87.54 $0.02
A7037 0.1231723257 $35.73 $28.58 $3.52
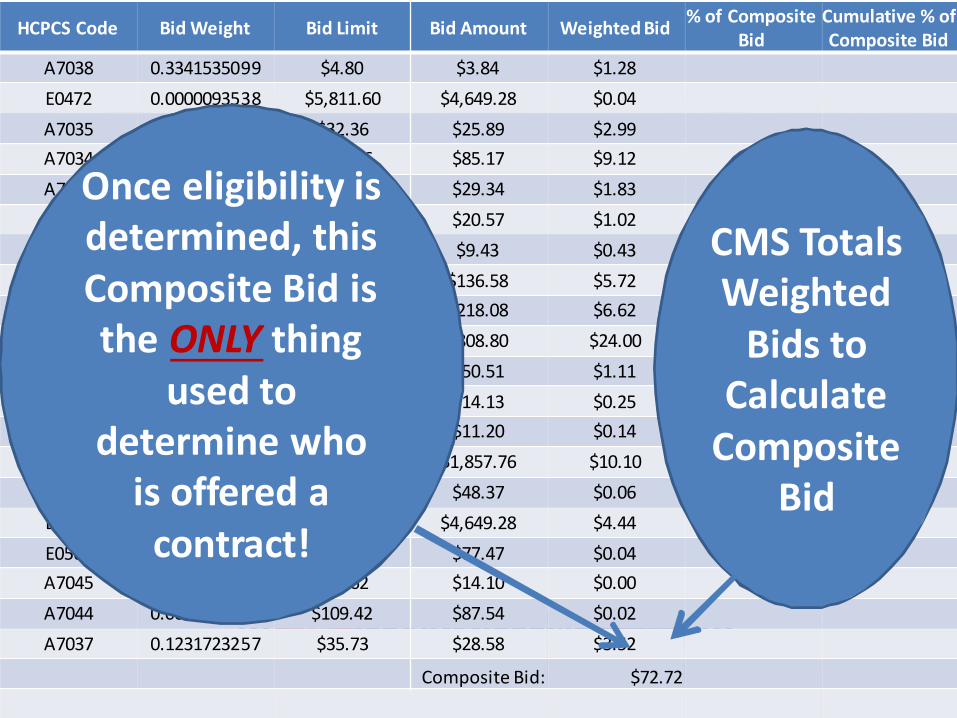
Composite Bid: $72.72
CMS TotalsWeighted
Bids toCalculate
CompositeBid
Once eligibility isdetermined, thisComposite Bid isthe ONLY thing
used todetermine who
is offered acontract!

HCPCS Code Bid Weight Bid LimitFinal BidAmount
Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80 $3.84 $1.28 1.76%
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04 0.06%
A7035 0.1155849542 $32.36 $25.89 $2.99 4.11%
A7034 0.1070640535 $106.46 $85.17 $9.12 12.54%
A7032 0.0623698474 $36.68 $29.34 $1.83 2.52%
A7033 0.0496539111 $25.71 $20.57 $1.02 1.40%
A7039 0.0458239180 $11.79 $9.43 $0.43 0.59%
A7030 0.0418602648 $170.72 $136.58 $5.72 7.86%
E0562 0.0303565011 $272.60 $218.08 $6.62 9.10%
E0601 0.0296715848 $1,011.00 $808.80 $24.00 33.00%
A7031 0.0219373840 $63.14 $50.51 $1.11 1.52%
A7046 0.0175893653 $17.66 $14.13 $0.25 0.34%
A7036 0.0122401256 $14.00 $11.20 $0.14 0.19%
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10 13.89%
A4604 0.0011388196 $60.46 $48.37 $0.06 0.08%
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44 6.11%
E0561 0.0004612878 $96.84 $77.47 $0.04 0.05%
A7045 0.0003492889 $17.62 $14.10 $0.00 0.01%
A7044 0.0001718137 $109.42 $87.54 $0.02 0.02%
A7037 0.1231723257 $35.73 $28.58 $3.52 4.84%
Composite Bid: $72.72
CMS Does NotShow You
This!!!
HCPCS Code Bid Weight Bid LimitFinal BidAmount
Weighted Bid% of Composite
BidCumulative % ofComposite Bid
A7038 0.3341535099 $4.80 $3.84 $1.28 1.76%
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04 0.06%
A7035 0.1155849542 $32.36 $25.89 $2.99 4.11%
A7034 0.1070640535 $106.46 $85.17 $9.12 12.54%
A7032 0.0623698474 $36.68 $29.34 $1.83 2.52%
A7033 0.0496539111 $25.71 $20.57 $1.02 1.40%
A7039 0.0458239180 $11.79 $9.43 $0.43 0.59%
A7030 0.0418602648 $170.72 $136.58 $5.72 7.86%
E0562 0.0303565011 $272.60 $218.08 $6.62 9.10%
E0601 0.0296715848 $1,011.00 $808.80 $24.00 33.00%
A7031 0.0219373840 $63.14 $50.51 $1.11 1.52%
A7046 0.0175893653 $17.66 $14.13 $0.25 0.34%
A7036 0.0122401256 $14.00 $11.20 $0.14 0.19%
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10 13.89%
A4604 0.0011388196 $60.46 $48.37 $0.06 0.08%
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44 6.11%
E0561 0.0004612878 $96.84 $77.47 $0.04 0.05%
A7045 0.0003492889 $17.62 $14.10 $0.00 0.01%
A7044 0.0001718137 $109.42 $87.54 $0.02 0.02%
A7037 0.1231723257 $35.73 $28.58 $3.52 4.84%
Composite Bid: $72.72
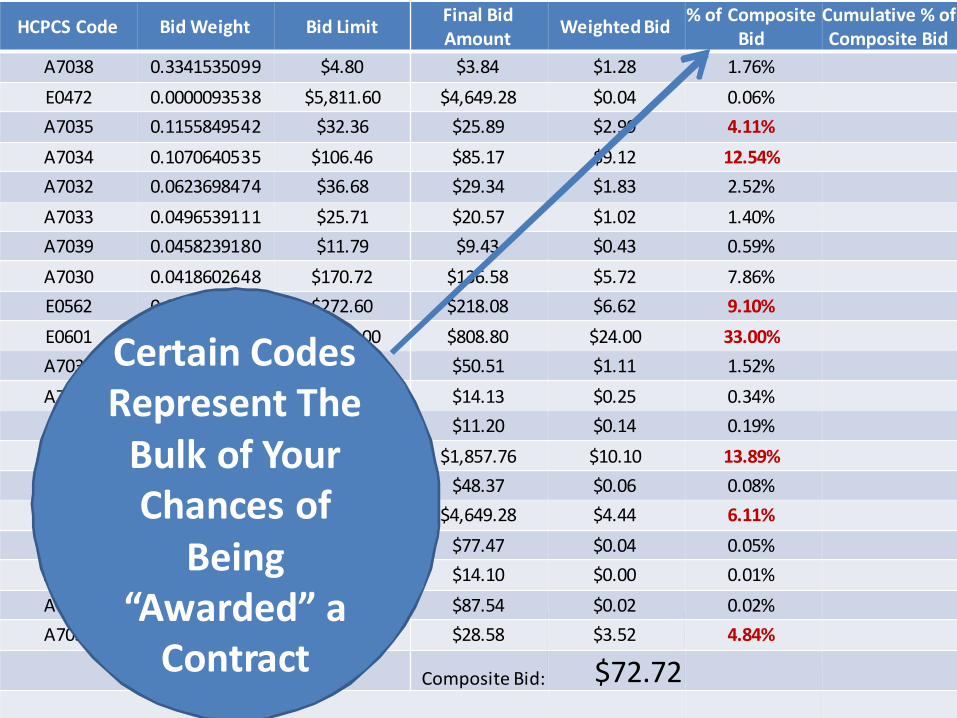
Certain CodesRepresent The
Bulk of YourChances of
Being“Awarded” a
Contract
HCPCS Code Bid Weight Bid LimitFinal BidAmount
Weighted Bid% of Composite
BidCumulative % ofComposite Bid
E0601 0.0296715848 $1,011.00 $808.80 $24.00 33.00% 33.00%
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10 13.89% 46.89%
A7034 0.1070640535 $106.46 $85.17 $9.12 12.54% 59.43%
E0562 0.0303565011 $272.60 $218.08 $6.62 9.10% 68.53%
A7030 0.0418602648 $170.72 $136.58 $5.72 7.86% 76.39%
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44 6.11% 82.50%
A7037 0.1231723257 $35.73 $28.58 $3.52 4.84% 87.34%
A7035 0.1155849542 $32.36 $25.89 $2.99 4.11% 91.45%
A7032 0.0623698474 $36.68 $29.34 $1.83 2.52% 93.97%
A7038 0.3341535099 $4.80 $3.84 $1.28 1.76% 95.74%
A7031 0.0219373840 $63.14 $50.51 $1.11 1.52% 97.26%
A7033 0.0496539111 $25.71 $20.57 $1.02 1.40% 98.66%
A7039 0.0458239180 $11.79 $9.43 $0.43 0.59% 99.26%
A7046 0.0175893653 $17.66 $14.13 $0.25 0.34% 99.60%
A7036 0.0122401256 $14.00 $11.20 $0.14 0.19% 99.79%
A4604 0.0011388196 $60.46 $48.37 $0.06 0.08% 99.86%
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04 0.06% 99.92%
E0561 0.0004612878 $96.84 $77.47 $0.04 0.05% 99.97%
A7044 0.0001718137 $109.42 $87.54 $0.02 0.02% 99.99%
A7045 0.0003492889 $17.62 $14.10 $0.00 0.01% 100.00%
Composite Bid: $72.72
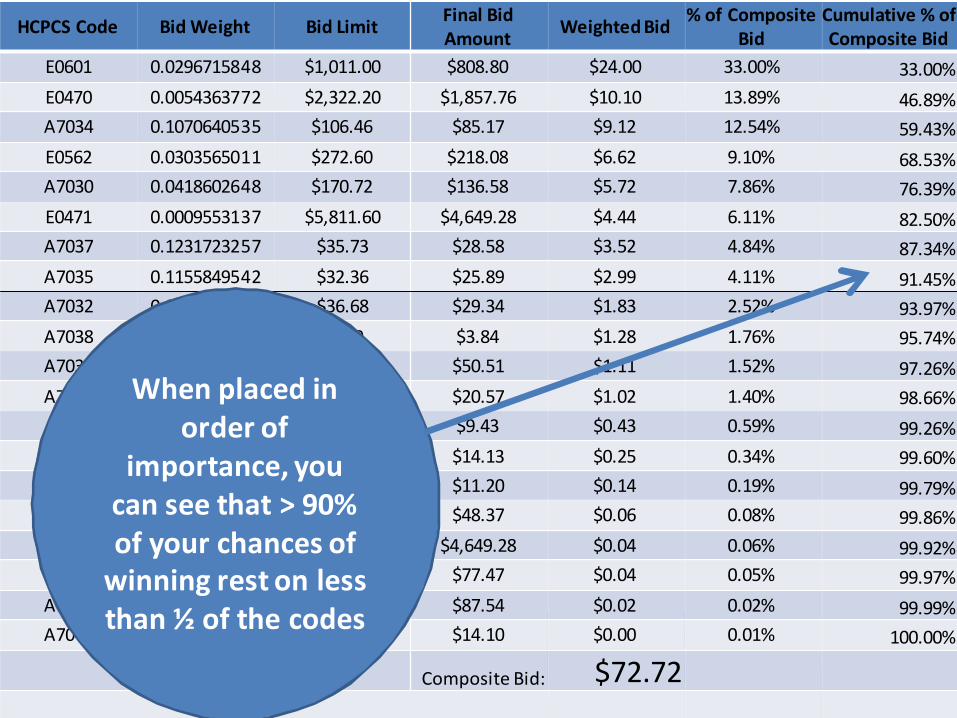
When placed inorder of
importance, youcan see that > 90%of your chances of
winning rest on lessthan ½ of the codes

HCPCS Code Bid Weight Bid LimitFinal BidAmount
Weighted Bid% of Composite
BidCumulative % ofComposite Bid
E0601 0.0296715848 $1,011.00 $808.80 $24.00 33.00% 33.00%
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10 13.89% 46.89%
A7034 0.1070640535 $106.46 $85.17 $9.12 12.54% 59.43%
E0562 0.0303565011 $272.60 $218.08 $6.62 9.10% 68.53%
A7030 0.0418602648 $170.72 $136.58 $5.72 7.86% 76.39%
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44 6.11% 82.50%
A7037 0.1231723257 $35.73 $28.58 $3.52 4.84% 87.34%
A7035 0.1155849542 $32.36 $25.89 $2.99 4.11% 91.45%
A7032 0.0623698474 $36.68 $29.34 $1.83 2.52% 93.97%
A7038 0.3341535099 $4.80 $3.84 $1.28 1.76% 95.74%
A7031 0.0219373840 $63.14 $50.51 $1.11 1.52% 97.26%
A7033 0.0496539111 $25.71 $20.57 $1.02 1.40% 98.66%
A7039 0.0458239180 $11.79 $9.43 $0.43 0.59% 99.26%
A7046 0.0175893653 $17.66 $14.13 $0.25 0.34% 99.60%
A7036 0.0122401256 $14.00 $11.20 $0.14 0.19% 99.79%
A4604 0.0011388196 $60.46 $48.37 $0.06 0.08% 99.86%
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04 0.06% 99.92%
E0561 0.0004612878 $96.84 $77.47 $0.04 0.05% 99.97%
A7044 0.0001718137 $109.42 $87.54 $0.02 0.02% 99.99%
A7045 0.0003492889 $17.62 $14.10 $0.00 0.01% 100.00%
Composite Bid: $72.72
Notice that themost impactful
codes aren’tnecessarily thosewith the highest“Bid Weight” or
“Bid Limit”. It’s thecorrelation
between the twothat’s mostimportant.

HCPCS Code Bid Weight Bid LimitFinal BidAmount
Weighted Bid% of Composite
BidCumulative % ofComposite Bid
E0601 0.0296715848 $1,011.00 $1,000.00 $29.67 37.85% 37.85%
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10 12.88% 50.73%
A7034 0.1070640535 $106.46 $85.17 $9.12 11.63% 62.36%
E0562 0.0303565011 $272.60 $218.08 $6.62 8.44% 70.81%
A7030 0.0418602648 $170.72 $136.58 $5.72 7.29% 78.10%
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44 5.67% 83.76%
A7037 0.1231723257 $35.73 $28.58 $3.52 4.49% 88.26%
A7035 0.1155849542 $32.36 $25.89 $2.99 3.82% 92.07%
A7032 0.0623698474 $36.68 $29.34 $1.83 2.33% 94.41%
A7038 0.3341535099 $4.80 $3.84 $1.28 1.64% 96.04%
A7031 0.0219373840 $63.14 $50.51 $1.11 1.41% 97.46%
A7033 0.0496539111 $25.71 $20.57 $1.02 1.30% 98.76%
A7039 0.0458239180 $11.79 $9.43 $0.43 0.55% 99.31%
A7046 0.0175893653 $17.66 $14.13 $0.25 0.32% 99.63%
A7036 0.0122401256 $14.00 $11.20 $0.14 0.17% 99.80%
A4604 0.0011388196 $60.46 $48.37 $0.06 0.07% 99.87%
E0472 0.0000093538 $5,811.60 $4,649.28 $0.04 0.06% 99.93%
E0561 0.0004612878 $96.84 $77.47 $0.04 0.05% 99.97%
A7044 0.0001718137 $109.42 $87.54 $0.02 0.02% 99.99%
A7045 0.0003492889 $17.62 $14.10 $0.00 0.01% 100.00%
Composite Bid: $78.40
Notice whathappens when
your bid forE0601 is
changed from$808.80 to$1,000.00
Composite Bidjumped from
$72.72 to$78.40

HCPCS Code Bid Weight Bid LimitFinal BidAmount
Weighted Bid% of Composite
BidCumulative % ofComposite Bid
E0601 0.0296715848 $1,011.00 $808.80 $24.00 32.34% 32.34%
E0470 0.0054363772 $2,322.20 $1,857.76 $10.10 13.61% 45.95%
A7034 0.1070640535 $106.46 $85.17 $9.12 12.29% 58.24%
E0562 0.0303565011 $272.60 $218.08 $6.62 8.92% 67.17%
A7030 0.0418602648 $170.72 $136.58 $5.72 7.71% 74.87%
E0471 0.0009553137 $5,811.60 $4,649.28 $4.44 5.99% 80.86%
A7037 0.1231723257 $35.73 $28.58 $3.52 4.75% 85.60%
A7035 0.1155849542 $32.36 $25.89 $2.99 4.03% 89.63%
A7032 0.0623698474 $36.68 $36.31 $2.26 3.05% 92.69%
A7038 0.3341535099 $4.80 $4.75 $1.59 2.14% 94.83%
A7031 0.0219373840 $63.14 $62.51 $1.37 1.85% 96.68%
A7033 0.0496539111 $25.71 $25.45 $1.26 1.70% 98.38%
A7039 0.0458239180 $11.79 $11.67 $0.53 0.72% 99.10%
A7046 0.0175893653 $17.66 $17.48 $0.31 0.41% 99.51%
A7036 0.0122401256 $14.00 $13.86 $0.17 0.23% 99.74%
A4604 0.0011388196 $60.46 $59.86 $0.07 0.09% 99.83%
E0472 0.0000093538 $5,811.60 $5,753.48 $0.05 0.07% 99.91%
E0561 0.0004612878 $96.84 $95.87 $0.04 0.06% 99.97%
A7044 0.0001718137 $109.42 $108.33 $0.02 0.03% 99.99%
A7045 0.0003492889 $17.62 $17.44 $0.01 0.01% 100.00%
Composite Bid: 74.20
Instead, what ifwe simply raisethe “irrelevant”
codes to 1%below Bid Limit
Composite Bidmoved from
$72.72 to$74.20
The Conclusion from this Analysis…
• …is that your bid strategy should be focused on asmall number of HCPCS codes within a given ProductCategory. The majority of included HCPCS codeshave such a minimal impact on the biddetermination as to be practically irrelevant.
• Discounting items with small Bid Values will not likelyhelp you win a bid but will almost certainly hurt youwhen the winning bid rate (fee schedule) isdetermined for each of the HCPCS codes within theProduct Category.
How Much Are Winning Bidders Paid?
• Once the winning bidder pool has been set,CMS can determine “Single PaymentAmounts”
• By HCPC code, the Single Payment Amount isset at the median bid of all winning bidders
• We will send each of you the “actual” bidworksheets upon their release by the CBICAND our “what if” worksheet tool to allow youto note and evaluate the true weight of eachcode.
• The worksheet tool will include “warning”colors for codes with high weights and also forbids that may trigger a bona fide (e.g., toolow) challenge and/or prevent typos.


• Morning Break…

Competitive Bidding:Part 2 – 2015 and Beyond…
The Affordable Care Act amended the MedicareModernization Act statute to mandate use of informationfrom the DMEPOS competitive bidding program to adjust
the fee schedule amounts for DME in areas wherecompetitive bidding programs are not implemented by no
later than January 1, 2016.
Before we get too far, let’s review anexcellent source of a real-time DME
provider locator tool…Start Here:


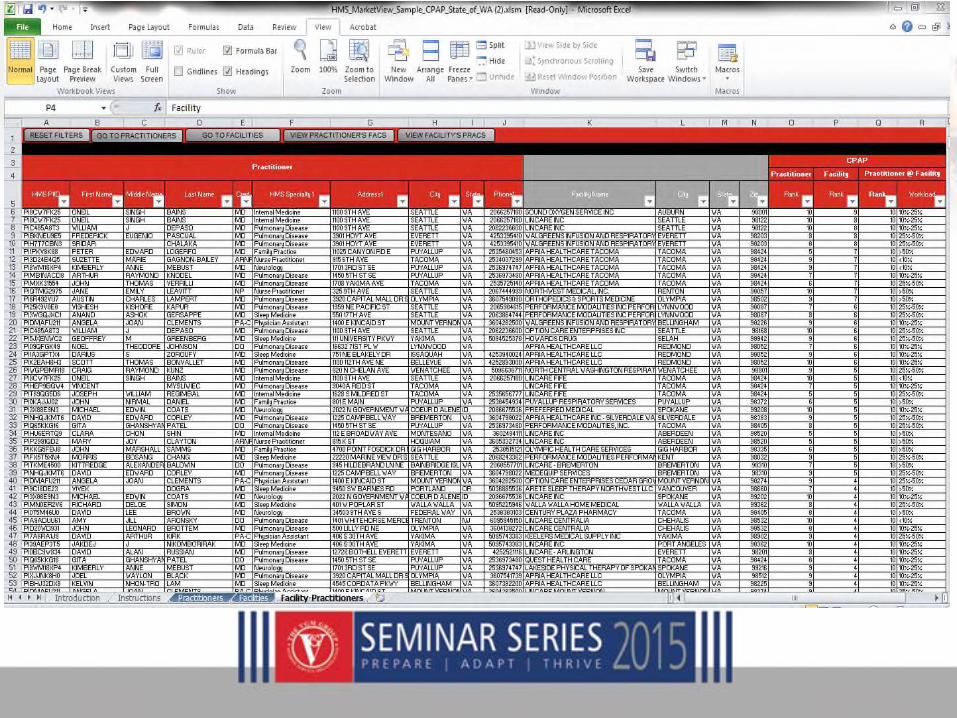
This spreadsheet may be copied/edited and iseasily manipulated via the Data/Sort function.
• For example, you may wish to copy a certain state orregion and obtain a listing of all suppliers in the areaby city for member prospecting, insurance, referrals,advocacy, and many other potential reasons.
• You can also sort these locations as to whichsuppliers offer certain products…for example CPAP.
• There are 80 product categories in which the NSCrecognizes and updates via the 855S format.

• Many full line suppliers offer dozens of products.Some niche suppliers (think opticians who offercataract sunglasses) may only be in one or twocategories. You will be able to sort these out by atool I reference below.
• The first 21 (A to X) identify the supplier bylocation/contact detail and to whether thesupplier has any competitive bid contracts. It alsoincludes a column (X) as to whether the entity is aparticipating Medicare supplier. See next slides...

EXCEL
ROW
A Competitive Bid Service Area
B Company Name
C DBA Name
D Address
E Address 2
F City
G State
H Zip
I Zip Plus 4
J Phone
K Oxygen Supplies and Equipment
L Mail-Order Diabetic Supplies
M Enteral Nutrients, Equipment and Supplies
N CPAP Devices, Respiratory Assist Devices, and Related Supplies and Accessories
O Hospital Beds and Related Accessories
P Negative Pressure Wound Therapy Pumps and Related Supplies and Accessories
Q Walkers and Related Accessories
R Support Surfaces (Group 2 mattresses and overlays)
S Standard (Power & Manual) Wheelchairs, Scooters, and Related Accessories
T External Infusion Pumps and Supplies
U General Home Equipment and Related Supplies and Accessories
V Respiratory Equipment and Related Supplies and Accessories
W Standard Mobility Equipment and Related Accessories
X Is Supplier Participating?

Example: Suppliers in Baldwin, CA; associated CBAs and to which contracts
(YES or NO) these suppliers have:
• Beginning with Column K (this is Oxygen Supplies andEquipment) the data option is either NO or YES.
• If NO this supplier has no competitive bid contract.
• If YES then the supplier (in this location) has acompetitive bid contract for that product category.
• Both Round 1 recompete and Round 2 productcategories follow in columns K through W.
• Remember there were differences in categoriesbetween these two rounds. At column X thecompetitive bid data set ends and, as noted, columnX is a YES or NO as to whether the supplier isparticipating.
The next series of columns include all 80product categories included within the
855S enrollment data.
• If the supplier location isaccredited/credentialed to bill Medicare forthe category, the indication is YES.
• If not NO.

Starting with Column Y and ending atColumn DA the products are as follows:

Automatic External Defibrillators (AEDS)
Commodes, Urinals , & Bedpans
Continuous Passive Motion (C PM) Devices
Dynamic Splints
Blood Glucose Monitors & Supplies: Non-Mail Order
Blood Glucose Monitors & Supplies: Mail O rder
Blood Glucose Monitors: Mail Order
Gastric Suction Pumps
Heat & Co ld Applications
Hospital Beds: Electric
Hospital Beds: Total Electric & Pediatric
Hospital Beds: Manual
Hospital Beds: Manual & Pediatric
Infrared Heating Pad Systems
Infusion Pumps &Supplies: External Infusion
Infusion Pumps: Implantable & Uninterrupted
Infusion Pumps &Supplies: Insulin Infusion
Infusion Pumps &Supplies: Implanted Infusion
Negative Pressure Wound Therapy Pumps & Supplies
Neuromuscular Electrical Stimu lato rs (NMES)
Osteogenesis Stimulators
Pneumatic Compres sion Devices
Speech Generating Devices
Support Surfaces: Pressure Reducing Beds, Mattresses, Overlays, & Pads
Support Surfaces (e.g. Air Fluidized bed)
Traction Equipment
Transcutaneous Electrical Nerve Stimulators (TENS) Units
Ultraviolet Light Devices
Home Dialysis Equipment & Supplies
Hemo dialysis Equipment &Supplies
Canes & Crutches
Patient Lifts
Power O perated Vehicles (Scoo ters)
Seat Lift Mechanisms
Walkers
Wheelchairs & Accessories: Standard Manual
Wheelchairs & Accessories: Standard Manual (e.g. Pediatrics)
Wheelchairs & Accessories: Standard Power
Wheelchairs & Accessories: Standard Power (e.g. Pediatrics and custom cushions )
Wheelchairs & Accessories: Complex Rehabilitative Manual
Whe elch air Seating/Cush ions
Whe elch air Seating/Cush ions (e.g. skin protecting seat cushions)
Orthoses: Custom Fabricated
Orthoses: Prefabricated
Orthoses: Off-the-Sh elf
Breast Prostheses & Accessories
Cochlear Implants
Facial Pro stheses
Neurostimulator s
Ocular P rostheses
Osto my Supp lies
Somatic Prostheses
Trach eostomy Suppl ies
Urological Suppl ies
Vo ice Prosthetics
Prosthetic Lenses: Convention al Eyeglasses
Prosthetic Lenses: Convention al Co ntact Lenses
Prosthetic Lenses:P rosthetic Cataract Lenses
Enteral Nutrient s, Equipment, & Supplies
Enteral Nutrient s& Su ppliesfor SpecialMet abo lic Needs and Pediatrics
Parenteral Nutrients, Equipmen t & Sup plies
Limb Pro stheses
Eye Prostheses
CPAP, RADs,& Related Supplies & Accesso ries
CPAP and RADs Suppl ies (e.g. combination masks)
High Frequ ency C hest Wall Oscillation (HFCWO) Devices
In vas ive Mechanical Ventilation
In termittent Posi tive Pressure B reathing (IPPB) Devices
In trapulmon ary Percussive Venti lation Devices
Mechanical In-Exsufflation Devices
Nebul izer Equip men t & Supp lies
Nebul izer Equip men t: Ultrasonic and Co ntrolled Dose
Oxygen Equipment & Suppl ies
Respiratory Suctio n Pumps
Ven tilators , Accessories& Supplies
SurgicalDressings
DiabeticSho es & Inserts: Prefabricated
DiabeticSho es & Inserts: Custom Fabricated
Now, I recognize that much data maybe difficult to comprehend (!!!)
• What you could do is select just a state or region,and copy it into another blank spreadsheet. Then,using the find and replace function, highlight fromColumn Y and all through the 80 other productcolumns and “find” all the “NO” cells.
• Replace it with a blank (insert nothing). Now thereare many cells with nothing in them and will beignored.
• Do the same thing with the YES “find” but replace itwith a 1 (one).

• Then highlight all of the product category columns, and, in thenext one to the right of all of them, use the “count” function.
• I will show you an example next, but it is merely @count(rownumber cell number..row number cell number) and copied allthe way down.
• This will give you how many categories this supplier location iseligible to bill.
• Then you can resort the entire list of suppliers from top tobottom by number of categories. Those suppliers “on top”(with the most categories) are likely your competitors or HMEsof interest. The ones at the bottom (with just a few) are likelyopticians or niche suppliers.

• As an example, I copied all of the Iowa DMEPOSsuppliers from the master spreadsheet.
• I then followed the instructions above andeliminated from any “counting” all of the Iowalocations with NO in the product columns by aFind and Replace.
• I did the same thing with YES, and then used the@count function to array them from top tobottom. (I inserted a new column next to thecompany name – B – and titled it “Yes’s –meaning that is the number of YES results Isorted.)
• Here is a sample of what I received…

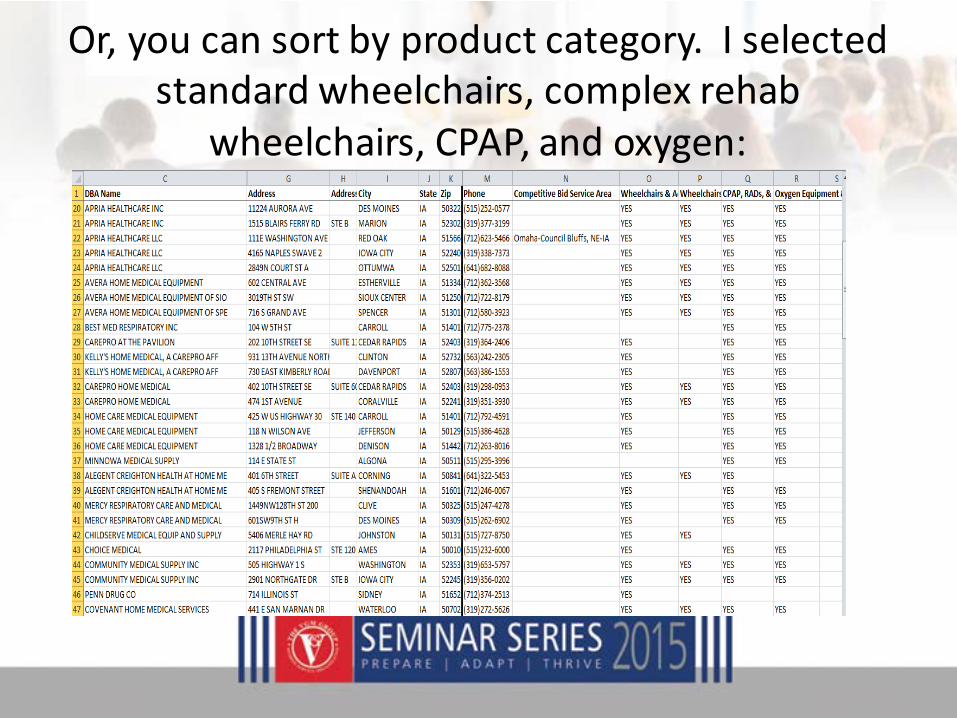
Or, you can sort by product category. I selectedstandard wheelchairs, complex rehab
wheelchairs, CPAP, and oxygen:
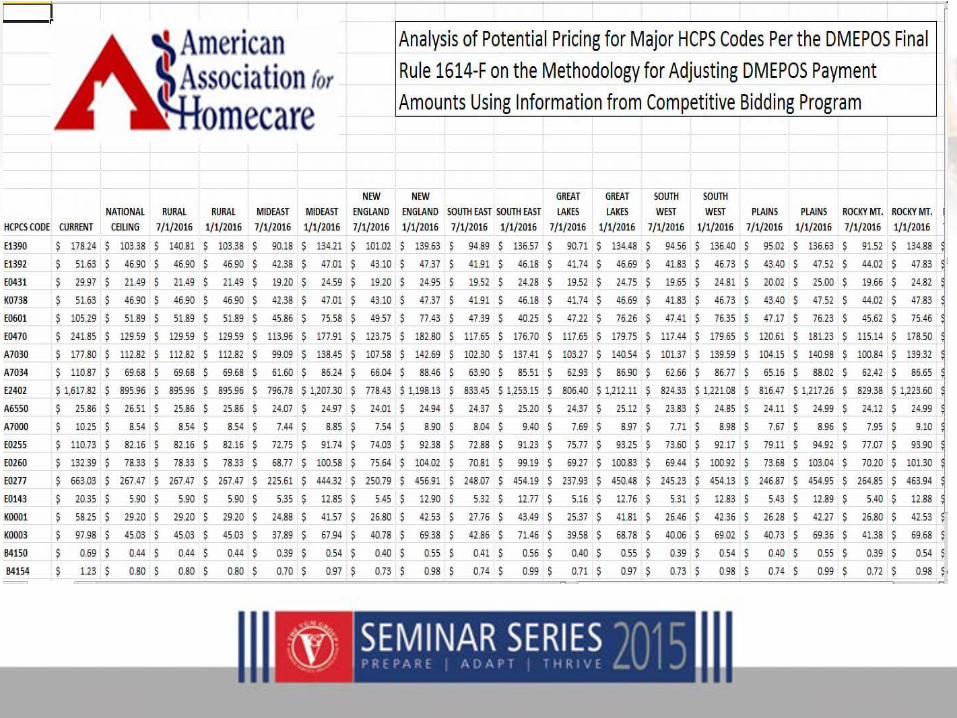
CMS-1614-P is now FINAL!• The Affordable Care Act amended the Medicare Modernization
Act statute to mandate use of information from the DMEPOScompetitive biddingprogram to adjust the fee schedule amountsfor DME in areas where competitive biddingprograms are notimplemented by no later than January 1, 2016.
• CMS estimates that by applyingbid rates throughout the entireUnited States it would save over $7 billion over FY 2016 through2020.
• This obviously affects the non-metro regions of Tennessee andthe adjoiningstates!


DME Provisions…
• Proposed (changes to) the methodology for makingnational price adjustments based upon informationgathered from (all previous) competitive biddingprogram (CBPs).
• And…A proposed phase in of “special payment rules”(bundling) in to-be-determined 12 metro areas.

“National” Pricing• How? Adjust fee schedule amounts for states in different regions
of the country based on previous competitive bidding roundpricing in these “regions”.
• The regional prices would be limited by a national ceiling (110%of the average of regional prices) and floor (90% of the averageof regional prices)
• There were three possible “Regions” (see next)
• Most attendees here today service the “Mideast” BEA region.


• CMS determines a regional price for each state equalto the average of the single payment amount for anitem or service from the CBAs that are fully orpartially located in the same region where the stateis located.
• CMS determines a national average price equal tothe average of the regional prices.
• The regional price cannot be greater than 110percent of the national average nor less than 90percent of the national average price.
• Adjust fee schedules annually using CPI-U
• Revise the SPA each time there is a new roundof bidding.
• Use national ceiling for rural states and outsidecontiguous US.

• “Although we believe that the costs of furnishing items andservices in rural areas are different than the costs offurnishing items and services in urban areas, there is noevidence to support a statement that the difference in costs issignificant.
• However, in order to proceed cautiously on this matter in theinterest of ensuring access to covered DMEPOS items andservices, we are proposing to phase in the price adjustments,as explained below, so that we can monitor the impact of theadjustments as they are gradually phased in.”
While not released…
• We have the current SPAs in all markets fromthe current programs.
• As CMS has provided us the methodology todetermine the regional payment amounts(RSPAs), and has confirmed that the “BEA”regional array will be utilized, we can hencedetermine the RSPAs now.
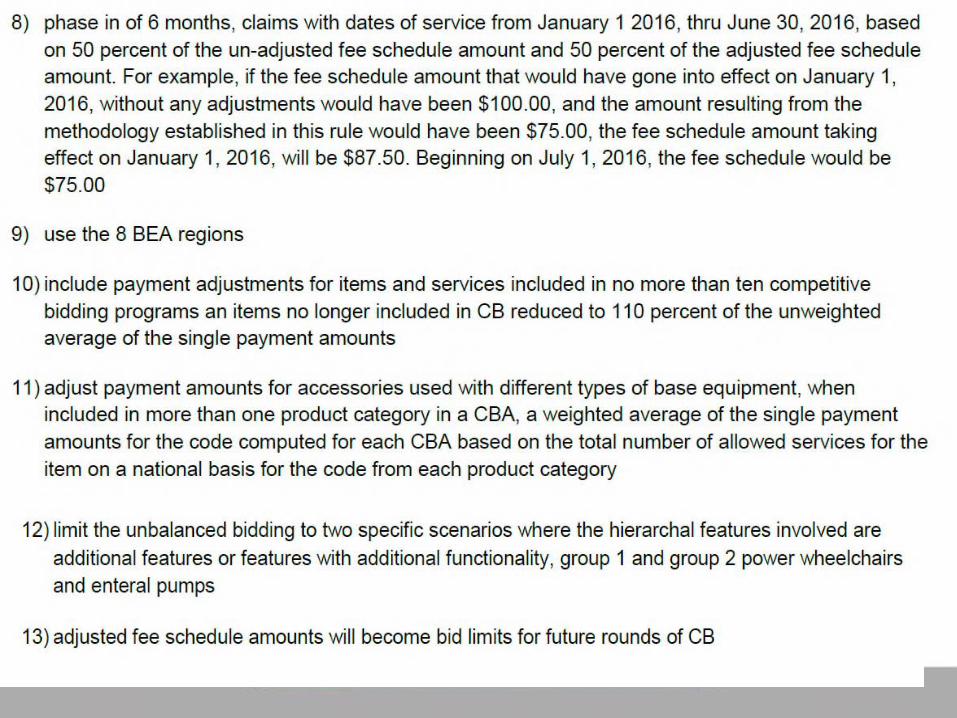
Summary of Provisions• The new adjusted pricing for DMEPOS CBP items will
begin on January 1, 2016. This will be a phase-inprocess over 6 months, allowables will be reduced by50% on 1/1/16 and 100% on 7/1/16.
• CMS finalized a pricing methodology for non-competitive bidding areas.
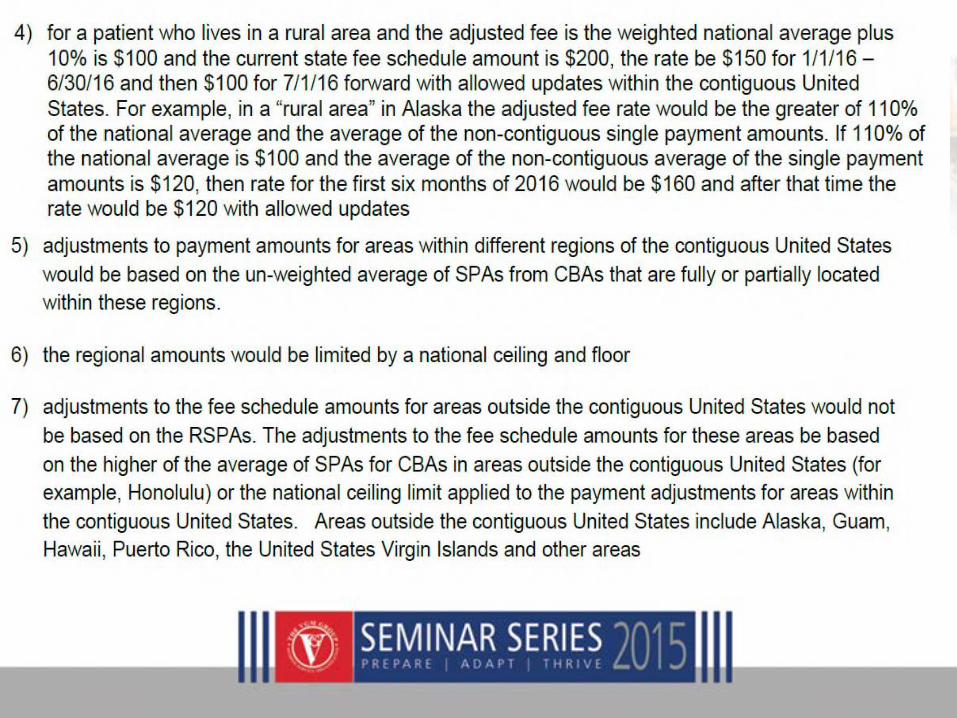
• A rural area will be defined as a postal zip code that hasmore than 50 percent of its geographic area outside ofa metropolitan area (MSA) or a zip code that has a lowpopulation density area that was excluded from acompetitive bidding area. The payment amount will be110 percent of the average of the SPAs of all the areaswhere CBPs are implemented.

• Let’s use an example.
• A fictional HME provider has asked me what thereimbursement would be in Massachusetts’Rockingham or Strafford counties for a month ofoxygen after July 1, 2016…
• These counties are in the Boston MSA but NOTincluded in the CBA (bid area).
• Massachusetts is in the New England region.
• Using the averages of the oxygen single paymentamounts of all CBAs in this regions, thereimbursement would be: $101.02

• Lastly, how about a state that has NO CBAs?? CMSdubs these states as “rural” or “frontier”
• In this case the SPA would be 110% of the nationalaverage.
• In this case, if the HME operated in Montana,for example, the monthly payment would be$103.38

Can we determine (now) the actualRSPAs?
• Yes! AAH Regulatory Council has created adocument which includes the high utilizationcodes. Go to:
http://vgmncbservices.com/Documents/RSPA-PricingAnalysis.xlsx

Summary…
Next: “Bundling”…
• This is a limited phase in (12 areas) of bundledmonthly payment amounts for the equipment,supplies, accessories, maintenance and repairs forenteral nutrition, oxygen, standard wheelchairs,hospital beds, CPAP/RAD in place of capped rentalpolicies.
• Bidding would start sometime after 1/1/2015.
• The SPA is based on bids submitted and accepted on amonthly basis for each month of medical need during thecontract period.
• Monthly single payment amount would include paymentfor all nutrients, supplies and equipment.
• Payment is made on a continuous monthly rental basisfor DME. The SPA Includes rent, maintenance andservice, and replacement of supplies and accessoriesnecessary.
• No separate payments for M&S

• CMS is moving forward with a limited versionof its proposed bundling phase-in.
• CMS will move forward with a bundling forpower wheelchairs and CPAP in up to 12markets.
• CMS did not move forward with bundling for:oxygen, standard manual wheelchairs, enteralnutrition, RADs, and hospital beds.

Summary…


Industry Arguments:
• CMS’ reliance on an 18 year old study was surprisinginasmuch as we stated in our comments on the ANPRM(proposed rule) that suppliershave closed facilities in hard-to-service areas because they can no longer offset the cost ofrunning these locationswith revenue from other branches.
• This is a tangible threat to access for beneficiaries outsideCBAs and a direct result of the austere payment rates underthe biddingprogram.
• We know that CMS recognizes geographic cost differencesunder payment systems that include “add-on” payments toreconcile those differences.

• We believe that CMS has access to data that would support add-onpayments for DMEPOS suppliers in rural and “frontier” areas. Werecommend that CMS incorporate supplemental payments in theform of add-ons to the basic reimbursement rate in areas outsideCBAs.
• “We are worried and alarmed because CMS has not thoughtthrough the possible ramificationsof this type of program and plansto move forwarddespite the lack of information. As far as we know,CMS has not determined how to align the needs of beneficiarieswith chronic, progressive conditionswith different bundles ofequipment, supplies and services.
• Unlike the home health or the skilled nursing facility (SNF)prospective payment systems (PPS), this proposal lacks anymechanism to tie the medical needs of the patient to the paymentfor the items and services he or she needs.
• On the contrary, the sole purpose of the proposed changes is drivethe price for DME and enteral products as far down as possible.”

Lunch!
Human Resource Management- Keys to Retention Success -
Consider the Fact –Your companies greatest asset is its employees…
What is the value of this asset?An employee making $38,500a year leaves your company.
It takes you a minimum of $4,648.40to hire and train a replacement employee.
http://us.drakeintl.com/hr-tools/cost-of-turnover-calculator.aspx

Monetary Costs of Turnover
•The cost of hiring a new employee includes: theadvertising, interviewing, screening, and hiring cost to findthis new employee.
•Cost of on-boarding a new person includes training andmanagement time. For example, over 2-3 years a businesslikely invests 10-20% of an employee's salary or more intraining.
•The cost of lost productivity... it may take a new employee1-2 years to reach the productivity of an existing person.

Non-Monetary Costs of Turnover
•Lost engagement... other employees who experience highturnover tend to disengage and lose productivity.
•Customer service and errors; for example new employeestake longer and are often less adept at solving problems.
•Cultural impact... Whenever someone leaves others taketime to ask "why?"
For businesses to thrivein today’s economy,
finding and retaining thebest employees is important.
This is especially true forsmall businesses competing
with larger businesses,and larger budgets,
for top talent.
The Retention Process Starts with Recruitmentand Follows the Entire Employee Life Cycle
We currently work in an environmentwhere retention is driven by the employee:• Pay for Performance and Experience• Increased Relocatability• Advancement Opportunities• Employees Leave Managers
More Often Than Companies
Often it’s Human Resources professionals who focus theirattention on the steps in this process in hopes of making animpact on the company's bottom line.
Unfortunately, HR is not the ones who really make adifference – managers are. People don't really work forcompanies; they work for a boss. To the extent that you canbe a good boss, you can keep employees, keep them happy,and reduce the costs and headaches associated withemployee turnover.
Supervisors, Managers and Owners,
- YOU -affect employee success and longevity the most.

How do you make an impact in theEmployee Life Cycle?
Don’t start whenit’s too late
Start before their evenhired and don’t stop

We’re Going to Talk About Retention Within EachPhase of the Employee Life Cycle
Attracting TalentSourcing TalentSelecting TalentTalent Selling
Developing TalentOnboarding
Continuing EducationPerformance Appraisals
Retaining TalentBest Fit for the Skill Set
Succession DevelopmentCoaching
Attracting TalentHiring Rock Stars not Future Former Employees
Consider hiring decisions that make you cringe?
• Did you play a part in hiring all your direct reports?• Do you wish you had…• Would you hire them today…• Would you hire someone you didn’t…
Why didn’t you have a key role in hiring theseindividuals?
•Recruiting is relationship building.•Do you have recruiting cards (not business cards)?•Do you engage your top talent in recruiting?
•Are they compensated for this?•Do you use talent solution agencies?
•What does that entail?•What communication avenues do you recruit through?(job posting sites, organizations etc.)•Source for soft skills and train the hard skills.
• In others words - hire for fit and train for skill
Attracting Talent: Talent Sourcing
Attracting Talent: Talent Selection
Interview Process
•Who’s Involved?•Interview Process Outline -
•Phone Screen, On-site Interview, Reference Check, Offer•Job Shadowing, is this valuable?•Background checks and what you need to know.

Think of the age generation you’re recruiting and how youmarket your company to them.
Quantifiable Benefits Unquantifiable Benefits
Health Benefits Unique Company Culture & Values
Personal Time ESOP
Incentive Pay Long-term Stability
401k Dress Code
Day Care Fitness Center or Programs
Attracting Talent: Talent Selling

Developing Talent
We like to believe it's caused by money & benefits…
The reality is:No Possibility of AdvancementLack of Recognition & RespectDesire for Meaningful, Challenging WorkPoor Work Environment
Reasons Employees Leave Companies

Developing Talent: Onboarding
Training For Success
•Have a plan prepared for training, demonstrate to thenew employee that you were ready for their arrival.•Initiate an Ambassador/Mentor Program; pair a newemployee with a tenured, high performing employee.•Perform 30/60/90 day evaluations.•Set a probationary period as a fail-safe.
Developing Talent: Continuing Education
Ongoing Training
•Yearly Continuing Education Requirements•Company Initiated•Employee Requested
•Tuition Reimbursement Opportunities•Leadership Programs for
•Up-and-Coming Leaders•Current Leaders
Developing Talent: Continuing Education
This is where you really can impact an employeesperception of the retention factors:
•No Possibility of Advancement•Lack of Recognition & Respect•Desire for Meaningful, Challenging Work
With the implementation of leadership programs thatrequire employees to apply and show interest you’ll set ahigher standard. Selection of participants is then done byexecutives or higher level leaders.

Developing Talent: Performance Appraisals
Consistently giving feedback shows an employee they areperforming meaningful work.
Consider these ways of improving feedback:•Employee self-review prior to the manager review,shows misperceptions of performance expectations.•360° feedback provides a well rounded view ofperformance.•Do not give merit increases at the same time asreviews.•Set goals at the beginning of each review cycleintended for review the following year.

Retaining Talent
Succession PlanningIt sounds great when verbalized, but until action isdone succession planning doesn’t bring value to anemployee.
Think Succession Development – identify areaswhere successors are needed and target employeesfor development.

•Identify positions critical to the organization•Skills and traits needed for these positions are recognized•Target employees as potential successors – communicatethis message to them•Individual employee skill deficiencies are recognized anddevelopment plans created
Retaining Talent:Succession Planning and Development
How to begin:
•Set up mentor programs•Introduce top talent across the company•Host Operational Leadership Ranking (OLR) meetings•Assign top talent stretch assignments•Engage top talent in new activities
Retaining Talent:Succession Planning and Development
Action Items:

Retaining Talent:Succession Planning and Development
•Identify displaced talent and find the right seat on the bus•Be transparent•Worse case: Coach Up or Coach Out
•Document, Document, Document
Not every targeted employee is the right candidate for afuture leadership role.
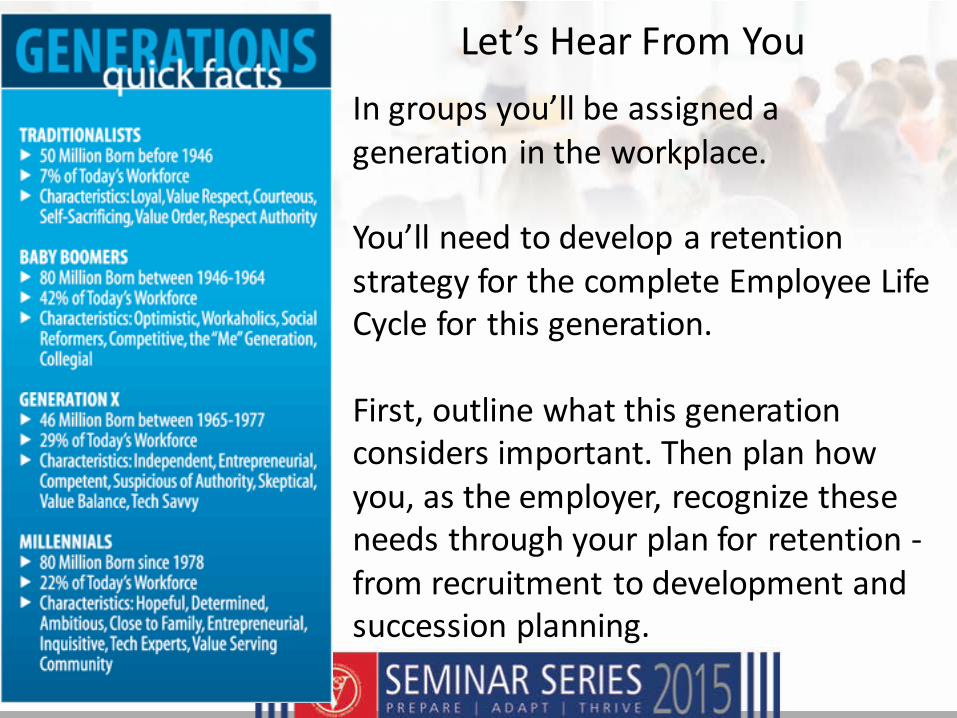
Let’s Hear From You
In groups you’ll be assigned ageneration in the workplace.
You’ll need to develop a retentionstrategy for the complete Employee LifeCycle for this generation.
First, outline what this generationconsiders important. Then plan howyou, as the employer, recognize theseneeds through your plan for retention -from recruitment to development andsuccession planning.
Wishing you Retention Succession in 2015 and Beyond
Part 3: How a non-contractHME can enter the
“competitive bid” arena
Used with permission - Brown and Fortunato, Inc.










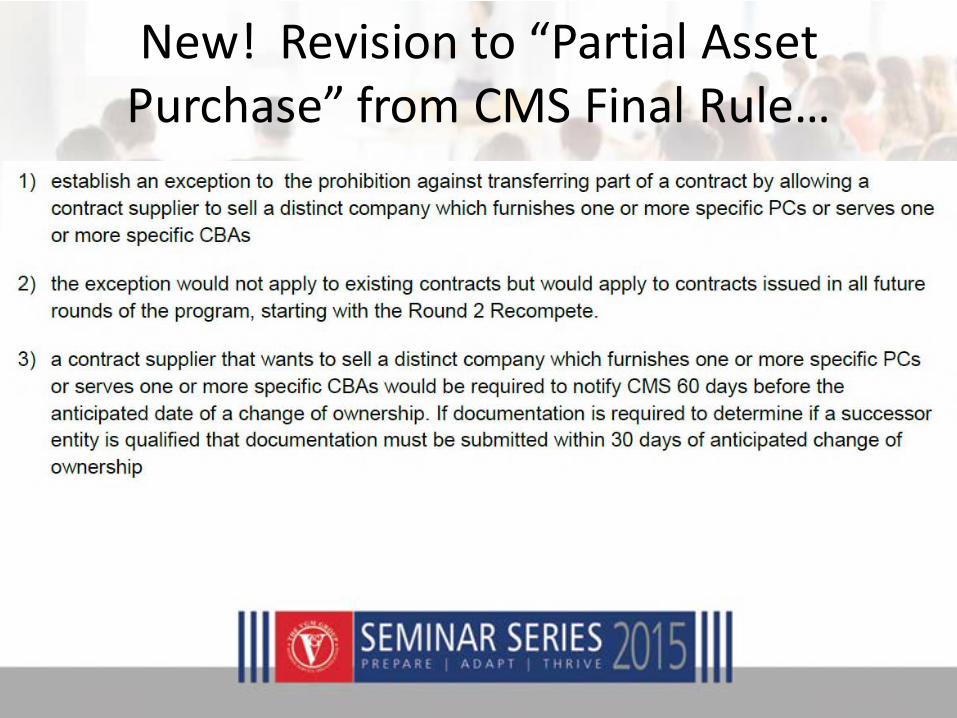
New! Revision to “Partial AssetPurchase” from CMS Final Rule…





What can VGM do for you?
Presented by: Gloria Murray
VGM & Associates

WHAT CAN VGM DO FORYOU?
Audit & Compliance Consultation - The van Halem Group• Merged with VGM in June, 2014
• Various audit protection programs
Reimbursement Training Program – U.S. Rehab• Basic – The basics in the DMEPOS fundamentals for delivery technicians, intake, customer service,
clinicians, repair technicians, and billing department
• Master – The fundamentals of detailed billing such as repairs, working audits, handling denials,and more for intake, customer service, managers, billing, auditing, compliance areas and themanagers/supervisors.

WHAT CAN VGM DO FORYOU?
Free Webinars
• Stay informed and educated on topics such as:
- Regulatory issues
- Billing and reimbursement
- Products and services

WHAT CAN VGM DO FORYOU?
Simplify CPAP Supply Re-Orders - VGM Fulfillment
• Process and ship CPAP supply orders directly to your patient
Maximize Cash Sales - Retail Services
• Comprehensive program designed to maximize retail sales

WHAT CAN VGM DO FORYOU?
Marketing Solutions
• Creative design and print services – VGM Creative & Strategic Imaging
• Educational marketing pieces for the consumer – Off the Shelf Marketing
• Promotional products and business apparel - Corporate Specialties
• Web design and online marketing – VGM Forbin

New!
VGM Market Data
Know your market!
• What is VGM Market Data?
• Who is Health Market Science?
• What type of data is available?
• How is Market Data different than traditionalDME data sources?
• How can you use Market Data?
• Questions
Overview
• VGM Market Data can provide data on thefollowing:
– Ranking of physicians that refer DME, specific toHCPCS code
– Which DME suppliers each physician works with
– What percentage of referrals from each physiciangoes to which DME supplier location
Key Deliverables

New VGM program designed to give members a market advantageover their competitors and drive growth opportunities
VGM exclusive agreement with Health Market Science to providetargeted physician and supplier referral data to independent DME’s
VGM is now exclusive sales channel for HMS data in DMEPOS up to$1billion
Specific knowledge of DME market data needs◦ Created targeted market views by most often billed HCPCS codes by
DME product category
What is VGM Market Data?

• Largest medical claims database in the US– ICD9 diagnosis and CPT codes– HCPCS product codes
• Data gathered from more than 2000 individualsources– Information on more than 8 million practitioners and 1.2
billion claims annually– Data provides the referring practitioner and supplier for
any HCPCS code or group of codes associated with aparticular product category/disease
– Data also ranks referring physicians in your market byvolume and ranks them according to supplier
Who is Health Market Science?

HMS has 250+ clients in healthcare market
24
Footer • Fixed Date [change this text via Insert tab>Header & Footer]
Working with industry leaders across all sectors of healthcare
Pharmacy/ PBMLife Sciences Healthcare Providers
Home Health & Hospice
Government
Payers and Health Plans

HMS Claims Universe - Capture and Coverage
Channels
› > 6,000 hospitals
› > 33,000 outpatient clinics
› > 15,000 LTC/Extended care facilities
› > 11,000 Home Health agencies
› > 3,000 Hospice Agencies
› > 50,000 DME Suppliers
› Physician offices representing 725,000community physicians
24
Footer • Fixed Date [change this text via Insert tab>Header & Footer]
The PxDx Solution Suite leverages the largest practitioner-level medical claimsdatabase in the industry
› Over 90% of practitioners in the non-retail setting.
› 40-80% of all adjudicated claims for those practitioners.
Metrics
› > 110 Million Unique Patients
› > 1.2 Billion Medical Claims
› >1.1 Million Unique Practitioners
› > 49 Million unique practitioner connectionsin our integrated Influence Network
Data Coverage
Capture Rate

Claims DataClaims DataClaims Data
Multiple Payers
Office PracticeManagement Software
Claims Switches/Clearinghouses
State Agencies
Where does this data come from?
PhysicianDiagnosis CodevsProduct HCPCSCode
Why does diagnosis matter?

BackBrace
Back Pain
Treat a lot of lowerback pain andprescribe brace
50%
Treat patientswith back pain,don’t prescribebrace
25%
Prescribeback bracewhen able
20%
Ignore!
High
High
Low
Opportunity!

V56.0
Drug Name & Strength, NDC: 12345-6789-01
01 06 03 01 06 03 11 1 99211 1 $$ $$
01 06 03 01 06 03 11 1 90782 1 $$ $$
01 06 03 01 06 03 11 1 J1055 1 $$ $$
123-45-6789 xxx xx
John Brown, M.D.111 Hospital DriveAnytown, USA 12345
123-45-6789 xxx xx
• Glean usefulinformation:
› Physician ID,diagnosesand procedurecodes, facilityID, etc
• Glean usefulinformation:
› Physician ID,diagnosesand procedurecodes, facilityID, etc
Health Care FinancingAdministration (HCFA) Claim Form
Drug Name & Strength, NDC: 12345-6789-01
01 06 03 01 06 03 11 1 99211 1 $$ $$
01 06 03 01 06 03 11 1 90782 1 $$ $$
01 06 03 01 06 03 11 1 J9010 1 $$ $$
123-45-6789 xxx xx
John Brown, M.D.111 Hospital Driv eAny town, USA 12345
123-45-6789 xxx xx
Diagnosis Code:ICD-9-CM code for appropriatediagnosis or nature of illness
Office Visit Code:CPT code for services providedto an established patient
Procedure Code:CPT code for an injection
Required: Drug CodeAppropriate HCPCS Drug Code
for medication administered
174 9
197 7
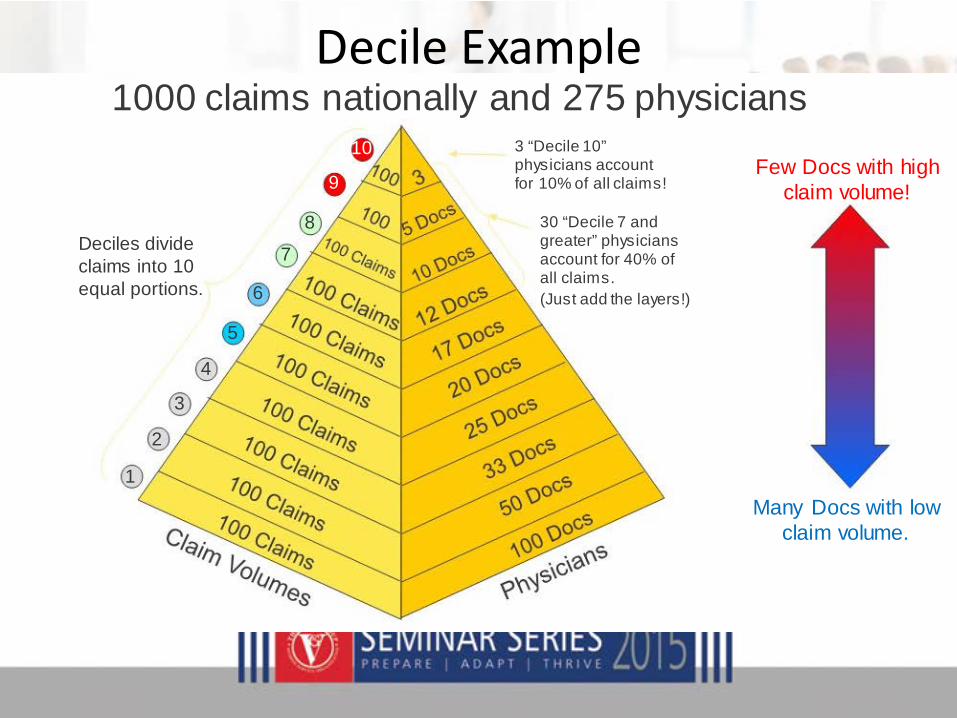
1000 claims nationally and 275 physicians
Deciles divideclaims into 10equal portions.
4
3
2
1
10
9
8
7
6
5
3 “Decile 10”physicians accountfor 10% of all claims!
30 “Decile 7 andgreater” physiciansaccount for 40% ofall claims.
(Just add the layers!)
Few Docs with highclaim volume!
Many Docs with lowclaim volume.
Decile Example

• Diversifying your business w/ a new product?– Let Market Data target the physicians you need to
build your new referral base from the ground up byfocusing on the key players in your market
• Building a home sleep testing network?– By focusing on CPT codes, you can identify which
physicians are ordering home or in lab sleep testingand utilize clinical personnel to discuss benefits ofworking with your program
Utilizing Market Data

• Quantify physician market potential– By understandingwhat % of a physiciansreferrals you
receive, you can triage which physiciansto target first andefficiently grow your business
• Promote Outcomes programs to key physicians– You’ve invested in outcomes program, let Market Data
identify the top referring physiciansfor oxygen, or the topdiagnosingphysiciansfor COPD
Utilizing Market Data, 2

• 2 ways to use data to grow revenue andincrease efficiencies
– 1. Identify additional opportunities to growbusiness with current referral sources and findnew referral sources
– 2. Reorganize your sales force and marketingefforts to focus on the important players

“Fish where the fish are!”
Questions?
Contact: Ryan BallVGM Market Data
844-236-4022
Questions / Next Steps
QUESTIONNAIRE
PLEASE TELL US WHAT’S ON YOURMIND FOR 2015!

Contact Information
• Mark Higley, [email protected]: 888.224.1631 C: 319.504.9515
• Amy Streeter, [email protected]: 855.874.6927 C: 319.415.1483
• Hans Gullickson, [email protected]: 877.840.1189 C: 303.547.5653





























