Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ieds20
Download by: [67.87.236.65] Date: 11 September 2015, At: 08:37
Expert Opinion on Drug Safety
ISSN: 1474-0338 (Print) 1744-764X (Online) Journal homepage: http://www.tandfonline.com/loi/ieds20
Safety and tolerability of antidepressant co-treatment in acute major depressive disorder:results from a systematic review and exploratorymeta-analysis
Britta Galling MD, Amat Calsina Ferrer MD, Margarita Abi Zeid Daou MD,Dinesh Sangroula MD, Katsuhiko Hagi PhD & Christoph U Correll MD
To cite this article: Britta Galling MD, Amat Calsina Ferrer MD, Margarita Abi Zeid Daou MD,Dinesh Sangroula MD, Katsuhiko Hagi PhD & Christoph U Correll MD (2015): Safety andtolerability of antidepressant co-treatment in acute major depressive disorder: results from asystematic review and exploratory meta-analysis, Expert Opinion on Drug Safety
To link to this article: http://dx.doi.org/10.1517/14740338.2015.1085970
Published online: 10 Sep 2015.
Submit your article to this journal
View related articles
View Crossmark data

1. Introduction
2. Methods
3. Results
4. Conclusion
5. Expert opinion
Review
Safety and tolerability ofantidepressant co-treatment inacute major depressive disorder:results from a systematic reviewand exploratory meta-analysisBritta Galling, Amat Calsina Ferrer, Margarita Abi Zeid Daou,Dinesh Sangroula, Katsuhiko Hagi & Christoph U Correll†
†The Zucker Hillside Hospital, Psychiatry Research, North Shore - Long Island Jewish Health
System, Glen Oaks, NY, USA
Introduction: Although antidepressant (AD) monotherapy is recommended
first-line for major depressive disorder (MDD), AD + AD co-treatment is
common.
Areas covered: We conducted the first systematic review searching PubMed/
MEDLINE/PsycInfo/Embase from database inception until 1 June 2015 for
acute randomized trials in ‡ 20 adults with MDD comparing AD monotherapy
with AD + AD co-treatment that reported quantitative data on adverse events
(AEs). Meta-analyzing 23 studies (n = 2435, duration = 6.6 weeks) AD mono-
therapy and AD + AD co-treatment were similar regarding intolerability-
related discontinuation (risk ratio [RR] = 1.38, 95% CI = 0.89 -- 1.10) and
frequency of ‡ 1 AE (RR = 1.19, 95% CI = 0.95 -- 1.49). Nevertheless, AD + AD
co-treatment was associated with significantly greater burden regarding
4/25 AEs (tremor: RR = 1.55, 95% CI = 1.01 -- 2.38; sweating: RR = 1.95, 95%
CI = 1.13 --3.38, ‡ 7% weight gain: RR = 3.15, 95% CI = 1.34 -- 7.41; weight
gain = 2.17, 95% CI = 0.71 -- 3.63 kg), but not more CNS, gastrointestinal,
sexual or alertness-related AEs. However, 11/25 AEs (44.0%) were reported
in only 1 -- 2 studies. Adding noradrenergic and specific serotonergic antide-
pressants (NaSSA) or tricyclic antidepressants (TCA) to selective serotonin
reuptake inhibitors (SSRIs) was specifically associated with more AEs.
Expert opinion: The potential for increased AEs with AD + AD co-treatment
needs to be considered vis-�a-vis unclear efficacy benefits of this strategy. In
particular, NaSSAs and TCAs should be added to SSRIs with caution. Clearly,
more data on side-effect burden of AD + AD co-treatment are needed.
Keywords: adverse effects, antidepressant, augmentation, combination, co-treatment,
depression, major depressive disorder, meta-analysis, safety, tolerability
Expert Opin. Drug Saf. [Early Online]
1. Introduction
For major depressive disorder (MDD), clinical guidelines suggest as first-linetreatment evidence-based, depression-focused psychotherapy with or withoutmonotherapy of an antidepressant (AD) [1-3]. Response rates to initial AD mono-therapy range between 50 and 75%, whereas remission rates are around 30% [4-9].For patients not responding to the initial treatment, optimization of the AD dose,a switch to another AD, augmentation with various non-ADs agents withantidepressant efficacy, or the co-treatment with two ADs are recommended [1-3].
10.1517/14740338.2015.1085970 © 2015 Informa UK, Ltd. ISSN 1474-0338, e-ISSN 1744-764X 1All rights reserved: reproduction in whole or in part not permitted
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

In clinical care, AD + AD co-treatment is widespread [10,11],
although results regarding the efficacy and safety of this
strategy are heterogeneous [12-18].The use of more than one antidepressant agent is mostly
explained by attempts to increase or speed up efficacy, and
to reduce adverse effects (AEs) allowing for a dose reduction
of the first antidepressant [19]. However, whereas the avoid-
ance of specific AEs often influences the choice of a specific
antidepressant, concerns about drug--drug interactions rarely
influence the selection [20].Main concerns regarding AD + AD co-treatment include
higher cost, the potential for decreased treatment adherence
due to complex drug regimes, the risk of drug--drug interac-
tions, unclear efficacy advantages and, particularly, the
increased risk of AEs. In a meta-analysis of six studies,
AD + AD combination treatment used from the beginning
was shown to be better than monotherapy regarding remis-
sion (relative risk [RR] = 2.71, 95% CI = 1.69 -- 4.35) and
response (RR = 1.5, 95% CI = 1.21 -- 1.97) [21], whereas a
review of five studies of AD augmentation of inefficacious
AD monotherapy showed heterogeneous results [22].
However, these meta-analyses focused on efficacy outcomes
and despite the relatively large use of AD + AD co-treatment
in MDD [10,11], the AE burden of this treatment strategy has
not been comprehensively assessed [21-23].
In order to allow for a comprehensive risk--benefit analysis,detailed knowledge about the short-term and long-term toler-ability and safety of AD + AD co-treatment in MDD isneeded. Therefore, we conducted a systematic review andmeta-analysis of the frequency and severity of AEs in patientswith MDD treated with AD monotherapy comparedAD + AD co-treatment. We hypothesized that the riskof AEs would be significantly greater with AD + AD co-treatment compared with AD monotherapy.
2. Methods
2.1 Literature searchTwo authors (AF, MD) independently conducted a system-atic literature search in PubMed/MEDLINE, PsycInfo andEmbase from database inception through 1 June 2015 withoutlanguage restrictions, using the following search terms: (anti-depressant* OR ‘SSRI’ OR ‘selective serotonin reuptakeinhibitor’ OR ‘SNRI’ OR ‘serotonin norepinephrine reuptakeinhibitor’ OR ‘TCA’ OR ‘tricyclic antidepressant’ OR‘MAOI’ or ‘monoamine oxidase inhibitor’ OR mianserinOR mirtazapine OR vortioxetine OR vilazodone OR levimil-nacipran OR melitracene OR phenelzine OR isocarboxazidOR tranylcypromine OR moclobemide OR amitriptylineOR clomipramine OR dosulepin OR doxepin OR imipra-mine OR lofepramine OR nortriptyline OR trimipramineOR desvenlafaxine OR duloxetine OR venlafaxine OR citalo-pram OR escitalopram OR fluoxetine OR fluvoxamine ORparoxetine OR sertraline OR trazodone OR agomelatineOR reboxetine OR selegiline) AND (augmentation* ORenhancement OR add-on* OR addition* OR supplement*OR cotreatment* OR co-treatment* OR adjunctive* OR con-current* OR concomitant* OR simultaneous* OR polyphar-macy* OR polytherapy OR combin*) AND (depress* ORMDD) AND (random* OR placebo).
The electronic search was supplemented by a manualreview of reference lists from eligible publications and relevantreviews to identify additional studies. Whenever data weremissing for the meta-analysis, the authors were contacted foradditional information.
2.2 Inclusion criteriaInclusion criteria were: i) randomized controlled trials;ii) populations containing ‡ 20 adults; iii) current primarydiagnosis of MDD; iv) randomization to AD monotherapyor the co-treatment of the same AD with a different ADand v) reporting of quantitative data on the frequency orseverity of AEs.
Included were studies investigating either AD augmenta-tion, defined as the addition of a second AD to existing ADmonotherapy, and AD combination, defined as the simulta-neous initiation of two ADs from beginning of the trial afterwashout of previous medications. Excluded were studiesthat; i) aimed at reducing AEs of AD monotherapy by addinga second AD or ii) that compared AD augmentation with AD
Article highlights.
. Although we identified 23 randomized controlledstudies with a total of 2435 participants, global andspecific adverse event (AE) frequencies and, especially,severity are insufficiently and incompletely assessed orreported in the available randomized controlled studies,with only 14/25 (56.0%) AEs being reported in at leastthree studies.
. Co-treatment strategies do not appear to be associatedwith significantly greater intolerability-relateddiscontinuations and incidence of at least one AE, butwere associated with a significantly greater incidence orseverity of 4 of 25 specific reported AEs thanmonotherapy strategies.
. Specific AEs that were more common duringantidepressant (AD) + AD co-treatment included tremor,sweating, weight gain and clinically significant weightgain.
. Sparse data suggest clinically relevant AE differencesacross individual AD + AD class combinations,disfavoring the addition of noradrenergic and specificserotonergic antidepressants (NaSSA) or tricyclicantidepressants (TCA) to selective serotonin reuptakeinhibitors (SSRIs). AE types in the co-treatment groupsgenerally reflected the known AE profiles of individualAD classes.
. In clinical care, potential efficacy advantages ofantidepressant co-treatment strategies need to beevaluated in light of potential AE disadvantages.
This box summarizes key points contained in the article.
B. Galling et al.
2 Expert Opin. Drug Saf. (2015) 14(10)
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

switch instead of continuation of the original ADmonotherapy.
2.3 Outcomes and data abstractionThis study focused solely on safety and tolerability-relatedoutcomes. The two co-primary outcomes were intolerability-related discontinuation and the proportion of patients withat least one AE. Secondary outcomes included; i) incidenceof any specific adverse effect and ii) severity of any specificadverse event (i.e., mean score ± standard deviation [SD], orpercent of patients with a certain level of severity). In addi-tion, we extracted data on the study design (e.g., blinding,duration, etc.), patient, illness and treatment characteristicsand co-medications.
Two authors (AF, DS) independently identified andextracted data from the eligible trials; inconsistencies wereresolved by consensus or involvement of a third reviewer(BG or CUC).
2.4 Data analysisWe conducted a meta-analysis of outcomes forwhich ‡ 2 studies contributed data, using ComprehensiveMeta-Analysis V3 (http://www.meta-analysis.com). Continu-ous outcomes were expressed as the standardized mean differ-ence (SMD) between the two groups in baseline to end pointchange scores (preferred) or end point scores (only preferred ifchange score results were skewed, that is, SD >twice themean), while dichotomous data were analyzed calculatingthe pooled risk ratio (RR) (Mantel-Haenszel RR), both withtheir 95% CI. Additionally, weighted mean difference(WMD) was calculated for weight change in kilograms. Tocombine studies, the random effects model by DerSimonianand Laird [24] was used, which is more conservative than fixedeffects models. We explored study heterogeneity using thechi-square test of homogeneity, with a p < 0.05 indicatingsignificant heterogeneity.
In the primary analyses, we pooled all studies thatcompared AD monotherapy with AD + AD co-treatment.In secondary analyses, we analyzed separately augmentationand combination studies as well as at individual AD combina-tions as long as data were reported in ‡ 2 trials. Forintolerability-related discontinuation, all randomized patientswere analyzed, including observed cases reports as long as thenumber of patients dropping out for adverse effects was men-tioned. For all other outcomes, we only abstracted data fromstudies reporting last observation carried forward data. Allanalyses were two-tailed with a = 0.05 and without adjust-ments for multiple comparisons. We used funnel plots toassess publication bias regarding the two co-primaryoutcomes, discontinuation due to AEs and patients with atleast one AE. To quantify whether publication bias couldhave influenced the results, we used Egger’s regressiontest [25] and the Duval and Tweedie’s trim and fill method [26],which is an interactive procedure to remove the most extremesmall studies from the positive side of the funnel plot or to
impute studies into the negative side of the funnel plot,re-computing the effect size at each iteration until the funnelplot is symmetric about the (new) effect size. In theory, thiswill yield an unbiased estimate of the effect size.
3. Results
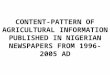
The initial search resulted in 6474 hits. Altogether, 6410 stud-ies were excluded being duplicates and/or on the title/abstractlevel. Of the remaining 64 references plus 6 additional studiesfound reviewing reference lists, 47 articles were excluded afterfull text review, yielding 23 studies that were included in themeta-analysis (Figure 1). Reasons for excluding articles wereas follows: different articles on the same RCT/overlappingsample: n = 23, no combination group: n = 5, study includingbipolar depression: n = 4; MDD in remission: n = 3; studynot randomized: n = 3; no MDD diagnosis: n = 2, focus ontreatment of SSRI-induced AEs: n = 2, no analyzable data:n = 2, study not finished: n = 1; case report data: n = 1,only switch to medication as comparison: n = 1.
3.1 Pooled AD + AD co-treatment versus AD
monotherapy
3.1.1 Study, patient and treatment characteristics3.1.1.1 Study characteristicsOf the 23 meta-analyzed studies [12-15,27-45], most wereconducted in Europe (studies = 11, 47.8%; n = 950)[14,30,32,33,35-37,39,41,44,45], followed by the USA/Canada (stud-ies = 8, 34.8%; n = 1164) [12,13,15,28,29,31,40,43] and other partsof the world (studies = 4, 17.4%; n = 321) (Table 1)[27,34,38,42]. Most studies (78.3%) were double-blind (stud-ies = 18, n = 1692), three were open-label (13.0%, n = 238)and two were single-blind (8.7%, n = 505). The majority ofstudies (studies = 15, 65.2%; n = 1219) evaluated AD combi-nation treatment from baseline. While less studies focused onAD augmentation after insufficient effects of AD monother-apy (studies = 8, 34.8%), the number of included patientswas similar to that in the AD combination treatment studies(n = 1216, 49.9% of all patients). The mean study durationwas 6.6 ± 2.5 (range = 4 -- 12) weeks.
3.1.1.2 Patient characteristicsAltogether, 2435 patients with MDD were studied. The meanpatient age was 41.9 ± 3.8 (range = 18 -- 84) years, with aminority of male participants (34.7%, studies = 21,n = 815) (Table 1). The severity of depression was moderateto severe in most studies (studies = 18, n = 1767, 76.2% ofsubjects). Fewer studies included patients with severe or verysevere depression (studies = 2, n = 360) or patients whowere mildly to moderately ill (study = 1, n = 135). The major-ity of subjects were outpatients (studies = 12, n = 1820), sixstudies included inpatients (n = 248) and three wereconducted in both in- and outpatients (n = 165), while twostudies did not specify the treatment setting (n = 202)(Table 1).
Safety and tolerability of antidepressant co-treatment in acute MDD
Expert Opin. Drug Saf. (2015) 14(10) 3
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

3.1.1.3 Treatment characteristicsMost studies compared monotherapy with a SSRI with co-treatment of an AD from another class (studies = 17,73.9%; n = 1405). The added non-SSRI ADs included norad-renergic and specific serotonergic antidepressants (NaSSA,studies = 7, n = 535), tricyclic antidepressants (TCA, stud-ies = 5, n = 139), norepinephrine-dopamine reuptake inhibi-tors (NDRI, studies = 3, n = 505) and norepinephrinereuptake inhibitors (NRI, studies = 2, n = 227). Other studiescompared TCA versus TCA + TCA (studies = 2, n = 173),TCA versus TCA + SSRI (studies = 2, n = 61), TCA versusTCA + monoamine oxidase inhibitor (MAOI, studies = 2,n = 135), MAOI versus MAOI + TCA (studies = 2,n = 79), TCA versus TCA + NaSSA (study = 1, n = 46),NDRI versus NDRI + SSRI (study = 1, n = 245),norepinephrine-reuptake inhibitor (NRI) versus NRI + SSRI(study = 1, n = 156), NaSSA versus NaSSA + SSRI (study = 1,n = 61), SNRI versus SNRI + NDRI (studies = 1, n = 48) andserotonin antagonist and reuptake inhibitors (SARI) versusSARI + SSRI (study = 1, n = 25) (Table 1).
3.1.2 AE risk with AD + AD co-treatment versus AD
monotherapyAll identified AE outcomes were reported by ‡ 2 studies,allowing meta-analytic calculations, but only 14/25 AEs(56.0%) were reported by ‡ 3 studies (Table 2).
There was no significant difference between AD monother-
apy and AD co-treatment regarding the two co-primary out-
comes, intolerability-related discontinuation (RR = 1.37,
95% CI = 0.89 -- 1.10, p = 0.80; heterogeneity: p = 0.80;
studies = 13, n = 1270) and frequency of ‡ 1 AE
(RR = 1.19, 95% CI = 0.95 -- 1.49, p = 0.14; heterogeneity:
p < 0.001; studies = 6, n = 1029) (Table 2).There was no indication of publication bias for the co-
primary outcomes across all meta-analyzable studies
(Figure 2A and B). The RRs remained virtually identical
even after applying the Duval and Tweedie’s trim and fill
method and after 4 missing studies for intolerability-related
discontinuation and two studies for frequency of ‡ 1 AE
were imputed.Regarding specific AEs, compared with AD monotherapy,
AD + AD co-treatment was associated with significantly
greater AE burden regarding 4/25 AEs. These four AEs
included tremor: RR = 1.55, 95% CI = 1.01 -- 2.38,
p = 0.044; sweating: RR = 1.95, 95% CI = 1.13 -- 3.38,
p = 0.017; ‡ 7% weight gain: RR = 3.15, 95%
CI = 1.34 -- 7.41, p = 0.009; body weight change:
SMD = 1.03, 95% CI = 0.27 -- 1.79, p = 0.008 and
WMD = 2.17, 95% CI = 0.71 -- 3.63 kg, p = 0.016) (Table 2).AD + AD co-treatment was not associated with greater AE
burden than AD monotherapy regarding CNS, gastrointesti-
nal, sexual and alertness-related AEs.
Unique articles identified and screened (n = 4796)
Articles excluded at abstract level (n = 4732)
Full text articles retrieved for evaluation of eligibility (n = 64)
Articles excluded (n = 47):• Overlapping sample (n = 23)• No combination group (n = 5)• Bipolar depression (n = 4)• MDD in remission (n = 3)• Not randomized (n = 3)• No MDD diagnosis (n = 2)• Study on SSRI-induced sexual dysfunction (n = 2)• Not analyzable data (n = 2)• Only switch as comparison (n = 1)• Case report data (n = 1)• Not finished studies (n = 1)
RCTs included in the meta-analysis (n = 23)
Potentially relevant articles (n = 6474)
Duplicate articles (n = 1678)
Individual hits in PubMed(n = 3847 )
Iden
tific
atio
nS
cree
ning
Elig
ibili
tyIn
clud
ed
Articles identified inreviews or meta-analyses (n = 6)
Individual hits in PsycINFO(n = 2319)
Individual hits in Embase(n = 308)
Figure 1. Flow chart for the systematic literature search.
B. Galling et al.
4 Expert Opin. Drug Saf. (2015) 14(10)
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,
illness
andtreatm
entch
aracteristics.
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Augmentationstudies
Balletal.(2014)
(USA)[28]
--Double-blind
--Augmentation
--Outpatient
8227(226)
DSM-IV-TR
--NR
--Recurrent(‡
1episodein
last
5yrs)
--Partialresponders
onSSRI
‡2failures
torespond
toAD
incurrent
episode,BP,
PSY
45.1
±10.8
(18--65)
30.4
SSRI:
--Ongoingtx,
PBO
--n=115
SSRI+EDV:
--SSRI:ongoing
tx,EDV:12.7
(6--18)
--n=111
Hypnotics
forinsomnia
(<15d)
Fava
etal.(2002)
(USA)[15]
--Double-blind
--Augmentation
--Outpatient
--Multicenter
467(67)
DSM-III-R
--NR
--Resistant(partialor
nonresponders)to
openlabelFLU
--17-HDRS‡16
BP,PSY
40.3
±10.7
(18--65)
52.2
FLU:--N
R(40--60)
--n=33
FLU
+DES:
--FLU
:20(fixed
dose),DES:NR
(25--50)
--n=34
LRZ,over-
the-counter
medication
Fava
etal.(1994)
(USA)[31]
--Double-blind
--Augmentation
--Outpatient
--Multicenter
427(27)
DSM-III-R
--NR
--Refractory
toFLU
--17-HDRS‡16
NR
39.6§±9.9§
(18--65)§
39.0§
FLU:
--Ongoingtx:
NR(40--60)
--n=15
FLU
+DES:
--FLU
:20(fixed
dose),DES:NR
(25--50)
--n=12
NR
Ferrerietal.(2001)
(France)[32]
--Double-blind
--Augmentation
--In-andoutpatient
--Multi-center
670(70)
DSM-III-R
--7.3
±8.5
mo§
--Atleast
6wksoftx
withFLU
20mg/d
--17-HDRS‡25
PSY,
substance
abuse,
medical
illness
46.6
±12.7
§26.0
§FLU:
--20(fixeddose)
--n=38
FLU
+MIA:
--FLU
:20(fixed
dose),MIA:60
(fixeddose)
--n=32
BZP
Gulrezetal.(2012)
(India)[34]
--Single-blind(sub-
jects)
--Augmentation
--Outpatient
460(60)
DSM-IV-TR
--NR
--partialresponders
--NR
BP
41.2
±13.6
(18--75)
48.3
SSRIs:
--NR(NR)
--n=30
SSRI+BUP-SR:
--SSRIs:NR(NR),
BUP-SR:NR
(150--300)
--n=30
NR
Lichtetal.(2002)
(Denmark)[36]
--Double-blind
--Augmentation
--Outpatient
--Multicenter
5295(293)
DSM-IV
--NR
--NR
--17-HDRS‡18
PSY,
suicidality,
substance
abuse,psy-
chotic
features
40.3
±11.0
(19--65)
37.9
SER:ongoingtx
--100(fixed
dose)
--n=98
SER+MIA:
--SER:100(fixed
dose),MIA:30
(10--30)
--n=98
OXA,ZLP
SER:
--200(fixed
dose)
--n=97
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,
illness
andtreatm
entch
aracteristics(continued).
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Maesetal.(1996)
(Belgium)[37]
--Double-blind
--Augmentation
after10days
wash-out
--Inpatient
425(22)
DMS-III
--9.5
yrs
--NR
--17-HDRS‡18
OtherAxisI
d/o
52.8
±14.2
(25--70)*
50.0
TRZ:
--100(fixed
dose)
--n=10*
TRZ+FLU:
--TRZ:100(fixed
dose),FLU:20
(fixeddose)
--n=12*
NR
Rush
etal.(COMED)
(2011)(USA)[29]
--Single-blind
--Augmentation
--Outpatient
--Multicenter
12
445(445)
DSM-IV-TR
--NR
--Chronic,recurrent
--Moderatelysevere
BP,PSY
43.0
±13.3
(18--75)
34.4
ESC:
--NR(10--20)
--n=224
ESC
+BUP:
--ESC:NR(10--
20),BUP:NR
(150--400)
--n=221
None
Total:Studies=8,n
=1216,34.8%
of
totalstudies;
USA
andCanada:Studies
=4,n=766,
17.4%
oftotal
studies;
Europe:
Studies=3,n=
390,13.0%
oftotal
studies;
Rest
ofthe
world:Study=1,n
=60,4.3%
oftotal
studies
--Double-blind:
Studies=6,n=
711,26.1%
of
totalstudies;
Single-blind:Stud-
ies=2,n=505,
8.7%
oftotal
studies;
Open-label:
Study=0
--Outpatients:Stud-
ies=6,n=1121,
46.0
%oftotal
patients;In-and
outpatients:Study
=1,n=70,2.9
%oftotalpatients;
Inpatients:Study=
1,n=25,1%
of
totalpatients
5.9
(4--12)
1216(1210)
DSM-IV-TR:
Studies=
3,n=732;
DSM-IV:
Study=1,
n=295;
DSM-III-R:
Studies=
3,n=164;
DSM-III:
Study=1,
n=25;
17-HDRS‡16:
Studies=5,n=
826;17-HDRS‡18:
Studies=2,n=
320;17-HDRS‡25:
Study=1,n=70
Severity
of
depression:Moder-
ate
tosevere:
Studies=7,n=
1146,47%
oftotal
patients
Very
severe:
Studies=1,n=70,
2.9
%oftotal
patients
42.8
(18--
75)
36.1
SSRIvs
SSRI+NaSSA:
Studies=2,n(SSRI)=233,n
(SSRI+NaSSA)=251
SSRIvs
SSRI+NDRI:
Studies=2,n(SSRI)=254,n
(SSRI+NDRI)=251
SSRIvs
SSRI+NRI:
Study=1,n(SSRI)=115,n(SSRI
+NDRI)=111
SSRIvs
SSRI+TCA:
Studies=2,n(SSRI)=48,n(SSRI
+TCA)=46
SARIvs
SARI+SSRI:
Study=1,n(SARI)=10,n(SARI
+SSRI)=12
Co-treatm
entstudies
Akkaya
etal.(2010)
(Turkey)
[27]
--Openlabel
--Co-start
--NR
--Pooleddata
10
156(156)
DSM-IV-TR
NRNR
17-HDRS‡16
OtherAxisI
orIId/o,
PSY,
suicidality
40.5
±10.9
(19--65)*
16.7
REB:
--NR(4
--8)
--n=50*
REB+SER:
--REB:NR(4
--8
BID),SER:50
(fixeddose)
--n=52*
NR
SER:
--50(fixeddose)
--n=54*
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,
illness
andtreatm
entch
aracteristics(continued).
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Blieretal.(2009)
(Canada)[12]
--Double-blind
--Co-start
--Outpatient
861(61)
DSM-IV
--NR
--First
episode(63%
)or
recurrent(37%
),‡1
failedtx
(24.6%
)--1
7-HDRS‡18
BP
43.1
±10.5
54.1
MIR:
--NR(30--45)
--n=21
MIR
+PAR:
--MIR:NR
(30--45),
PAR:NR
(20--30)
--n=21
CLN
PAR:
--NR(20--30)
--n=19
Blieretal.(2010)
(Canada)[13]
--Double-blind
--Co-start
--Outpatients
--Multicenter
653(53)
DSM-IV
--NR
--Recurrent(68%
),‡
1failedtx
(50%
),‡
1yr
(43%
)--1
7-HDRS‡18
(Hypo)
mania,seiz-
ures,medical
illness
44.7
±2.3
NR
FLU:
--20(fixeddose)
--n=28
FLU
+MIR:
--FLU
:20(fixed
dose),MIR:30
(fixeddose)
--n=25
CLN
,ZOP,
ZLP
Dam
etal.(1998)
(Denmark)[30]
--Double-blind
--Co-start
--In-and
outpatients
634(34)
ICD-10,
DSM-III-R
--NR
--NR
--Moderate
tosevere,
--17-HDRS>16,
MES>14
Psychotic
DEP
NR(18--70)
*NR
FLU:
--20(fixeddose)
--n=18*
FLU
+MIA:
--FLU
:20(fixed
dose),MIA:30
(fixeddose)
--n=16*
NR
Fornaro
etal.(2014)
(Italy)[33]
--Double-blind
--Co-start
--Outpatient
648(45)
DSM-IV
--NR
--Currentepisode
withatypical
features
--NR
Epilepsy,
organicbrain
disease
39.0
±11.7
(19--65)
34.8
DUL:
--91.3
(60--
120)
--n=22
DUL+BUP:
--DUL:
86.1
(60
--120),BUP:
215.2
(150--
300)
--n=23
LRZ
Lauritzenetal.
(1992)(Denmark)
[35]
--Double-blind
--Co-start
after3
days
washout--N
R
646(40)
DSM-III
--NR
--17-HDRS>16
--Melancholia
scale
score:15--67
Current
episode‡12
m,suicidality
60z
(44--84)
25.0
IMI:
--NR(50--100)
--n=18
IMI+MIA:
--IMI:NR(50--
100),MIA:30
(fixeddose)
--n=22
OXA
Maesetal.(1999)
(Belgium)[37]
--Double-blind
--Co-start
--Inpatient
523(21)
DSM-III-R
--NR
--NR
--Allseveritiesof
MDD
(stages0--5)
OtherAxisI
d/o
49.1
±15.2
(25--70)
57.1
FLU:
--20(fixeddose)
--n=11
FLU
+MIA:
--FLU
:20(fixed
dose),MIA:30
(fixeddose)
--n=10
CDP,LRZ
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,
illness
andtreatm
entch
aracteristics(continued).
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Matreja
etal.(2012)
(India)[38]
--Openlabel
--Co-start
--Inpatient
660(60)
ICD-10,
DSM-IV
--3.7
±2.8
yrs
--Newlydiagnosed,
partialandnon-
responders
included
--17-HDRS‡18
BP,PSY
40.1
±12.9
(18--75)
50.0
SSRIs:
--NR(NR)
--n=30
SSRI+MIR:
--SSRI:NR(NR),
MIR:7.5
(fixed
dose)
--n=30
Concomitant
medication
allowed,but
notspecified
Murphyetal.(1977)
(UK)[39]
--Double-blind,
--Co-start
--Outpatient
--Multicenter
4173(173)
NR
--50.4
mo
--Endogenousand
reactivedepression
--Severe
enoughto
qualifyforTCAtx,
butbeanoutpatient
population
Medical
illness
and
pt.onother
psychotropic
medication
42.4
(18--65)
22.0
CLO
:--1
0TID
(fixeddose)
--n=57(57)
CLO
+DES:
--CLO
:10TID
(fixeddose),
DES:25TID
(fixeddose)
--n=58(58)
HYP
DES:
--25TID
(fixed
dose)
--n=58(58)
Nelsonetal.(2004)
(USA)[40]
--Double-blind
--Co-start
--Inpatient
--Multicenter
639(39)
DSM-IV
--NR
--MDD,sometx
resistantpatients,no
psychoticfeatures
--17-HDRSscore
‡18
BP,PSY,Sz,
SzA
,sub-
stance
abuse,clus-
terB
personality
d/o,medical
illness
44.8
±12.5
(>21)
43.6
DES:
--293.7
(100--350)
--n=12
DES+FLU:
--DES:98.1
(100
--350),FLU:20
(fixeddose)
--n=13
BZP
FLU:
--20(fixeddose)
--n=14
O’Brienetal.(1992)
(Ireland)[41]
--Double-blind
--Co-start
--Inpatient
679(79)
Research
diagnostic
criteria
(RDC)
--NR
--NR
--17-HDRSscore
‡16
Txresistant
DEP,other
medicalor
psychiatric
illness
41.4
±12.1
(18--65)*
43.0
TCP:
--18.5
(10--30)
--n=26*
TCP+AMI:
--TCP:19.7
(10
--30),AMI:
108.7
(50--150)
--n=25*
BZP
AMI:
--114.3
(50--
150)
--n=28*
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,
illness
andtreatm
entch
aracteristics(continued).
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Raisietal.(2006)
(Iran)[42]
--Double-blind
--Co-start
after
wash-out
--Outpatient
845(45)
DSM-IV
--10.6
±6.8
mo--N
R--1
7-HDRSscore
‡20
NR
33.0
±10.7
(18--54)
40
CIT:
--40(NR)
--n=22
CIT
+NOR:
--CIT:40(NR),
NOR:50(NR)
--n=23
None
Stewart
etal.(2014)
(USA)[43]
--Double-blind
--Co-start
--Outpatient
--Multicenter
12
245(245)
DSM-IV-TR
--DCE:80.1
±--1
31.1
mo
(6.7
±10.9)
--NR
--NR
BP,PSY
40.3
±10.7
(18--65)
33.5
BUP-XL:
--NR(150--450)
--n=83
BUP-XL+ESC:
--BUP-XL:
NR
(150--450),
ESC:NR
(10--40)
--n=78
NR
ESC:
--NR(10--40)
--n=84
Vezm
aretal.(2009)
(Serbia)[44]
--Openlabel
--Co-start
--Inpatient
4--6**
22(22)
DSM-IV
--NR--N
R--H
DRS
score
‡18
OtherAxisI
andIId/o
43.6
±11.4
31.8
AMI:
--75(fixeddose)
--n=9
AMI+FLV:
--AMI:75(fixed
dose),FLV:100
(fixeddose)
--n=7
NR
FLV:
--100(fixed
dose)
--n=6
Youngetal.(1979)
(UK)[45]
--Double-blind
--Co-start
--Outpatient
6135(135)
NR
--14.49m
--NR--M
ildto
moderate
OtherAxisI
orIId/o,
medical
illness
36.2
(20--70)
36.3
TRI:--1
06{
(50--150)
--n=34
TRI+PHE:
--TRI:102{
(50--150),PHE:
44(15--60)
--n=26
NIT,DIA
PHE:--4
5{
(15--60)
--n=25
TRI+ISO:
--TRI:96{
(50--150),ISO:
30(10--30)
--n=25
ISO
:--3
2{,#
(10--30)
--n=25
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,
illness
andtreatm
entch
aracteristics(continued).
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Total:Studies=15,
n=1219,65.2
%oftotalstudies;
Europe:Studies=8,
n=560,34.8
%of
totalstudies;
USA
andCanada:Studies
=4,n=398,17.4
%oftotalstudies;
Rest
oftheworld:
Studies=3,n=
261,13.0
%oftotal
studies
--Double-blind:
Studies=12,n=
981,52.2
%of
totalstudies;
Open-
label:Studies=3,
n=238,13.0%
of
totalstudies;
--Single-blind:Stud-
ies=0
--Outpatients:Stud-
ies=6,n=699,
28.7%
oftotal
patients;Inpatients:
Studies=5,n=
223,9.2
%of
totalpatients;--In-
andoutpatients:
Studies=2,n=
95,3.9
%oftotal
patients
--NR:
Studies=2,n=
202,8.3
%of
totalpatients
6.7
(4--
12)
1219(1209)
DSM-IV-TR:
Studies=
2,n=401;
NR:Studies
=2,n
=308;DSM-
IV:Studies
=6,n=
268;
Research
Diagnostic
Criteria:
Studies=
1,n=79;
ICD-10,
DSM-IV:
Studies=
1,n=60;
--NR:Studies=2,n
=308;17-HDRS‡
16:Studies=4,n=
292;MADRS‡22:
Study=1,n=245;
17-HDRS‡18:
Studies=3,n=
174;HDRS‡18:
Studies=2,n=61;
21-HDRS‡14:Study
=1,n=48;HDRS‡
16,MES>15:Study
=1,n=46;
17-HDRS‡20:Study
=1,n=45--Severity
ofdepression:
Moderate
tosevere:
Studies=11,n=
621,25.5%
oftotal
patients;Severe
tovery
severe:Studies
=2,n=290,11.9%
oftotalpatients;NR:
Studies=1,n=
173,7.1
%oftotal
patients;Mild
tomoderate:Studies=
1,n=135,5.5
%oftotalpatients
40.9
(18--84)
33.2
SSRIvs
SSRI+NaSSA:Studies=
5,n(SSRI)=106,n(SSRI+
NaSSA)=92
SSRIvs
SSRI+TCA:Studies=3,n
(SSRI)=42,n(SSRI+TCA)=34
SSRIvs
SSRI+NDRI:Study=1,n
(SSRI)=84,n(SSRI+NDRI)=39
SSRIvs
SSRI+NRI:Study=1,n
(SSRI)=54,n(SSRI+NRI)=26
TCA
vsTCA
+MAOI:Studies=2,
n(TCA)=62,n(TCA+MAOI)=
38
TCA
vsTCA
+NaSSA:Study=1,
n(TCA)=18,n(TCA+NaSSA)=
22
TCA
vsTCA
+SSRI:Studies=2,
n(TCA)=21,n(TCA+SSRI)=9
TCA
vsTCA
+TCA:Studies=2,
n(TCA)=115,n(TCA
+TCA)=
58
MAOIvs
MAOI+TCA:Studies=2,
n(M
AOI)=76,n(M
AOI+TCA)
=38
NaSSA
vsNaSSA
+SSRI:Study=
1,n(NaSSA)=21,n(NaSSA
+SSRI)=10
NDRIvs
NDRI+SSRI:Study=1,n
(NDRI)=83,n(NDRI+SSRI)=39
NRIvs
NRI+SSRI:Study=1,n
(NRI)=50,n(NRI+SSRI)=26
SNRIvs
SNRI+NDRI:Study=1,n
(SNRI)=23,n(SNRI+NDRI)=23
Summary
oftotalstudies
Total:Studies=23,
n=2435;USAand
Canada:Studies=8,
n=1164,34.8%
of
totalstudies;
Europe:
--Double-blind:
Studies=18,n=
1692,78.3%
of
totalstudies;;
Single-blind:
6.4
(4--
12)
2435(2419)
DSM-III:
Studies=
1,n=46;
ICD-10,
DSM-III:
17-HDRS‡16:
Studies=9,n=
1118;17-HDRS‡
18:Studies=5,n=
494;NR:studies=2,
41.9
(18--84)
34.7
SSRIvs
SSRI+NaSSA:Studies=
7,n(SSRI)=339,n(SSRI+
NaSSA)=222
SSRIvs
SSRI+TCA:Studies=5,n
(SSRI)=90,n(SSRI+TCA)=80
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
1.Design,patient,illness
andtreatm
entch
aracteristics(continued).
Study(year)
Design:--B
linding
--Co-start/A
ug-
mentation
--Setting
--Multicenter
Trial
duration
(wks)
NRandom-
ized(ITT)
Diagnostic
criteria
MDD
MDD:
--Meanduration
(years)
--Illness
state
--Illness
severity
Exclusion
criteria
Age:years
±SD
(range)
Sex:
Male
(%)
Monotherapy:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Combination:
--Meandose,
range(m
g)
--Numberof
patients
(ITT)
Adjunctive
medication
allowed
Studies=11,n=
950,47.8%
oftotal
studies;
Rest
ofthe
world:Studies=4,n
=321,17.4%
of
totalstudies
Studies=2,n=
505,8.7%
oftotal
studies;;Open-
label:Studies=3,
n=238,13.0%
of
totalstudies;
--Co-
treatm
ent:Studies
=15,n=1219,
65.2%
oftotal
studies;
--Augmentation:
Studies=8,n=
1216,34.8%
of
totalstudies;
--Outpatients:Stud-
ies=12,n=1820,
74.7%
oftotal
patients;Inpatients:
Studies=6,
n=248,10.2%
of
totalpatients;NR:
Studies=2,n=
202,8.3%
oftotal
patients;In-and
outpatients:Studies
=3,n=165,
6.8%
oftotal
patients
Studies=
1,n=34;
DSM-III-R:
Studies=
1,n=23
n=308;17-HDRS‡
25:Study=1,n=
70;HDRS‡18:
Studies=2,n=61;
21-HDRS‡14:Study
=1,n=48;MADRS
‡22:Study=1,n=
245;HDRS‡16,
MES>15:Study=
1,n=46;17-HDRS
‡20:Study=1,n=
45;Severity
of
depression:Mild
tomoderate:Studies=
1,n=135,5.5%
of
totalpatients
Moderate
tosevere:
Studies=18,n=
1767,72.6%
of
totalpatients
Severe
tovery
severe:
Studies=2,n=
290,11.9%
oftotal
patients
Very
severe:
Studies=1,n=70,
2.9%
oftotal
patients,NR:studies
=1,n=173,7.1%
oftotalpatients
SSRIvs
SSRI+NDRI:Studies=3,
n(SSRI)=338,n(SSRI+NDRI)=
290
SSRIvs
SSRI+NRI:Studies=2,n
(SSRI)=169,n(SSRI+NRI)=137
TCAvs
TCA+MAOI:Studies=2,
n(TCA)=62,n(TCA+MAOI)=
38
TCAvs
TCA+NaSSA:Study=1,
n(TCA)=18,n(TCA+NaSSA)=
22
TCAvs
TCA+SSRI:Studies=2,
n(TCA)=21,n(TCA+SSRI)=9
TCAvs
TCA+TCA:Studies=2,
n(TCA)=115,n(TCA
+TCA)=
58
MAOIvs
MAOI+TCA:Studies=
2,n(M
AOI)=76,n(M
AOI+
TCA)=38
NaSSA
vsNaSSA
+SSRI:Study=
1,n(NaSSA)=21,n(NaSSA
+SSRI)=10
NDRIvs
NDRI+SSRI:Study=1,n
(NDRI)=83,n(NDRI+SSRI)=39
NRIvs
NRI+SSRI:Study=1,n
(NRI)=50,n(NRI+SSRI)=26
SNRIvs
SNRI+NDRI:Study=1,n
(SNRI)=23,n(SNRI+NDRI)=23
SARIvs
SARI+SSRI:Study=1,n
(SARI)=10,n(SARI+SSRI)=12
*Numbers
basedonobservedcases.
z Median.
§
Numbers
basedonwhole
studysample.{ M
eansofthelast
3weeksofthetrial.
#Asreportedin
thearticle
(meanrange).**AMIstudyarm
:6weeks,
FLVandFLV+AMIstudyarm
s:4wks.
AD:Antidepressant;AMI:Amitriptyline;BP:Bipolardisorder;BUP:Bupropion;BUP-XL:
Bupropionextendedrelease;BUP-SR:Bupropionsustainedrelease;BZP:Benzodiazepine;CDP:Chlordiazepoxide;CLN
:Clonazepam;CLO
:Clomipramine;
CIT:Citaloprame;DCE:Durationofcurrentepisode;DEP:Depression;DES:Desipramine;DIA:Diazepam;d/o:disorder;d:day;
DSM-III:
TheDiagnostic
andStatisticalManualofMentalDisorders,ThirdEdition;DSM-IV(TR):TheDiagnostic
andStatisticalManualofMentalDisorders,FourthEdition(Text
Revised);DUL:
Duloxetine;ESC:Escitalopram;FLU:Fluoxetine;FLV:Fluvoxamine;HYP:Hypnotics;ISO:Isocarboxazid;IM
I:Im
ipramine;ITT:Intentionto
treat;LRZ:Lorazepam;
m:Month(s);MIA:Mianserin;MIR:Mirtazapine;Mono:Monotherapy;
N:Numberofstudies;
n:Numberofrandomizedsubjects;
NIT:Nitrazepam;NOR:Nortryptiline;NR:Notreported;OXA:Oxazepam;PAR:Paroxetine;PBO:Placebo;
PHE:Phenelzine;PSY:Psychosis;
REB:Reboxetine;SD:Standard
deviation;SER:Sertraline;SSRI:Selectiveserotonin
reuptakeinhibitor;TCA:Tricyclic
antidepressant;TCP:Tranylcypromine;TRI:Trimipramine;TRZ:Trazodone;tx:Treatm
ent;
wk:Week;yrs:
Years;ZLP:Zolpidem;ZOP:Zopiclone.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

3.1.3 AE risk with specific AD + AD class co-treatment
versus AD monotherapyRegarding individual AD co-treatment, addition of NaSSAs toSSRIs was associated with significantly more incidenceof ‡ 1 AE (RR = 1.63, 95% CI = 1.19 -- 2.23); sedation(RR = 3.22, 95% CI = 2.16 -- 4.081); ‡ 7% weight gain(RR = 3.81, 95% CI = 1.37 -- 10.55; SMD = 1.0, 95%CI = 1.03, 95% CI = 0.27 -- 1.79; WMD = 2.17, 95%CI = 0.71 -- 3.63 kg) than SSRI monotherapy (Table 3).Furthermore, TCA augmentation of SSRIs was associatedwith significantly greater incidence of dry mouth (RR = 1.96,95% CI = 1.17 -- 3.28) compared with SSRI monotherapy.
3.2 AD + AD augmentation versus AD monotherapy
3.2.1 Study, patient and treatment characteristics3.2.1.1 Study characteristicsIn total, 8 of the 23 studies (34.8%) with 16 treatment armsinvestigated AD augmentation, that is, the addition of a
second AD after insufficient response of AD monotherapy(Table 1) [15,28,29,31,32,34,36,37]. Augmentation studies weredouble-blind (75.0%, studies = 6, n = 1692) or single-blind(25%, studies = 2, n = 505). The mean study duration was6.1 ± 2.3 (range = 4 -- 12) weeks.
3.2.1.2 Patient characteristicsAltogether, 1216 patients with MDD were studied. The meanpatient age was 42.8 ± 4.5 (range = 18 -- 75) years, with aminority of male participants (36.1%, studies = 8, n = 439)(Table 1). All studies were conducted in patients who hadfailed prior antidepressant treatment or who were consideredtreatment resistant. The severity of depression was reportedto be moderate to severe in seven studies (n = 1146, 87.5%of subjects), while only one study included severely ill patients
(n = 70). The majority of subjects were outpatients (studies = 6,n = 1121), whereas one study was conducted with inpatients(n = 25), and one with in- and outpatients (n = 70).
-2.0
A.
B.
-1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0
0.0
0.5
1.0
1.5
2.0
Sta
nd
ard
err
or
MH log risk ratio
Funnel plot of standard error by MH log risk ratio
-2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0
Sta
nd
ard
err
or
MH log risk ratio
Funnel plot of standard error by MH log risk ratio0.0
0.2
0.4
0.6
0.8
1.0
Figure 2. (A) Funnel plot analysis for discontinuation due to adverse effect (all the studies are included). Observed RR (open
diamond) = 1.368 (95% CI: 0.894, 2.096); Egger’s test: p = 0.135. Adjusted RR (black diamond) after imputation of 4 missing
studies (black circles) = 1.204 (95% CI: 0.798 -- 1.815). (B) Funnel plot analysis for at least one adverse effect (only LOCF studies
are included). Observed RR (open diamond) = 1.180 (95% CI: 0.964, 1.444); Egger’s test: p = 0.344. Adjusted RR (black
diamond) after imputation of 2 missing studies (black circles) = 1.107 (95% CI: 0.904 -- 1.357)
B. Galling et al.
12 Expert Opin. Drug Saf. (2015) 14(10)
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
2.Adverseeffect
outcomesin
patients
onantidepressantmonotherapyversusantidepressantco
-treatm
ent(augmentationorco
mbination).
Outcome
Allstudies
Augmentation-studies
Combinationtreatm
ent-studies
Outcome
Nn
Riskratio/
SMD
95%
CI
p-
Value
p-Value
heterogeneity
Nn
Risk
ratio/
SMD
95%
CI
p-
Value
p-Value
heterogeneity
NN
Riskratio/
SMD
95%
CI
p-
Value
p-Value
heterogeneity
Co-primary
outcomes
Discontinuation
dueto
AE
18
1270
1.368
0.894,
2.096
0.149
0.797
3323
1.737
0.386,
7.807
0.471
0.220
15
947
1.434
0.887,
2.319
0.142
0.833
Atleast
oneAE
91029
1.185
0.945,
1.486
0.142
<0.001
3589
AD
mono"
1.498z
1.299,
1.726z
< 0.001§
0.406
6440
0.982
0.840,
1.149
0.824
0.140
Movementdisorder
Tremor
4576
AD
mono"
1.552z
1.012,
2.380z
0.044§
0.811
1293
1.327
0.383,
4.592
0.656
--3
283
AD
mono"
1.585z
1.006,
2.499z
0.047§
0.640
Anticholinergic
AE
Dry
mouth/
reduced
salivation
8839
1.516
0.910,
2.526
0.110
0.002§
3430
AD
mono"
2.082z
1.234,
3.513z
0.006§
0.403
5409
1.289
0.674,
2.465
0.443
0.002§
Blurredvision
265
2.265
0.556,
9.230
0.254
0.730
127
3.692
0.164,
83.268
0.411
--1
38
2.000
0.415,
9.650
0.388
--
Arousal-relatedAE
Sedation
5636
1.655
0.858,
3.194
0.133
0.023§
1293
AD
mono"
3.198z
2.134,
4.792z
< 0.001§
--4
343
1.149
0.700,
1.888
0.583
0.675
Fatigue/tired-
ness/drowsiness
5420
1.227
0.749,
2.010
0.418
0.445
2137
2.018
0.511,
7.975
0.317
0.251
3283
1.052
0.578,
1.915
0.867
0.431
Asthenia/lack
of
energy
2108
0.739
0.254,
2.150
0.579
0.325
170
0.297
0.035,
2.524
0.266
--1
38
1.000
0.292,
3.426
1.000
--
Insomnia
6702
0.855
0.566,
1.291
0.456
0.202
1293
1.279
0.574,
2.851
0.547
--5
409
0.778
0.481,
1.257
0.305
0.180
CardiovascularAE
Fainting/
Dizziness
8839
1.063
0.754,
1.498
0.729
0.998
3430
1.074
0.610,
1.892
0.804
0.791
5409
1.056
0.685,
1.627
0.805
0.990
Tachycardia
3164
0.836
0.192,
3.640
0.811
0.215
00
----
----
3164
0.836
0.192,
3.640
0.811
0.215
CNSAE
Confusion
3283
1.470
0.754,
2.867
0.258
0.419
00
----
----
3283
1.470
0.754,
2.867
0.258
0.419
Mania
4393
0.995
0.455,
2.176
0.990
0.549
00
----
----
4393
0.995
0.455,
2.176
0.990
0.549
Tension/inner
restlessness
3419
0.684
0.305,
1.536
0.358
0.932
1293
0.569
0.120,
2.686
0.476
--2
126
0.733
0.284,
1.891
0.521
0.799
*Averagechange,endpointonly
ifnoaveragechangeavailable.
z,§pvalues:
p<0.05;continuousdata
initalics.
":Superior;AD:Antidepressant;AE:Adverseevent;CNS:Centralnervoussystem;mono:Monotherapy;
N:Numberofstudies;
n:Numberofparticipants;SMD:Standardizedmeandifference;WMD:Weightedmeandifference.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
2.Adverseeffect
outcomesin
patients
onantidepressantmonotherapyversusantidepressantco
-treatm
ent(augmentationorco
mbination)(continued).
Outcome
Allstudies
Augmentation-studies
Combinationtreatm
ent-studies
Outcome
Nn
Riskratio/
SMD
95%
CI
p-
Value
p-Value
heterogeneity
Nn
Risk
ratio/
SMD
95%
CI
p-
Value
p-Value
heterogeneity
NN
Riskratio/
SMD
95%
CI
p-
Value
p-Value
heterogeneity
Headache
7772
1.022
0.747,
1.400
0.890
0.797
2363
0.707
0.142,
3.514
0.671
0.227
5409
1.038
0.746,
1.445
0.823
0.819
GastrointestinalAE
Constipation
3164
0.951
0.190,
4.769
0.952
0.025§
138
1.000
0.474,
2.108
1.000
--2
126
1.430
0.025,
81.597
0.862
0.012
Diarrhea
2331
0.448
0.188,
1.065
0.069
0.771
1293
0.474
0.184,
1.218
0.121
--1
38
0.333
0.038,
2.925
0.322
--
Nausea
81007
0.918
0.683,
1.234
0.570
0.723
3589
1.411
0.643,
3.097
0.390
0.312
5418
0.840
0.604,
1.168
0.299
0.949
Abdominalpain/
GIdistress
2137
0.890
0.557,
1.421
0.625
0.377
2137
0.890
0.557,
1.421
0.625
0.377
00
----
----
Decreased
appetite
3283
0.827
0.521,
1.313
0.422
0.842
00
----
----
3283
0.827
0.521,
1.313
0.422
0.842
WeightchangeAE
Weight
gain
‡7%
or
reportedasside
effect
3401
AD
monosu-
perior3.148z
1.338,
7.405z
0.009§
0.511
2363
AD
monosu-
perior3.807z
1.374,
10.548z
0.010§
0.348
138
2.000
0.415,
9.650
0.388
--
Bodyweight
change(SMD)*
2346
AD
monosu-
perior1.033z
0.271,
1.794z
0.008§
0.019§
1293
AD
monosu-
perior0.692z
0.443,
0.941z
< 0.001§
--1
53
AD
monosu-
perior1.476z
0.868,
2.084z
< 0.001§
--
Bodyweight
change(W
MD:
kg)*
2346
AD
monosu-
perior2.170z
0.708,
3.631z
0.004§
0.016§
1293
AD
monosu-
perior1.500z
0.974,
2.026z
< 0.001§
--1
53
AD
monosu-
perior3.000z
1.904,
4.096z
< 0.001§
--
EndocrineAE
Sexualdysfunc-
tion(any)
5569
1.403
0.861,
2.287
0.174
0.378
1226
5.179
0.251,
106.673
0.287
--4
343
1.346
0.793,
2.284
0.271
0.323
OtherAEs
Paresthesia
2264
1.818
0.553,
5.973
0.325
0.720
1226
3.107
0.128,
75.472
0.486
--1
38
1.667
0.462,
6.008
0.435
--
Sweating/
Perspiration
7928
AD
monosu-
perior1.951z
1.127,
3.376z
0.017§
0.057
2519
2.530
0.398,
16.092
0.326
0.078§
5409
AD
monosu-
perior2.016z
1.017,
3.996z
0.045§
0.059
*Averagechange,endpointonly
ifnoaveragechangeavailable.
z,§pvalues:
p<0.05;continuousdata
initalics.
":Superior;AD:Antidepressant;AE:Adverseevent;CNS:Centralnervoussystem;mono:Monotherapy;
N:Numberofstudies;
n:Numberofparticipants;SMD:Standardizedmeandifference;WMD:Weightedmeandifference.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
3.Adverseeffect
outcomesin
patients
onantidepressantmonotherapyversussp
ecificantidepressantclass
co-treatm
ents.
SSRIvsSSRI+TCA
SSRIvsSSRI+NaSSA
SSRIvsSSRI+NDRI
MAOIvs
MAOI+TCA
TCA
vsTCA
+TCA
TCA
vsTCA
+SSRI
TCA
vsTCA
+MAOI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
Co-primary
outcomes
Numberofcomparisons
(OC/LOCF)
=5
Numberofcomparisons
(OC/LOCF)
=7
Numberof
comparisons
(OC/LOCF)
=3
Numberof
comparisons(OC/
LOCF)
=3
Numberof
comparisons(OC/
LOCF)
=2
Numberof
comparisons(OC/
LOCF)
=2
Numberof
comparisons(OC/
LOCF)
=3
Discontinuation
dueto
AE
1(27)
6.154
0.323,117.205
5(247)
1.339
0.413,4.342
1(123)
3.231
0.562,18.563
1(40)
6.692
0.292,153.546
2(173)
1.586
0.662,3.803
0(0)
--1(39)
1.000
0.100,10.037
Numberofcomparisons
(LOCF)
=5
Numberofcomparisons
(LOCF)
=6
Numberof
comparisons
(LOCF)
=3
Numberof
comparisons
(LOCF)
=2
Numberof
comparisons
(LOCF)
=2
Numberof
comparisons
(LOCF)
=2
Numberof
comparisons
(LOCF)
=2
Atleast
oneAE
1(10)
4.500
0.689,29.388
2(363)
AD
monosuperior
1.626
1.185,2.231z
1(123)
0.969
0.875,1.074
0(0)
--2(173)
0.688
0.446,1.061
1(12)
2.000
0.589,6.790
0(0)
--
Movementdisorder
Anyextrapyramidal
AE
0(0)
--0(0)
--1(123)
1.077
0.472,2.455
0(0)
--0(0)
--0(0)
--0(0)
--
Rigidity
0(0)
--0(0)
--1(123)
1.077
0.472,2.455
0(0)
--0(0)
--0(0)
--0(0)
--
Tremor
1(38)
3.000
0.342,26.327
1(293)
1.327
0.383,4.592
1(123)
1.846
0.944,3.612
0(0)
--0(0)
--0(0)
--0(0)
--
Anticholinergic
AE
Dry
mouth/reduced
salivation
2(105)
AD
monosuperior
1.962
1.172,3.284z
2(363)
3.118
0.477,20.388
1(123)
1.675
0.932,3.010
0(0)
--0(0)
--0(0)
--0(0)
--
Blurredvision
2(65)
2.265
0.556,9.230
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Arousal-relatedAE
Sedation
1(38)
1.167
0.481,2.829
2(353)
AD
monosuperior
3.224
2.159,4.813z
1(123)
0.887
0.401,1.962
0(0)
--0(0)
--0(0)
--0(0)
--
Fatigue/tiredness/
drowsiness
2(105)
1.630
0.782,3.398
1(70)
8.273
0.443,154.418
1(123)
0.718
0.281,1.835
0(0)
--0(0)
--0(0)
--0(0)
--
Asthenia/lack
of
energy
1(38)
1.000
0.292,3.426
1(70)
0.297
0.035,2.524
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Insomnia
1(38)
0.400
0.088,1.813
1(293)
1.279
0.574,2.851
1(123)
0.957
0.545,1.683
0(0)
--0(0)
--0(0)
--0(0)
--
*Averagechange,endpointonly
ifnoaveragechange.
z p-values:
p<0.05;continuousdata
initalics.
AD:Antidepressant;AE:Adverseevent;MAOI:Monoamineoxidase
inhibitor;mono:Monotherapy;
N:Numberofcomparisons;
n:Numberofparticipants;NaSSA:Noradrenergic
andspecificserotonergic
antidepressant;NDRI:
Norepinephrine-dopaminereuptakeinhibitor;RR:Riskratio;SMD:Standardizedmeandifference;SSRI:Serotonin
reuptakeinhibitors;TCA:Tricyclic
antidepressant;WMD:Weightedmeandifference.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
3.Adverseeffect
outcomesin
patients
onantidepressantmonotherapyversussp
ecificantidepressantclass
co-treatm
ents
(continued).
SSRIvsSSRI+TCA
SSRIvsSSRI+NaSSA
SSRIvsSSRI+NDRI
MAOIvs
MAOI+TCA
TCA
vsTCA
+TCA
TCA
vsTCA
+SSRI
TCA
vsTCA
+MAOI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
Agitation
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--Irritability
0(0)
--0(0)
--1(123)
0.862
0.175,4.247
0(0)
--0(0)
--0(0)
--0(0)
--
CardiovascularAE
Faintness/dizziness
2(105)
1.123
0.616,2.049
2(363)
0.908
0.336,2.452
1(123)
1.077
0.558,2.078
0(0)
--0(0)
--0(0)
--0(0)
--
Tachycardia
1(38)
1.000
0.230,4.343
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Sweating/
perspiration
1(38)
1.750
0.612,5.006
1(293)
1.257
0.636,2.482
1(123)
1.657
0.797,3.444
0(0)
--0(0)
--0(0)
--0(0)
--
Flush
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--CNSAE
Confusion
1(38)
2.000
0.198,20.244
0(0)
--1(123)
0.994
0.408,2.420
0(0)
--0(0)
--0(0)
--0(0)
--
Mania
0(0)
--1(30)
5.000
0.221,113.183
1(162)
1.346
0.375,4.833
0(0)
--0(0)
--0(0)
--0(0)
--
Concentration
difficulty
0(0)
--0(0)
--1(123)
1.256
0.536,2.943
0(0)
--0(0)
--0(0)
--0(0)
--
Tension/inner
restlessness
0(0)
--1(293)
0.569
0.120,2.686
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Vertigo
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--Headache
1(38)
0.800
0.253,2.529
2(363)
0.707
0.142,3.514
1(123)
1.077
0.642,1.806
0(0)
--0(0)
--0(0)
--0(0)
--
GastrointestinalAE
Constipation
1(38)
1.000
0.474,2.108
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Diarrhea
1(38)
0.333
0.038,2.925
1(293)
0.474
0.184,1.218
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Nausea
1(38)
0.500
0.049,5.061
2(363)
1.015
0.465,2.214
1(123)
0.875
0.520,1.473
0(0)
--0(0)
--0(0)
--0(0)
--
Abdominalpain/GI
distress
1(67)
0.863
0.537,1.385
1(70)
3.545
0.149,84.143
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Decreasedappetite
1(38)
0.600
0.166,2.163
0(0)
--1(123)
0.923
0.467,1.826
0(0)
--0(0)
--0(0)
--0(0)
--
*Averagechange,endpointonly
ifnoaveragechange.
z p-values:
p<0.05;continuousdata
initalics.
AD:Antidepressant;AE:Adverseevent;MAOI:Monoamineoxidase
inhibitor;mono:Monotherapy;
N:Numberofcomparisons;
n:Numberofparticipants;NaSSA:Noradrenergic
andspecificserotonergic
antidepressant;NDRI:
Norepinephrine-dopaminereuptakeinhibitor;RR:Riskratio;SMD:Standardizedmeandifference;SSRI:Serotonin
reuptakeinhibitors;TCA:Tricyclic
antidepressant;WMD:Weightedmeandifference.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

Table
3.Adverseeffect
outcomesin
patients
onantidepressantmonotherapyversussp
ecificantidepressantclass
co-treatm
ents
(continued).
SSRIvsSSRI+TCA
SSRIvsSSRI+NaSSA
SSRIvsSSRI+NDRI
MAOIvs
MAOI+TCA
TCA
vsTCA
+TCA
TCA
vsTCA
+SSRI
TCA
vsTCA
+MAOI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
N(n)
RR/SMD,
95%
CI
WeightchangeAE
Weightgain
‡7%
orreportedasside
effects
1(38)
2.000
0.415,9.650
2(363)
AD
monosuperior
3.807
1.374,10.548z
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Bodyweight
change(SMD)*
0(0)
--2(346)
AD
monosuperior
1.033
0.271,1.794z
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
Bodyweight
change(W
MD:kg)
*
0(0)
--2(346)
AD
monosuperior
2.170
0.708,3.631z
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
EndocrineAE
Sexualdysfunction
(any)
1(38)
0.800
0.253,2.529
1(60)
0.333
0.014,7.870
1(123)
1.197
0.610,2.346
0(0)
--0(0)
--0(0)
--0(0)
--
Erectile
dysfunction
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--OtherAEs
Exanthema/Rash
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--Paresthesia
1(38)
1.667
0.462,6.008
0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--0(0)
--
*Averagechange,endpointonly
ifnoaveragechange.
z p-values:
p<0.05;continuousdata
initalics.
AD:Antidepressant;AE:Adverseevent;MAOI:Monoamineoxidase
inhibitor;mono:Monotherapy;
N:Numberofcomparisons;
n:Numberofparticipants;NaSSA:Noradrenergic
andspecificserotonergic
antidepressant;NDRI:
Norepinephrine-dopaminereuptakeinhibitor;RR:Riskratio;SMD:Standardizedmeandifference;SSRI:Serotonin
reuptakeinhibitors;TCA:Tricyclic
antidepressant;WMD:Weightedmeandifference.
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

3.2.1.3 Treatment characteristicsAll but one study compared SSRI monotherapy with AD aug-mentation from another class (studies = 7, 87.5% of studies,n = 1191), including NaSSAs (studies = 2, n = 365), TCAs(studies = 2, n = 94), NDRIs (studies = 2, n = 505) andNRIs (study = 1, n = 226). One study compared monother-apy with a SARI with augmentation by a SSRI (n = 22)(Table 1).
3.2.2 AE risk with AD + AD augmentation versus AD
monotherapyTen AE outcomes (40.0%) were reported by ‡ 2 studies,allowing meta-analytic calculations, but only 5/25 AEs(20.0%) were reported by ‡ 3 studies, and 4 AEs (16.0%)were not reported at all (Table 2).There was no significant difference between AD monother-
apy and AD augmentation regarding intolerability-relateddiscontinuation (RR = 1.74, 95% CI = 0.39 -- 7.81,p = 0.47; heterogeneity: p = 0.22; studies = 3, n = 323). Incontrast, AD augmentation was associated with a significantlygreater risk of ‡ 1 AE (RR = 1.50, 95% CI = 1.30 -- 1.73,p < 0.001; heterogeneity: p = 0.41; studies = 6, n = 589)(Table 2).Regarding specific AEs, compared with AD monotherapy,
adding a second AD to ongoing AD therapy was associatedwith significantly greater AE burden regarding meta-analyzable 3/25 AEs. These three AEs included ‡ 1 adverseeffect (RR = 1.498, 95% CI = 1.299 -- 1.726, p ‡ 0.001);dry mouth (RR = 2.08, 95% CI = 1.23 -- 3.51, p = 0.006);and ‡ 7% weight gain (RR = 3.81, 95% CI = 1.37 -- 10.55,p = 0.010). In one study each, AD augmentation treatmentwas also associated with significantly more sedation andweight gain (Table 2).
3.3 AD + AD combination versus AD monotherapy3.3.1 Study, patient and treatment characteristics3.3.1.1 Study characteristicsIn total, 15 out of the 23 studies (65.2%) with 25 treatmentarms investigated AD combination treatment, that is, the con-current initiation of 2 ADs at the beginning oftreatment [12,13,27,30,33,35,37,38,40-45]. Combination studieswere double-blind (80.0%, studies = 12, n = 981) or open-label studies (20.0%, studies = 3, n = 238). The mean studyduration was 6.7 ± 2.0 (range = 6 -- 12) weeks.
3.3.1.2 Patient characteristicsAltogether, 1219 patients with MDD were studied. The meanpatient age was 40.9 ± 4.2 (range = 18 -- 84) years, with aminority of male participants (33.2%, studies = 13,n = 376). The severity of depression was reported to be mod-erate to severe in eight studies (n = 352, 28.9% of subjects),while two studies included patients with a severe to very severedepression (n = 290, 23.8% of subjects) and one study was onmildly to moderately depressed patients (n = 135, 11.1% of
subjects). Severity of depression was not reported by one study(n = 173, 14.2% of subjects).
Studies were conducted in outpatients (studies = 6,n = 699) or inpatients (studies = 5, n = 223). Two studiesincluded both, in- and outpatients (n = 95) and two studiesdid not specify the setting (n = 202).
3.3.1.3 Treatment characteristicsMost studies compared SSRI monotherapy with combineduse of an AD from another class (studies = 10, 66.7% of stud-ies, n = 738), that is, NaSSAs (studies = 5, 33.3% of studies,n = 231), TCAs (studies = 3, 20% of studies, n = 106),NDRIs (study = 1, 6.7% of studies, n = 245) or NRIs(study = 1, 6.7% of studies, n = 156). Five studies with eighttreatment arms compared monotherapy with a TCA withcombined use of an AD from the same or another class, thatis, TCA (study = 1, study arms = 2, n = 173), SSRIs(studies = 2, n = 61), MAOIs (studies = 2, study arms = 3,n = 214) and NaSSAs (study = 1, n = 46). Other studiesfocused on the following combinations: MAOI versusMAOI + TCA (studies = 2, study arms = 3, n = 214),NDRI versus NDRI + SSRI (study = 1, n = 245), NRI versusNRI + SSRI (study = 1, n = 156), NaSSA versus NaSSA +SSRI (study = 1, n = 61) and SNRI versus SNRI + NDRI(studies = 1, n = 48).
3.3.2 AE risk with AD + AD combination versus AD
monotherapySixteen AE outcomes (64.0%) were reported by ‡ 2 studies,allowing meta-analytic calculations, but only 11/25 AEs(44.4.0%) were reported by ‡ 3 studies, and only 1 AE(4.0%) was not reported at all (Table 2).
There was no significant difference between AD monother-apy and AD co-treatment regarding the two co-primaryoutcomes, intolerability-related discontinuation (RR = 1.43,95% CI = 0.89 -- 2.32, p = 0.14; heterogeneity: p = 0.83;studies = 10, n = 947) and frequency of ‡ 1 AE (RR = 0.98,95% CI = 0.84 -- 1.15, p = 0.82; heterogeneity: p = 0.14;studies = 3, n = 440) (Table 2).
Regarding specific AEs, compared with AD monotherapy,AD + AD co-treatment was associated with significantlygreater AE burden regarding 2/25 meta-analyzable AEs.These two AEs included tremor (RR = 1.59, 95%CI = 1.01 -- 2.50, p = 0.047 and sweating: RR = 2.02, 95%CI = 1.0 -- 4.0, p = 0.045). In one study, AD combinationtreatment was also associated with significantly more weightgain (Table 2).
4. Conclusion
Results from this first systematic review and exploratory meta-analysis of AEs associated with AD + AD co-treatment com-pared with AD monotherapy studied in randomized con-trolled trials in adults with acute MDD indicate thefollowing: i) although we identified 23 randomized controlled
B. Galling et al.
18 Expert Opin. Drug Saf. (2015) 14(10)
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

studies with a total of 2435 participants, global and specificAE frequencies and, especially, severity are insufficiently andincompletely assessed or reported in the available randomizedcontrolled studies, with only 14/25 (56.0%) AEs beingreported in at least three studies; ii) co-treatment strategiesdo not appear to be associated with significantly greaterintolerability-related discontinuations and incidence of atleast one AE, but were associated with a significantly greaterincidence or severity of 4 of 25 specific reported AEs thanmonotherapy strategies; iii) specific AEs that were more com-mon during AD + AD co-treatment included tremor, sweat-ing, weight gain and clinically significant weight gain;iv) sparse data suggest clinically relevant AE differences acrossindividual AD + AD class combinations, disfavoring theaddition of NaSSAs and TCAs to SSRIs and v) AE types inthe co-treatment groups generally reflect the known AE pro-files of individual AD classes.
5. Expert opinion
Studies comparing AD + AD co-treatment with AD mono-therapy in MDD are scare. Some studies have demonstratedsuperior efficacy regarding the reduction of depressive symp-toms [13,14,40,46], whereas others did not show a benefit ofAD co-treatment strategies compared with AD monother-apy [31,36,38,39]. Reflecting this situation, results from availablereviews and meta-analyses have been heterogeneous regardingthe efficacy of AD + AD co-treatment in patients withMDD [21-23]. Similar to the imbalance of reported and ana-lyzed efficacy versus safety and tolerability data concerningco-treatment versus monotherapy strategies in bipolar disor-der [47], AE data associated with AD + AD co-treatment com-pared with AD monotherapy have been barely and so far onlyincompletely reported or analyzed [21-23].
This systematic review and exploratory meta-analysis ofrandomized studies comparing AD + AD co-treatment toAD monotherapy indicates that AD co-treatment was notassociated with more frequent AE-related treatment discon-tinuations or incidences of at least one AE, but that some spe-cific AEs were more likely or more severe than in the ADmonotherapy groups. Based on the potential pharmacody-namically additive effects of ADs [16,48-51] as well as on poten-tial pharmacokinetic interactions [52-55], we expected morethan isolated disadvantages of the AD + AD co-treatmentgroups that would be reflected by greater dropout rates dueto intolerability and/or more patients suffering from at leastone AE. At least at that level, AD + AD co-treatment doesnot seem to have significant AE disadvantages over ADmonotherapy.
However, it is important to recognize that the data baseconsisted in the majority of studies (65.2%) of combinationtrials in which two ADs were started concurrently. The initi-ation of two ADs at once may have masked individual AEs ofthe second AD due to the fact that period incidence rates arereported and that AEs are most common in the beginning of
treatment. In other words, adverse effects, even mild in natureof the AD used also in the monotherapy arm could have beenmanifold, at least in the beginning, creating a ceiling effect.This idea is supported by the fact that when analyzing sepa-rately augmentation studies where AEs associated with theaddition of a second AD were assessed in greater isolation,AD + AD co-treatment was indeed associated with a higherincidence of at least one AE compared with AD monotherapy.Moreover, tremor, dry mouth, sedation, sweating and differ-ent measures of body weight gain seem to be more likelywhen combining ADs with each other.
While it was still surprising that only few specific AEs weremore likely with AD + AD co-treatment than AD monother-apy, one has to also bear in mind that only little more thanhalf (56%) of analyzable AEs were reported in at least threestudies, limiting the power greatly to show significant differ-ences. Moreover, studies did not compare AEs at differenttimes during the study to assess durability versus developmentof tolerance to certain AEs, and only weight gain was assessedas a scalable outcome, for which severity could be judged.Thus, although there was no difference in AEs leading tostudy discontinuation, it is still possible that AD + ADco-treatment could lead to more severe or impairing AEsthan AD monotherapy. This uncertainty about the degreeand relevance of specific AEs highlights the need for random-ized controlled studies to not only assess efficacy with detailedand frequently repeated rating sales that reflect changes overtime, but to also do the same for adverse effects that are cur-rently mostly assessed by use of global questioning and barely,if ever, analyzed with inferential statistical methods.
Nevertheless, based on the results of this review, potentialefficacy advantages of co-treatment strategies [19-21] need tobe evaluated in light of potential AE disadvantages [16], whichrequire that clinicians regularly asses and document bothefficacy and safety/tolerability of the frequently occurringcombination therapies in patients with MDD as part of rou-tine care [1-3]. Furthermore, although based on a very smallsubset of studies with data, our results of AD co-treatmentgrouped by AD class suggest that AE types reflect the knownprofiles of individual AD classes [56-64], such as sedation andweight gain when adding NaSSAs to SSRIs, and anticholiner-gic AEs when adding TCAs to SSRIs. Whether or not sweat-ing could have been a potential sign of low-grade serotoninsyndrome [48], is unclear based on the available data.
Clearly, the results of this study need to be interpretedwithin its limitations. In particular, this review is limited by:i) the low number of randomized studies comparing ADmonotherapies with AD + AD co-treatment in MDD report-ing AE data; ii) heterogeneous designs, especially with regardto blinding (double-blind: 78.3%, open label: 8.7%, single-blind: 13.0%), measurements and outcomes; iii) lack ofspecific AE rating scales in most studies and for most AEs,precluding a comprehensive assessment, including the evalua-tion of severity, clinical meaningfulness or patient impact aswell and time course of AEs and iv) selective reporting of
Safety and tolerability of antidepressant co-treatment in acute MDD
Expert Opin. Drug Saf. (2015) 14(10) 19
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

assessed AEs or a complete lack of reporting of quantitativeAE data in most of the published studies. Subsequently,subgroup and moderator analyses of individual AD combina-tions, dose levels, patient characteristics, illness phase/episodetype, etc., were not possible.Moreover, the role of pharmacogenetic effects and their
potential influence not only on efficacy, but also on AEswere not taken into account [65,66].To address these shortcomings, more acute trials in patients
with MDD are needed that concurrently assess efficacy andtolerability/safety of different AD co-treatment strategies,especially of agents associated with a low adverse effect burdenor, at least, those with complementary AE profiles. Addition-ally, both short- and long-term studies that report AEs atdifferent follow-up times and fundamental research on differ-ent mechanisms of action and their variability against thebackground of genetics and gene environment interactionsare needed.In summary, the results of this systematic review and
exploratory meta-analysis indicate that AD + AD co-treatment is associated with some increased AE risk that mightdiffer in clinically relevant ways among individual AD classes.Further research is needed in order to better understand theefficacy and safety/tolerability of specific combinations, ide-ally head-to-head and in long-term studies. In clinical care,
AD monotherapy should be considered as a first-line treat-ment and only be augmented with a second AD when mono-therapy is not sufficiently effective. AD + AD co-treatmentshould be restricted to combination treatments that haveproven efficacy, after adequate management of comorbiditiesand after considering co-treatment with non-pharmacologicinterventions, balancing benefits and associated risks carefullythrough ongoing monitoring and shared decision making.
Declaration of interest
CU Correll has been a consultant and/or advisor to or hasreceived honoraria from AbbVie, Acadia, Actavis, Alkermes,Bristol-Myers Squibb, Eli Lilly, Genentech, Gerson LehrmanGroup, IntraCellular Therapies, Janssen/J&J, Lundbeck,MedAvante, Medscape, Otsuka, Pfizer, ProPhase, Reviva,Roche, Sunovion, Supernus and Takeda. He has receivedgrant support from Bristol-Myers Squibb, Otsuka andTakeda. K Hagi is an employee of Dainippon SumitomoPharma. The authors have no other relevant affiliations orfinancial involvement with any organization or entity with afinancial interest in or financial conflict with the subjectmatter or materials discussed in the manuscript apart fromthose disclosed.
BibliographyPapers of special note have been highlighted as
either of interest (�) or of considerable interest(��) to readers.
1. American Psychiatric Association.
Practice guideline for the treatment of
patients with major depressive disorder
[Internet]. American Psychiatric
Association, Washington, DC;
2010. Available from: http://
psychiatryonline.com [Last accessed
8 May 2015]
2. National Institute for Health and
Clinical Excellence. Depression: The
treatment and management of depression
in adults (G90). National Institute for
Health and Care Excellence;
2009. Available from: https://www.nice.
org.uk/guidance/cg91/resources/guidance-
depression-in-adults-with-a-chronic-
physical-health-problem-pdf [Last
accessed 1 September 2015]
3. Harter M, Klesse C, Bermejo I, et al.
Unipolar depression: diagnostic and
therapeutic recommendations from the
current S3/National Clinical Practice
Guideline. Dtsch Arztebl Int
2010;107(40):700-8
4. Kennedy SH, Eisfeld BS, Meyer JH,
Bagby RM. Antidepressants in clinical
practice: limitations of assessment
methods and drug response.
Hum Psychopharmacol
2001;16(1):105-14
5. Nemeroff CB, Entsuah R, Benattia I,
et al. Comprehensive analysis of
remission (COMPARE) with venlafaxine
versus SSRIs. Biol Psychiatry
2008;63(4):424-34
6. Bowden CL, Schatzberg AF,
Rosenbaum A, et al. Fluoxetine and
desipramine in major depressive disorder.
J Clin Psychopharmacol
1993;13(5):305-11
7. Tignol J. A double-blind, randomized,
fluoxetine-controlled, multicenter study
of paroxetine in the treatment of
depression. J Clin Psychopharmacol
1993;13(6 Suppl 2):18S-22S
8. Ansseau M, Papart P, Troisfontaines B,
et al. Controlled comparison of
milnacipran and fluoxetine in major
depression. Psychopharmacology (Berl)
1994;114(1):131-7
9. Bennie EH, Mullin JM, Martindale JJ.
A double-blind multicenter trial
comparing sertraline and fluoxetine in
outpatients with major depression.
J Clin Psychiatry 1995;56(6):229-37
10. Valenstein M, McCarthy JF, Austin KL,
et al. What happened to lithium?
Antidepressant augmentation in clinical
settings. Am J Psychiatry
2006;163(7):1219-25
11. K€ohler S, Unger T, Hoffmann S, et al.
Comparing augmentation with non-
antidepressants over sticking to
antidepressants after treatment failure in
depression: a naturalistic study.
Pharmacopsychiatry 2013;46(2):69-76
12. Blier P, Gobbi G, Turcotte JE, et al.
Mirtazapine and paroxetine in major
depression: A comparison of
monotherapy versus their combination
from treatment initiation.
Eur Neuropsychopharmacol
2009;19(7):457-65
13. Blier P, Ward HE, Tremblay P, et al.
Combination of antidepressant
medications from treatment initiation for
major depressive disorder: a double-blind
randomized study. Am J Psychiatry
2010;167(3):281-8
14. Maes M, Libbrecht I, van Hunsel F,
et al. Pindolol and mianserin augment
the antidepressant activity of fluoxetine
in hospitalized major depressed patients,
including those with treatment resistance.
B. Galling et al.
20 Expert Opin. Drug Saf. (2015) 14(10)
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

J Clin Psychopharmacol
1999;19(2):177-82
15. Fava M, Alpert J, Nierenberg A, et al.
Double-blind study of high-dose
fluoxetine versus lithium or desipramine
augmentation of fluoxetine in partial
responders and nonresponders to
fluoxetine. J Clin Psychopharmacol
2002;22(4):379-87
16. Dodd S, Horgan D, Malhi GS, Berk M.
To combine or not to combine?
A literature review of antidepressant
combination therapy. J Affect Disord
2005;89(1-3):1-11
17. Fleurence R, Williamson R, Jing Y, et al.
A systematic review of augmentation
strategies for patients with major
depressive disorder.
Psychopharmacol Bull 2009;42(3):57-90
18. Chang C-M, Sato S, Han C. Evidence
for the benefits of nonantipsychotic
pharmacological augmentation in the
treatment of depression. CNS Drugs
2013;27(Suppl 1):S21-7
19. De la Gandara J, Aguera L, Rojo JE,
et al. Use of antidepressant
combinations: which, when and why?
Results of a Spanish survey.
Acta Psychiatr Scand 2005;112:32-5
20. Zimmerman M, Posternak M,
Friedman M, et al. Which Factors
Influence Psychiatrists’ Selection of
Antidepressants? Am J Psychiatry
2004;161(7):1285-9
21. Rocha FL, Fuzikawa C, Riera R,
Hara C. Combination of antidepressants
in the treatment of major depressive
disorder: A systematic review and
meta-analysis. J Clin Psychopharmacol
2012;32(2):278-81
.. Latest systematic review and meta-
analysis on the efficacy of
combination/augmentation therapy in
major depressive disorder (MDD).
22. Lopes Rocha F, Fuzikawa C, Riera R,
et al. Antidepressant combination for
major depression in incomplete
responders–a systematic review.
J Affect Disord 2013;144(1-2):1-6
23. Connolly KR, Thase ME. If at first you
don’t succeed: a review of the evidence
for antidepressant augmentation,
combination and switching strategies.
Drugs 2011;71(1):43-64
.. Comprehensive review of different
antidepressant augmentation,
combination and switching strategies.
24. DerSimonian R, Laird N. Meta-analysis
in clinical trials. Control Clin Trials
1986;7(3):177-88
25. Egger M, Davey Smith G, Schneider M,
Minder C. Bias in meta-analysis detected
by a simple, graphical test. BMJ
1997;315(7109):629-34
26. Duval S, Tweedie R. A Nonparametric
“Trim and Fill” Method of Accounting
for Publication Bias in Meta-Analysis.
J Am Stat Assoc 2000;95(449):89-98
27. Akkaya C, Kirli S, Eker SS, et al.
Comparison of the efficacy and safety of
sertraline, reboxetine, and venlafaxine in
patients with major depressive disorder:
A pooled analysis of four randomized,
open-label trials. Klin Psikofarmakol Bul
Bull Clin Psychopharmacol
2010;20(4):274-87
28. Ball S, Dellva MA, D’Souza DN, et al.
A double-blind, placebo-controlled study
of edivoxetine as an adjunctive treatment
for patients with major depressive
disorder who are partial responders to
selective serotonin reuptake inhibitor
treatment. J Affect Disord
2014;167:215-23
29. Rush AJ, Trivedi MH, Stewart JW, et al.
Combining medications to enhance
depression outcomes (CO-MED): Acute
and long-term outcomes of a single-blind
randomized study. Am J Psychiatry
2011;168(7):689-701
. Largest placebo-controlled trial
combining medications in patients
with MDD.
30. Dam J, Ryde L, Svejsø J, et al. Morning
fluoxetine plus evening mianserin versus
morning fluoxetine plus evening placebo
in the acute treatment of major
depression. Pharmacopsychiatry
1998;31(2):48-54
31. Fava M, Rosenbaum JF, McGrath PJ,
et al. Lithium and tricyclic augmentation
of fluoxetine treatment for resistant
major depression: a double-blind,
controlled study. Am J Psychiatry
1994;151(9):1372-4
32. Ferreri M, Lavergne F, Berlin I, et al.
Benefits from mianserin augmentation of
fluoxetine in patients with major
depression non-responders to fluoxetine
alone. Acta Psychiatr Scand
2001;103(1):66-72
33. Fornaro M, Martino M, Mattei C, et al.
Duloxetine-bupropion combination for
treatment-resistant atypical depression:
a double-blind, randomized, placebo-
controlled trial.
Eur Neuropsychopharmacol J Eur
Coll Neuropsychopharmacol
2014;24(8):1269-78
34. Gulrez G, Badyal DK, Deswal RS,
Sharma A. Bupropion as an augmenting
agent in patients of depression with
partial response. Basic Clin
Pharmacol Toxicol 2012;110(3):227-30
35. Lauritzen L, Clemmesen L, Klysner R,
et al. Combined treatment with
imipramine and mianserin: A controlled
pilot study. Pharmacopsychiatry
1992;25(4):182-6
36. Licht RW, Qvitzau S. Treatment
strategies in patients with major
depression not responding to first-line
sertraline treatment: A randomised study
of extended duration of treatment, dose
increase or mianserin augmentation.
Psychopharmacology (Berl)
2002;161(2):143-51
37. Maes M, Vandoolaeghe E, Desnyder R.
Efficacy of treatment with trazodone in
combination with pindolol or fluoxetine
in major depression. J Affect Disord
1996;41(3):201-10
38. Matreja PS, Badyal DK, Deswal RS,
Sharma A. Efficacy and safety of add on
low-dose mirtazapine in depression.
Indian J Pharmacol 2012;44(2):173-7
39. Murphy JE. A comparative trial of
Anafranil, Pertofran and an Anafranil/
Pertofran combination. J Int Med Res
1977;5(1 Suppl):16-23
40. Nelson JC, Mazure CM, Jatlow PI, et al.
Combining norepinephrine and serotonin
reuptake inhibition mechanisms for
treatment of depression: a double-blind,
randomized study. Biol Psychiatry
2004;55(3):296-300
41. O’Brien S, McKeon P, O’Regan M,
et al. Blood pressure effects of
tranylcypromine when prescribed singly
and in combination with amitriptyline.
J Clin Psychopharmacol
1992;12(2):104-9
42. Raisi FR, Habibi N, Nasehi AA,
Mohammadi MR. Combination of
Citalopram and Nortriptyline in
Treatment of Moderate to Severe Major
Depression: A Double-blind, Placebo-
controlled Trial. Iran J Psychiatry
2006;1(1):35-8
43. Stewart JW, McGrath PJ, Blondeau C,
et al. Combination antidepressant
therapy for major depressive disorder:
Safety and tolerability of antidepressant co-treatment in acute MDD
Expert Opin. Drug Saf. (2015) 14(10) 21
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015

speed and probability of remission.
J Psychiatr Res 2014;52:7-14
44. Vezmar S, Miljkovic B, Vucicevic K,
et al. Pharmacokinetics and efficacy of
fluvoxamine and amitriptyline in
depression. J Pharmacol Sci
2009;110(1):98-104
45. Young JP, Lader MH, Hughes WC.
Controlled trial of trimipramine,
monoamine oxidase inhibitors, and
combined treatment in depressed
outpatients. Br Med J
1979;2(6201):1315-17
46. Carpenter LL, Yasmin S, Price LH.
A double-blind, placebo-controlled study
of antidepressant augmentation with
mirtazapine. Biol Psychiatry
2002;51(2):183-8
47. Galling B, Garcia MA, Osuchukwu U,
et al. Safety and tolerability of
antipsychotic-mood stabilizer co-
treatment in the management of acute
bipolar disorder: results from a systematic
review and exploratory meta-analysis.
Expert Opin Drug Saf 2015;1-19
48. Boyer EW, Shannon M. The serotonin
syndrome. N Engl J Med
2005;352(11):1112-20
49. Decoutere L, De Winter S,
Vander Weyden L, et al. A venlafaxine
and mirtazapine-induced serotonin
syndrome confirmed by de- and
re-challenge. Int J Clin Pharm
2012;34(5):686-8
50. Talarico G, Tosto G, Pietracupa S, et al.
Serotonin toxicity: a short review of the
literature and two case reports involving
citalopram. Neurol Sci 2011;32(3):507-9
51. Schellander R, Donnerer J.
Antidepressants: clinically relevant drug
interactions to be considered.
Pharmacology 2010;86(4):203-15
. Comprehensive review of
drug interactions.
52. Paslakis G, Gilles M, Deuschle M.
Clinically relevant pharmacokinetic
interaction between venlafaxine and
bupropion: a case series.
J Clin Psychopharmacol
2010;30(4):473-4
53. Hori H, Yoshimura R, Ueda N, et al.
A case with occurring adverse effects
when cross-over titration from
fluvoxamine to paroxetine associated with
increasing the plasma fluvoxamine level
in major depressive disorder. World J
Biol Psychiatry 2009;10(4 Pt 2):620-2
54. Vlase L, Leucuta A, Farcau D,
Nanulescu M. Pharmacokinetic
interaction between fluoxetine and
metoclopramide in healthy volunteers.
Biopharm Drug Dispos
2006;27(6):285-9
55. Sennef C, Timmer CJ, Sitsen JMA.
Mirtazapine in combination with
amitriptyline: a drug-drug interaction
study in healthy subjects.
Hum Psychopharmacol
2003;18(2):91-101
56. Purgato M, Papola D, Gastaldon C,
et al. Paroxetine versus other anti-
depressive agents for depression.
Cochrane Database Syst Rev
2014;4:CD006531
57. Magni LR, Purgato M, Gastaldon C,
et al. Fluoxetine versus other types of
pharmacotherapy for depression.
Cochrane Database Syst Rev
2013;7:CD004185
58. Cipriani A, Koesters M, Furukawa TA,
et al. Duloxetine versus other anti-
depressive agents for depression.
Cochrane Database Syst Rev
2012;10:CD006533
59. Cipriani A, Purgato M, Furukawa TA,
et al. Citalopram versus other anti-
depressive agents for depression.
Cochrane Database Syst Rev
2012;7:CD006534
60. Cipriani A, La Ferla T, Furukawa TA,
et al. Sertraline versus other
antidepressive agents for depression.
Cochrane Database Syst Rev
2010(4):CD006117
61. Omori IM, Watanabe N, Nakagawa A,
et al. Fluvoxamine versus other anti-
depressive agents for depression.
Cochrane Database Syst Rev
2010(3):CD006114
62. Watanabe N, Omori IM, Nakagawa A,
et al. MANGA (Meta-Analysis of New
Generation Antidepressants) Study
Group. Safety reporting and adverse-
event profile of mirtazapine described in
randomized controlled trials in
comparison with other classes of
antidepressants in the acute-phase
treatment of adults with depression:
systematic review and meta-analysis.
CNS Drugs 2010;24(1):35-53
63. Nakagawa A, Watanabe N, Omori IM,
et al. Milnacipran versus other
antidepressive agents for depression.
Cochrane Database Syst Rev
2009(3):CD006529
64. Cipriani A, Furukawa TA, Salanti G,
et al. Comparative efficacy and
acceptability of 12 new-generation
antidepressants: a multiple-treatments
meta-analysis. Lancet Lond Engl
2009;373(9665):746-58
65. Kovacs D, Gonda X, Petschner P, et al.
Antidepressant treatment response is
modulated by genetic and environmental
factors and their interactions.
Ann Gen Psychiatry 2014;13:17
66. Fabbri C, Porcelli S, Serretti A. From
pharmacogenetics to pharmacogenomics:
the way toward the personalization of
antidepressant treatment. Can J
Psychiatry Rev Can Psychiatr
2014;59(2):62-75
AffiliationBritta Galling1 MD, Amat Calsina Ferrer2 MD,
Margarita Abi Zeid Daou3 MD,
Dinesh Sangroula1 MD,
Katsuhiko Hagi1,4 PhD &
Christoph U Correll†1,5,6,7 MD†Author for correspondence1The Zucker Hillside Hospital, Psychiatry
Research, North Shore - Long Island Jewish
Health System, Glen Oaks, NY, USA
Tel: +1 71 84 70 48 12;
Fax: +1 71 83 43 16 59;
E-mail: [email protected] d’Assistencia Sanit�aria, Hospital de Santa
Caterina, Salt, Spain3Vanderbilt Psychiatric Hospital, Nashville, TN,
USA4Dainippon Sumitomo Pharma Co, Ltd, Osaka,
Japan5Hofstra North Shore LIJ School of Medicine,
Hempstead, NY, USA6The Feinstein Institute for Medical Research,
Manhasset, NY, USA7Albert Einstein College of Medicine, Bronx, NY,
USA
B. Galling et al.
22 Expert Opin. Drug Saf. (2015) 14(10)
Dow
nloa
ded
by [
67.8
7.23
6.65
] at
08:
37 1
1 Se
ptem
ber
2015