-
8/9/2019 Sacrum & Coccyx
1/26
m & Coccyx
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Printout from Orthoteers.com website, member id 1969. 2007 All
rights reserved.Please refer to the site policies for rules on
diseminating site content.
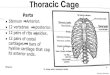
Sacrum & Coccyx
Sacroiliac joint pain
Elicited with patient lying on the affected side without support
(Gaenslen's test), directcompression or FABER test (flexion
abduction and external rotation)
Local anaesthetic injection can be diagnostic and
therapeutic
Fusion only indicated when an infection is present
Ideopathic coccydynia
Frequently associated with psychological conditions
Four types of coccyx:
Type of coccyx Coccyx morphology Coccydynia
1 Slight forward curve, apex dorsal Rare11 Marked curve, apex
ventral Common111 Sharp angulation between coccyx
segmentsCommon
1V Ventral subluxation of segments Common
Conservative treatment, donut pillow, NSAIDS, local steroid
injection
Complete or partial coccygectomy, in type 111 or 1V may help but
hgh risk ofcomplications with wound
Sacral Insufficiency fracture
Occurs in older patients with osteopenia and no history of
trauma
Treat conservatively with rest analgesia
[ Close Window ]
-
8/9/2019 Sacrum & Coccyx
2/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Printout from Orthoteers.com website, member id 1969. 2007 All
rights reserved. Please refer to thesite policies for rules on
diseminating site content.
Spinal Injuries - Principles
General Principles Initial Management Definitive Management
Neurological Assessment Incomplete Cord Injuries Long Term
Management
GENERAL PRINCIPLES [Back To Top]
Complications of spinal injury
Neurological damage
Damage to vertebral column causing deformity and pain
Stable injuries
Vertebral components won't be displaced by normal movement.
An undamaged spinal cord is not in danger
There is no development of incapacitating deformity or pain
Unstable injuries
Further displacement of the injury may occur
Loss of 50% of vertebral height
Angulation of thoracolumbar junction of > 20 degrees
Failure of at least 2 of Denis's 3 columns
Compression # of three sequential vertebrae can lead to
posttraumatic kyphosis
Anatomical considerations
The upper thoracic spine (T1-T10) is protected by the ribs,
sternum and the facet joint orientation
At the thoracolumbar junction there is a fulcrum of increased
motion, so there is increased risk of injury
The middle thoracic spine is a vascular 'watershed', vascular
insult can cause cord ischaemia (Artery ofAdamkiewitz)
Cauda equina begins at L1-L2. Lesions below L1 have a better
prognosis as nerve roots, not cord areaffected
Mechanisms of injury
-
8/9/2019 Sacrum & Coccyx
3/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Hyperextension -common in the neck. Anterior ligaments and disc
may be damaged.1.
Flexion- If posterior ligaments intact, wedging of vertebral
body occurs. If posterior ligaments torn, maycause subluxation
2.
Axial compression- Causes burst #s. Bony fragments may be pushed
into spinal canal3.
Flexion, with posterior distraction- May disrupt middle and
posterior columns.4.
Flexion with rotation- Causes dislocation with or without
#.5.
Shear.6.
SPINAL SHOCK
Diaphragmatic breathing1.
Flaccid limbs2.
warm periphery3.
decr. pain sensation4.
reduced reflexes5.
erection6.
Urinary retention7.
decr. BP + decr. pulse rate = Neurogenic8.
decr. body temp.9.
Return of bulbocavernosus reflex at 24hrs= end of Spinal
Shock10.
INITIAL MANAGEMENT OF SPINAL INJURY PATIENTS [Back To Top]
ABC, Spinal board, hard collar
History
Strongly suspect spinal injury if any major accident,
unconscious patient, fall from a height, sudden jerkof neck after
rear end car collision, facial injuries or head injury
Ask about neck or back pain, numbness, tingling, weakness,
ability to pass urine
Examination
Logroll- look for bruising, palpate for a step, tenderness
Repeated neurological examination to determine neurological
damage and its progression/resolution
Thorough overall examination for fractures etc as patient may
not feel pain
Imaging
Xrays-Cervical spine AP, Lateral including C7/T1, open mouth
view of odontoid. Swimmers view or pullarms down. AP and lateral
view of other tender areas of spine
CT scan shows bony injury
MR scan shows soft tissue involvement
If neurological damage
Catheterise
Note reduced BP and bradycardia due to neurogenic shock
(temporary generalised sympathectomy).Rule out hypotension due to
haemorrhage elsewhere. May need treatment with vasopressors, not
fluid
-
8/9/2019 Sacrum & Coccyx
4/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
resuscitation.
Invasive monitoring required
Give methylprednisolone IV 30mg/kg over 15 mins then 5.4mg/kg/hr
for next 23 hours. Needs to begiven within 8 hrs. Discuss with the
spinal team.
Attend to skin by turning
Cochrane Database Syst Rev 2000;(2):CD001046
Pharmacological interventions for acute spinal cord injury.
Bracken MB; Department of Epidemiology and Public Health, Yale
School of Medicine, 60 College street,Box 20834, New Haven,
Connecticut 06520-8034, USA. [email protected]
BACKGROUND: Acute spinal cord injury is a devastating condition
typically affecting young people with a
preponderance of males. Pharmacological treatment in the early
hours of the injury is aimed at reducing theextent of permanent
paralysis during the rest of the patient's life.
OBJECTIVES: To review randomized trials of pharmacological
therapies for acute spinal cord injury.
SEARCH STRATEGY: The review draws on the search strategy
developed by the Cochrane Injuries Group.In addition, files of the
National Acute Spinal Cord Injury Study have been reviewed.
SELECTION CRITERIA: All published or unpublished randomized
controlled trials of pharmacologicaltreatment for acute spinal cord
injury in any language.
DATA COLLECTION AND ANALYSIS: Data have been abstracted from
original trial reports. For theNASCIS, Japanese and French trials,
additional data (e.g. SDs) have been obtained from the
originalauthors.
MAIN RESULTS: There are few trials in this area of medical care.
Only one therapy has been extensivelystudied, methylprednisolone
sodium succinate, which has been shown to improve neurologic
outcome up toone year post injury if administered within 8 hours of
injury and in a dose regimen of: bolus 30mg/kgadministered over 15
minutes with a maintenance infusion of 5.4 mg/kg per hour infused
for 23 hours. Theinitial North American trial was replicated in a
Japanese trial but not in the one from France. Data has
beenobtained from the latter study to permit appropriate
meta-analysis of all three trials. This analysis
indicatessignificant recovery in motor function after
methylprednisolone therapy. A more recent trial indicates that
ifmethylprednisolone therapy is given for an additional 24 hours
(for a total of 48 hours), additionalimprovement in motor
neurologic function and functional status is observed. This is
particularly observed if
treatment cannot be started until between 3 to 8 hours after
injury. The same methylprednisolone therapyhas been found effective
in whiplash injuries and a modified regimen found to improve
recovery after surgery
for lumbar disc disease.
REVIEWER'S CONCLUSIONS: High dose methylprednisolone steroid
therapy is the only pharmacologicaltherapy shown to have efficacy
in a Phase Three randomized trial when it can be administered
within 8 hours
of injury. High dose methylprednisolone has been accepted as
standard therapy in many countries. A recenttrial indicates
additional benefit by extending the maintenance dose from 24 to 48
hours if start of treatmentmust be delayed to between 3 and 8 hours
after injury. There is an urgent need for more randomized trials
of
pharmacological therapy for acute spinal cord injury.)
DEFINITIVE MANAGEMENT [Back To Top]
Objectives
Preserve neurological function1.
Relieve reversible nerve or cord compression2.
Stabilise the spine3.
Rehabilitate patient4.
With no neurological deficit
If stable spinal injury- pain relief, collar or brace. Exception
can be a burst #, ? operatively stabilise
If unstable injury, reduce and hold secure until bone / ligts
heal with ORIF or traction in tongs, halo vest
-
8/9/2019 Sacrum & Coccyx
5/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
With complete sensory and motor loss
Usually an unstable injury
Only consider conservative management for high thoracic
injuries
Early operative stabilisation- to help with nursing, prevent
spinal deformity and pain. Speeds up rehab
With Incomplete neurological loss
Stable injury- conservative bed rest, brace. Exception can be
burst # ?operatively stabilise
Unstable injury- early reduction and stabilisation
Site for Pedicle Screw Insertion:
NEUROLOGICAL ASSESSMENT IN SPINAL INJURIES [Back To Top]
Aims
To determine the level of the lesion- counted as the lowest
level at which neurological function is intactbilaterally
To determine whether damage is complete/ incomplete
To determine prognosis
May be difficult until period of spinal shock (flaccidity,
areflexia) is over (24-48 hrs after injury)
1. Tone
2. Power
Diaphragm C3-4-5Shrugging shoulders C4Flex elbows C5,6Extend
elbows C7
Abduct fingers C8Active chest expansion T1-T12Hip flexion L2Knee
extension L3-4
Ankle dorsiflexion L5-S1Ankle plantar flexion S1-S2Eversion of
foot L5Inversion of foot L4
-
8/9/2019 Sacrum & Coccyx
6/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
MRC Power Grading
0 No active contraction1 Visible contraction without movement2
Movement with gravity eliminated3 Movement against gravity4
Movement against resistance but weak5 Normal power
3. Reflexes
Biceps C5-6Triceps C6-7Supinator C5-6Knee jerk L3-4
Ankle jerk L5-S1Plantar response If upgoing = UMN lesion
Abdo cutaneous reflexes If lost = UMN lesionBulbo cavernosis
reflex Pull penis, causes anal sphincter tightening
If returned, period of spinal shock is over
4. Sensation
5. PR
Always perform this to assess S2, 3, 4
INCOMPLETE CORD INJURIES [Back To Top]
-
8/9/2019 Sacrum & Coccyx
7/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Syndrome injury/pathology Features Prognosis
BrownSequard
Penetrating trauma Loss of ipsilateral motor function and
vibration and positionsense, contralateral loss of pain and
temp
Best
Anterior cord Flexion compression Motor loss , dorsal columns
spared PoorCentral cord Age>50 extension
injuriesAffects upper limbs more than lower limbs, motor
andsensory loss
Fair
LONG TERM CARE OF NEUROLOGICALLY INJURED SPINAL PATIENTS [Back
To Top]
Frankel grade- Useful in monitoring functional improvement from
spinal cord injury
Frankel grade FunctionA Complete paralysisB Sensory function
only below injury levelC Incomplete motor function below injury
level (1or 2/5)D Fair to good motor function (3-4/5) below injury
levelE Normal function below injury level
Highest mortality in the first 2 weeks
Most common causes of morbidity and mortality:
Respiratory insufficiency - atelectasis and pneumonia. Any
deficit proximal to T10 causes increasedreliance on the diaphragm.
Treat with IPPV, physio, tracheostomy and suction,
repeatedbronchoscopy
1.
Paralytic ileus - Keep NBM initially for 24 hours, IV
fluids2.
GI bleeds from haemorrhagic gastritis -? Due to unopposed
parasympathetic activity. Give H2antagonists
3.
Urological complications- UMN lesion of bladder, catheterise
intermittently to stop urinary stasis andinfection. LMN, may manage
with suprapubic pressure to relieve bladder
4.
Pressure sores - Turn every 2 hrs, teach to relieve pressure
later5.
Joint contractures - Passive movements +/- splintage 2x per
day6.
Psychological withdrawal- multi disciplinary approach.7.
-
8/9/2019 Sacrum & Coccyx
8/26
l Injuries - Principles
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
[ Close Window ]
-
8/9/2019 Sacrum & Coccyx
9/26
l Stenosis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Printout from Orthoteers.com website, member id 1969. 2007 All
rights reserved. Please refer to thesite policies for rules on
diseminating site content.
Spinal Stenosis
Anatomy Aetiology Pathophysiology Clinical
Investigations Natural History Treatment References
Lumbar spinal stenosis is one manifestation of the general
process of spinal degeneration that occurs with aging,and often
becomes symptomatic in the seventh and eighth decades of life.
Stenosis = narrowing of a hollow tubular structure.
Anatomy [Back To Top]
The central canal of the spinal column conveys the spinal cord
in the cervical, thoracic and upper lumbarlevels.In most
individuals, the spinal cord ends by the L1 level; below this level
the remaining lumbar and sacralnerve roots travel as the cauda
equina.The nerve roots are more tolerant of chronic pressure than
the spinal cord, which is why an individual maytolerate a higher
degree of stenosis in the lower lumbar spine than in the cervical
or thoracic region.The boundaries of the central canal vary with
the level of the vertebral body:
At the level of a vertebral body, the canal is bordered by the
body itself anteriorly, the pedicleslaterally, and the laminae
posteriorly. This is the site that is affected in cases of
congenitalstenosis , where the pedicles are typically
shortened.
At the level of the intervertebral disc, the anterior border is
formed by the annulus, the posterolateralborders by the facet
joints and capsules, and the posterior border by the ligamentum
flavum. Theseare the structures that are most affected by
degenerativeprocesses .
The dimensions of the spinal canal and foramen are influenced by
dynamic and postural factorswhen a person rises from recumbency to
standing, the resulting axial load on the intervertebral disccauses
further bulging of the annulus, which in turn further compromises
the central canal and theforamen.
The foramina decrease in size while the nerve roots increase in
diameter as you move down the
spine . Thus the lumbar spine is most commonly affected.
Aetiology [Back To Top]
Classification -Arnoldi (1976) [Picture ]
CongenitalDevelopmental1.
Achondroplasia2.
1.
AcquiredDegenerative1.
2.
-
8/9/2019 Sacrum & Coccyx
10/26
l Stenosis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Spondylolistheticworseifimposedonadevelopmentalnarrowing
DiscHerniation
2.
Degenerative& DiscHerniation
3.
Degenerative&congenital
4.
Others:Paget's1.Spinal tumour2.Infection
(TB)3.Post-surgery4.Trauma5.
3.
The L4-L5 segment is the most commonly affected, followed by the
L3-L4.Men are more commonly affected than women, because their
spinal canals are narrower at the L3-L5levels.
Pathophysiology [Back To Top]
Narrowing of the central canal and/or intervertebral foramina is
due to:
annular bulging1.bone spur formation2.facet joint
enlargement3.ligamentous hypertrophy4.
Classification by site:
A. Central stenosis
Compression of the thecal sac & cauda equinacaused by:
arthritic facets with medial encroachment; congenitally narrow
canal ('trefoil' shape);spondylolisthesis; Central disc herniation;
Posttraumatic; Post-surgical
B. Lateral stenosi s [ Picture]
compression of the nerve rootsuperior articular facet
enlargement; lateral disc herniation; ligamentum flavum
hypertrophy; uncinatespurring
lateral recess stenos is - affects the traversing (lower) nerve
root1.
-
8/9/2019 Sacrum & Coccyx
11/26
l Stenosis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
foraminal stenosis - affects the exiting (upper) nerve
root2.extra-forami nal (far-out)3.
Mechanism: (Howe et al. Pain , 1977)
when standing or walking the lumbar lordosis increases the
stenosissubarachnoid obstruction occursdiffusion of fluid from the
endoneurium into the subarachnoid space is impairedincreased
endoneurial pressure-> 'Compartment Syndrome' in the nerve
roots-> conduction disturbancesa nerve which has been
repetitively injured becomes more easily irritated by dynamic
factors
-
8/9/2019 Sacrum & Coccyx
12/26
l Stenosis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Clinical [Back To Top]
Virtually all individuals in their seventies have at least some
degree of spinal stenosis on imaging studies, but only afraction
manifest the true symptoms of central and/or foramenal
stenosis.
Central stenosis:
neurogenic claudication. (from compression on the cauda
equina)increased unsteadiness or loss of balancefeeling better if
they walk stooped forwardRarely - urinary incontinence & cauda
equina syndrome
Foramenal stenosis:
Radicular signs from narrowing of the lateral recess or the
neural foramen.
Physical examination can be unimpressive in patients with
central stenosis.
ambulate with a forward-leaning posture and a moderately
broad-based gait.check distal pulses to screen for vascular causes
of claudication.Stress Test = walk until symptoms occur
Difference to Vascular claudication:
Activity Vascular Claudication Neurogenic Claudication
Walking Distal-proximal pain; calf pain Proximal-distal thigh
pain
Uphill Walking Symptoms develop sooner Symptoms develop
later
Rest relief with standing relief with sitting or bending
Bicycling Symptoms develop No symptoms
-
8/9/2019 Sacrum & Coccyx
13/26
l Stenosis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Lying Flat Relief May increase symptoms
Investigations [Back To Top]
X-rays:
bone spurs, decreased disc height and facet hypertrophy in older
patients.
CT:
more accurate and detailed picture of the bony anatomyless
accurate than MRI in estimating the degree of compromise of the
soft tissue elements.thus can underestimate the degree of
stenosisspinal canal < 10mm AP diameter = Absolute Stenosis
MRI: (without gadolinium)
currently represents the "gold standard" in the evaluation of
central stenosis.It allows the visualization of the disc, neural
elements, ligamentum flavum & thecal sac
Epiradicular Nerve root block:
improvement of radicular symptoms after injection of anaesthetic
is suggestive of lateral (foraminal)stenosis.
Myelography: is no longer routinely necessary, although it can
be useful in selected cases
Natural History [Back To Top]
2 studies following 49 patients (Hayashi) and 32 patients
(Johnsson) for 5 years (with non-operative treatment):
Symptoms unchanged in 60-70%Worse in 15-20%Improved in
15-20%
Treatment [Back To Top]
Non-Operative:
NSAIDs1.
Muscle relaxants2. Antidepressants for chronic radicular
pain3.Epidural & nerve root block steroid injections - good
long-term relief in patients with foramenal or lateralrecess
stenosis
4.
Physiotherapy (with massage, ultrasound, TENS, braces or
supports, acupuncture, biofeedback, hot orcold packs, traction, or
manipulation) can offer symptomatic relief of radicular or low back
pain, but not forclaudicant symptoms.
5.
Flexion brace (Williams brace) - prevents lordosis. Not well
tolerated.6.Calcitonin7.
Operative
Indications:
Severe neurological symptoms1.
failed conservative treatment + impaired ADL (activities of
daily living)2.
Decompression Procedures
Central Stenosis
Partial Laminectomy - for patients without segmental instability
(eg. spondylolisthesis)Total Laminectomy - should be avoided
Lateral Recess Stenos is
Medial Facetectomy - the medial margin of the superior facet,
facing the spinal canal, is resectedonly
Foraminal & extra-foraminal Stenosis
extra-spinal approach to dorsal root ganglion (in the
intervertebral foramen)resect the lower lamina laterally &
caudally until the dural sac is seen; pediculotomy may be
required
-
8/9/2019 Sacrum & Coccyx
14/26
l Stenosis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Spinal Fusion
preoperative instabilty (spondylolisthesis)instability expected
from resection of the facet jointsagittal inclination of the facet
jointhigh demand post-op activities
Operative Results
Variable due to:
not all stenotic sites necessarily cause symptoms, therefore
selecting decompression levels can be difficult1.insufficient
decompression2.incorrect levels3.post-operative
instability4.regrowth of resected tissue & scarring5.
Multi-level involvement does not do well due to post-op
instability (should consider fusion, but very invasive)
Careful attention to patient selection and meticulous operative
planning are important in optimizing surgicaloutcome.
Refereneces: [Back To Top]
Current Orthopaedics. Mini-Symposium: 13(3). July
1999.ApleyMiller
[ Close Window ]
-
8/9/2019 Sacrum & Coccyx
15/26
Embryology
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Printout from Orthoteers.com website, member id 1969. 2007 All
rights reserved. Please refer to the site policies forrules on
diseminating site content.
Spine Embryology
Vertebral Growth
Vertebral formation at 3-5 weeks with segmentation occurring at
6-8 weeks
Each vertebrae forms from 2 adjacent sclerotomes and so becomes
an inter segment structure
Notochord degenerates but between vertebrae it persists to form
the nucleus pulposusDuring the 6th week chondrification occursTwo
centres in each centrum fuse at the end of the embryonic period
resulting in one centre evident in the centrum after thisperiod
(defects here -> hemi vertebrae)2 Centres in the neural arches
fuse with each other and the centrumThe two 1/2's of the neural
arch usually fuse in the first year and these to the centrum in ~
the 3rd to 6th year
At about puberty five secondary centres appear (upper and lower
body, and one in the tip of the TPs and spinous process)
Ossification begins in the embryonic period and ends at about 25
years.Longitudinal growth is via superior and inferior
apophysis.
Horizontal growth is by periosteal apposition
Spinal canal enlarges by growth of the pedicles and posterior
elements, enlarging rapidly from birth to five years and more
slowlyfrom 5-10 years.
The spinal canal reaches its final dimensions relatively early
compared with the continual growth of the rest of the
vertebralstructuresThe final height of vertebral column is
reachedgirls by 11 - 13 yearsboys by 14 - 16 yearsBoys grow ~ 3.5cm
and girls 1.5cm after Risser IV
-
8/9/2019 Sacrum & Coccyx
16/26
Embryology
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
The Developing Human - Moore & Persuad
[ Close Window ]
-
8/9/2019 Sacrum & Coccyx
17/26
dylolysis & Spondylolisthesis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Printout from Orthoteers.com website, member id 1969. 2007 All
rights reserved. Please refer to the site policies for rules on
diseminating site content.
Spondylolysis & Spondylolisthesis
SPONDYLOLYSIS
caused by a defect in the pars interarticularis
usually a fatigue fracture from repetitive hyperextension
stresses (gymnasts)
most common cause of LBP in adolescents
Radiology
plain x-rays demonstrate 80% of lesions
oblique views - additional 15% picked up - 'Scottie dog' sign
(Lachapelle)
CT - may miss fracture
Bone Scan - incr. uptake indicates an acute lesion which will
probably heal
Non-union is common
SPONDYLOLISTHESIS
"spondy" refers to the vertebrae and "listhesis" means "to
slip"
usually L4/5 and L5/S1
Normally laminae & facets constitute a locking mechanism
preventing forward slippage [see Video ]
Classification: (Newman, Wiltse, McNab)
Congenital/Dysplastic (20%)superior articular facets are
congenitally defectiveassociated with spina bifida occulta
Isthmic (50%)
caused by spondylosis (L5/S1)
a. Lytic-fatigue fracture of the pars interarticularisb.
Elongated but intact pars interarticularisc. Acute fracture of the
pars interarticularis
Degenerative (25%) degenerate facet joints (L4/L5)
Post-traumatic
from an acute fracture in some other portion of the vertebra
that allows a slip to occur.An isolated pars fract ure is not seen
with this lesion.
Pathological tumours, Paget's
Post-operative
Severity of Slip:
1. Percentage of slip of the AP diameter of the vertebra
below:
Grade I - < 25%
Grade II - 25-50%
Grade III - 50-75%
Grade IV - 75-100%
Grade V - >100% (spondyloptosis)
2. Slip Angle
normal = > 0 degrees
Clinical
-
8/9/2019 Sacrum & Coccyx
18/26
dylolysis & Spondylolisthesis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
may be discovered only incidentally on x-rays
injury may aggravate any symptoms
usually pain begins insidiously during the second or third
decade with walking and standing
Flattening of the back
Spinous process step-off
Claudication may signal the development of lateral stenosis
Radiology
Plain x-rays should be taken standing
grade slip
slip angle
Oblique x-rays
Bone scans - (see above)
MRI
evaluates disc
but can see a pseudodisc herniation due to rotatory element of
slip
Treatment
Non-operative:
reduce sports
adolescents - x-rays every 6 months until maturity
Risk factors for Slip progression:
young age at presentation1.
females2.
slip angle > -10 degrees3.
high grade slip4.
dome shaped sacrum5.
inclined sacrum (>30deg. beyond vertical)6.
Operative:
Indications:
slip > 50% or progressing in adolescents
back and/or leg pain unresponsive to non-operative treatment
functionally significant neurological deficit
Grade I & II - in situ fusion (& decompression);
Repair of the pars defect & fixation using a lag screw or
wires has been described for low grade slips (
-
8/9/2019 Sacrum & Coccyx
19/26
dylolysis & Spondylolisthesis
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
[ Close Window ]
-
8/9/2019 Sacrum & Coccyx
20/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Printout from Orthoteers.com website, member id 1969. 2007 All
rights reserved.Please refer to the site policies for rules on
diseminating site content.
Waddells Nonorganic Signs
Screening for Psychological Factors in Patients With Low
Back Problems: Waddell's Nonorganic Signs
Adapted from: Scalzitti DA. Screening for psychological factors
in patients with low back
problems: Waddell's nonorganic signs. Phys Ther.
1997;77:306-312.
For the majority of patients with low back pain (LBP), the cause
of their pain is unknown.1
Psychological factors, which may include behavioral, cognitive,
or somatoform components,can be just as important as the diagnosis
of pathology affecting the low back in a patient's
recovery from a low back problem.2-5A recent US Agency for
Health Care Policy andResearch clinical practice guideline
recommends exploration of psychological factors when anindividual
with an acute low back problem is having difficulty regaining his
or her tolerance to
activity.4
Feuerstein and Beattie5 discussed several biobehavioral
instruments that can be used toidentify psychological factors in
individuals with LBP. If factors are identified that are
potentialcontributors to the low back problem, the physical
therapist can then refer the patient to theappropriate
professional. Routine application of these instruments, however,
may beimpractical during physical therapy examinations because of
the time required foradministration and scoring as well as the
expertise needed to interpret the results. Thus, thereis a need for
a brief screening tool to help identify patients who may require
more detailedpsychological testing. A review of the description and
diagnosis of psychological disorders thatmay relate to LBP is
beyond the scope of this update. For further information on these
areas,
the reader is referred elsewhere.5-7
Signs of organic problems are findings from the physical
examination that indicate thepresence of pathology or disease.
Paresthesia over the lateral border of the foot, for example,is a
sign for S-1 nerve root involvement. Signs of nonorganic problems,
in contrast, are findings
that deviate from the usual presentation of disease.8 Both
organic and nonorganic signs maybe present in a patient with LBP.
Therefore, the presence of nonorganic signs should not beequated
with malingering or the presence of a psychological problem, but
only with the needfor further investigation.
Waddell et al8 described a group of signs that indicate the
presence of nonorganic problemsfor patients with LBP. Waddell has
also referred to these signs as "behavioral signs" or
"inappropriate signs."2,9 Testing for these signs is performed
as part of the physical
examination and takes less than 1 minute.8 Nonorganic signs have
been used to describedifferent characteristics of patients with
LBP. The purpose of this update is to describe the useof Waddell's
nonorganic signs as a screening tool for psychological factors in
patients withLBP. Additionally, the relationship between the
nonorganic signs and physical impairments,disability, and treatment
outcomes will be discussed.
Waddell's Nonorganic Signs
In the early 1900s, nonorganic signs were frequently used to
detect malingering in patients with
LBP.10,11As medical and psychological knowledge progressed, it
became clear that thediagnosis of malingering may have been based
on overly simplistic assumptions, and the useof these nonorganic
signs fell out of favor. The modern use of nonorganic signs for
patients
with low back problems increased greatly after 1980, when
Waddell et al8 grouped eight signsinto five types. These five
types, or categories of signs, are tenderness, simulation,
distraction,regional disturbances, and overreaction (Table).
Waddell and colleagues investigated 16 othersigns, including grip
strength, lumbar sensory changes, and pretibial tenderness, but did
notinclude them in their final battery because of poor intertester
and intratester reliability, overlapwith other signs, and
difficulty for the examiner to learn.
According to Waddell et al,8 a nonorganic sign (an indication of
a nonorganic contribution to apatient's low back problem) observed
during the physical examination is scored as positive. If asign is
positive, then that type of nonorganic sign is present. One
nonorganic sign in isolationmay be present with some organic
conditions and should therefore be discounted. A sensory
-
8/9/2019 Sacrum & Coccyx
21/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
regional disturbance, for example, may be present in persons
with spinal stenosis with multiplenerve root involvement.
Waddell et al8 found that the presence of three or more types of
nonorganic signs correlatedwith the results of psychological tests
indicating problems. According to Waddell et al, thepresence of a
single sign is not associated with an indication of psychological
problems. Thepresence of three or more types of nonorganic signs
has been the most consistently usedcriterion for the finding of a
positive Waddell's nonorganic signs test, although other
methods
have been proposed.12,13 Unless otherwise specified in this
update, therefore, a positive testfor nonorganic signs refers to
finding the presence of three or more types of nonorganic
signs.
A negative nonorganic signs test is the finding of only one or
two types of signs, although apatient may have more than three
nonorganic signs because of multiple signs within a
specifictype.
Reliability
Agreement was high (86%) for two examiners in detecting the
presence of nonorganic signs in
a group of 50 patients with chronic LBP.8Agreement between
examinations in the samepatients was 85%. (The mean length of time
between examinations was 23 days.) McCombe
et al14 reported poor intertester reliability between two
orthopedic surgeons and between asurgeon and a physical therapist
in detecting individual nonorganic signs. Confidence intervalsof
Kappa coefficients included zero for the nonorganic signs of
tenderness and regionaldisturbances, suggesting that agreement was
not better than chance. McCombe et al,however, did not examine the
reliability of the examiners in determining the presence of three
or
more nonorganic signs. This finding should caution clinicians
regarding the use of positivenonorganic signs in isolation.
The nonorganic sign of overreaction requires the clinician to
make judgments based onobservations of the patient's behavior. The
other signs are from tests conducted during routineexaminations.
The presence of overreaction, therefore, may be more difficult to
identify thanother nonorganic signs. Several methods and
instruments can be used to quantify observation
of a patient's behavior during the physical examination.15 Keefe
and Block16 described amethod for observing overt pain behaviors to
provide a means of identifying the presence ofguarding, bracing,
rubbing, grimacing, and sighing during a physical examination.
Waddell and
Richardson9 obtained a Pearson product-moment correlation
coefficient of .65 whenexamining the relationship between the
nonorganic signs test and overt pain behaviors in 120patients who
had LBP for at least 3 months. Measurements obtained with the UAB
PainBehavior Rating Scale, which is one instrument for measuring
pain behavior, were also highly
correlated (r=.73) with the results of the nonorganic signs test
in 103 patients with LBP.17
Nonorganic Signs and Psychological Findings
In their original study of nonorganic signs, Waddell et al8
reported a correlation between thepresence of nonorganic signs and
scores on the hypochondriasis, depression, and hysteriascales of
the Minnesota Multiphasic Personality Inventory. These scales of
the MinnesotaMultiphasic Personality Inventory traditionally
represent a measure of psychological distress inpatients with LBP.
In addition, correlations have been found between the presence
ofnonorganic signs and other psychological instruments, including
the disease affirmation and
hypochondrial disturbance scales of the Illness Behavior
Questionnaire (IBQ),18 the Distress
and Risk Assessment Method (DRAM),19 and pain drawings.8,20
Waddell et al8 caution,however, that nonorganic signs should not be
overinterpreted and used as substitutes forcomprehensive
psychological assessment. Instead, they should be used as part of
an
examination to identify patients who require more detailed
testing.
The sensitivity and the specificity of eight psychometric
instruments, including Waddell'snonorganic signs test, for
detecting psychological disturbances in patients with LBP were
determined in a group of 264 persons.12 Results from each
instrument were compared with a"gold standard" of psychological
disturbance, which was defined as a positive response tothree or
more of the eight psychometric tests. Specificity of the nonorganic
signs for correctlyidentifying patients who were nonpsychologically
disturbed was 86% in men and 84% inwomen. Sensitivity of the
nonorganic signs for correctly identifying patients who
werepsychologically disturbed was 44% in men and 48% in women. This
study was limited,however, by the lack of a universal "gold
standard" of psychological disturbances with which tocompare the
different instruments. In the study, measurements with each
instrument werecompared with a compilation of measurements obtained
with the other instruments.Correlations among the eight instruments
may not have been found if the instruments were
-
8/9/2019 Sacrum & Coccyx
22/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
measuring different aspects of psychological disturbances.
Nonorganic Signs and Demographics
Age, gender, occupation, or compensation status do not appear to
influence the results of the
nonorganic signs test.8 Hayes et al,21 however, found nonorganic
signs more frequently inpatients with LBP who were anticipating or
receiving financial compensation as compared withthose who were not
anticipating or receiving compensation. In this study, however,
otherfactors differed between the two groups of patients. Thus, the
role of the nonorganic signs isdifficult to assess.
The length of time that a patient has had LBP appears to
increase the likelihood of finding a
positive nonorganic signs test. Waddell et al8 reported that 12%
of patients with LBP who wereseeing an orthopedist for the first
time showed three or more nonorganic signs. The authorsreported
three or more nonorganic signs in 33% of two different samples of
patients withchronic LBP and in 50% of a third sample of patients
with chronic LBP. The three samples ofpatients had all been off
from work for many months with a high incidence of previously
failedtreatments. No positive tests were detected among subjects
without LBP. Factors responsiblefor the increased occurrence of
nonorganic findings in patients with chronic LBP have notbeen
identified. The likelihood of finding three or more nonorganic
signs may increase with theduration of the problem or because of
the failed treatments.
Nonorganic Signs and Tests of Musculoskeletal Performance
Nonorganic contributions to a patient's LBP may coexist with
organic contributions. Organicfindings may be influenced by
nonorganic factors, and in some patients, nonorganic findings
may be influenced by organic factors. Waddell et al22 evaluated
the relationship between thepresence of the nonorganic signs and 27
tests of musculoskeletal impairments in 120 patientswith chronic
LBP. Reproduction of the patient's pain during hip and knee
movements andlimitations in passive knee flexion, hip flexion
force, hip abduction force, and prone isometrictrunk extension were
positive more frequently in the patients who had two or more
nonorganicsigns (29%) than in the patients who had only one or no
nonorganic signs (71%). The onlyimpairments not correlated with a
nonorganic component were those related to spinal postureand lumbar
flexion. Based on these findings, the authors concluded that the
physical tests ofmusculoskeletal impairments that they investigated
were better indicators of illness behaviorthan of physical
impairment.
Groups of patients with LBP with three or more nonorganic signs
performed poorer on tests offorce production, range of motion, and
motor skills than did groups of patients with LBP
without nonorganic signs.23-26 These tests included tests of
lumbar range of motion andisometric force on an Isostation B-200
lumbar dynamometer,23,24 and tests of lifting,
gripping, and physical dexterity on an ERGOS Work Simulator,25
Menard et al26 found thatpatients with LBP with nonorganic signs
produced lower torques for isometric elbow flexionand isometric
knee extension than did patients without nonorganic signs. The
authorscontended that musculoskeletal performance as measured by
dynamometers does notnecessarily reflect maximum physical capacity.
Low values on any of these tests, however,could not be used to
identify individuals with nonorganic problems, because some
individualswith a positive nonorganic signs test scored as well as
some individuals without nonorganicsigns.
Cooke et al24 measured force and range of motion in patients
with chronic LBP, using alumbar dynamometer. The same test was
repeated after 4 weeks of an active reconditioningexercise program.
Patients with a positive nonorganic signs test demonstrated
improvements in
force that were greater than improvements that might be expected
as a result of physiologicchanges or a learning effect of the test
procedure. The authors suggested that the improvedforce generation
might have been due to alterations in illness behavior rather than
to animprovement in physical capacity.
Findings that nonorganic components may contribute to measures
of musculoskeletalimpairments suggest that these measures, which
are frequently used by physical therapists forpatients with LBP,
may also reflect a psychological component of disability. In
addition, thesedata suggest that physical therapists may want to
continue measuring musculoskeletalimpairments but need to consider
the influence of other factors, such as illness behavior, onthese
tests. Likewise, benefits from treatment focused on physical
reconditioning may result inreducing disability by improving an
individual's psychological status, and thus his or hertolerance to
activity, rather than just improvements in the measurement of
musculoskeletalimpairments, such as peak torque of the lumbar
extensors.
-
8/9/2019 Sacrum & Coccyx
23/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
Relationship Between Nonorganic Signs and Treatment Outcomes
Nonorganic phenomena can interact with expected treatment
outcomes in patients with LBP.
Several investigators27-29 have described poorer results from
lumbar surgery in patients with
nonorganic signs. McCulloch27 found that 97 of 109 patients with
a nonorganic componentwho underwent chemonucleolysis continued to
have back or leg pain that prevented theirreturn to full activity.
One hundred eighty-six of 327 patients without nonorganic signs,
incontrast, were free of pain or had minimal limitations in
activity following the chymopapain
injection. Dzioba and Doxey28 found that only 49% of patients
with two or more nonorganicsigns were approved to return to work by
a physician 12 months after various forms of lumbarsurgery, as
compared with 78% of patients who had only one or no nonorganic
signs followingsurgery.
In a prospective study by Waddell et al,29 psychological
factors, including the presence of apositive test for nonorganic
signs, correlated with a poor surgical outcome, as assessed by
aphysician, the patient, and the patient's work status. A poor
surgical outcome in this study wasdefined as postsurgical episodes
of disabling back or leg pain, chronic use of narcoticmedications,
further surgery, or inability to return to work. Relief from pain
and reduceddisability depended on the presence of an accurate
diagnosis of a surgically treatablepathological condition without
the presence of nonorganic signs.
Outcomes of nonsurgical treatments of patients with LBP have
also been influenced by the
presence of nonorganic signs. Lehmann et al30 found that
electroacupuncture treatment of
patients with chronic LBP who had three or more nonorganic signs
was no more effective forpain reduction than a sham treatment. In
contrast, the authors found that treatment of patientswith
electroacupuncture, in the absence of nonorganic signs, resulted in
a greater decrease inpain than did the sham treatments.
Patients with illness behavior as measured by the presence of
nonorganic signs, nonorganicsymptoms, and a pain drawing received
more treatments than did patients who did not exhibit
illness behavior in a study by Waddell et al.31 These treatments
included medication use,lumbar injections, orthopedic supports,
physical therapy, spinal manipulation, and bed rest.Based on this
finding, a clinician should seriously consider whether there is
overutilization oftreatments when patients who test positive for
nonorganic signs show no progress. For thesepatients, treatment
might be directed toward addressing the illness behavior.
Ability of Nonorganic Signs to Predict Return to Work
A common goal in the rehabilitation of workers with LBP is to
return them to work. There isconflicting evidence about the ability
to use nonorganic signs for predicting return to work.
Bradish et al32 reported that a positive nonorganic signs test
at initial assessment in a group ofworkers with a low back injury
(N=120) did not correlate with work status between 12 and 18
months after injury. In contrast, hlund et al17 found a
relationship (r=.34) betweennonorganic signs and the time needed by
a group of automobile workers (N=103) to return towork. In this
study, return to work was defined as the return to the same job at
least half-time.
Lancourt and Kettelhut,33 in a study of 134 patients with LBP,
found that the nonorganic signsof axial loading, simulated
rotation, distraction, and a sensory regional disturbance were
amongthe factors that were better predictors of return to work than
were ankle and knee reflexes,motor loss, and sensory loss in a
dermatomal pattern. This relationship was seen for patientswho
returned to work within the first 6 months after injury but not for
patients who were off
work for greater than 6 months. Recently, Kummel34
described two new nonorganic signs:lumbar pain during isolated
cervical movement and lumbar pain limiting active shouldermovement.
The presence of these two signs in addition to the presence of
three or more ofWaddell's nonorganic signs improved the ability to
predict patients who failed to return to workin this retrospective
study of 717 patients.
The treatment received by injured workers may influence their
return to work. Werneke et al13
evaluated a physical conditioning program designed to meet each
patient's job requirement for170 workers with LBP. One hundred
fifteen of the patients showed work status improvementwithin 3
months of completing the program. At least one nonorganic sign was
present in 47%of the patients whose work status did not improve, as
compared with 12% of the patients whodemonstrated improvement. The
number of nonorganic signs present at discharge from theprogram was
reduced for 82% of the patients whose work status improved. In
contrast to thehigh success rate from physical conditioning, when
patients with nonorganic findings received
-
8/9/2019 Sacrum & Coccyx
24/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
treatments described as "symptomatic and at the discretion of
the physician," less than 40%
returned to work.32
Other factors, besides the presence of nonorganic signs, may
influence an injured worker
returning to previous job duties. Waddell et al29 found return
to work after lumbar surgery waspredicted by physical,
psychological, and occupational factors. Physical therapists
shouldconsider the relationship of these factors in the treatment
of injured workers. The referral to anappropriate professional or
multidisciplinary team should be made for management of
anyconfounding factors when a patient's work tolerance fails to
improve from physical therapy.
Clinical Implications
A physical problem may coexist with the presence of nonorganic
signs. Thus, the presence ofnonorganic signs does not eliminate the
need for a complete physical examination. A patientwith a cauda
equina syndrome, for example, may be classified as exhibiting
nonorganicbehavior based on sensory and motor losses and
overreaction to the examination because ofthe intensity of
symptoms. Physical examination, however, should identify the
structural etiologyof the problem, and appropriate treatment should
be directed toward the pathologicalcondition.
According to Waddell et al,8 nonorganic signs by themselves
should not be equated withmalingering or the presence of a
psychological problem. Rather, the finding of nonorganicsigns
should alert the clinician to the need for more comprehensive
testing. Labeling a patientas a malingerer does little to help the
patient enhance his or her tolerance for activity. Instead,the
factors that are limiting the patient from recovering his or her
tolerance for activity should be
identified, and interventions should be targeted toward
modification of the limiting factors.5
Classification of movement dysfunction in patients with LBP may
help clinicians to identifyindividuals who will benefit from
specific treatments. Failure to account for the presence
ofnonorganic findings may lead to the misclassification of
patients, because nonorganic factors
may influence patients' performance on tests used to classify
them. Delitto et al35 screen fornonorganic signs in their
treatment-based classification scheme and suggest referral to
an
appropriate practitioner when screening is positive. Marras et
al36 developed a classificationscheme for patients with low back
disorders based on the higher derivatives of trunk velocity.Using
this method, Marras et al found that patients with nonorganic
findings weredistinguishable from patients in nine other low back
disorder categories.
The utility of Waddell's nonorganic signs has been described for
patients with LBP. To date,nonorganic signs tests for
musculoskeletal problems in other regions of the body are not
commonly used. Development of nonorganic signs tests for
patients with other musculoskeletalproblems may help to guide
management of these patients.
Nonorganic signs are found more frequently in persons with
chronic LBP as compared withpersons with acute LBP. Further
investigation may reveal how nonorganic behaviors increaseand
develop in patients with chronic LBP. Treatment focused on
prevention of thedevelopment of nonorganic signs may reduce the
occurrence of chronic LBP and back-relateddisability.
Summary
The role of Waddell's nonorganic signs test as a screening tool
for psychological factors in theexamination of patients with low
back problems has been described. The presence ofnonorganic signs
should alert the physical therapist to the need for additional
psychologicaltests and should not necessarily be considered an
indicator of malingering. Nonorganic signsmay coexist with organic
findings. An illness behavior role of the nonorganic signs
issuggested, as they have been related with disability in addition
to physical impairments.Physical therapy management for these
patients should focus on treatment of illness behaviorand on
combating disability.
AcknowledgmentsI thank Louise J White, PT, and Pamela J Woodall,
PT, for their kind assistance with thepreparation of this
update.
References
1 Spitzer WO. Diagnosis of the problem (the problem of
diagnosis): scientific approach to theassessment and management of
activity-related spinal disorders-a monograph for clinicians:report
of the Quebec Task Force on Spinal Disorders. Spine.
1987;12:S16-S21.
-
8/9/2019 Sacrum & Coccyx
25/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
10/6/2007 1
2 Waddell G, Main CJ, Morris EW, et al. Chronic low-back pain,
psychologic distress, andillness behavior. Spine.
1984;9:209-213.
3 Delitto A. Are measures of function and disability important
in low back care? Phys Ther.1994;74:452-462.
4 Bigos S, Bowyer O, Braen G, et al.Acute Low Back Problems in
Adults: Clinical PracticeGuideline No. 14. Rockville, Md: Agency
for Health Care Policy and Research, Public HealthService, US
Department of Health and Human Services; 1994. AHCPR publication
95-0642.
5 Feuerstein M, Beattie P. Biobehavioral factors affecting pain
and disability in low back pain:mechanisms and assessment. Phys
Ther. 1995;75:267-280.
6 Diagnostic and Statistical Manual of Mental Disorders. 4th ed.
Washington, DC: AmericanPsychiatric Association, 1994.
7 McCahill ME. Somatoform and related disorders: delivery of
diagnosis as first step.Am FamPhysician. 1995;52:193-203.
8 Waddell G, McCulloch JA, Kummel E, Venner RM. Nonorganic
physical signs in low-backpain. Spine. 1980;5:117-125.
9 Waddell G, Richardson J. Observation of overt pain behaviour
by physicians during routineclinical examination of patients with
low back pain. J Psychosom Res. 1992;36:77-87.
10 Collie J. Malingering and Feigned Sickness. London, England:
Edward Arnold (Publishers)Ltd; 1913.
11 Hoover CF. A new sign for the detection of malingering and
functional paresis of the lowerextremities. JAMA.
1908;51:746-747.
12 Greenough CG, Fraser RD. Comparison of eight psychometric
instruments in unselectedpatients with back pain. Spine.
1991;16:1068-1074.
13 Werneke MW, Harris DE, Lichter RL. Clinical effectiveness of
behavioral signs for screeningchronic low-back pain patients in a
work-oriented physical rehabilitation program.
Spine.1993;18:2412-2418.
14 McCombe PF, Fairbank JCT, Cockersole BC, Pynsent PB.
Reproducibility of physical signsin low-back pain. Spine.
1989;14:908-918.
15 Solomon PE. Measurement of pain behaviour. Physiotherapy
Canada. 1996;48:52-58.
16 Keefe FJ, Block AR. Development of an observation method for
assessing pain behavior inchronic low back pain patients. Behav
Ther. 1982;13:363-375.
17hlund C, Lindstrm I, Areskoug B, et al. Pain behavior in
industrial subacute low backpain, part I: reliability-concurrent
and predictive validity of pain behavior assessments.
Pain.1994;58:201-209.
18 Waddell G, Pilowsky I, Bond MR. Clinical assessment and
interpretation of abnormal illnessbehaviour in low back pain. Pain.
1989;39:41-53.
19 Main CJ, Wood PLR, Hollis S, et al. The Distress and Risk
Assessment Method: a simplepatient classification to identify
distress and evaluate the risk of poor outcome. Spine.
1992;17:42-52.
20 Chan CW, Goldman S, Ilstrup DM, et al. The pain drawing and
Waddell's nonorganicphysical signs in chronic low-back pain. Spine.
1993;18:1717-1722.
21 Hayes B, Solyom CAE, Wing PC, Berkowitz J. Use of
psychometric measures andnonorganic signs testing in detecting
nomogenic disorders in low back pain patients.
Spine.1993;18:1254-1262.
22 Waddell G, Somerville D, Henderson I, Newton M. Objective
clinical evaluation of physicalimpairment in chronic low back pain.
Spine. 1992;17:617-628.
23 Hirsch G, Beach G, Cooke C, et al. Relationship between
performance on lumbardynamometry and Waddell score in a population
with low-back pain. Spine.
-
8/9/2019 Sacrum & Coccyx
26/26
dells Nonorganic Signs
http://orthoteers.com/(S(l4gom345o1tssvrsb0qg1c55))/printPage.a
1991;16:1039-1043.
24 Cooke C, Menard MR, Beach GN, et al. Serial lumbar
dynamometry in low back pain.Spine. 1992;17:653-662.
25 Cooke C, Dusik LA, Menard MR, et al. Relationship of
performance on the ERGOS worksimulator to illness behavior in a
workers' compensation population with low back versus limbinjury. J
Occup Med. 1994;36:757-762.
26 Menard MR, Cooke C, Locke SR, et al. Pattern of performance
in workers with low backpain during a comprehensive motor
performance evaluation. Spine. 1994;19:1359-1366.
27 McCulloch JA. Chemonucleolysis. J Bone Joint Surg [Br].
1977;59:45-52.
28 Dzioba RB, Doxey NC. A prospective investigation into the
orthopaedic and psychologicpredictors of outcome of first lumbar
surgery following industrial injury. Spine. 1984;9:614-623.
29 Waddell G, Morris EW, Di Paola MP, et al. A concept of
illness tested as an improved basisfor surgical decisions in
low-back disorders. Spine. 1986;11:712-719.
30 Lehmann TR, Russell DW, Spratt KF. The impact of patients
with nonorganic physicalfindings on a controlled trial of
transcutaneous electrical nerve stimulation andelectroacupuncture.
Spine. 1983;8:625-634.
31 Waddell G, Birchner M, Finlayson D, Main CJ. Symptoms and
signs: physical disease orillness behaviour? BMJ.
1984;289:739-741.
32 Bradish CF, Lloyd GJ, Aldam CH, et al. Do nonorganic signs
help to predict the return toactivity of patients with low-back
pain? Spine. 1988;13:557-560.
33 Lancourt J, Kettelhut M. Predicting return to work for lower
back pain patients receivingworker's compensation. Spine.
1992;17:629-640.
34 Kummel BM. Nonorganic signs of significance in low back pain.
Spine.1996;21:1077-1081.
35 Delitto A, Erhard RE, Boling RW. A treatment-based
classification approach to low backsyndrome: identifying and
staging patients for conservative treatment. Phys
Ther.1995;75:470-489.
36 Marras WS, Parnianpour M, Ferguson SA, et al. The
classification of anatomic- and
symptom-based low back disorders using motion measure models.
Spine.1995;20:2531-2546.
[ Close Window ]