Embed Size (px)
Citation preview

Running the Ironman
Brad LewisSFGH
Blood alone moves the wheels of history.Benito Mussolini
Blood will tell, but often it tells too much.Don Marquis

AnemiaAn Approach to Anemia
?

AnemiaAn Approach to Anemia
SmearLDH
BilirubinIron Studies
B12Coombs
?

Evaluating HemolysisThe Bucket with The Hole

Evaluating HemolysisThe Bucket with The Hole
Retic
Hemoglobin Level
Loss or Hemolysis

Reticulocytes
Retic #=1/mmRetic %= 20%
Retic # = 1/mmRetic % = 30%
Corr Retic = Retic x hgb/nl hgb
RPI = corrected retic. count/Maturation time (Maturation time = 1 for Hct=45%, 1.5 for 35%, 2 for 25%, and
2.5 for 15%.)

Retic Hi Retic Low
AnemiaAn Approach to Anemia

Retic Hi Retic Low
Anemia
MCV HiMCV NlMCV Lo
An Approach to Anemia

Retic Hi Retic Low
Anemia
Destruction Loss MCV HiMCV NlMCV Lo
IntrinsicExtrinsicSplenicMechanicalRecovery
TissueOn FloorOccult
Iron(Lead)ThalFrags
B12FolateLiverETOHThyroidToxicMDS
Chronic DiseaseRenalMixedMild/TreatedEarlyTransfusedEndocrineIntrinsic BMDilution
An Approach to Anemia

Retic Hi Retic Low
Anemia
Destruction Loss MCV HiMCV NlMCV Lo
Iron(Lead)ThalassemiaFragmentationSideroblastic Anemia
acquiredcongenital

Diagnostic TestsLow Retic Microcytic
Iron/TIBC vs. FerritinHemoglobin Electropheresis
• GENETIC SCREENING OF FAMILY• The “Normal” Electropheresis
Smear?Value of MCV and RDWLead?

23 yo Chinese Woman 13 wks Pregnant Hgb 11, MCV 72
• What Tests?

23 yo Chinese Woman 13 wks Pregnant Hgb 11, MCV 72
• What Tests?• Iron Studies first
• may mask beta-Thal by decreasing Hgb A2
• What if Hemoglobin Electropheresis is normal?• If iron nl, then not beta-thal• BUT alpha-thal carrier state has normal HPLC

Diagnostic TestsLow Retic Microcytic
• Iron/TIBC vs. Ferritin• Hemoglobin Electropheresis
• GENETIC SCREENING OF FAMILY• The “Normal” Electropheresis
• Smear?• Value of MCV and RDW• Lead?

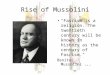
Andrews NC. N Engl J Med. 1999;341:1986–1995.
Body Iron Distribution and Storage
Dietary iron
Utilization UtilizationDuodenum
(average, 1-2 mgper day)
Muscle(myoglobin;
300 mg)
Liver(1000 mg)
Bone marrow(300 mg)Circulating
erythrocytes(hemoglobin;
1800 mg)
Reticuloendothelialmacrophages
(600 mg)
Sloughed mucosal cellsDesquamation/menstruation
Other blood loss(average, 1-2 mg per day)
Storageiron
Plasma
Iron loss
transferrin(3 mg)

Iron Metabolism
PlasmaFe-Tf
RBC
Bone MarrowDuodenum
Spleen
Tomas Ganz ASH 2006
Liver

Iron Metabolism
PlasmaFe-Tf
RBC
Bone MarrowDuodenum
Spleen
Tomas Ganz ASH 2006
20 mg/d

Iron Metabolism
PlasmaFe-Tf
RBC
Bone MarrowDuodenum
Spleen
Tomas Ganz ASH 2006

Hepcidin
• Small molecule which blocks iron movement
• Evolutionary conservation• Problems with assays
• Regulation• Increased by dietary iron <1day• Congenital absence>>juvenile hemochromatosis• Decreased by anemia, hypoxia

Hepcidin Regulation
Hepcidin
Adequate Iron Intake
InflammationIL-6
RBC turnover
Hypoxia
Hemochromatosis
Increased
Decreased
Anemia?

Hepcidin and Inflammation
• Suppressed in hours by IL-6 (?others)• Not in IL-6 deficient mice
• Plasma Iron turnover q3hrs• 30% drop in 1 hour if recycling blocked• “Anemia of Acute Disease”
• ??Role in host defense
Bone Marrow
Tomas Ganz ASH 2006
PlasmaFe-Tf
3 mg
RBC
Spleen 20 mg/d

Infectious Risk of Iron Overload
• Bacterial• Hepcidin, lactoferrin, transferrin bacteriostatic in
vitro• Listeria, Yersenia, Aeromonus• Cunninghamella bertholletiae
• Fungal• Increased growth in vitro• Case reports of increased Mucor in MDS pts
• ? Increased risk with chelation with streptomyces pilosis

Hepcidin and Iron Transport
Fpn
Fpn
Low Hepcidin High HepcidinIron Iron
ferritinferritin
Hepcidin
Iron release into Plasma
lysosome
EnterocytesMacrophages
DMT1

Iron Metabolism
PlasmaFe-Tf
HepcidinHepcidin
Hepcidin
Iron Signal
Erythropoiesis Signal
RBC
Bone MarrowDuodenum
Spleen
Tomas Ganz ASH 2006
Hep
cidin

Iron Metabolism
PlasmaFe-Tf
HepcidinHepcidin
Hepcidin
Iron Signal
Erythropoiesis Signal
RBC
Bone MarrowDuodenum
Spleen
Tomas Ganz ASH 2006
Hep
cidin

Evaluating IronStores vs. Response
Ferritin• Sensitive/specific
• Except increased in inflammation, liver disease, malignancy
Fe/TIBC (Transferrin) and Saturation• Decreased in inflammation, malignancy
THEREFORE:• Iron Trial• Serum (soluble) Transferrin Receptor
• Mediates iron transfer into cell• Increased in Fe-def, rapid cell production
• CHR-Retic Hemoglobin Concentration?Follow-up GI Eval
• 10 -15% with malignancy• ?Only if ferritin <100?

Colon CA in Iron Deficiency
Am J Gastroenterol. 2007;102(1):82-88.

Evaluating Iron in Inflammation
Bone Marrow Iron Stores?? Saturation (Fe/Transferrin) <8-10% Iron Trial
?IV repletion, check 1 month % Hypochromic RBC’s
Nl. <2.5%, Fe-deficient >10% correlates with Fe response Reticulocyte Hgb Concentration?
Sensitive, specific for diagnosis in dialysis pts Responds to iron in 48 hours
Serum (soluble) Transferrin Receptor Increased in Fe deficiency or increased RBC turnover

Treatment of Iron Deficiency
Oral always preferred• ?low dose equally effective (325 mg FeSO4)• ?role for Vitamin C
When to use IV iron• Recent decreased risk of anaphylaxis• Poor compliance
• Side-effects, etc
• Poor Absorption• Jejeunal/duodenal disease• Sprue• “Chronic Disease”• Anemia of Malignancy

Iron Overload
NTBI circulates in the plasma
LiverLiver
Insoluble iron complexes are
deposited in body tissues
PancreasPancreas EndocrineEndocrine
Serum transferrin iron binding capacity exceeded
Iron overload
CardiacCardiac ReproductiveReproductive
NTBI = non-transferrin bound ironAdapted from: Olivieri NF, et al. Blood. 1997;89:739-761; Olivieri NF. N Engl J Med. 1999;341:99-109.
Excess iron promotes free radical formation

Basic Causes of Iron Overload
• Acquired iron overload1
• Transfusional • Ineffective erythropoiesis• Toxic ingestion (very rare in adults)
• Hereditary• HFE hemochromatosis
• Homozygous C282Y mutation in HFE gene2
• Defective regulatory receptor in intestine results in increased absorption of iron
• Other genetic mutations
1. Porter JB. Br J Haematol. 2001;115:239–252.2. Feder JN, et al. Nat Genet. 1996;13:399–408.

Diseases With High Risk of Iron Overload
• Diseases requiring frequent or repeatedtransfusions• -Thalassemia (major and intermedia)• Sickle cell anemia• Myelodysplastic syndromes (MDS)• Aplastic anemia• Rare chronic anemias
• Blackfan-Diamond anemia (red cell aplasia)• Fanconi anemia (hypoplastic anemia)• Others

Iron Loading From Blood Transfusions
• 1 unit of blood contains 200 mg of iron1
• Chronic transfusion-dependent patients have an iron excess of ~0.4 to 0.5 mg/kg/day2
• There is no physiologic mechanism to remove excess iron
• Therefore, iron accumulates with repeated blood transfusions
• Signs of iron overload can be seen anywhere between 10 and 20 transfusions1
• Iron overload can result in iron-related dysfunction of key organs1,2
1. Porter JB. Br J Haematol. 2001;115:239–252.2. Kushner JP, et al. Hematology. 2001;47–61.

Iron Metabolism
PlasmaFe-Tf
HepcidinHepcidin
Hepcidin
Iron Signal
Erythropoiesis Signal
RBC
Bone MarrowDuodenum
Spleen
Tomas Ganz ASH 2006

Hereditary Hemochromatosis
• Autosomal recessive• HFE gene in 90% (hepcidin deficiency)
• Rare Transferrin Receptor 2 defect• Variable penetrance, caucasions only
• Severe Disease• Hemojuvelin• HAMP (hepcidin)
• Autosomal dominant• Rare, ferroportin defect• Severe, early onset, Hepatocytes only
• Other rare defects• DMT1(microcytosis), atransferrenemia, ceruloplasmin

Hemochromatosis Diagnosis
• Consider in :
• Chronic fatigue• Arthropathy• Impotence• Hyperpigmentation• Cirrhosis• DM• Cardiomyopathy• Screening elevated Fe sat or Ferritin

Hemochromatosis Diagnosis
• Fe/TIBC >60%• Decreased in early, family-hx diagnosis• Decreased with inflammation
• HFE testing (C282Y)• Compound hetero C282Y/H63D
• Rarely a problem, unless ETOH
• Ferritin to quantify iron overload• IF confusing, consider MRI

Hemochromatosis Management
• Ferritin >1000 associated with sx• Fe/TIBC saturation >75%
• Unstable/labile iron with increased risk of oxidant damage• Urgent phlebotomy
• IF sx or end organ damage• Weekly to <1000 ferritin as tolerated• Target ferritin <50
• ? Role of deferasirox (Exjade)• Rarely in hemochromatosis• intolerance