Embed Size (px)
Citation preview

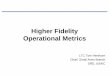
SFGH Inpatient Dashboard: Key Operational and Quality Metrics
Improving Health
Outcomes
Optimizing Efficiency and
Access
Improving the Patient
Experience
For more detail on Harm results, see Patient Safety Dashboard (pg 3). For more detail on Core Measures, see Core Measures
dashboard (pg. 2)
67 69 77 74
81
Dec-13 Jan-14 Feb-14 Mar-14
Communication w/ Drs
SFGH NRC Avg
57 66 71 69
79
Dec-13 Jan-14 Feb-14 Mar-14
Communication w/ RNs
SFGH NRC Avg
53 58 64 65
71
Dec-13 Jan-14 Feb-14 Mar-14
Overall Rating of SFGH
SFGH NRC Avg
56
68 60
65
72
Dec-13 Jan-14 Feb-14 Mar-14
Pain Management
SFGH NRC Avg
0.90 0.82
1.18
0.76 0.84
Dec-13 Jan-14 Feb-14 Mar-14
Mortality O/E
SFGH NAPH Median
5.56
5.81 5.70
5.31
5.69
Dec-13 Jan-14 Feb-14 Mar-14
Avg LOS
SFGH NAPH Median
11% 13% 12%
9%
Dec-13 Jan-14 Feb-14
30 day Readmissions %
SFGH NAPH Median
474 435
474 495
338
2013-1 2013-2 2013-3 2013-4
ED arrival to Admit time (mins)
SFGH UHC Median
288 280 256 239
180
2013-1 2013-2 2013-3 2013-4
ED arrival to discharge time (mins)
SFGH UHC Median
93% 97%
80%
100%
AMI SCIP PN HF
Core measure composites Q4 2013
SFGH UHC Median
20
10
17
23
Oct-13 Nov-13 Dec-13 Jan-14
Instances of Harm
12.6% 10.6% 10.6% 9.1%
76% 70% 66%
50%
2013-2 2013-3 2013-4 2014-1
% Days at Lower Level of Care
MedSurg Psych
Brought to you by the Quality Data Center: Informing, engaging, and transforming practice through clinical and operational data.

SFGH Inpatient Dashboard: Key Operational and Quality Metrics
NOTES/DEFINITIONS
Operational and Quality metrics were selected based on SFGH strategic goals and external measurement by agencies like
CMS, Joint Commission, and America's Essential Hospitals (formerly NAPH). Metrics are organized around CMS's triple aim to
improve health outcomes, optimize efficiency and access, and improve patient experience.
UHC Median: Comparisons are based on the median score of all hospitals in the University Healthsystem Consortium (UHC);
they are not specific to service.
NAPH Median: National Association of Public Hospitals (now America's Essential Hospitals) median is used when available for
comparison to similar public hospitals.
Core Measure Composites: Each composite represents the total measure compliance for all eligible cases. Core Measures
are calculated by our Joint Commission vendor, the University Healthcare Consortium (UHC) and assesses inpatient clinical
performance with Acute Myocardial Infarction (AMI), Heart Failure (HF), Surgical Care (SCIP), and Pneumonia (PN). Core
measure results affect up to 2% of SFGH's Medicare fee-for service annual reimbursements, as part of the CMS Value Based
Purchasing program.
30 day Readmission Rate: The all-cause readmission rate is the proportion of patients who return to the hospital within 30
days of discharge from the prior (index) admission for all causes. Chemotherapy, radiation therapy, dialysis, rehabilitation
and delivery/birth are excluded from the numerator, and alcohol abuse and mental health cases are included in the
numerator and denominator. Bad data and deaths at first admission are excluded from the numerator and denominator.
The calculation formula is: Readmission Rate = number of readmissions/number of index admissions. This rate is taken from
UHC’s Readmissions report.
Mortality O/E: The mortality O/E ratio are taken from UHC’s Patient Outcomes Report, which looks at the same population
described in “Total Cases” above. The Mortality O/E is observed mortality rate divided by the UHC expected mortality rate.
A Mortality O/E of greater than 1 indicates that more patients died than expected. A Mortality O/E of less than 1 indicates
that fewer patients died than expected.
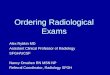
Instance of Harm: A monthly count of all instances of avoidable harm that happened at SFGH in one of the following
categories: falls wtih injuries, central line- associated bloodstream infections, C-difficile, potentially preventable sentinel
events, catheter-associated UTIs, possible ventilator-associated pneumonias, surgical site infections, hospital acquired
pressure ulcers, and medication errors.
Avg LOS: Average length of stay for all patients discharged that month.
ED arrival to Admit: The average time from patient arrival to the Emegency Department to the time of their admission, in
minutes, for all patients admitted through the ED that quarter.
ED arrival to discharge: The average time from patient arrival to the ED to the time of patient discharge, in minutes, for all
patients discharged from the ED that quarter.
% Days at Lower Level of Care: the percent of patient days at lower level of care (LLOC) days include administrative (skilled
nursing) and denied (custodial) days, out of total patient days in medsurg and psych each quarter.
Patient Experience measures: The Hospital Consumer Assessment of Health Providers and Systems (HCAHPS) is a national
survey administered to SFGH’s inpatients via mail following their stay at the hospital. Results shown are the percentage of
patients that scored the HCAHPS questions with a "top box" answer, i.e., "Always", "Would Definitely Recommend". These
top box scores are tracked by CMS as a measure of patient experience at our hospital. Responses to questions on the same
subject are rolled up into composite measures, which affect our annual Medicare reimbursement rate.
Brought to you by the Quality Data Center: Informing, engaging, and transforming practice through clinical and operational data.

Core Measures Performance Dashboard: Q4 2013 2013-4 2013-3
INPATIENT MEASURES UHC Median
HEART ATTACK (AMI) n rate Q3 2013 rate n rate n rate n rate n rate n rate n rate n rate n
Aspirin at arrival 39 97% 100% 97% 65 100% 4 100% 7
Aspirin at discharge 36 97% 100% 97% 51 100% 4 100% 7
ACEI/ARB for LVSD 12 100% 100% 100% 13 100% 1 100% 3
Beta Blocker at Discharge 37 95% 100% 97% 48 100% 4 75% 8
PCI within 90 minutes of arrival (VBP) 6 100% 100% 100% 14
Statin Prescribed at Discharge 35 97% 100% 97% 50 100% 4 100% 7
HEART FAILURE
Discharge Instructions include 6 elements (VBP)* 61 100% 100% 100% 81 100% 29 100% 18
Evaluation of LVS Function 63 100% 100% 100% 82 100% 29 100% 20
ACEI or ARB for LVSD 33 100% 100% 100% 47 100% 12 100% 7
PNEUMONIA
Blood Cx within 24 hrs (ICU pts) 9 100% 100% 100% 2 100% 4 100% 8 100%
Appropriate antibiotic selection (VBP) 17 100% 100% 100% 4 100% 6 100% 22
Blood Cultures taken in ED prior to Antibiotics on Admit (VBP) 31 77% 100% 67% 5 88% 18 74% 39 100%
Initial Abx CAP Selection in Immunocompetent - ICU 3 100% 100% 100% 2 1 100% 3
Initial Abx CAP Selection in Immunocompetent: Non-ICU 14 100% 100% 100% 2 100% 5 100% 19
SURGICAL CARE IMPROVEMENT
Prophylactic antibiotic within one hour of incision (VBP) 57 98% 100% 100% 1 100% 26 100% 5 100% 46 93% 26
Antibiotic selection (VBP) 57 100% 100% 1 100% 26 100% 5 100% 46 100% 26
Prophylactic antibiotic discontinued within 24 hours (VBP) 57 100% 100% 1 100% 26 100% 5 100% 46 100% 26
Appropriate hair removal 78 100% 100% 100% 1 100% 29 100% 6 100% 4 100% 52 100% 5 100% 54
Urinary catheter removed on POD 1 or 2 (VBP) 47 100% 99% 1 100% 5 100% 50 100% 28
Pts on beta blockers rcvd beta blocker during periop period 15 100% 100% 1 100% 6 100% 2 100% 10 1 100% 8
Surgery Pts with periop temperature management 77 100% 100% 1 100% 29 100% 6 100% 5 100% 51 100% 4 100% 52
Pts rcvd VTE Prophylaxis w/in 24 hrs post surgery 64 98% 100% 1 100% 21 100% 4 100% 4 96% 48 100% 4 100% 42
SOURCE= University Healthsystem Consortium (UHC)
Brought to you by the Quality Data Center: Informing, engaging, and transforming practice through clinical and operational data.
ORT URO TRASFGH CAR FPR GYN MED NSU

Hospital-Wide Patient Safety DashboardAim: Reduce preventable harm to zero
2
4
1
4 5
3
5 4 4
5 6
5
012345678910
# o
f ev
ents
Catheter-Associated UTIs
10
6
4 5
6 5 5 5 5
4
2
8
012345678910
# o
f ev
en
ts
C-DIFF
9
2 1
6
4 3
5 4 4
2 2 1
012345678910
# o
f e
ven
ts
Falls with Injuries
0 1 1
0 1 1
0 1
0 0 0
2
012345678910
# o
f e
ven
ts
Possible Ventilator- Associated Pneumonias
0 1
0 1 1
0 0 0 0 1
0 1
012345678910
# o
f ev
ents
Central Line-Associated Blood Stream Infections
2 3
1 0
3
1
3
5
7 7
3 2
012345678910
# o
f ev
en
ts
Hospital-Acquired Pressure Ulcers
2
4 3
1
5
1
8
4
10
3
0
1
2
3
4
5
6
7
8
9
10
# o
f e
ven
ts
Surgical Site Infections
0 0 0 0 0 0 0 0 0 0 0 0 0 012345678910
# o
f ev
en
ts
Med Errors
Coming Soon!
0 0 0 0 1
3
1 1 1 1 1 1 012345678910
# o
f ev
ents
Potentially Preventable Sentinel Events
Total Cases of Harm over the Past 12 Months
256 23 17
10
20 24
17
24 21
29 24 24 23 23
05101520253035404550
# o
f e
ven
ts
Harm by Month
Brought to you by the Quality Data Center: Informing, engaging, and transforming practice through clinical and operational data.
For Questions, please contact the Quality Data Center 415-206-4161