Embed Size (px)
Citation preview

CIMT 1
Running head: CONSTRAINT INDUCED MOVEMENT THERAPY
The Effects of Constraint-Induced Movement Therapy and Modified Constraint-Induced
Movement Therapy on Quality of Life among Persons with Chronic Hemiparesis
Ashley Morrow, Elizabeth Ballor, Jill Killingbeck, and Megan Haskin
Saginaw Valley State University
CIMT 2
Abstract
Purpose: This study examined the effects of constraint-induced movement therapy (CIMT) and
modified constraint-induced movement therapy (mCIMT) on quality of life among persons
demonstrating learned nonuse of an affected upper extremity status post CVA.
Method: A mixed methods approach, consisting of both qualitative and quantitative
methodology, was used to examine the impact of CIMT and mCIMT on quality of life for
persons demonstrating upper extremity learned nonuse following a CVA.
Results: The Stroke Impact Scale showed improvement in all areas of quality of life in both
CIMT and mCIMT groups. However, the CIMT group showed greater gains than the mCIMT
group over the assessment areas.
Conclusion: The data collected suggested that both CIMT and mCIMT can produce increased
overall gains in quality of life among persons demonstrating learned nonuse of an affected upper
extremity status post CVA.
CIMT 3
The Effects of Constraint-Induced Movement Therapy and Modified Constraint-Induced
Movement Therapy on Quality of Life Among Persons with Chronic Hemiparesis
Cerebral vascular accidents (CVAs), otherwise known as strokes, account for nearly
780,000 deaths annually in the United States. A CVA occurs as a result of the blood and oxygen
supply to the brain becoming disrupted, causing an insufficient amount of nutrients to reach the
brain. CVAs are the third most common cause of death, and impact the lives of Americans every
40 seconds in the United States. CVAs are also the leading cause of long-term disability among
Americans (“Stroke Statistics,” 2008).
Hemiparesis, or weakness on one side of the body, is one deficit that may be experienced
by individuals who have sustained CVAs. Learned non-use is a common condition that often
arises when hemiparesis is present, as an individual begins to rely on his or her unaffected side to
compensate for weakness to the contralateral side. Learned non-use or inactivity of the affected
side may further contribute to disability and hinder occupational performance in areas of daily
life activities and experienced quality of life (Wu et al., 2007).
Quality of life has been identified as a problem for many people post-stroke. As
discussed by King (1996), there is a need to assist stroke survivors in coping with the effects of
stroke. In a study examining quality of life, 30 percent of the 86 participants were measured to be
within a depressed range. Within the four domains examined, the quality of life of stroke
survivors was measured as lowest in health and functioning. Objectives such as participation in
leisure recreations, usefulness to others, and general mobility were some of the areas most
affected by stoke observed in this study (King, 1996).
Constraint-induced movement therapy (CIMT) is a promising approach for the treatment
of hemiparesis and learned non-use following a CVA. CIMT involves forcing the use of the
CIMT 4
affected limb in order to improve function of a partially paralyzed upper extremity in clients who
have experienced a stroke. The unaffected limb is immobilized by a constraint as a part of an
intense treatment protocol that involves therapy for six hours a day for two weeks, as well as in a
home program, with a goal of forcing movement of the affected extremity (Caimmi et al., 2008).
A modified version of this protocol, called modified constraint-induced movement therapy
(mCIMT), involves constraint of the unaffected extremity for three hours per day, five days per
week, for a total of four weeks. A home program is also included with this protocol (Earley,
2008).
Research Problem
Limited research has been completed to examine the effects of CIMT/mCIMT on quality
of life post-stoke. For example, Dettmers and colleagues found in a study of 11 participants, that
some aspects including quality of life were improved after completing a modified CIMT
program (Dettmers et al., 2005). However, there is an overall lack of literature discussing the
effectiveness of CIMT/mCIMT on the improvement of quality of life. Yet it appears that, due to
its reputation as having a positive impact on individuals with chronic hemiparesis and learned
non-use, CIMT and mCIMT may have a positive effect on the quality of life for those who are
post stroke (Jamison & Orchaniam, 2007).
Purpose of the Study
The purpose of this two-phase, sequential, mixed methods research study was to examine
the effects of constraint-induced movement therapy (CIMT) and modified constraint-induced
movement therapy (mCIMT). This study focused on the effects of the programs on the quality of
life of persons who had sustained a stroke and who demonstrated learned nonuse of the affected
upper extremity.
CIMT 5
Research Questions and Hypotheses
The first two research questions were answered through the use of quantitative data
collected through the Stroke Impact Scale.
1) Does participation in mCIMT improve the quality of life for clients who have
experienced chronic hemiparesis status post CVA?
Null hypothesis: There is no significant difference in the pre- to post-intervention Stroke Impact
Scale Version 3.0 scores among participants involved in a mCIMT program.
HO: µ1 = µ2, where
µ1 = Stroke Impact Scale Version 3.0 pretest scores
µ2 = Stroke Impact Scale Version 3.0 posttest scores
Alternative Hypothesis: There is a significant difference in the pre- to post-intervention Stroke
Impact Scale Version 3.0 scores among participants involved in a mCIMT program.
HA: µ1 ≠ µ2
2) Does participation in CIMT improve the quality of life for clients who have experienced
chronic hemiparesis status post CVA?
Null hypothesis: There is no significant difference in the pre- to post-intervention Stroke Impact
Scale Version 3.0 scores among participants involved in a CIMT program.
HO: µ1 = µ2, where
µ1 = Stroke Impact Scale Version 3.0 pretest scores
µ2 = Stroke Impact Scale Version 3.0 posttest scores
Alternative Hypothesis: There is a significant difference in the pre- to post-intervention Stroke
Impact Scale Version 3.0 scores among participants involved in a CIMT program.
HA: µ1 ≠ µ2

CIMT 6
The final two research questions were answered through the use of qualitative data
collected through post treatment focus groups.
3) Does participation in mCIMT/CIMT improve the occupational performance of clients
who have experienced chronic hemiparesis status post CVA?
4) Does participation in mCIMT/CIMT improve the client’s perceived quality of life status
post CVA?
Definition of Terms
Brain plasticity. Brain plasticity is the capability of the brain to compensate for loss of
function due to a possible disruption of neuronal organization or damage to the brain (Kolb &
Whishaw, 2003).
Cerebral vascular accident. A cerebral vascular accident, or stroke, is a disorder of the
blood vessels within the brain that is the result of an interrupted blood flow. Disruptions of the
blood and nutrient supply to the brain will cause subsequent neuronal death to the brain vessels,
and cause neurological symptoms (Eckert, 2007).
Constraint induced movement therapy. Constraint Induced Movement Therapy (CIMT) is
a treatment program that is implemented by forcing the use of the affected limb in order to
improve function of a partially paralyzed upper extremity among clients who have experienced a
stroke (Caimmi et al., 2008).
Hemiparesis. Hemiparesis is weakness or partial paralysis affecting one side of the body.
It is frequently caused by a cerebral vascular accident, or brain lesion. Paresis typically occurs on
the side of the body opposite to the lesion, due to the decussating or crossing of the motor tracts
of the brain (Eckert, 2007).
CIMT 7
Learned non-use. Learned non-use is a condition that often results from the consequences
of a stroke. This condition leads to the discontinuation of the client’s use of his/her affected
extremity for daily life tasks due to sustained cortical disorganization. Permanent disability or
dependency may result after continued disuse of an affected extremity, which can decrease
occupational performance (Wu et al., 2007).
Modified constraint-induced movement therapy. Modified constraint induced movement
therapy (mCIMT) is a treatment protocol in which the duration and amount of therapy or the
constraint regimen differs from original CIMT program (Hakkennes & Keating, 2005).
Treatment is implemented by forcing the use of the affected limb in order to improve function of
a partially paralyzed upper extremity among clients who have experienced a stroke (Caimmi et
al., 2008).
Occupational performance. Occupational performance is the act of being able to
complete or participate in activities that are necessary for an individual to survive. These include
any activity that an individual completes on a daily basis. Occupational performance allows the
individual to learn and adapt to the environment and activities (Hansen, Dirette, & Atchison,
2007).
Quality of life. Quality of life is an individual’s global feelings of well-being and
satisfaction within the cultural context and value system within which one resides (Campos &
Johnson, 1990). For the purposes of this study, quality of life will be measured using the Stroke
Impact Scale. This scale assesses how a stroke has affected an individual’s health and daily
living.
CIMT 8
Significance of the Study
The study explored whether mCIMT/CIMT had an effect on the quality of life and
occupational performance of clients who were post stroke. The results of this study showed that
the use of the mCIMT/CIMT program improved the participant’s occupational functioning and
quality of life after sustaining a stroke. The data obtained from this study also contributed to the
body of knowledge concerning mCIMT/CIMT, and also supports the existing studies that
suggest the use of mCIMT/CIMT for rehabilitation in clinical settings to address deficits in
quality of performance in occupations and quality of life post stroke.
Review of the Literature
Recently, there has been an increased amount of well-designed research studies that have
investigated the therapeutic benefits of mCIMT/CIMT on physical functioning post-CVA.
However, quality of life among stroke survivors who have received mCIMT/CIMT has yet to be
thoroughly examined. This review will provide an overview of the existing literature related to
mCIMT/CIMT and quality of life of individuals post stroke. First, the literature review will
discuss hemiparesis and its impact on learned non-use on the affected extremity. Second, the
review will address the origins of CIMT in early CVA rehabilitation, and the gains achieved
through the use this approach to treatment. Finally, neuroplasticity will be discussed and the
implications of cortical reorganization on improved brain recovery in chronic stroke patients.
Constraint Induced Movement Therapy (CIMT)
Constraint-induced movement therapy and modified constraint-induced movement
therapy are rehabilitative treatment techniques that are used to improve the quality of function of
an affected limb experiencing hemiparesis. Strokes may result in hemiparesis, which causes
weakness on one side of the body. Strokes are an increasingly common health problem in the
CIMT 9
United States, with four million Americans struggling daily with the effects of a stroke. Strokes
are the leading cause of sensorimotor disability in the United States (“Stroke Statistics,” 2008).
However, upper extremity (UE) function, which can be negatively affected by a stroke, is
needed to complete activities of daily living, improve independence, and maintain a high quality
of life (Hakkennes & Keating, 2005).
Learned nonuse
CIMT and mCIMT are therapeutic interventions that aim to restore upper extremity
functioning that has been lost secondary to learned nonuse (Wolf et al., 2006). Learned nonuse
is a phenomenon in which stroke survivors stop using their affected extremities, despite the
presence of intact motor ability in the affected extremity. Early research conducted by Taub in
the Silver Springs Monkey Experiment provided the first information regarding this
phenomenon. During the Silver Springs experiment, sensation in one of the monkeys’ arms was
taken away, but the motor ability was left intact (a process known as deafferentiation). Taub
observed that, not long after sensation was taken away from the arm, the monkeys stopped using
their affected arms, even though motor ability was present. The monkeys relied solely on their
non-affected arm to perform within their environment. However, when Taub applied a
constraint to the non-affected arm of the monkeys, and forced them to use their affected arms,
functional use of the affected arm was gradually restored (Taub et al., 1999).
The information learned from the Silver Springs experiment was later applied to research
with humans who had sustained strokes and subsequently demonstrated learned nonuse. CIMT
was first used on patients who were status post CVA by Taub in 1980. Taub’s treatment
protocol required clients to have their unaffected limb restrained for 90% of their waking hours
for two weeks, and participate in exercise training for six hours a day (Hakkennes & Keating,
CIMT 10
2005). Taub found that individuals with weakness of one side of the body (hemiparesis) could
benefit from CIMT (Taub et. al., 1999).
Therapeutic protocols
Taub’s therapy has since evolved since the early research with monkeys, and today there
are two main types of CIMT used in the rehabilitation of persons with upper extremity
hemiparesis status post CVA. Both CIMT and mCIMT involve constraining the unaffected limb,
in efforts to force the affected arm to regain movement through participation functional
movement. The CIMT constraint is worn for six hours a day, for five days a week, for a total of
two complete weeks. The mCIMT protocol involves wearing a constraint on the unaffected
extremity for three hours a day, five days a week for four total weeks of constraint wear (Taub et.
al., 1999).
CIMT/mCIMT techniques include restricting the unaffected limb for a sustained period
of time and encouraging client participation in exercises that are task-specific, to retrain the
affected limb to do functional daily activities. CIMT/mCIMT therapy exercises consist of
participation in activities requiring functional movement patterns including grasping, pinching,
reaching, lifting, and placing. The participant completes these tasks in a repetitive fashion.
Repetitive practice and shaping are used to retrain the brain and rebuild the neuropathways that
were damaged as a result of the stroke. Repetitive practice of specific tasks may encourage motor
planning and experience-related adaptations. Daily tasks are also integrated into the therapeutic
protocol to increase strength, range of motion, and muscle tone in the affected upper extremity
(Boake et al., 2007).
Blanton and Wolf (1999) discussed the success of CIMT in terms of restoring upper
extremity function 3 to 9 months post CVA, compared to traditional stroke rehabilitation. The
CIMT 11
researchers noted that the benefits of restricting the unaffected arm remained after the constraint
was removed. Their research showed that learned non-use does exist, and when an individual is
forced to use their affected arm, the phenomenon can be reversed. With the help of an intense
CIMT protocol, learned non-use can be overcome and clients can regain some function and
movement in their affected limb.
Neuroplasticity
When learned non-use occurs, the individual compensates for the lack of movement from
the affected extremity, making the non-affected extremity more dominant. Individuals acquire
non-use when they attempt to use their affected limb in an activity and fail at the task, after
sustaining an injury. Unfortunately, individuals who do not use or ignore one side of the body are
limiting their freedom and independence, and decreasing their quality of life (Bonifer, Anderson,
& Arciniegas, 2005).
The idea of neuroplasticity has been used to explain the effects of repetitive, forced use
on upper extremity function post brain insult. Neuroplasticity is the brain’s ability to reorganize
itself in efforts to compensate for loss of function due to damage to one area of the brain.
Research conducted by Dombovy (2004) demonstrated that repetitive use of an involved
extremity is key to optimal brain reorganization status post CVA. According the neuroplasticity
theory, the structures of the brain lying adjacent to the area where the damage (infarct) occurred,
will reorganize and function for that area. CIMT and mCIMT have indeed been shown to
produce both clinical improvement and cortical reorganization in chronic stroke patients.
Furthermore, early forced arm use or exercise of the affected extremity post CVA has been
shown to stop cell loss and disuse that will lead to degeneration (Kleim, Jones, & Schallert,
2003).
CIMT 12
Outcome Potential
Hakkennes and Keating (2005) completed a metaanalysis of a number of trials that
examined the effectiveness of CIMT compared to other rehabilitative techniques in the areas of
quality of life, patient satisfaction, health care costs, and improved function. Overall, it appears
that CIMT benefits those who comply with the strict protocol and commit themselves fully to the
program. According to Wolf et al. (2006), in the EXCITE randomized clinical trial, CIMT
participants showed statistically significant improvements of upper extremity function in
comparison to participants receiving traditional therapy. The results of this study, which
included 222 participants within seven clinical sites, were that arm mobility increased
significantly and lasted for more than a year.
According to Ching-yi, Chia-ling, Wen-chung, and Keh-chung (2007), learned non-use
may also occur if patients are advised by others to rely on their unaffected arm to complete tasks,
to avoid becoming frustrated with attempts to use their affected side. CIMT can be implemented
with those who have experienced a stroke and have hemiparesis, to reverse the debilitation of
learned non-use. Through consistent constraint wear, the individual will begin to relearn that it
is possible to use the affected arm in daily tasks (Hakkennes & Keating, 2005).
Quality of Life
Quality of life may be simply described as a person’s individual perception and feelings
of overall enjoyment and satisfaction with life. Quality of life after a stroke is evaluated by
looking at various factors. Age, gender, the ability to perform activities of daily living (ADL),
level of disability, support of friends and family, the presence of depression, and living
arrangements can all have a significant impact on the level of quality of life post stroke (Nichols-
Larsen, Clark, Zeringue, Greenspan, & Blanton, 2005). Quality of life is an important factor to
CIMT 13
consider when investigating the effects of a stroke and outcomes of stroke rehabilitation.
Feelings of well-being are important in order to promote the continuation of positive healthcare
outcomes throughout rehabilitation and after. However, despite the importance of quality of life
at this time, there has been limited research exploring the impacts of various approaches to stroke
rehabilitation on quality of life (Carod-Artal, Egido, Gonza´lez, & de Seijas, 2000).
Carod-Artal et al. (2000) have suggested that four areas of health (physical, psychosocial,
functional, and social) must be explored in the assessment of post-stroke quality of life. Physical
health includes any physical symptoms experienced as a result of disease. Psychological health
is described as functioning within the emotional and cognitive domains. Functional health refers
to independent living capabilities, such as care of self, mobility and successful role opportunities
and fulfillment. Social health includes the presence and amount of support available through
family, friends, and the community.
Measuring Quality of Life Post-CVA
As reported by Carod-Artal et al. (2000), quality of life is difficult to consistently
measure, specifically in regards to a cerebral vascular accident, due to problems with construct
validity. The quality of life an individual reports is based on his/her own perception, and may
vary greatly when compared from person to person. In addition, it is difficult to compare
statistics or opinions taken from patients who have variability in the effects of their condition,
and treatment programs received (such as programs at general rehabilitation centers versus
specialized stroke rehabilitation centers). Despite these issues, it is vital that therapists attempt to
provide treatment that may address quality of life, and help promote functioning at the highest
level possible, to ensure positive results are maintained and continued after the rehabilitation
program has ceased (Carod-Artal et al.). However, there is minimal research exploring this
CIMT 14
aspect of functioning after a CVA, or how specific types of treatment interventions affect quality
of life (Hakkennes & Keating, 2005).
The quality of life of an individual may be compromised as a result of a stroke.
Immediate changes in function that occur after a stroke may lead a person to believe that he/she
may never use his/her extremities to their full potential again. Learned non-use occurs as a result
of compensating for hemiparesis. CIMT forces an individual to overcome learned non-use by
using the affected limb as the primary limb in activities of daily living.
CIMT has been gaining in popularity due to its consistent effectiveness in remediating
deficits in upper extremity function resulting from CVA. However, there is very little research
available on the effects of CIMT on quality of life. Yet, the success of CIMT and mCIMT on
individuals post stroke in other areas of function, such as improved performance and use of the
affected limb after participating in such a program, provides reason to believe that quality of life
may be a targeted outcome to be improved through mCIMT/CIMT as well. Restoration of upper
extremity function may lead to improved participation, promoting an increase in the perception
of quality of life.
Method
Research Design
A mixed methods approach, consisting of qualitative and quantitative methodology, was
used in this study. The quantitative portion of the study involved use of a quasi-experimental,
nonequivalent, two-group pretest-posttest design (as described in Portney & Watkins, 2008).
Qualitative data was collected via client journaling and a post-treatment focus group. Together,
these approaches allowed the researchers to examine the effects of CIMT and mCIMT on quality
of life. Treatment groups were determined via participants’ stated preference (CIMT vs. mCIMT
CIMT 15
protocol), as well as participants’ individual capabilities and therapeutic tolerance for the
requirements of each protocol.
Participants
In order to participate in this study, participants were required to meet specific criteria for
CIMT, as outlined by Blanton and Wolf (1999). These criteria included the ability to complete a
specific set of active movements with the affected arm. These movements included: 45-90
degrees of shoulder flexion and abduction; 45 degrees of external rotation at the shoulder;
minimal active elbow extension; 45 degrees of forearm supination and pronation; at least five
degrees of wrist extension; and five degrees of active digital extension (specifically in the thumb,
index, and middle fingers). Each participant was also required to be able to grasp and release a
washcloth three times within one minute (Blanton & Wolf).
Exclusion criteria included the presence of any prior medical issues that could potentially
interfere with CIMT/mCIMT treatment, such as recent myocardial infarction, seizures, severe
osteoporosis, or any condition that a referring physician may have considered to be dangerous
for participants’ health. Shoulder pain (such as rotator cuff pain, bursitis, or tendonitis), with the
exception of arthritis, was also an exclusionary criterion. In addition, that participants had to be
six months or more post-stroke at initial evaluation, able to understand verbal and written
instructions, and have satisfactory activity tolerance. Potential clients also needed to have
enough strength and endurance to complete each day’s therapeutic interventions, and be able to
participate in the pre and post-test assessments and reassessments. The participants were also
required commit to the two or four week program and adhere to the strict protocol.
Ten participants were selected from a convenience sample of people who responded to
advertisements for the study. The sample was split into two treatment groups, with four
CIMT 16
participants in each based on client preference, individual capabilities, and therapeutic tolerance
for each protocol. Although ten participants began the study, eight participants followed
protocol and completed the program.
Instrumentation
The Stroke Impact Scale Version 3.0 was used to gather quantitative data regarding
participants’ quality of life in the areas of physical, mental, social, and emotional functioning.
The Stroke Impact Scale (SIS) is a 60-item self report that takes approximately 10 to 15 minutes
to complete. It evaluates eight domains of functioning believed to impact an individual’s quality
of life: strength, mobility, hand function, ADLs and IADLs, memory and thinking, emotion,
communication, and social participation. Clients rate how their stroke has affected each domain,
on a Lickert scale. The SIS also contains a final question that asks clients to rate their perception
of overall recovery, from 0 (no recovery) to 100 (full recovery) (Carod-Artal et al., 2008).
The Stroke Impact Scale 3.0 has been previously evaluated for validity and reliability. It
was found to have satisfactory internal reliability, test-retest reliability, and adequate convergent
validity. Thus, the Stroke Impact Scale has been deemed a valid tool to assess the quality of life
of stroke patients (Carod-Artal et al., 2008).
In the present study, qualitative data was collected throughout the program via progress
notes and journals, as well as at the end of the program through the use of a focus group. Overall
satisfaction with the CIMT/mCIMT program was determined from the clients’ feedback
recorded in progress notes and how well they use their affected arm in daily occupations after
participating in the program.
Questions asked during the focus group were designed to facilitate communication
between participants and to allow the participants to verbalize their perceptions regarding quality
CIMT 17
of life following a stroke. The questions focused on participants’ thoughts regarding the
CIMT/mCIMT program and protocol, and quality of life before and after participation in the
program. Follow-up interviews with four participants were also carried out in the fall of 2009,
three-month post-treatment. The purpose of the interviews was to evaluate the long-term effects
of CIMT/mCIMT on the involved participants.
Procedures
Study site. The study was completed on the campus of a public medium-sized university
in the Midwestern United States. All treatment was provided in a group setting. However, all
participants worked individually with occupational therapy graduate students with advanced
training in CIMT/mCIMT, under the supervision of at least one professor who was a registered
occupational therapist (OTR). The student therapist to participant ratio was 1:1 or 2:1. The
study was approved by the University’s Institutional Review Board prior to implementation.
Data collection. The Stroke Impact Scale 3.0 was administered pre and post treatment
within the treatment facility. Participants were instructed to complete the scale independently or
with assistance from family or caregivers. Assistance from the student therapist was provided if
necessary for correct completion of the assessment.
Researchers also took notes of progress or decline of individual participants throughout
the completion of various exercises and activities, in order to effectively document responses for
qualitative data collection. Additional data regarding the participants’ perception of themselves
throughout the program was collected from several different sources to establish themes and
enable the participants to be active members of the intervention process. The clients were given
journals to log their experiences of the CIMT/mCIMT program and to reflect on mini-milestones
CIMT 18
achieved. They were encouraged to reflect upon their daily journal entries with their student
therapist.
Two focus groups were also conducted to allow the participants to share how
CIMT/mCIMT treatment affected their perceived level of function. The first focus group took
place two weeks into treatment, and included all participants. The second one took place four
weeks post treatment on the final day of assessment; it included only the mCIMT participants.
Researchers took notes during the focus groups, noting clients’ feelings of satisfaction about the
program, as well as any issues or concerns that participants may have had regarding the
treatment. Questions focused on changes in occupational performance or quality of life
experienced by participants from pre to post intervention. Both focus groups were digitally
recorded.
Intervention. During activities, each participant wore a mitt on the unaffected upper
extremity to force the use of the affected upper extremity. Mitts were fabricated with cotton and
netting to provide comfort and breathability for each client; the hand and wrist were kept in a
neutral position during activities. The mitt served as a physical barrier and reminder to refrain
from using unaffected upper extremity.
Activities that the clients participated in were based on theories concerning shaping and
repetition, with the overall goal being the reduction of the learned nonuse phenomenon that
typically occurs with hemiplegia (Wolf et al., 2006). The participants completed many
shaping/adaptive activities involving preparatory methods and purposeful activities, as well as
occupation-based activities. Some examples of purposeful activities that were implemented
include putting pennies in a bank, peg boards, and manipulating nuts and screws. Some
CIMT 19
examples of occupation-based activities included home maintenance, work-simulation, preparing
and eating meals, and playing cards, board games, and outdoor games.
Individuals’ treatment was centered on their goals, strengths, weaknesses, and current
recovery stage. Participants’ interests were considered during treatment planning so that clients
would perceive treatment activities as being both meaningful and purposeful (Kramer, Hinojosa,
& Royeen, 2003). All interventions were planned with reference to the Occupational Therapy
Practice Framework: Domain & Process in regards to activities of daily living (American
Occupational Therapy Association, 2008) as well as theory of CIMT/mCIMT.
Intervention activities focused on progressive arm movements deviating away from
flexor synergy. Therapeutic activities (tabletop and functional tasks, such as use of clothespins
and thera-putty) were used to facilitate repetitive use of the affected upper extremity.
Neurorehabilitative techniques were incorporated in blocked and random practice. Rood
techniques (or associated reactions), proprioceptive neuromuscular facilitation (PNF) methods,
and Affolter techniques (hand over hand guidance) were also used during treatment sessions.
There were no activities integrated into treatment specifically to address quality of life.
However, in completing the previously mentioned activities, the goal of treatment was to
increase independence and confidence in performing a variety of daily tasks, leading to an
overall increase in quality of life. Furthermore, many activities were chosen to facilitate
socializing and relationship building between the clients, in order to make treatment more
enjoyable and encourage building of support systems.
For participants at a Brunnstrom level four, the student therapists utilized a bottom-up
approach to treatment with a focus on occupation as a means (Kramer et al., 2003), preparatory
methods, and purposeful activity (AOTA, 2008). For participants at Brunnstrom levels five or
CIMT 20
six, therapy was based on a top-down approach, with increased focus on occupation-based
activities (AOTA). This approach allowed clients to focus on fine motor abilities and successful
task completion.
For participants receiving the traditional CIMT protocol, lunch was utilized as a part of
the program intervention; for participants in the mCIMT group, snacks were provided as a
chance to improve functional abilities and provide social interaction. Lunch was used as an
opportunity to encourage social interaction and rapport building within the group of clients.
Short breaks were given throughout the treatment session, and all tasks were graded to provide a
just right challenge to control the level of fatigue of the participant.
Another aspect of the program was the daily review of clients’ journals. In these
journals, the clients were asked to record the amount of time spent wearing the constraint, “mini
milestones” achieved within occupational performance, and the participants’ feelings about the
program. This was used so that both the therapists and participants could gain insight into
clients’ perceptions of the program and of their progress. If a certain skill was found to be
frustrating to a client at home, the client and student therapist worked together to come up with a
possible solution, such as treatments that focused on mastering the skill.
Data analysis. Descriptive statistics were used to analyze the quantitative data collected
from the Stoke Impact Scale. Analyses were done individually to examine each of the client’s
scores within each question in order to average and group the scores. The percentage differences
between individuals’ pre and post treatment scores were also determined. Calculations were also
completed to find averages between treatment groups. Differences were compared between the
CIMT and mCIMT groups; the researchers examined which group benefitted the most
concerning the impact each program had on quality of life.
CIMT 21
Due to a small sample size, the researchers were unable to use inferential statistics to test
for significance within the hypotheses. The researchers sought to determine if there was a
significant difference in the pre- to post-intervention Stroke Impact Scale Version 3.0 scores
among participants involved in a CIMT and mCIMT program. While examining the results,
researchers noted an inconsistency within two subquestions. These questions were eliminated
upon investigation due to the confusing nature of the reversal of Lickert scale values.
Qualitative data was also used to evaluate the impact of CIMT/mCIMT treatment on the
perceived quality of life and occupational functioning of participants. The coding process that
took place after the focus group consisted of the student therapists listening to the focus group
transcription, recording notes, and referencing daily progress notes to identify themes to
determine the effectiveness of CIMT/mCIMT in promoting quality of life in post-stroke clients.
Trustworthiness was a priority while gathering and assessing qualitative data during the
CIMT/mCIMT study. Any changes within the context are noted in limitations in order to
increase the dependability of this study. The researchers gathered information from multiple
sources at various times and contexts throughout the study, which supported triangulation on the
data collected (including the focus group, journals, and conversations with the clients during
each treatment session). Member checking was also completed to ensure that the client’s
perceptions accurately matched the therapists’ interpretation of progress made in CIMT/mCIMT.
Furthermore, data was themed and organized by thirteen student therapists involved with the
project, to ensure multiple perspectives and viewpoints were utilized to ensure content validity to
the qualitative findings.
Results
Results of Quantitative Data Analysis
CIMT 22
Eight participants (four who received CIMT and four who received mCIMT) were
evaluated in regards to their quality of life pre and post intervention using the Stroke Impact
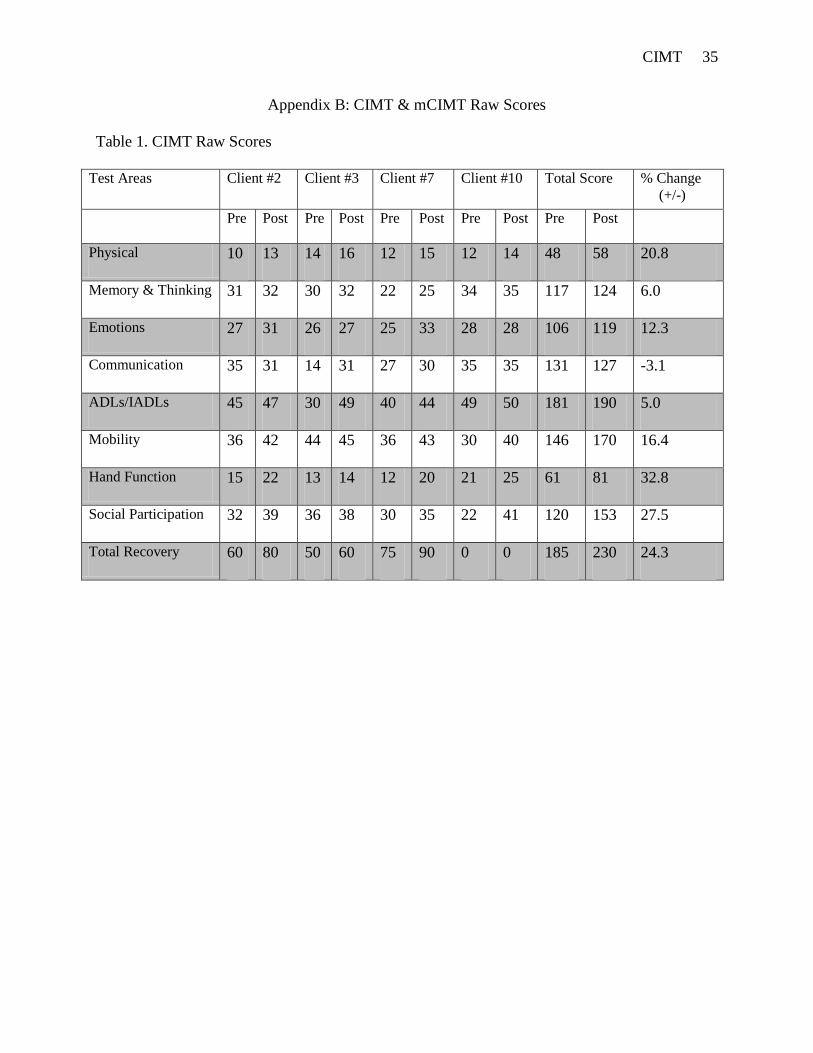
Scale. Themes were derived (see Appendix A). The final analysis indicated that the four CIMT
participants (Appendix B, Table 1) showed improvements in all subquestions, with the exception
of communication, of the Stroke Impact Scale. The mCIMT participants (Appendix B, Table 2)
showed positive improvements in all subsections of the Stroke Impact Scale. On average, the
CIMT participants increased their overall quality of life perception of themselves by 24.3%
between pre and post testing periods. In comparison, the mCIMT participants increased their
overall recovery perception by an average 17.9 percent. The percentage difference between pre
and post individual scores is found in Appendix C, Tables 1 and 2.
Results of Qualitative Data Analysis
The qualitative data demonstrated that overall, there was a perceived positive change
within the clients in their quality of life from pre to post intervention in both the CIMT and
mCIMT groups. Seven themes were gained from the data analysis of the qualitative portion of
the study. The data was collected from daily journals, daily notes, and a focus group for which
both two and four week participants were present. The themes identified included: 1) change of
lifestyle; 2) positive improvement; 3) “I want to see how far I can go”; 4) “Yes, I got what I
expected”; 5) decreased pain; 6) “It’s like having a job again”; and 7) overall enjoyment. These
themes are described in the following paragraphs, using direct quotes as well as summarized
thoughts from the participants.
Change of lifestyle. Participants were asked how their lifestyle was affected due to their
stroke. The common theme was a complete change of lifestyle. One participant stated that
his/her “lifestyle changed drastically, especially in the areas of work and leisure.” The stroke
CIMT 23
impacted not only the physical aspect of the participants’ lives but also the mental aspect. One
person described it as “a life-changing experience.” Yet, other participants were optimistic in
saying that you have to “accept it and make it better” and “if it takes me thirty years, I will get
better.”
Positive improvement. Participants noted high levels of satisfaction with mCIMT/CIMT
in terms of its impact on final occupational performance. There was a consensus of overall good
improvement among the clients, based upon client feedback received during and after the
program. One participant noted that now “I catch myself using my [affected] arm and hand” and
another stated that “other people are noticing changes,” as a result of participation in CIMT.
Participants stated that they were feeling better about themselves and the potential for improved
occupational performance. Several participants commented that they were doing “most
everything with my affected hand.” Another participant commented in a progress note, “I am
happy I can straighten my hand out; my fingers were on vacation for ten years.”
The progress that was seen during and after the program helped to improve the
participants’ quality of life by increasing their motivation to attempt things that they were not
able to do after experiencing the stroke. This motivation also improved their self-esteem and also
encouraged them to be more independent while at home.
“I want to see how far I can go.” Another area examined during the final evaluation
concerned how clients’ own perceptions of themselves changed as a result of the participation in
the mCIMT/CIMT program. The comments were both positive and negative. A participant
noted that “I can’t get past it; I feel people look at me,” when discussing having difficulty
confidently participating in activities without feeling self conscious due to the physical side
effects of stroke. However, other participants said that the little gains in life are what keep them
CIMT 24
going, one commented “look at it this way: people aren’t doing things like I am,” implying that
they have found different ways to continue to complete tasks that are important to them.
Expectations met. The next question asked all of the participants if they were satisfied
with the results obtained from participating in the CIMT/mCIMT program. There was an
overwhelming, unanimous yes. One exclaimed, “Yes, I am thrilled” while another stated “I am
seventy-five percent better [and] that’s good.” Another client claimed, “Yes, I got what I
expected.” Many of the participants were happy with the results of the program; one individual
stated that he is “Glad to participate” and he noticed that his affected arm had more endurance
when completing functional activities, contributing to his quality of life through participation.
Several clients were impressed by the results in such a way that they added they would like to
participate in the program again if it were to be offered.
Decreased pain. Several participants noted during daily discussion, documented through
SOAP notes, that they were experiencing noticeable changes in their pain. Pain experienced was
primarily noted within the shoulder of most clients. Reduced pain contributed to increased
function. One client stated, “I can button my shirt by myself now that my shoulder does not hurt
as much.” This client initially reported pain at a level of eight out of ten; at the end of the study
he reported a pain level of four out of ten. In addition, another client came in with low pain,
which increased with the sudden addition of intense treatment. By the end of the study, he was
experiencing no pain. Several clients noted decreased levels of pain contributed to improved
quality of life through enhanced sleep and functional skills.
“It’s like having a job again.” The participants were then asked what aspect of their lives
was most affected by participation in the CIMT/mCIMT program. One participant stated that the
program provided a daily schedule that made them feel like they had a job again. The early
CIMT 25
morning start each day provided a reason to get up in the morning, as well as a structured
environment for at least three hours on the weekdays. Having these resources gave the
participants an opportunity to complete tasks that were valuable to them every day and give each
day further purpose, contributing to their overall perception of quality of life.
Overall enjoyment. When participants were asked whether or not they enjoyed the
treatment activities, each responded positively. One participant responded, “Yes, I enjoyed it.
You guys made it interesting and fun.” Another participant stated that they wanted to come back
if the program were to be offered again. Overall, everyone enjoyed the activities that were
offered during the program, which helped make the program a success. Participants worked and
played together, fostering encouragement and amiability throughout the program.
Discussion
This study examined the effects of CIMT and mCIMT on quality of life among persons
demonstrating learned nonuse of an affected upper extremity status post CVA. The overall
findings of this study conclude that participants experienced positive outcomes concerning
improvement of quality of life after each of the programs. Our results show that although both
groups improved, mCIMT showed the biggest gains.
The qualitative information gathered from the therapists observations and focus group
resulted in seven themes, as earlier mentioned: change of lifestyle, positive improvement, “I
want to see how far I can go”, “Yes, I got what I expected”, Decreased pain, “It’s like having a
job again”, overall enjoyment). A common theme expressed among the research participants
was a dramatic increase in positive improvements and motivation to continue therapeutic gains.
Overall, participants met their expectations with the CIMT/mCIMT program stating that “now I
want to see how far I can go” because of participation in this study. In addition, another
CIMT 26
participant commented, “After participating in this program, I feel like I’m not alone in the
world” with this condition, and “Now I catch myself when I’m using my good hand and
consciously switch to my other hand.”
Limitations
While gathering qualitative data, the researchers noted that some participants were less
apt to consistently fill out daily journal entries. Daily progress notes were not always completed
throughout each session, causing post-session notes to be incomplete, which may have led to
some subjective information being unnoted.
The small sample size also prevented the researchers from testing for statistical
significance in the Stroke Impact Scale. Portney and Watkins (2000) stated that
the influence of sample size on the power of a test is critical. The larger the sample size,
the greater the statistical power. Smaller samples are less likely to be good
representatives of population characteristics, and therefore, true differences between
groups are less likely to be recognized. When very small samples are used (n<30), as is
often the case in clinical research, power is substantially reduced. (pp. 403)
In addition, neither single nor double blinding was used upon initial evaluation. Participants
were also given the choice of which treatment group to be in, in effort to fit schedules and
encourage attendance. Lack of randomization may have also been a limitation in this study.
Small sample size prevented the use of inferential statistics in the data analysis of this
study. Additional general limitations involving this CIMT/mCIMT study include having a small
sample size of Caucasian participants, each of middle socioeconomic class, from a limited
geographic region. The participants were screened for underlying conditions; however, clients
who had assistive devices and expressive aphasia were also accepted. Additionally, two
CIMT 27
participants had prior obligations and were unable to make it to a few of the therapy sessions.
Finally, inconsistency in constraint-wearing schedule and attendance may have weakened the
ability to compare these results to future CIMT/mCIMT study results.
Conclusions
The results of this study indicated that quality of life in clients that have experienced
stroke can be impacted through the use of this treatment protocol. In conclusion, the quantitative
findings showed that both groups, the two week group and the four week group, showed
improvement; the four-week group showed a greater increase in their perception of their quality
of life post treatment than the two-week group.
The qualitative data gathered through daily notes, daily journals, and a focus group
illustrated that participants found CIMT and mCIMT to be beneficial in impacting their recovery
post-stroke. Seven themes were found to be relevant to participants, which included: change of
lifestyle, positive improvement, “I want to see how far I can go”, “Yes, I got what I expected”,
Decreased pain, “It’s like having a job again”, and overall enjoyment. Participants agreed that
the treatment was worthwhile and although the protocol was demanding, they would be willing
to participate in a future program.
Future recommendations for research in the impact of CIMT/mCIMT on clients with
stroke include investigation into (a) the adjustment of roles and (b) the effects of a follow-up
CIMT/mCIMT program with adults. Role adjustment was shown to be a great impacting factor
for participants’ quality of life in this study. Performance within these roles was very important
to participants. Several participants also mentioned that they would again participate in a
CIMT/mCIMT program; a follow up program may show additional benefits for experienced
clients. In addition, examining and utilizing a consistent warm up phase may show to be
CIMT 28
beneficial for optimal results in future studies. Examination of these areas may further
contribute to the knowledge of the most effective way to use CIMT protocol.
Overall, this program showed that both groups experienced increases in function and
quality of life, especially in their perception of themselves in areas of: physical strength,
memory, emotional control, communication skills, mobility, hand use, and performance of
meaningful daily activities. The examination of these areas revealed that the clients’ self
efficacy of participation was shown to improve. Both CIMT and mCIMT groups expressed
satisfaction with the program and the results. The results of this study will contribute to the
current supportive evidence of the effectiveness of CIMT and mCIMT as a treatment for people
who have experienced stroke and have lowered levels of quality of life.
CIMT 29
Acknowledgments
This study was completed in partial fulfillment of the requirements for the student
researcher’s Master of Science in Occupational Therapy degree campus of a public state
university campus in the Midwestern United States. We would like to thank Donald Earley,
OTD, MA, OTRL, associate professor of Occupational Therapy, for the CIMT/mCIMT training,
continuous support, guidance, and vast knowledge throughout the treatment sessions. We would
also like to thank Ellen Herlache, MA, OTRL, Research Coordinator for the Occupational
Therapy program, for supervising during the treatment sessions, and guidance throughout the
research project design, implementation, and statistical analysis portion of our study. In
addition, we thank Jill Ewend, OTRL, Simulation Learning Laboratory Associate for the OT
department, for her supervision and assistance during the treatment sessions. We would like to
thank J.J. Boehm for his assistance with advertising. Finally, we would like to thank our
participants. Without their commitment and cooperation, our study would have not taken place.
CIMT 30
References
American Heart Association. (2008, June 9). Stroke statistics. Retrieved from
http://www.americanheart.org/presenter.jhtml?identifier=4725.
American Occupational Therapy Association (2008). Occupational therapy framework: Domain
and process. American Journal of Occupational Therapy, 56, 609-639.
Blanton, S., & Wolf, S. L. (1999). An application of upper-extremity constraint-induced
movement therapy in a patient with subacute stroke. Physical Therapy, 79, 847-853.
Boake, C., Noser, E.A., Ro, T., Baraniuk, S., Gaber, M., Johnson, R., et al. (2007). Constraint-
induced movement therapy during early stroke rehabilitation. Neurorehabilitation and
Neural Repair, 21, 14-24.
Bonifer, N. M., Anderson, K. M., & Arciniegas, D. B. (2005). Constraint-induced movement
therapy after stroke: Efficacy for patients with minimal upper-extremity motor ability
Archive Physical Medical Rehabilitation, 86, 1867-1873.
Caimmi, M., Carda S., Giovanzana, C., Maini, E. S., Sabatini, A. M., Smania, N., et al. (2008).
Using kinematic analysis to evaluate constraint-induced movement therapy in chronic
stroke patients. The American Society of Neurorehabilitation, (22)1, 31-39.
Campos, S. S., & Johmson, T.M. (1990). Cultural considerations. In B. Spilker (Ed.), Quality of
life assessment in clinical trials (pp. 163-170). New York: Raven.
Carod-Artal, J., Coral, L. F., Trizotto, D. S., & Moreira, C.M. (2008). The Stroke Impact Scale
3.0 evaluation of acceptability, reliability, and validity of the Brazilian version. Journal
of American Heart Association, 39, 2477-2484.
CIMT 31
Carod-Artal, J., Egido, J.A., Gonza´lez, J.L., & De Seijas, E. V. (2000). Quality of life among
stroke survivors evaluated 1 year after stroke: Experience of a stroke unit. Stroke, 31,
2995-3000.
Ching-yi, W., Chia-ling, C., Wen-chung, T., Keh-chung, L., & Shih-han, C. (2007). A
randomized controlled trial of modified constraint-induced movement therapy for elderly
stroke survivors: Changes in motor impairment, daily functioning, and quality of life.
Archive Physical Medical Rehabilitation, 88, 273-278.
Dettmers, C., Teske, U., Hamzei, F., Uswatte, G., Taub, E., & Weiller, C. (2005). Distributed
form of constraint-induced movement therapy improves functional outcome and quality
of life after stroke. Archive Physical Medical Rehabilitation, 86, 204-209.
Dombovy, M. L. (2004). Understanding stroke recovery and rehabilitation: Current and
emerging approaches. Current Neurology and Neuroscience Reports, 4; 31–35.
Earley, D. (2008). Constraint induced movement therapy for the rehabilitation of stroke patients.
University Center, MI: Saginaw Valley State University.
Eckert, J. (2007). Cerebrovascular accident. In B. Atchison & D. Dirette (Eds.), Conditions in
occupational therapy: Effects on occupational performance (pp. 177-179). Baltimore,
MD: Lippincott Williams & Wilkins.
Hansen, R., Dirette, D. K., & Atchison, B.J. (2007). Thinking like an OT. In B. Atchison & D.
Dirette (Eds.), Conditions in occupational therapy: Effects on occupational performance
(pp. 6). Baltimore, MD: Lippincott Williams & Wilkins.
Hakkennes, S., & Keating, J.L. (2005). Constraint-induced movement therapy following stroke:
A systematic review of randomized controlled trials. Australian Journal of
Physiotherapy, 51, 221–231.
CIMT 32
Jamison, P.W., & Orchanian, D.P. (2007). Cerebrovascular accident. In B. Atchison & D. Dirette
(Eds.), Conditions in occupational therapy: Effects on occupational performance (pp.
186). Baltimore: Lippincott Williams & Wilkins.
King, R. B. (1996). Quality of life after stroke. Stroke, 27, 1467-1472.
Kleim, J.A., Jones, T.A., & Schallert, T. (2003). Motor enrichment and the induction of plasticity
before or after brain injury. Neurochemical Research, 28 (11).
Kolb, B., & Whishaw, I. (2003). Fundamentals of human neuropsychology. New York, NY:
Worth Publishers.
Kramer, P., Hinojosa, J., & Royeen, C. B. (2003). Perspectives in human occupation:
Participation in life. Baltimore, MD: Lippincott Williams & Wilkins.
Lewis, C., Freeman, J., Fox, M., Bower, L., & Pena, F. (2005). Constraint-induced movement
therapy as a home activity-A case report. Palaestra, 21, 38-55.
Macko, R. F., Benvenuti, F., Stanhope, S., Macellari, V., Taviani, A., Nesi, B., et al. (2008).
Adaptive physical activity improves mobility function and quality of life in chronic
hemiparesis. Journal of Rehabilitation Research and Development, 45, 323-328.
Nichols-Larsen, D.S., Clark, P.C., Zeringue, A., Greenspan, A., & Blanton, S. (2005). Factors
influencing stroke survivors’ quality of life during subacute recovery. Stroke, 36, 1480-
1484.
Portney, L., & Watkins, M. (2009). Foundations of clinical research: Applications to practice
(3rd
ed.). Upper Saddle River, NJ: Pearson Prentice Hall.
Wolf, S. L., Winstein, C. J., Miller, P., Taub, E., Uswatte, G., Morris, D., et al. (2006). Effect of
constraint-induced movement therapy on upper extremity function 3 to 9 months after
CIMT 33
stroke: The EXCITE randomized clinical trial. The Journal of the American Medical
Association, 296, 2095-2104. Retrieved from http://jama.ama-assn.org.
Wu, Ching-yi, Keh-chung Lin, Hsieh-ching Chen, I-hsuen Chen, & Wei-hsien (2007). Effects of
modified constraint-induced movement therapy on movement kinematics and daily
function in patients with stroke: A kinematic study of motor control mechanisms. The
American Society of Neurorehabilitation 21(5), 460-66.
CIMT 34
Appendix A
Table 1: Stroke Impact Scale Questionnaire Themes
1) Physical problems which may have occurred as a result of your stroke.
2) Memory and thinking
3) How you feel, about changes in your mood and about your ability to control your
emotions.
4) Your ability to communicate with other people, as well as your ability to understand what
you read and what you hear in a conversation.
5) Activities you might do during a typical day.
6) Your ability to be mobile, at home and in the community.
7) Your ability to use your hand that was MOST AFFECTED by your stroke.
8) How stroke has affected your ability to participate in the activities that you usually do,
things that are meaningful to you and help you to find purpose in life.
9) On a scale of 0 to 100, with 100 representing full recovery and 0 representing no recovery,
how much have you recovered from your stroke?
CIMT 35
Appendix B: CIMT & mCIMT Raw Scores
Table 1. CIMT Raw Scores
Test Areas Client #2 Client #3 Client #7 Client #10 Total Score % Change
(+/-)
Pre Post Pre Post Pre Post Pre Post Pre Post
Physical 10 13 14 16 12 15 12 14 48 58 20.8
Memory & Thinking 31 32 30 32 22 25 34 35 117 124 6.0
Emotions 27 31 26 27 25 33 28 28 106 119 12.3
Communication 35 31 14 31 27 30 35 35 131 127 -3.1
ADLs/IADLs 45 47 30 49 40 44 49 50 181 190 5.0
Mobility 36 42 44 45 36 43 30 40 146 170 16.4
Hand Function 15 22 13 14 12 20 21 25 61 81 32.8
Social Participation 32 39 36 38 30 35 22 41 120 153 27.5
Total Recovery 60 80 50 60 75 90 0 0 185 230 24.3
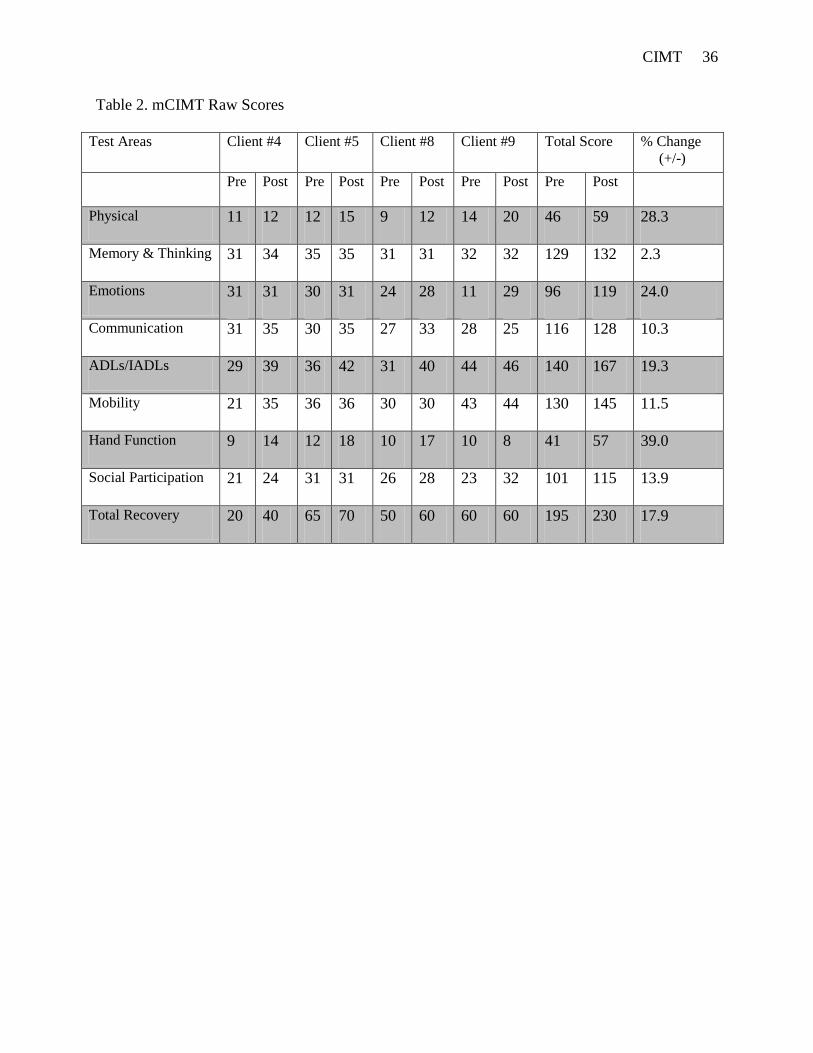
CIMT 36
Table 2. mCIMT Raw Scores
Test Areas Client #4 Client #5 Client #8 Client #9 Total Score % Change
(+/-)
Pre Post Pre Post Pre Post Pre Post Pre Post
Physical 11 12 12 15 9 12 14 20 46 59 28.3
Memory & Thinking 31 34 35 35 31 31 32 32 129 132 2.3
Emotions 31 31 30 31 24 28 11 29 96 119 24.0
Communication 31 35 30 35 27 33 28 25 116 128 10.3
ADLs/IADLs 29 39 36 42 31 40 44 46 140 167 19.3
Mobility 21 35 36 36 30 30 43 44 130 145 11.5
Hand Function 9 14 12 18 10 17 10 8 41 57 39.0
Social Participation 21 24 31 31 26 28 23 32 101 115 13.9
Total Recovery 20 40 65 70 50 60 60 60 195 230 17.9
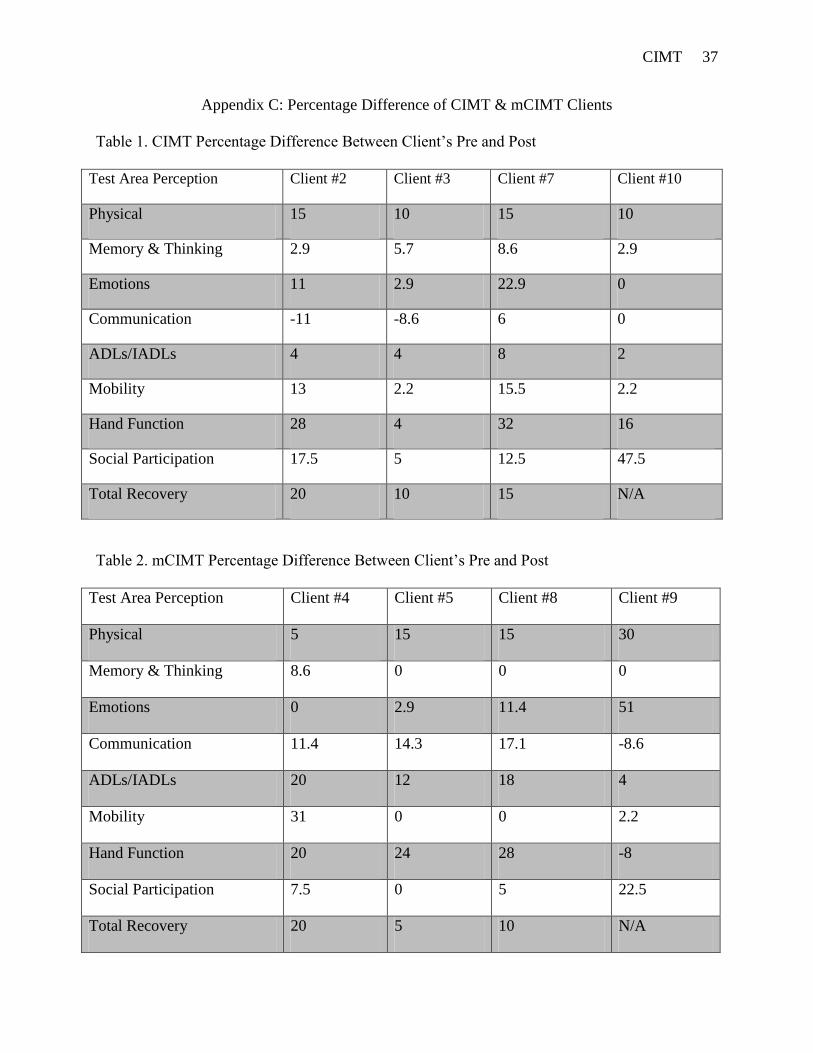
CIMT 37
Appendix C: Percentage Difference of CIMT & mCIMT Clients
Table 1. CIMT Percentage Difference Between Client’s Pre and Post
Test Area Perception Client #2 Client #3 Client #7 Client #10
Physical 15 10 15 10
Memory & Thinking 2.9 5.7 8.6 2.9
Emotions 11 2.9 22.9 0
Communication -11 -8.6 6 0
ADLs/IADLs 4 4 8 2
Mobility 13 2.2 15.5 2.2
Hand Function 28 4 32 16
Social Participation 17.5 5 12.5 47.5
Total Recovery 20 10 15 N/A
Table 2. mCIMT Percentage Difference Between Client’s Pre and Post
Test Area Perception
PPPPerPercePerception
Client #4 Client #5 Client #8 Client #9
Physical 5 15 15 30
Memory & Thinking 8.6 0 0 0
Emotions 0 2.9 11.4 51
Communication 11.4 14.3 17.1 -8.6
ADLs/IADLs 20 12 18 4
Mobility 31 0 0 2.2
Hand Function 20 24 28 -8
Social Participation 7.5 0 5 22.5
Total Recovery 20 5 10 N/A

CIMT 38





























