Embed Size (px)
Citation preview

Phill Harniess (Physio) and Jackie Gordon (OT) 22.11.12
Community Therapies Hackney Ark
Homerton University Trust
From Trial to Application:
Constraint Induced
Movement Therapy (CIMT)
in Paediatrics
Constraint induced movement therapy: A randomised
controlled Trial in Children with Hemiplegic cerebral
palsy – CATCH Trial

• To discuss our involvement in the CATCH trial
• Critically evaluate the trial and literature in relation to practice
• Where next in our service?
• Questions at end

• Cerebral Palsy: most common childhood neuromotor disability - prevalence 2 per 1000 children born in Europe (Johnson, 2002)
• Hemiplegia cerebral palsy (HCP) most common presentation (Stanley et al, 2000 cited by, Sakzewski et al, 2011)
• Lack of strong evidence base for treatment approaches (Sakzewski et al, 2009a)

• Taub’s monkeys – de-afferented peripheral sensory nerve
• Established in Adult stroke rehabilitation
• Now in paediatrics growing body of evidence > 6 years
What do you know about CIMT?

A randomised controlled Trial in Children with HCP
• Research Project (multi-site): largest UK CIMT RCT in paeds to date (n=60)
• Cast vs. manual constraint - control (1hr/day) • Children with HCP aged 18 months – 4 years old
• Application pragmatic and transferable to National Health
Service (NHS)
CATCH Trial Background

• A RCT to compare two methods of upper limb
constraint induced movement therapy
• Power calculation: Sample size of 29 in each group 80%
power to detect an effect size of 0.75 at 24 weeks (p=<0.05, 2tailed t-test)
• Null Hypothesis:
Using CIMT with casting in pre-school children with HCP
has no significant effect on improving functional abilities compared to manual restraint

Parents/guardians of suitable participants
are approached
Control arm
(2-4 weeks after randomisation)
Outcome measure post intervention (10 weeks)
Outcome measure at 24 weeks
Intervention arm
(2-4 weeks after randomisation)
Outcome measure post intervention (10 weeks)
Outcome measure at 24 weeks
Exclusion: Parent not wanting to participate continue with normal
therapy input Informed Consent
Baseline Assessments
Randomisation
Exit Study

• Heterogenous
• Too severe? – Most studies select higher level clients (Huang et al, 2009)
- Children with less hand function can benefit more (Sakzewski et al, 2009b)
• Lack of potential engagement? - Research needs to be representative (Greenhalgh and Wessely, 2004)
Our Participants (n=4)

Assisting Hand Assessment
(AHA)
Quality of Upper Extremity Skill Test (QUEST)
PEDsQL and PEDs CP
questionnaires
Parental and Nursery
Feedback
Pre and Post Outcome Measures
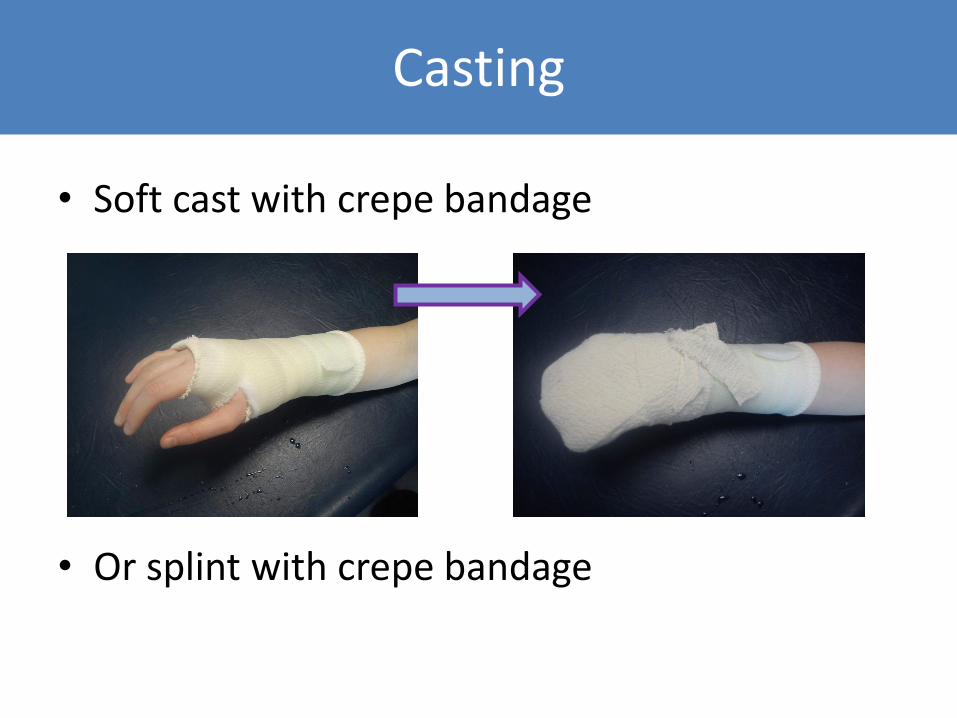
• Soft cast with crepe bandage
• Or splint with crepe bandage
Casting

• 6 weeks of active CIMT within 10 weeks, 2 week active – 2 week rest
• Therapy 1x/week
• Input - training nursery and clinic/home to carry out home programme
• Daily diaries
Therapy Intervention

• Therapy through play (follow child):
• Aim (Choosing achievable tasks with achievable motor patterns): » Spontaneous use/activity
» Reduced inattention affected side
» Reaching
» Finger extension
» Gross grasp
» Etc…
Therapy (with home programme – 1 hour/day)

• Parent feedback “ His hand is more open and he uses it more as a support.” • Nursery feedback “She uses her hand during eating and is looking at her hand now”. • Therapy observations Reduced tone in affected hand/arm Increased active range of movement Increased spontaneous use of assisting hand to support activity
Observations

CST ipsilateral and contralateral
connectivity in spinal cord
Cortical activity drives CST refinement
CST predominantly contralateral
connectivity (10% ipsilateral
connections)
Neonate 2 years
(Martin et al, 2011)
Effect of Unilateral Cortical Lesion on Corticospinal Tract (CST)
Normal development

CST ipsilateral and contralateral
connectivity in spinal cord
Non-effected Cortical hemisphere activity predominantly drives
CST refinement
Abnormal connectivity - Increased ipsilateral
connections from non-effected hemisphere
Aberrant Ipsilateral connectivity associated with decreased fine motor function (Eyre et al, 2007).
Unilateral lesion

Literature Overview
No Significant effect:
Cast 2 hours/day
1hr wk OT/ 6weeks
(Sung et al, 2005: n=31; <96mths)
Mitt 2 hours/day
8 weeks
(Wallen et al, 2011; n=50)
Significant Effect:
Splint glove 2 hours/day
2 hours therapy/ day
8 wks
(Eliasson et al, 2005; n=41)
6 hours sling/day
PT/OT - 6hr/d
10 days
(Gordon et al, 2006; n=20),
(Charles et al, 2006; n=22)
CIMT compared with Bimanual training (same protocol as above)
(Sakzewki et al, 2011; n=63)
CIMT significantly greater effect
Significant effect:
Cast 24 hours/day
PT/OT - 6 hrs/d
21 days
(Taub et al, 2004; n=18)
(De Luca et al, 2006; n=18)
INTENSITY

• More intensive = more effective
• Therapy input crucial
• But is boot camp therapy input realistic on NHS?
• Will each child tolerate 24 hours cast
• Argument for 6-12 month age application • before changes to CST and learned non-use (Martin et al, 2011)
Reflection Is our thinking constrained?

Meaningful change to
activity
Personal and environmental
factors
Impairment level
Intensity of Therapy Time
Our Reflections

• Protocol Pre- assessment 4 treatment session over 3 weeks while cast -> 1 week bimanual tasks Post treatment outcome measure assessment • Parent Information Sheet/Consent form
• Therapist competencies and training
• Treatment Pathway
• Evaluate service (future: school aged children/groups)
Service Development

• CIMT protocol transferrable to NHS
• Further consideration of therapy input intensity
• Treatment and research available for clients of all backgrounds
• Exciting new effective treatment available for children with hemiplegia in Hackney!
Conclusions

• Pauline Christmas – Chief Investigator
• Parents and children involved in the trial
Acknowledgements

References
• Charles JR, Wolf SL, Schneider JA and Gordon AM, 2006, Efficacy of a child-friendly form of constraint-induced movement therapy in hemiplegic cerebral palsy: a randomised control trial, Developmental Medicine and Child Neurology, 48: 635-642.
• DeMatteo C, Law M, Russell D, Pollock N, Rosenbaum P and Walter S, 1993, The Reliability
and Validity of the quality of upper extremity skills test, Physical and Occupational Therapy in Paediatrics, 13: 1-18.
• DeLuca SC, Echols K, Law CR and Ramey SL, 2006, Intensive pediatric constraint-induced therapy for children with cerebral palsy: randomized controlled crossover trial, Journal of Child Neurology, 21: 931-938.
• Eliasson AC, Krumlinde-Sundholm L, Shaw K and Wang C, 2005, Effects of constraint induced movement therapy in young children with hemiplegic cerebral palsy: an adapted model, Developmental Medicine and Child Neurology, 47: 266–275.
• Eyre JA, Smith M, Dabydeen L, Clowry GJ, Petracchi E, Battini R, Guzzetta A and Cioni G, 2007, Is Hemiplegic Cerebral Equivalent to Amblyopia of the Corticospinal System?, Annals of Neurology, 62: 493-503.

References
• Gordon A, 2011, To Constrain or not to Constrain, and other stories of intensive training for children with unilateral cerebral palsy, Developmental Medicine and Child Neurology, 53: (suppl. 4), 56-61.
• Gordon AM, Charles J and Wolf SL, 2006, Efficacy of constraint-induced movement therapy on involved upper-extremity use in children with hemiplegic cerebral palsy is not age dependent, Pediatrics, 117: 363-373.
• Greenhalgh T and Wessely S, 2004, ‘Health for me’: a sociocultural analysis of
healthism in the middle classes, British Medical Bulletin, 69: 197–213.
• Huang H, Fetters L, Hale J and McBride A, 2009, Bound for Success: A Systematic review of Constraint-Induced Movement Therapy in Children with Cerebral Palsy Supports Improved Arm and Hand Use, Physical Therapy, 89: 1126-1141.
• Johnson , 2002, Prevalence and characteristics of children with cerebral palsy in Europe, Developmental Medicine & Child Neurology, 44:9:633-640.

References
• Krumlinde-Sundholm L and Eliasson AC, 2003, Development of the Assisting Hand Assessment, A Rash-built measure intended for children with unilateral upper limb impairments, Scandanavian Journal of Occupational Therapy, 10: 16-26.
• Krumlinde-Sundholm L, Holmefur M, Kottorp A and Eliasson AC, 2007, The Assisting Hand Assessment: Current evidence of validity, reliability and responsiveness to change, Developmental Medicine and Child Neurology, 49: 259-264.
• Martin JH, Chakrabarty S and Friel KM, 2011, Harnessing Activity-Dependent Plasticity to Repair the Damaged Corticospinal Tract in an Animal Model of Cerebral Palsy, Developmental Medicine and Child Neurology, 53 (suppl. 4): 9-13.
• Sakzewski L, Ziviani J, Abbott DA, Macdonnell RA, Jackson GD and Boyd RN, 2011,
Randomized trial of constraint-induced movement therapy and bimanual training on activity outcomes for children with congenital hemiplegia, Developmental Medicine & Child Neurology, 53: 313–320.

References
• Sakzewski L, Ziviani J and Boyd RN, 2009a, Systematic Review and Meta-analysis of Therapeutic Management of Upper-Limb Dysfunction in Children with Congenital Hemiplegia, Pediatrics, 123: e1111- e1122.
• Sakzewski L, Ziviani J and Boyd RN, 2009b, Best Responders After Intensive Upper –limb training for Children with Unilateral Cerebral Palsy, Archive of Physical Medicine and Rehabilitation, 92: 578-584.
• Sung IY, Ryu JS and Pyun SB, 2005, Efficacy of forced-use therapy in hemiplegic cerebral palsy, Archive of Physical Medicine and Rehabilitation, 86: 2195-2198.
• Taub E, Ramey SL, DeLuca SC and Echols K, 2004, Efficacy of constraint-induced
movement therapy for children with cerebral palsy with asymmetric motor impairment, Pediatrics, 113: 305-312.
• Wallen M, Ziviani J, Naylor O, Evans O, Novak I and Herbert RD, 2011, Modified
constraint-induced therapy for children with hemiplegic cerebral palsy: a randomized trial, Developmental Medicine & Child Neurology, 53: 1091–1099.





























