Embed Size (px)
Citation preview

Referat
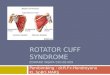
ROTATOR CUFF SYNDROME
Arranged by:
Esti Rahmawati Suryaningrum G0007064
Tutor:
dr. Tangkas Sibarani, SpOT, FICS
Clinical Department of Orthopaedic & Traumatology Sebelas Maret University
Hospital of Dr. Moewardi/ Orthopaedic Hospital of Prof. Dr. Soeharso
Surakarta

2012
LEGALY SHEET
Referat entitled “Rotator Cuff Syndrome” is arranged to fulfill the
requirement of clinical department of Orthopaedic & Traumatology Sebelas Maret
University Hospital of Dr. Moewardi/Orthopaedic Hospital of Prof. Dr. Soeharso, by:
Esti Rahmawati Suryaningrum G0007064
Has been approved by the referat tutor of the Orthopaedic Hospital of Prof.
Dr. Soeharso on May, 2012.
Tutor
dr. Tangkas Sibarani, SpOT, FICS

ROTATOR CUFF SYNDROME
DEFINITION
Rotator cuff syndrome is damage to the rotator cuff, is a part of the shoulder.
The rotator cuff is a group of four muscles that sit around the shoulder joint in a cuff-
like pattern. The rotator cuff attaches from the scapula, or shoulder blade, to the
humerus, or arm bone, and it functions to pull the arm into the shoulder socket,
stabilizing the arm, so that overhead movements can be performed.
Rotator cuff syndrome is a disorder most frequently diagnosed in those whose
work involves repeated or sustained raising of the upper arms more than 30° over
horizontal. Such repetitive motion irritates the muscles and tendons by putting
pressure against the bone at the top of the shoulder blade. When the arm is raised
repeatedly, front edge of the shoulder blade (acromion) can rub across the rotator cuff
(impingement syndrome or painful arc syndrome). If rotator cuff injuries are
diagnosed early, causes can be identified and effective treatments implemented,
thereby preventing further injury or deterioration.
INCIDENCE AND PREVALENCE
Shoulder pain is the third most common musculoskeletal disorder; estimates of
all shoulder disorders are 10 per 1,000 population, with a peak incidence of 25 per
1,000 population aged 42 to 46 years. Among those age 60 years or older, 21% were
found to have shoulder syndromes, most of which were attributable to the rotator cuff
(Roy). Nevertheless, the actual incidence of rotator cuff syndrome is uncertain since
about 34% of the population may have a torn rotator cuff but no pain (Roy).
RISK FACTOR
Workers at risk for rotator cuff syndrome are those required to repeatedly
move heavy weights over their heads, such as painters, welders, plate workers, and
slaughterhouse workers. This syndrome also has been reported in sewing machine
operators. It can occur in athletes who engage in sports such as swimming, tennis,
weightlifting, and baseball in which the arm is repeatedly raised over the head.
Younger individuals are more likely to experience rotator cuff syndrome as a result of

trauma, overuse, shoulder (glenohumeral) joint instability, or muscle imbalance. In
older individuals, the syndrome is more commonly related to chronic wear and
shoulder degeneration. Rotator cuff syndrome is most common in the dominant arm.
ANATOMY OF ROTATOR CUFF
The "cuff" is actually a group of four muscles and their tendons that work as a
unit to hold the bones of the shoulder together, allowing individuals to lift their arms
and reach overhead. Repetitive motion and overuse, along with individual variations
in the anatomy of the shoulder and trauma can lead to rotator cuff injuries.
The rotator cuff is the sheath of conjoint tendons which run over the top of the
shoulder capsule and inserts into the greater tuberosity of the humerus
the tendons are those of the short muscles of the shoulder - supraspinatus,
infraspinatus, teres minor and subscapularis
the cuff is covered anteriorly by the coracoacromial arch with the subacromial
bursa in between
the main role of the cuff is to stabilise the humeral head within the glenoid,
particularly when the arm is flexed or abducted by the deltoid muscle.

MuscleOrigin on scapula
Attachment on humerus
Function
Innervation
subscapularis muscle
subscapular fossa
lesser tuberosity (60%) or humeral neck (40%)
internally rotates the humerus
subscapular nerve (C5-6)
supraspinatus muscle
supraspinous fossa
inserts on the middle facet of the greater tuberosity
abduction of the arm
suprascapular nerve (C5)
infraspinatus muscle
infraspinous fossa
inserts posterior facet of theon the greater tuberosity
externally rotates the arm
suprascapular nerve (C5-6)
teres minor muscle
middle half of the lateral border
inserts on the inferior facet of the greater tuberosity
externally rotates the arm
axillary nerve (C5)
The subacromial space lies underneath the acromion, the coracoid process, the
acromioclavicular joint and the coracoacromial ligament. A bursa in the subacromial
space provides lubrication for the rotator cuff.
Supraspinatus is the cuff tendon most liable to injury. It is the most exposed of
the tendons - running over the top of the shoulder under the anterior edge of the
acromion and the adjacent acromioclavicular joint - and also has a relatively poor
arterial blood supply near to it's insertion into the greater tuberosity. Consequently,
`supraspinatus' is often used synonymously with `rotator cuff' when describing lesions
of this area.
the rotator cuff is the dynamic stabilizer of the glenohumeral joint
o the static stabilizers are the capsule and the labrum complex, including
the glenohumeral ligaments
o although the rotator cuff muscles generate torque, they also depress the
humeral head

o the deltoid abducts the shoulder
o without an intact rotator cuff, particularly during the first 60 degrees of
humeral elevation, the unopposed deltoid would cause cephalad
migration of the humeral head, with resulting subacromial
impingement of the rotator cuff
in patients with large rotator cuff tears, the humeral head is
poorly depressed and can migrate cephalad during active
elevation of the arm. This migration is sometimes evident even
on plain radiographs
the space between the undersurface of the acromion and the superior
aspect of the humeral head is called the impingement interval
this space is normally narrow and is maximally narrow when the
arm is abducted. Any condition that further narrows this space can
cause impingement
CLASIFICATION
Rotator cuff syndrome is divided into three stages of severity. In stage I,
swelling (edema) and/or bleeding (hemorrhage) occurs. Stage I is frequently
associated with an overuse injury. At this stage, the syndrome can either be reversed
or it can progress. In stage II, there is inflammation of the tendon (tendinitis) and
development of scar tissue (fibrosis). Stage III frequently involves a tendon rupture or
muscle tear and often represents years of fibrosis and tendinitis.
Stage I rotator cuff syndrome is found most often in individuals under age 25;
stage II occurs most often in individuals between 25 and 40; stage III occurs mainly in
individuals over age 50 (Quintana). Men develop rotator cuff syndrome twice as often
as women, possibly because of work activities as noted above. The syndrome occurs
independently of race, ethnicity, or geographic location.
DIAGNOSIS
History: A complete medical history, including the individual's occupation and
recreational activities will be taken. A good description of the shoulder pain including
the onset, timing, location, radiation, quality of pain, aggravating and alleviation
factors, presence of associated symptoms, and association with any activities helps to
diagnose rotator cuff syndrome. The individual frequently reports aching pain in the

shoulder or referred pain along the outside upper arm. The pain worsens when the arm
is lifted overhead and at night. Other symptoms may include weakness and reduced
range of motion. The onset of symptoms is often gradual. The first
dysfunction/symptom to arise is pain. When weak, the rotator cuff can no longer
handle the load of raising (abduction) and flexing the arm. Reaching for a glass in the
cupboard
Reaching to switch on a light
Putting on a seatbelt
Washing one's hair
Driving (steering) with the affected arm
Physical exam: Examination of the shoulder begins with a thorough
inspection for any deformities, scars, edema, or decrease in muscle bulk (atrophy).
Next, the entire shoulder joint and all of its muscle groups are palpated for tenderness.
Both active and passive range of motion are determined by rotating the individual’s
arm through different planes, noting any decrease in range of motion and any pain.
The pain may be more intense with certain movements or when pressure is applied; it
can disappear with other movements. There may be a grating, clicking or cracking
sound (crepitus) in the shoulder. Muscle strength testing and neurological testing
should be performed. Special maneuvers during the physical examination (such as the
Neer impingement, Hawkins-Kennedy impingement, drop-arm, apprehension, and
relocation tests) may be helpful. A thorough exam includes evaluation of the cervical
spine along with both arms and shoulders.
Tests: X-rays (Anteroposterior view, axillary view, supraspinatus view) are an
essential component of evaluation to rule out calcium deposits in the joint, and bone
or joint diseases. If symptoms do not improve following 3 to 6 weeks of conservative
therapy, other advanced imaging modalities may prove helpful, especially in
diagnosing suspected rotator cuff tears. MRI detects a wide spectrum of rotator cuff
disease, including degeneration and partial to complete tears. It can also reveal soft
tissue abnormalities, and proves especially valuable in tracking postoperative healing.
Ultrasonography proves useful in diagnosing moderately large rotator cuff tears and
evaluating other cuff disease. Widespread use of arthrography has decreased with the
advent of MRI, but it remains useful in individuals for whom MRI is contraindicated
(e.g., those with a pacemaker, cerebral aneurysm clip, or recent cardiac stent).

Arthrography involves injection of contrast media into the glenohumeral joint
followed by plain x-rays. Observed leakage of contrast material into the subacromial
or subdeltoid spaces following injection indicates a full-thickness rotator cuff tear.
Other diagnostic tests for rotator cuff syndrome are bone scintigraphy and CT scan,
often with contrast media (CT-arthrography). Electromyography (EMG) and nerve
conduction velocity studies (NCVs) may be helpful if neurologic involvement is
suspected.
TREATMENT
During the acute phase of rotator cuff syndrome, conservative treatment
consists of rest and activity modification, ice, and the use of (NSAIDs). The goals are
to decrease inflammation and pain and restore normal shoulder function. Activities
causing the pain should be resumed gradually when pain is gone. Sometimes a
cortisone injection into the space above the rotator cuff tendon (subacromial
corticosteroid injection) helps relieve swelling and inflammation. Application of ice
to the tender area for 15 minutes 3 to 4 times a day also is helpful as is a supervised
program of stretching and strengthening exercises to increase range-of-motion.
Recovery of function should be stressed. An on-going home exercise program is
essential to help prevent recurrence. Surgery may be considered for those individuals
who show no improvement after 3 months of aggressive therapy or who continue to
be bothered by weakness.
Indications for surgery vary but should take into consideration an individual’s
age, type and severity of tear (partial to full-thickness muscle tears), duration of
symptoms, and willingness and ability to comply with postoperative therapy. The
main goals of surgery are improved strength, increased function, and pain relief.
Chronic rotator cuff syndrome with severe impingement may be treated by cutting
into the shoulder and repairing the bone and/or tendon and/or the muscle (arthroscopic
acromioplasty). Rotator cuff surgery is done to repair a torn rotator cuff. Bone spurs
or calcium deposits causing impingement may be removed at the same time. Surgery
must be followed by physical therapy to improve strength and range-of-motion
followed by an on-going home exercise program.
PROGNOSIS

Recovery often depends on the stage of the syndrome and the age of the
individual. Some individuals whose rotator cuff syndrome is caused by repetitive
above-the-shoulder lifting may recover completely if the repetitive work is stopped
and an aggressive, nonsurgical treatment plan (i.e., ice, strengthening, and range-of-
motion exercises) is followed. Success rates with such conservative treatment range
from 33% to 90%, with longer recovery times noted in older individuals (Quintana).
Surgical outcomes often depend on the willingness and ability of an individual to
participate actively in postoperative physical therapy and home exercise. The reported
success rate for surgery to treat torn rotator cuffs is between 77% and 95% ("Shoulder
Rotator"; Quintana). In many individuals who resume overhead work or other activity
that initially caused the problem, recurrent episodes may continue despite appropriate
acute treatment. These individuals need to alter their work or recreational activities.
REHABILITATION
Rotator cuff syndrome represents a chronic shoulder impingement syndrome.
The early goals of rehabilitation for rotator cuff syndrome are to decrease pain and
inflammation and to reduce the stress on the irritated tendon and/or tissues (Morrison,
"Shoulder Impingement"; Rubin). In conjunction with pharmacological management,
individuals are instructed in the use of cold treatments to the shoulder to decrease
inflammation. Reduction of stress to the irritated tissue(s) is often achieved through
education, ergonomic adjustments, and/or work modifications aimed at reducing the
offending activities, which often include repetitive movements or sustained positions
where the elbow is raised above the shoulder level. Stiffness may be prevented by
passive range of motion exercises conducted during supervised rehabilitation and a
home exercise program (Ludewig).
Rehabilitation also aims to reduce the stress on the irritated tendon and/or
tissues by improving strength and flexibility around the shoulder (Morrison,
"Shoulder Impingement"; Rubin). The strengthening is usually aimed at the shoulder
girdle musculature (Morrison, "Non-Operative Treatment"; Morrison, "Shoulder
Impingement"; Rubin). Flexibility exercises vary, based on the physical examination
findings. Some evidence from randomized controlled trials suggests that manual
therapy in conjunction with a program of strengthening and stretching is more
beneficial than strengthening and stretching alone (Bang). Throughout rehabilitation,

exercise intensity and duration should be increased until full functional ability is
regained (Rubin).
While many individuals respond well to the conservative management of
rotator cuff syndrome, surgical intervention may be required.
COMPLICATIONS
The main complication of rotator cuff syndrome occurs when rotator cuff tears
go undiagnosed. Symptoms will persist until the rotator cuff is repaired surgically.
Another complication results from inadequate treatment. If the shoulder is
immobilized in a sling, the individual can develop "frozen shoulder" (adhesive
capsulitis). Conditions such as a rotator cuff tear or impingement syndrome may also
lead to decreased range of motion in the shoulder. An estimated 4% of rotator cuff
ruptures result in joint disease (arthropathy) of the shoulder (Quintana). Proper care,
whether conservative or surgical, and appropriate follow-up lessen the likelihood of
joint disease and other long-term consequences of rotator cuff syndrome.

REFERENCES
Bang, M. D., and G. D. Deyle. "Comparison of Supervised Exercise with and without Manual Physical Therapy for Patients with Shoulder Impingement Syndrome." Orthopedic and Sports Physical Therapy 30 3 (2000): 126-137. National Center for Biotechnology Information. National Library of Medicine.
Fongemie AE, Buss DD, Rolnick SJ. Management of shoulder impingement syndrome and rotator cuff tears.Am Fam Physician. 1998 May 15;57(4):667-74, 680-2.
Ludewig, P. M., and J. D. Borstad. "Effects of a Home Exercise Programme on Shoulder Pain and Functional Status in Construction Workers." Occupational and Environmental Medicine 60 11 (2003): 841-849. National Center for Biotechnology Information. National Library of Medicine.
Mercier, L. R. "Rotator Cuff Syndrome." Ferri's Clinical Advisor 2009. Ed. Fred Ferri. Philadelphia: Mosby, Inc., 2009
Morrison, D. S., A. D. Frogameni, and P. Woodworth. "Non-Operative Treatment of Subacromial Impingement Syndrome." Journal of Bone and Joint Surgery 79 5 (1997): 732-737. National Center for Biotechnology Information. National Library of Medicine.
Morrison, D. S., B. S. Greenbaum, and A. Einhorn. "Shoulder Impingement." Orthopedic Clinics of North America 31 2 (2000): 285-293. National Center for Biotechnology Information. National Library of Medicine.
Quintana, Eileen C., and Richard Sinert. "Rotator Cuff Injuries." eMedicine. Eds. Joseph A. Salomone, et al. Medscape. <http://emedicine.com/emerg/topic512.htm>.
Roy, Andre. "Rotator Cuff Disease." eMedicine. Eds. Robert E. Windsor, et al. Medscape. <http//emedicine.com/pmr/topic125.htm>.
Rubin, B. D., and W. B. Kibler. "Fundamental Principles of Shoulder Rehabilitation: Conservative to Postoperative Management." Arthroscopy 18 9 Suppl 2 (2002): 29-39. National Center for Biotechnology Information. National Library of Medicine.
"Shoulder Rotator Cuff Disease." Orthopaedic Associates of Portland. <http://www.orthoassociates.com/shoulderRCD.htm>.