Embed Size (px)
DESCRIPTION
Role of the multidisciplinary team in the diagnosis and treatment of hepatocellular carcinoma
Citation preview

173
Review
www.expert-reviews.com ISSN 1747-4124© 2012 Expert Reviews Ltd10.1586/EGH.11.105
Clinical overview of hepatocellular carcinomaEpidemiology & etiologic risk factorsWorldwide, hepatocellular carcinoma (HCC) is responsible for approximately 600,000 deaths each year, making it the sixth most common cause of cancer-related death [1]. In the USA alone, there were roughly 24,000 new cases of HCC in 2010, with a male-to-female ratio of 2.5:1, as well as approximately 17,000 HCC-related deaths [2]. In general, HCC is associ-ated with a poor prognosis, particularly because many patients also suffer from chronic infec-tion with hepatitis B virus (HBV) or hepatitis C virus (HCV), and therefore almost always have underlying liver cirrhosis [3].
The incidence of HCC varies widely by region. Some countries, such as Mongolia, South Korea, Congo and Japan, have a high incidence (>50 per 100,000 population per year), whereas Australia, New Zealand and countries in north-ern Europe and North America have a much lower incidence [4]. Developing countries have shown marked increases in yearly incidence, including a remarkable jump of 55% in China [5]. In Europe, the age-standardized incidence
was higher in southern than in northern coun-tries, with the incidence in southern Europe con-tinuing to increase [6]. This increasing incidence has been ascribed to increases in hepatitis B and C infection and a rise in alcohol intake.
In addition to viral hepatitis, risk factors for HCC include fatty liver, ethanol abuse and exposure to aflatoxins [7–12]. The most com-mon risk factor for HCC is cirrhosis of the liver, which has been implicated as the underlying cause in 60–80% of cases [13]. Viral hepatitis is present in approximately 75% of patients, and is HBV-related in approximately half and HCV-related in approximately a third of patients worldwide. Chronic alcohol use appears to be a cofactor in the development of HCC in many patients, as well as a primary cause in some. Geographic variations in the prevailing etiol-ogy have been observed, with HBV-associated HCC predominant in China, South Korea and African countries; and HCV- and alcohol-asso-ciated HCC predominant in Japan, Europe and North America [14–16].
Patients diagnosed with an advanced stage of HCC have a grave prognosis. Earlier diagnosis improves the chances of candidacy for curative
Robert G Gish*1, Riccardo Lencioni2, Adrian M Di Bisceglie3
Jean-Luc Raoul4 and Vincenzo Mazzaferro5
1Center for Hepatobiliary Disease, University of California, San Diego, 200 West Arbor Drive, San Diego, CA 92103-8413, USA 2Division of Diagnostic Imaging and Intervention, Pisa University Hospital and School of Medicine, Pisa, Italy 3Division of Gastroenterology and Hepatology, Department of Internal Medicine, St Louis University School of Medicine, St Louis, MO, USA 4Institut Paoli-Calmettes, Federation Nationale des Centres de Lutte Contre le Cancer (FNCLC), Marseille, France 5National Cancer Institute, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Foundation, Milan, Italy *Author for correspondence: Fax: +1 619 543 2766 [email protected]
It has long been appreciated that hepatocellular carcinoma (HCC) is a complex disease. HCC is typically preceded by liver cirrhosis, which is itself caused by various types of hepatitis of both viral and nonviral etiologies. Thus, the treatment of patients with HCC requires multiple healthcare professionals, including hepatologists, medical oncologists, surgical oncologists, transplantation surgeons, diagnostic radiologists, pathologists, nurses, nurse practitioners and interventional radiologists. These specialists should meet regularly to review patients’ progress, ensure that treatments are individualized for each patient and agree on next steps. We review case presentations provided by the authors to illustrate the benefits and advantages of the multidisciplinary team matrix in the management of patients with HCC, including the effects of this treatment technique on patient outcome, survival and quality of life.
Keywords: hepatocellular carcinoma • hepatologist • interventional radiologist • medical oncologist • multidisciplinary team • natural history • outcomes • surgical oncologist • targeted therapy • treatment
Role of the multidisciplinary team in the diagnosis and treatment of hepatocellular carcinomaExpert Rev. Gastroenterol. Hepatol. 6(2), 173–185 (2012)
For reprint orders, please contact [email protected]

Expert Rev. Gastroenterol. Hepatol. 6(2), (2012)174
Review
treatment, and may result in 5-year survival rates as high as 70%. This observation underscores the importance of early detection, accurate staging and expeditious initiation of treatment in order to optimize liver function to the greatest extent possible, as well as reduce the odds of disease progression and mortality [17]. An under-standing of the most likely etiology of HCC in a particular patient may guide therapeutic decisions and, in fact, may shape the con-stitution of the medical team caring for that patient. Nevertheless, despite the efficacy of curative therapies, HCC has high recurrence rates, except in selected patients who undergo liver transplantation.
Introduction to the multidisciplinary team approach in HCCTo optimize care and to improve quality of life (QoL) and clini-cal outcomes, patients with advanced HCC are best managed by a multidisciplinary team (MDT) composed of specialists with specific roles and functions [18–20]. Ideally, each patient should be treated on an individualized basis, with therapy guided by evidence-based guidelines based on the results of prospective, randomized controlled clinical trials [21,22].
The typical MDT employed for patients with HCC includes a medical oncologist, a hepatologist/gastroenterologist, a surgeon, a diagnostic radiologist and an interventional radiologist (IR), who meet on a regular basis to discuss individual patients and treatment approaches. This multidisciplinary matrix approach has been shown to improve communication among team members with specific skills, thereby improving patient outcomes [23,24]. The MDT allows for a standardized screening procedure and agreed-upon treatment protocols, and helps to coordinate patient care in general. It also promotes the rapid transfer of clinical information among the members of the treatment team, thereby enhancing strong interpersonal working relationships [24,25].
It is important that HCC care be individualized. A coordinated approach is required to achieve optimal outcomes and to ensure that patients are evaluated and treated in a nonhierarchical manner. The team functions best with frequent joint conferences, where all aspects of the treatment plan are discussed within the management matrix [26]. The principal goals of the MDT are to identify those patients who may be eligible for curative options, including liver resection or transplantation, as well as to use ablative techniques and targeted therapies to reduce disease progression, prolong life and improve patient QoL during treatment [20].
The MDT members need to concur on optimal diagnosis and staging and then proceed to a treatment plan [20,27]. A broad range of specialists is required in the identification, diagnosis, treatment and management of patients with HCC. The contribution of each member of the MDT will depend upon the institution, the levels of expertise within the various departments and the disease stage of each patient. In addition to those directly responsible for the treatment of the patient, team members typically include patholo-gists, palliative care physicians, transplant coordinators, nurses, pharmacists, social workers, clinical psychologists and religious counselors [19,24,27].
A single-institution, observational study performed in the USA and published in 2008 found that the use of the MDT paradigm
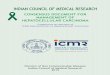
resulted in statistically significant benefits in the treatment of patients with advanced HCC [26]. The number of patients referred for treatment doubled, significantly more patients were seen at an earlier stage of disease (p < 0.001) and the propor-tions of patients receiving curative treatment and palliative care increased significantly, from 6 to 19% and from 31 to 45%, respectively (both p < 0.001). Overall survival also increased significantly following the introduction of the MDT approach (p < 0.001). Thus, the MDT provided dramatic improvements in outcomes, both statistically and clinically, indicating that improved communication within the matrix of professionals with specialized skills led to improved outcomes for patients with advanced HCC (Figure 1).
The hepatologist/gastroenterologistFor many patients with advanced HCC, the hepatologist/gas-troenterologist is the first point of contact with the MDT. The hepatologist/gastroenterologist is responsible for identifying those patients at highest risk for HCC (see updated HCC guidelines of the American Association for the Study of Liver Diseases [AASLD]), for treating the underlying liver disease, for advising patients on steps to take to avoid HCC, for monitoring patients for disease progression, for arranging surveillance plans and for diagnosing HCC, if present. In addition, the hepatologist/gas-troenterologist is responsible for assessing underlying liver func-tion and monitoring treatment complications, including decom-pensation and tolerance to therapy, and for referring patients for potential liver transplantation [28].
Depending on the expertise and experience available at the local institution, the hepatologist/gastroenterologist may treat patients with molecular targeted therapies or consult with the medical oncologist on whether and when to begin treatment with a tyrosine kinase inhibitor (TKI). The hepatologist/gastroenterologist may also enroll patients with unresectable HCC into clinical trials [29].
The medical oncologistThe medical oncologist is often responsible for initiating systemic or targeted therapy in patients newly diagnosed with HCC but not eligible for resection or transplant, as well as for initiating adjuvant chemotherapy in patients who have undergone resection. The medical oncologist is generally familiar with all major classes of chemotherapeutic agents and is generally knowledgeable about large ongoing clinical trials. Many large multicenter clinical trials have been conducted worldwide, using most of the larger classes of chemotherapeutic agents, either singly or in combination, for the treatment of patients with HCC [1,20,26,29–31]. Together with the hepatologist, the medical oncologist will also screen patients for inclusion in new clinical trials.
The use of AFP concentration in the screening and surveillance of HCC is controversial and has been removed from guidelines, such as those of the AASLD. AFP concentration, however, remains clinically useful and is therefore part of the work-up and manage-ment of HCC. AFP and supplementary biomarkers, such as the Lens culinaris agglutinin-reactive fraction of a-fetoprotein (AFP-L3) and des-g-carboxy prothrombin, are utilized to help determine
Gish, Lencioni, Di Bisceglie, Raoul & Mazzaferro

www.expert-reviews.com 175
Review
the presence of vascular invasion, risk of postsurgical recurrence and risk of HCC recurrence after liver transplantation [32–36].
Systemic therapy in advanced HCCSystemic chemotherapy has been the backbone of treatment for patients with advanced HCC. Although doxorubicin has long been the most utilized single agent for this disorder, high-quality data from large randomized trials have never been available, and the outcomes of treatment with doxorubicin have been found to be suboptimal, with substantial toxicity and dose-limiting issues in patients with decompensated liver disease, resulting in
poor anti-tumor activity and minimal effect on overall survival [28]. In searching for more effective systemic agents, researchers have focused on the molecular pathogenesis of HCC, identi-fying angiogenic pathways that, when blocked, often result in tumor necrosis. Many of these new anti-angiogenic agents may be applicable to HCC because of the highly vascular nature of these tumors. The therapeutic advantages of these anti-angio-genic agents are based on the pharmacodynamics of growth fac-tors involved in tumor vascularization. These therapy-targeted cytokines include VEGF, PDGF, TGF-b, EGF, HGF, IGF and FGF, as well as their respective receptors. Manipulation of these
1. Hepatologist/ gastroenterologist
• Expert opinion on optimal Tx choices• Guide systemic Tx• Tx cirrhosis and EtOH addiction• Cryoablation• Consults
2. Medical oncologist
• Establishes adjuvant chemotherapy regimen• Suggests new Tx protocols
3. Surgical oncologist
• Suggests early-stage resection candidates• Performs resections
4. Transplantation surgeon
• Suggests candidates for liver transplants• Performs necessary transplants
5. Diagnostic radiologist
• Ultrasound• CT, MRI and PET scans• Assess and evaluate Tx effectiveness
7. Radiation oncologist
• External beam• Local ablative Tx• Conformal radiation Tx• Charged particle Tx• Microwave ablation
8. Primary care
• Screens for underlying liver disease• Refers to hepatologist/ gastroenterologist• Tx comorbidities (e.g., HTN, CHF, DM2)
9. Other participants
• Hospitalist and intensivist• Palliative care physician• Endocrinologist• Pathologist• Oncology nurse
6. Interventional radiologist
• Directs MRI and CT scans• Directs Tx• Establishes staging• TACE• RFA• PEI
Figure 1. Illustration showing members of the multidisciplinary team surrounding the hepatocellular carcinoma patient. CHF: Congestive heart failure; CT: Computed tomography; DM2: Type 2 diabetes mellitus; EtOH: Ethanol; HCC: Hepatocellular carcinoma; HTN: Hypertension; PEI: Percutaneous ethanol injection; RFA: Radiofrequency ablation; TACE: Transcatheter arterial chemoembolization; Tx: Treatment.
Role of the multidisciplinary team in diagnosis & treatment of hepatocellular carcinoma

Expert Rev. Gastroenterol. Hepatol. 6(2), (2012)176
Review
factors has formed the foundation for the development of new sys-temic therapeutic agents, which have been shown to halt tumor growth [37].
Sorafenib in HCCIn addition to blockers of tumor angiogenesis, the multi-targeted TKIs have emerged as an important new class of chemotherapeu-tic agents. To date, sorafenib is the only TKI approved by the US FDA for the treatment of patients with advanced HCC [38–44]. Sorafenib functions both as an anti-angiogenic agent and as an inhibitor of tumor-cell proliferation, and may also directly induce cell death via apoptosis. This triple activity has made sorafenib useful in the treatment of HCC. Two important Phase III clinical trials of sorafenib in HCC were the SHARP and the Sorafenib AP trials [39,40]. In the SHARP trial, median overall survival (10.7 vs 7.9 months; p < 0.001) and median time to radiologic pro-gression (5.5 vs 2.8 months; p < 0.001) were significantly longer in the sorafenib than in the placebo group [39]. Similarly, in the Sorafenib AP trial, median overall survival (6.5 vs 4.2 months; p = 0.014) and median time to progression (2.8 vs 1.4 months; p = 0.005) were significantly longer in the sorafenib than in the placebo group [40]. Case presentations illustrating the use of sorafenib in selected patients with HCC have been included in this review.
Case presentation 1A patient with newly diagnosed HCC & a Child–Pugh designation of class A as a candidate for transarterial chemoembolizationA 58-year-old Caucasian man with long-standing chronic HCV infection and liver cirrhosis, and comorbidities of Type 2 diabetes mellitus and peripheral vascular disease, was diagnosed with HCC during an annual routine check-up. He was found to have an inter-mediate multinodular tumor 5.0 cm in diameter and located in liver segment six, as well as satellite lesions 1.0–3.0 cm in diameter just anterior to the main lesion without metastatic disease in the chest or abdomen and no vascular invasion of any of the portal vessels (Figure 2).
The patient was asymptomatic, with an Eastern Cooperative Oncology Group performance status of 0, lack of macrovascular invasion (MVI) or extrahepatic spread (EHS), a Model for End-Stage Liver Disease score of 6, a Child–Pugh designation of class A and Barcelona Clinic Liver Cancer (BCLC) stage B disease. He did not have any ascites. Laboratory tests showed a serum total bilirubin concentration of 1.8 mg/dl, a direct bilirubin concentra-tion of 1.0 mg/dl, a serum albumin concentration of 3.2 g/dl, an AFP concentration of 1100 ng/ml and an international normalized ratio of 1.3. The MDT determined that this patient had unresect-able HCC and was a candidate for transarterial chemoemboliza-tion with doxorubicin-containing beads. A 6-month follow-up four-phase MRI of the liver revealed a primary tumor response, with no areas of hypervascularity and a small hypoenhancing defect where the previous tumor had been, and with no evidence of metastasis or additional tumor nodes in the liver. Laboratory testing showed that his serum AFP concentration had decreased to
65 ng/ml. He continues to be stable and is undergoing surveillance and laboratory monitoring at frequent intervals.
Despite the good response, however, the transplant surgeon and transplant hepatologist, after consulting with a cardiologist, decided not to list this patient for liver transplantation owing to the presence of a high-grade lesion in his left anterior descending artery on cardiac catheterization and an ejection fraction of 45%, indicating substantial left ventricular dysfunction.
The surgical oncologistThe role of the surgical oncologist or transplant surgeon is to evaluate whether a tumor is resectable and to remove any primary tumor. Surgical excision is the method of choice in the treatment of stage I HCC provided that the patient has no, or minimal, portal hypertension [45]. Owing to underlying liver disease and the potential for liver failure after surgery combined with general anesthesia, the risks involved in major hepatectomy are high, with mortality rates of 5–10% or greater, depending on the severity of portal hypertension and liver dysfunction. Patients with either cirrhotic or noncirrhotic liver disease who are classified as Child–Pugh class A may have a better outcome when minimally invasive ablative techniques are employed instead of open resection [46].
Although open excision is the most reliable approach to remov-ing a primary tumor, laparoscopic procedures may produce com-parable outcomes. Laparoscopic approaches using surgical resec-tion of a dominant tumor and radiofrequency ablation (RFA), percutaneous RFA or percutaneous ethanol injection of additional smaller lesions have been used successfully in selected patients [47].
The transplantation surgeonThe role of the transplantation surgeon, who is frequently the same person as the surgical oncologist, is to determine, along with trans-plant hepatologists, whether liver transplantation is the best option for cancer-free patient survival. Liver transplantation has shown excellent survival outcomes in selected patients with HCC. The guidelines of the United Network for Organ Sharing for transplan-tation in HCC are based on the Milan criteria, which recommend liver transplant in patients with one lesion ≤5 cm and in those with three or fewer lesions, each ≤3 cm in diameter. In these patients, liver transplantation has resulted in a 5-year survival rate of >70% and a recurrence rate of <15% [48]. Other, newer methods for staging HCC to select patients for the best outcomes are being evaluated [49–56].
A recent study assessed surgical decision-making in the choice between liver transplantation, liver resection or RFA as initial therapy for patients with early HCC [57]. Surgeons with an inter-est in liver surgery completed a web-based survey on ten case scenarios. Surgeons who did and did not specialize in liver trans-plantation showed significantly different recommendations, with clinical factors – including tumor size and number, type of resec-tion and platelet count – having significant effects on treatment choices. After adjusting for these clinical factors, nontransplanta-tion surgeons were significantly more likely to choose resection than transplantation. However, when the weight of each clinical factor was allowed to vary by specialty, the residual independent effect of specialty on the choice of resection or transplantation
Gish, Lencioni, Di Bisceglie, Raoul & Mazzaferro

www.expert-reviews.com 177
Review
became negligible, indicating that certain clinical factors are weighed differently by surgeons in different specialties.
Owing to the high risk of recurrence following resection in patients with HCC and cirrhosis as a comorbid condition, liver transplan-tation may be a superior modality for certain patients because it treats both the HCC and the underlying liver disease, with 5-year recurrence rates of 70–80% for resection versus 10–20% for trans-plantation [17]. Some studies have suggested, however, that the two modalities are comparable, with 5-year survival rates ranging from 50 to 70% [48,58]. In addition, treatment with sorafenib may reduce tumor burden sufficiently to allow resection or transplantation [59].
The diagnostic radiologistThe role of the diagnostic radiologist, who is a specialist in abdom-inal imaging, is to perform and/or supervise imaging methods that establish a definitive diagnosis and, once HCC is diagnosed, to help direct surveillance and the staging of disease and its man-agement [20,27]. Imaging modalities provided by the diagnostic radiologist include ultrasound, contrast ultrasound, computed tomography (CT) scanning, MRI and PET scanning, although PET scanning has no role in the staging of HCC according to international guidelines. The diagnostic radiologist also performs follow-up CT and MRI scans to evaluate the effectiveness of treat-ments recommended by the other members of the MDT [49,60].
The interventional radiologistThe IR is especially important in the care of patients with early- to intermediate-stage HCC who are not candidates for surgical resection. The IR may also work to downstage patients for surgical resection or liver transplantation. The IR is occasionally involved in
the diagnosis of HCC by obtaining tumor tissue samples for inter-pretation and evaluation by the pathologist, as well as by directing imaging protocols and interpreting their results, thus assessing the full scope of HCC pathology. Following the establishment of a definitive diagnosis of HCC and its proper staging, the IR inter-acts with other members of the MDT in selecting and performing other ablative treatments [20,21,49,61,62]. For example, the IR performs localized thermo- or chemo-ablative procedures recommended for patients with small HCCs who are not candidates for resection or liver transplantation. In ablative treatments, tumor cells are destroyed, either by increasing the temperature (e.g., RFA, micro-wave ablation [MwA] or laser targeting), decreasing the tempera-ture (i.e., cryotherapy) or by injecting chemicals directly into the tumor (e.g., chemotherapy and soybean oil, chemotherapy-laden beads, ethanol or acetic acid) [20,26,27]. If follow-up scans reveal new lesions or recurrence of the original lesion, thermal ablation or a second attempt at bead embolization could be considered.
Radiofrequency ablationIn RFA, the deposition of electromagnetic energy is used to ther-mally ablate hepatic tumor tissue, resulting in coagulated necro-sis. Depending on the type of electrode used, ablation diameters between 5 and 7 cm are possible [63–66]. RFA is effective and well tolerated and can be performed on an outpatient basis.
Microwave ablationMwA is similar to RFA, with microwave energy used to thermally destroy tumor tissue [67–69]. MwA also results in necrosis spheres approximately 7 cm in diameter, is effective and well tolerated, and can be performed on an outpatient basis. The benefits of MwA
Tumor lesionin liver
segment 6
ASatellite
tumor lesionsSatellite
tumor lesions
B
Figure 2. Computed tomography scans of the liver of patient number 1. (A) Intermediate nodular tumor, 5 cm in diameter, in liver segment 6 and a satellite lesion (arrows). (B) A second satellite lesion (arrow).
Role of the multidisciplinary team in diagnosis & treatment of hepatocellular carcinoma

Expert Rev. Gastroenterol. Hepatol. 6(2), (2012)178
Review
include heating of the tumor much more rapidly than with RFA and the lack of a ‘heat sink’ effect from nearby vessels. This method has expanded the application of thermal ablation, as well as reducing cost by decreasing time in the operating room or intervention room.
Percutaneous ethanol injection Percutaneous ethanol injection relies upon coagulation necrosis of tumors by cellular dehydration. It has been shown to be effective in 90–100% of HCC tumors <2 cm in diameter and in 50% of tumors between 3 and 5 cm in diameter [66,70]. This procedure, however, is rarely performed in the USA.
Transcatheter arterial chemoembolization & transarterial bead embolizationTranscatheter arterial chemoembolization (TACE) and transarte-rial bead embolization are techniques that employ body imaging to locate arterial supplies to the tumor. This is followed by injec-tion of thrombotic agents (TACE) or beads loaded with chemo-therapeutic agents or yttrium-90 (Y90; transarterial radiotherapy), which block blood flow to the tumor and result in tissue necrosis. These methods have been used extensively in patients with HCC, especially those who are not candidates for surgical resection, delaying HCC progression until liver donors become available for transplantation [65,71]. Because arterial and thermoablative techniques may promote angiogenesis, TKIs, such as sorafenib, are being assessed in clinical trials to determine if they can retard the metastatic sequelae of TACE-induced angiogenesis.
The radiation oncologistBecause the liver has a very low tolerance to irradiation, radia-tion therapy has limited use in the treatment of HCC. Moreover, radiation-induced liver disease is often a problem, especially in patients with underlying liver diseases, such as hepatitis B [72]. The radiation oncologist, however, may still be involved with several treatment modalities for patients with HCC, particularly those who are not candidates for surgical intervention [1,72].
Transarterial radiotherapyThis treatment modality consists of radiation, delivered to the tumor mass through the hepatic artery or via extrahepatic collateral arteries [73]. New combinations of transarterial radiotherapy with TKIs are evolving because the latter may promote angiogenesis, and sorafenib has been shown to moderate angiogenesis and resultant metastases.
RadioisotopesRadiation can be delivered to tumors by direct injection of radio-isotopes, particularly Y90, incorporated into stable glass micro-spheres [74] and iodine-131, attached to ferritin antibodies or lipi-odol and injected through the hepatic artery. In a study involving 40 patients with HCC who were treated with iodine-131 lipiodol, the response rate was 48% and the median duration of response was 18 months, with 1-year and 2-year survival rates of 90 and 60%, respectively [75]. In many centers, Y90 is delivered by an IR, not by a radiation oncologist, thereby further emphasizing the multidisciplinary nature of HCC treatment.
Other treatment modalities include external-beam radiation, laser ablation, microwave coagulation therapy, palliative radiation therapy, conformal radiation therapy, charged particle therapy and brachytherapy. If recurrences are observed in a metastatic location, such as the spinal cord, stereotactic external beam radiation could be considered for primary treatment or symptom management.
The hepatology, transplantation & oncology nurse, physician assistant & nurse practitionerThe oncology nurse or nurse practitioner is responsible for ensur-ing patient compliance with all therapy protocols, for noticing any adverse reactions to drugs and for helping to manage the side effects of drug treatment. The oncology nurse or nurse prac-titioner may be the first person to notice any untoward reactions patients may have to complex protocols. Their participation in the MDT is invaluable in helping patients and their families cope with the many stresses encountered in surgery, radiation therapy and chemotherapy. The nursing staff plays an important role in the maintenance of QoL for all patients with HCC [1,19,24].
The primary care physician/internistIn the strictest sense, the primary care physician (PCP) is not con-sidered integral to the MDT. Rather, the principal role of the PCP is the identification of elevated liver enzymes, resulting in the early detection of chronic liver disease, the diagnosis of its underlying cause (e.g., HBV, HCV and cirrhosis) and the referral of patients to a liver specialist for treatment and to assess the risk of HCC. Patients at greatest risk for HCC (i.e., those with cirrhosis, accord-ing to AASLD guidelines) should undergo diligent surveillance. Thus, close interaction between the PCP and specialist physicians is important [61].
PCPs are likely to see patients following hospital discharge after the treatment of complications of cirrhosis or treatment of HCC, making them ideally positioned to assess the results of treatment and to manage side effects in patients treated for any underlying liver disease. In addition, the PCP is available to diagnose and treat any unrelated comorbidities, such as diabetes, hypertension and chronic heart failure, as well as to treat any adverse reactions arising from other treatment modalities, such as paresthesias, painful erythema, desquamation, ulcers and blistering [61]. Thus, while not integral to the MDT, the PCP may play an essential role in the post-treatment phase [18].
Other participants in the MDTThe pathologistThe pathologist characterizes the properties and histologic architecture of HCC tumor tissue removed during resection or transplantation or obtained at biopsy. The pathologist is also responsible for determining the stage of progression of HCC and for assaying biomarkers in this tumor type that can guide the medical oncologist in choosing optimal treatment options [1,76,77].
The hospital-based physicianThe hospital-based physician provides up-to-date information on emerging modalities in the management of HCC and acts as
Gish, Lencioni, Di Bisceglie, Raoul & Mazzaferro

www.expert-reviews.com 179
Review
a vital contact point for inpatients. This physician may suggest alternative treatment strategies and may help improve patient QoL, thus prolonging survival.
The palliative care physicianThe palliative care physician manages pain in terminally ill patients. In patients with HCC, pain is generally caused by metas-tases to bone, brain, lymph nodes and other sites. Pain may be alleviated by radiation therapy or pharmacotherapy [78].
The endocrinologistThe endocrinologist is responsible for monitoring patients with HCC and comorbid conditions, such as diabetes mellitus, as well as managing any sequelae resulting from treatment modalities that may alter the balance of the endocrine system, such as thyroid, adrenal and pituitary functions, imbalances that may also affect the treatment of HCC.
The following case presentations will help to illustrate the value of the MDT in the treatment of patients with HCC and related liver comorbidities.
Case presentation 2A patient with recurrent HCC as a candidate for transarterial chemoembolization & subsequently treated with sorafenibA 60-year-old Caucasian woman, who contracted HCV from a needle-stick injury 30 years earlier and later developed liver cirrho-sis, presented with a chief complaint of right upper-quadrant pain during a routine examination. Radiologic examination showed a single 4-cm tumor in the right lobe of her liver (Figure 3). There was no evidence of EHS and she had a normal portal vein and normal bilirubin concentrations. A transjugular portal venous pressure measurement showed a gradient of 6 mmHg. Liver func-tion tests revealed an albumin concentration of 3.4 g/dl, a bili-rubin concentration of 1.2 mg/dl, and an international normal-ized ratio of 1.0. She was diagnosed with a BCLC stage A HCC. Her Model for End-Stage Liver Disease score was 6, her Eastern Cooperative Oncology Group performance status was 0, her AFP was 600 ng/ml and her liver function was classified as Child–Pugh class A-6 owing to the presence of very mild encephalopathy.
The MDT recommended resection of the single tumor. Pathologic evaluation of the tissue sample showed evidence of MVI, making her at higher risk for HCC recurrence. Her postoperative AFP concentration was 300 ng/ml.
A 12-month follow-up examination showed five additional lesions, measuring between 1.0 and 3.5 cm in diameter, in the right lobe of her liver (segment 5). Laboratory tests revealed no EHS or portal vein thrombosis, and her AFP concentration was 550 ng/ml. She underwent two sessions of TACE with lipiodol, doxorubicin, cisplatin and mitomycin at 8-week intervals with particle embo-lization. A follow-up CT scan after completion of two treatment cycles demonstrated disease progression (Figure 3).
The MDT decided that treatment with sorafenib was indicated. The patient was treated with 400-mg sorafenib (two tablets) both in the morning and evening, and developed a grade 3 hand–foot
syndrome (HFS) at 3 weeks. She underwent intensive therapy with emoliants, and her dose of sorafenib was reduced to 200 mg per orem (p.o.) twice per day (b.i.d.) without dose interruption. Within 2 weeks her HFS had been reduced to grade 1 and her dose of sorafenib was increased to 400 mg in the morning and a 200-mg dose in the evening. Three weeks later, with her HFS remain-ing at grade 1, her dose of sorafenib was increased to 400 mg p.o. b.i.d. The patient responded well to this treatment regimen, with follow-up four-phase MRI examinations at 3 and 6 months show-ing a 20% decrease in arterial vascularization and no evidence of further disease progression. Moreover, chest CT, bone scans and abdominal imaging showed no evidence of metastatic disease.
Case presentation 3A patient diagnosed with BCLC stage B HCC & progressive disease following transarterial chemoembolization as a candidate for sorafenibA 52-year-old Asian male with documented HBV infection, who was receiving antiviral therapy for 5 years and was HBV DNA negative, was regarded as at high risk for HCC and underwent regular ultrasound surveillance. Approximately 18 months after his last ultrasound test, he presented with multinodular HCC, consisting of three tumors, 3.0–5.0 cm in diameter, in the right lobe of his liver, but no evidence of metastases on four-phase CT (Figure 4). He was diagnosed with BCLC stage B HCC. His serum AFP concentration was 700 ng/ml.
The MDT determined that the proper intervention for this patient was three sessions of TACE at 8-week intervals. Subsequent four-phase CT scans showed that his HCC had progressed, the number of nodes had increased and there were metastases to the lung (Figure 4). He was classified as having unresectable HCC BCLC stage C disease. Laboratory analysis revealed an ALT of 51 U/l, an AST of 38 U/l and an AFP of 900 ng/ml.
The MDT agreed to treat with sorafenib 400 mg p.o. b.i.d. to attempt to retard disease progression. The patient responded well to this treatment regimen, and at 3-month follow-up four-phase CT examination demonstrated no disease progression, although extrahepatic disease was present, with a lymph node metastasis in the portal region of the liver. The patient’s phosphorus concen-tration was low (2.0 mg/dl) owing to sorafenib-induced diarrhea that was minimally controlled with imodium (diphenoxylate). Diarrhea, however, markedly worsened following oral phospho-rus supplementation. Sorafenib had to be discontinued when the patient developed left ventricular dysfunction attributed to the hypophosphatemia.
Case presentation 4A patient with newly diagnosed, unresectable HCC & a Child–Pugh designation of class B as a candidate for sorafenibA 55-year-old, actively employed Caucasian man was diagnosed with multinodular, infiltrative, unresectable HCC with MVI, categorized as BCLC stage C disease (Figure 5).
Based on the lack of a surgical option and the presence of BCLC stage C disease, the MDT determined that this patient
Role of the multidisciplinary team in diagnosis & treatment of hepatocellular carcinoma

Expert Rev. Gastroenterol. Hepatol. 6(2), (2012)180
Review
was a candidate for sorafenib therapy. Following 6 months of treatment with sorafenib 400 mg b.i.d., this patient showed slight improvement with regard to MVI in the main portal vein. He had slight ascites, a serum bilirubin concentration of 1.5 mg/dl, an albumin concentration of 3.0 g/dl and an AFP concentration of 940 ng/ml. He was followed closely, undergo-ing frequent four-phase MRI and ultrasound surveillance of the liver to determine whether any metastases or additional nodes had developed.
DiscussionHCC is an aggressive tumor associated with poor prognosis if left untreated [101]. The median survival of patients with advanced untreated HCC is 5–8 months and the 5-year survival rate is approximately 3% [28]. Employment of the MDT para-digm has been shown to provide important advantages in the treatment and management of patients with HCC [24–26,79]. For example, 90% of responders to a survey in the UK reported that management with an MDT improved clinical decision-making,
MultinodularHCC
MultinodularHCC
Diffuse,recurrent HCC
Diseaseprogression
and new tumors
Progression ofmultinodular
HCC
Figure 3. Computed tomography scans of the liver of patient number 2. (A & B) Recurrence of HCC in the right lobe of the liver after resection of a single HCC lesion 4 cm in diameter. (C & D) Progression of HCC after two sessions of transcatheter arterial chemoembolization with lipiodol. HCC: Hepatocellular carcinoma.
Gish, Lencioni, Di Bisceglie, Raoul & Mazzaferro

www.expert-reviews.com 181
Review
New tumorlesion
Lung metastases
Tumorlesions
Tumorprogression
Figure 4. Computed tomography scans of the liver and lungs of patient number 3. (A & B) Multinodular lesions (arrows) before TACE. (B) Progression of hepatocellular carcinoma (arrows) after three sessions of TACE with lipiodol. (C) Development of new hepatocellular carcinoma lesion (arrow) after TACE. (D) Development of lung metastases (arrows) after TACE. TACE: Transcatheter arterial chemoembolization.
provided better coordination of patient care, improved patient QoL and improved overall treatment outcomes [28].
Incorporation of the MDT matrix into the management plan for patients with HCC is important – particularly for those who are not candidates for resection or transplantation – to gain a broad, multispecialist perspective of each patient, to assess all available treatment options and provide access to new treat-ment options, to monitor the progress of therapy, to mitigate the potential for adverse effects and to address any side effects that do occur [22]. Treatment with sorafenib has been shown to be effective in many of these patients [39,40], and other agents and therapies for HCC are currently being evaluated [79,80]. Integrating sorafenib treatment into an MDT approach, when
indicated, may benefit patient outcomes, including survival and QoL.
As in any group of individuals, conflicts may arise regard-ing diagnosis, patient management, treatment and many other aspects involved in treating patients with a complex disease such as HCC. Personal conflicts among professionals and egotism may arise. Medical centers should be aware of potential prob-lems in setting up MDTs to deal with patients. Members of the team should get along well with each other, but not to the extent where all members automatically accede to the views of the most senior and/or prestigious team member. If conflicts arise among team members over patient care, other profession-als should be brought in to resolve these conflicts, even if it
Role of the multidisciplinary team in diagnosis & treatment of hepatocellular carcinoma

Expert Rev. Gastroenterol. Hepatol. 6(2), (2012)182
Review
Key issues
• For optimal care, patients with hepatocellular carcinoma (HCC) should be managed by a multidisciplinary team (MDT) of specialists. A coordinated approach is required to ensure optimal outcomes. The MDT should include the primary care physician, a hepatologist, a medical oncologist, an interventional oncologist, a surgeon and a radiation oncologist working as a finely tuned unit.
• Surgeons can assess, with hepatologists and the HCC integrated team, whether patients are eligible for liver resection or transplant.
• Diagnostic radiologists and interventional radiologists can provide important direction to guide patient care.
• Oncologists, hepatologists and interventional radiologists can provide expert opinion on the best choices of therapy.
• Hepatologists and oncologists can guide the use of newer systemic agents and help manage adverse effects associated with these agents.
• Primary care physicians and other providers play an important role, including nurses, nurse practitioners and physician assistants, because they are often the providers who monitor the patient and assess the impact of the course of therapy prescribed by the MDT.
• Incorporation of the MDT matrix into the management plan for patients with HCC is important now that effective, targeted drug treatments are available – particularly for those patients who are not candidates for resection or transplantation – to monitor the progress of therapy, mitigate the potential for adverse effects and address any side effects that do occur.
means bringing in professionals from outside the institution. Patient advocates should be included in all teams. This is espe-cially true for a complex disease such as HCC, where the costs of treatment may become prohibitive. Medical centers should therefore establish protocols for dealing with MDTs, including, if necessary, the submission of details about a patient to more than one team simultaneously.
Expert commentary & five-year viewEvidence to date supports use of the MDT matrix in the manage-ment of patients with HCC. The MDT approach has been shown – both clinically and in observational studies – to improve commu-nication among team members with specific skills, thereby leading to significantly improved outcomes for patients [23,24]. The MDT
approach has many benefits. It provides a multisource environ-ment within which participants are able to exchange ideas and share their collective consultative findings. It also allows for standardized screening procedures, alignment with treatment protocols and coor-dination of patient care. Finally, the MDT provides an infrastruc-ture for the rapid transfer of clinical information among members of the treatment team, which, in turn, contributes to optimization of care. Principles designed to enhance the benefits to patients of the MDT approach in general have recently been described [81]. The closely coordinated and integrated participation of the MDT in the care of patients with HCC has resulted in earlier diagnosis, increased referrals for cancer treatment and increases in the pro-portion of patients receiving curative and palliative treatments. A multidisciplinary approach helps optimize the treatment of patients
MVI in right portalvein and segmental
branches
InfiltrativeHCC
Tumornodule
Figure 5. Computed tomography scans of the liver of patient number 4 at presentation. (A) An infiltrative HCC (arrow) and (B) a tumor nodule together with macrovascular invasion in the portal vein and segmental branches (arrows). HCC: Hepatocellular carcinoma; MVI: Macrovascular invasion.
Gish, Lencioni, Di Bisceglie, Raoul & Mazzaferro

www.expert-reviews.com 183
Review
ReferencesPapers of special note have been highlighted as:• of interest•• of considerable interest
1 Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 127(12), 2893–2917 (2010).
2 Jemal A, Siegel R, Xu J, Ward E. Cancer statistics. CA Cancer J. Clin. 60(5), 277–300 (2010).
3 Thompson Coon J, Rogers G, Hewson P et al. Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis. Health Technol. Assess. 11(34), 1–206 (2007).
4 Bosch FX, Ribes J, Díaz M, Cléries R. Primary liver cancer: worldwide incidence and trends. Gastroenterology 127(5 Suppl. 1), S5–S16 (2004).
5 Sherman M. Hepatocellular carcinoma: epidemiology, surveillance, and diagnosis. Semin. Liver Dis. 30(1), 3–16 (2010).
6 Capocaccia R, Sant M, Berrino F, Simonetti A, Santi V, Trevisani F. EUROCARE working group. Hepatocellular carcinoma: trends of incidence and survival in Europe and the United States at the end of the 20th century. Am. J. Gastroenterol. 102(8), 1661–1670 (2007).
7 McCracken M, Olsen M, Chen MS Jr et al. Cancer incidence, mortality, and associated risk factors among Asian Americans of Chinese, Filipino, Vietnamese, Korean, and Japanese ethnicities. CA Cancer J. Clin. 57(4), 190–205 (2007).
8 Schütte K, Bornschein J, Malfertheiner P. Hepatocellular carcinoma – epidemiological trends and risk factors. Dig. Dis. 27(2), 80–92 (2009).
9 Amarapurkar D, Han KH, Chan HL, Ueno Y. Asia–Pacific working party on prevention
of hepatocellular carcinoma. Application of surveillance programs for hepatocellular carcinoma in the Asia–Pacific region. J. Gastroenterol. Hepatol. 24(6), 955–961 (2009).
10 Poon D, Anderson BO, Chen LT et al. Asian oncology summit. Management of hepatocellular carcinoma in Asia: consensus statement from the Asian oncology summit 2009. Lancet Oncol. 10(11), 1111–1118 (2009).
11 Shariff MI, Cox IJ, Gomaa AI et al. Hepatocellular carcinoma: current trends in worldwide epidemiology, risk factors, diagnosis and therapeutics. Expert Rev. Gastroenterol. Hepatol. 3(4), 353–367 (2009).
• Reviewdescribingtheepidemiologyandriskfactorsforhepatocellularcarcinoma(HCC),aswellassummarizingdiagnosticandtreatmentmethods.
12 Cabibbo G, Craxì A. Epidemiology, risk factors and surveillance of hepatocellular carcinoma. Eur. Rev. Med. Pharmacol. Sci. 14(4), 352–355 (2010).
13 Tiribelli C, Melato M, Crocè LS, Giarelli L, Okuda K, Ohnishi K. Prevalence of hepatocellular carcinoma and relation to cirrhosis: comparison of two different cities of the world – Trieste, Italy, and Chiba, Japan. Hepatology 10(6), 998–1002 (1989).
14 Colombo M. The role of hepatitis C virus in hepatocellular carcinoma. Recent Results Cancer Res. 154, 337–344 (1998).
15 Andrisani OM, Barnabas S. The transcriptional function of the hepatitis B virus X protein and its role in hepatocarcinogenesis (review). Int. J. Oncol. 15(2), 373–379 (1999).
16 Ho SB, Groessl E, Dollarhide A, Robinson S, Kravetz D, Dieperink E. Management of chronic hepatitis C in veterans: the
potential of integrated care models. Am. J. Gastroenterol. 103(7), 1810–1823 (2008).
17 Llovet JM, Burroughs A, Bruix J. Hepatocellular carcinoma. Lancet 362(9399), 1907–1917 (2003).
18 Schwartz ME, Sung M, Mor E et al. A multidisciplinary approach to hepatocellular carcinoma in patients with cirrhosis. J. Am. Coll. Surg. 180(5), 596–603 (1995).
19 Van Cleave J, Devine P, Odom-Ball P. Multidisciplinary care of hepatocellular carcinoma. Cancer Pract. 7(6), 302–308 (1999).
20 Rilling WS, Drooz A. Multidisciplinary management of hepatocellular carcinoma. J. Vasc. Interv. Radiol. 13(9 Pt 2), S259–S263 (2002).
21 Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects. Semin. Liver Dis. 30(1), 61–74 (2010).
22 Gish RG, Marrero JA, Benson AB. A multidisciplinary approach to the management of hepatocellular carcinoma. Gastroenterol. Hepatol. (NY) 6(3 Suppl. 6), 1–16 (2010).
• ReviewofmultidisciplinarymanagementofpatientswithHCC.
23 Chan AC, Poon RT, Ng KK, Lo CM, Fan ST, Wong J. Changing paradigm in the management of hepatocellular carcinoma improves the survival benefit of early detection by screening. Ann. Surg. 247(4), 666–673 (2008).
24 Taylor C, Munro AJ, Glynne-Jones R et al. Multidisciplinary team working in cancer: what is the evidence? BMJ 340, c951 (2010).
25 Fennell ML, Das IP, Clauser S, Petrelli N, Salner A. The organization of multidisciplinary care teams: modeling internal and external influences on cancer
with HCC and is particularly important when anticancer therapy is coupled with the treatment of underlying liver disease.
Prospective studies are warranted to definitively establish this modality as a gold standard of care, after which incorporation into treatment guidelines would be appropriate.
Financial & competing interests disclosureRG Gish has consultancy and investigator relationships with Bayer HealthCare Pharmaceuticals and Onyx Pharmaceuticals, Inc. As of December 2010, all monies from these companies have been deposited in a University of California-San Diego institutional account for research and education. R Lencioni has received research support and honoraria from Bayer HealthCare Pharmaceuticals. AM Di Bisceglie is a consultant and member of the advisory
board and has received research support from Bristo–Myers Squibb, Inc.; is a consultant for Abbott Laboratories; and is a member of the Data Safety Monitoring Board of Bayer Healthcare Pharmaceuticals. JL Raoul is a member of the advisory boards and has received honoraria from Bristol–Myers Squibb, Inc. and Bayer Healthcare Pharmaceuticals. V Mazzaferro has received research support and honoraria from Bayer HealthCare Pharmaceuticals. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
The authors thank BelMed Professional Resources, New Rochelle, NY, USA, for editorial support with funding provided by Bayer HealthCare Pharmaceuticals and Onyx Pharmaceuticals, Inc.
Role of the multidisciplinary team in diagnosis & treatment of hepatocellular carcinoma

Expert Rev. Gastroenterol. Hepatol. 6(2), (2012)184
Review
care quality. J. Natl Cancer Inst. Monogr. 2010(40), 72–80 (2010).
26 Chang TT, Sawhney R, Monto A et al. Implementation of a multidisciplinary treatment team for hepatocellular cancer at a Veterans Affairs Medical Center improves survival. HPB (Oxford) 10(6), 405–411 (2008).
27 Verslype C, Van Cutsem E, Dicato M et al. The management of hepatocellular carcinoma. Current expert opinion and recommendations derived from the 10th World Congress on gastrointestinal cancer, Barcelona, 2008. Ann. Oncol. 20(Suppl. 7), vii1–vii6 (2009).
28 Bruix J, Sherman M. Practice guidelines committee, American association for the study of liver diseases. Management of hepatocellular carcinoma. Hepatology 42(5), 1208–1236 (2005).
29 Llovet JM, Di Bisceglie AM, Bruix J et al. Panel of experts in HCC-design clinical trials. Design and end points of clinical trials in hepatocellular carcinoma. J. Natl Cancer Inst. 100(10), 698–711 (2008).
30 Martin RC II, Jarnagin WR. Randomized clinical trials in hepatocellular carcinoma and biliary cancer. Surg. Oncol. Clin. N. Am. 11(1), 193–205 (2002).
31 Lopez PM, Villanueva A, Llovet JM. Systematic review: evidence-based management of hepatocellular carcinoma – an updated analysis of randomized controlled trials. Aliment Pharmacol. Ther. 23(11), 1535–1547 (2006).
32 Yamamoto K, Imamura H, Matsuyama Y et al. AFP, AFP, AFP-L3, DCP, and GP73 as markers for monitoring treatment response and recurrence and as surrogate markers of clinicopathological variables of HCC. J. Gastroenterol. 45(12), 1272–1282 (2010).
33 Beppu T, Sugimoto K, Shiraki K et al. Clinical significance of tumor markers in detection of recurrent hepatocellular carcinoma after radiofrequency ablation. Int. J. Mol. Med. 26(3), 425–433 (2010).
34 Zhang XF, Lai EC, Kang XY et al. Lens culinaris agglutinin-reactive fraction of a-fetoprotein as a marker of prognosis and a monitor of recurrence of hepatocellular carcinoma after curative liver resection. Ann. Surg. Oncol. 18(8), 2218–2223 (2011).
35 Yamashiki N, Sugawara Y, Tamura S et al. Diagnostic accuracy of a-fetoprotein and des-g-carboxy prothrombin in screening for hepatocellular carcinoma in liver
transplant candidates. Hepatol. Res. 41(12), 1199–1207 (2011).
36 Sterling RK, Wright EC, Morgan TR et al. Frequency of elevated hepatocellular carcinoma (HCC) biomarkers in patients with advanced hepatitis C. Am. J. Gastroenterol. 107(1), 64–74 (2012).
37 Pang R, Poon RT. Angiogenesis and antiangiogenic therapy in hepatocellular carcinoma. Cancer Lett. 242(2), 151–167 (2006).
38 Abou-Alfa GK, Schwartz L, Ricci S et al. Phase 2 study of sorafenib in patients with advanced hepatocellular carcinoma. J. Clin. Oncol. 24(26), 4293–4300 (2006).
39 Llovet JM, Ricci S, Mazzaferro V et al. SHARP investigators study group. Sorafenib in advanced hepatocellular carcinoma. N. Engl J. Med. 359(4), 378–390 (2008).
•• FirstPhaseIIIrandomized,double-blind,placebo-controlledclinicaltrialshowingtheefficacyofsorafenibinthetreatmentofpatientswithadvancedHCC.
40 Cheng AL, Kang YK, Chen Z et al. Efficacy and safety of sorafenib in patients in the Asia–Pacific region with advanced hepatocellular carcinoma: a Phase 3 randomised, double-blind, placebo-controlled trial. Lancet Oncol. 10(1), 25–34 (2009).
•• PhaseIIIrandomized,double-blind,placebo-controlledclinicaltrialshowingtheefficacyofsorafenibinthetreatmentofAsianpatientswithadvancedHCC.
41 Keating GM, Santoro A. Sorafenib: a review of its use in advanced hepatocellular carcinoma. Drugs 69(2), 223–240 (2009).
42 Rimassa L, Santoro A. Sorafenib therapy in advanced hepatocellular carcinoma: the SHARP trial. Expert Rev. Anticancer Ther. 9(6), 739–745 (2009).
43 Siegel AB, Olsen SK, Magun A, Brown RS Jr. Sorafenib: where do we go from here? Hepatology 52(1), 360–369 (2010).
44 Zhu AX. Beyond sorafenib: novel targeted therapies for advanced hepatocellular carcinoma. Expert Opin. Investig. Drugs 19(5), 663–672 (2010).
45 Donckier V, Van Laethem JL, Van Gansbeke D et al. New considerations for an overall approach to treat hepatocellular carcinoma in cirrhotic patients. J. Surg. Oncol. 84(1), 36–44 (2003).
46 Wei AC, Tung-Ping Poon R, Fan ST, Wong J. Risk factors for perioperative
morbidity and mortality after extended hepatectomy for hepatocellular carcinoma. Br. J. Surg. 90(1), 33–41 (2003).
47 Laurent A, Cherqui D, Lesurtel M, Brunetti F, Tayar C, Fagniez PL. Laparoscopic liver resection for subcapsular hepatocellular carcinoma complicating chronic liver disease. Arch. Surg. 138(7), 763–769 (2003).
48 Mazzaferro V, Regalia E, Doci R et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 334(11), 693–699 (1996).
49 Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin. Liver Dis. 19(3), 329–338 (1999).
• DescriptionoftheBarcelonaClinicLiverCancerstagingsystemforHCC.
50 Carr BI, Pancoska P, Branch RA. Tumor and liver determinants of prognosis in unresectable hepatocellular carcinoma: a large case cohort study. Hepatol. Int. 4(1), 396–405 (2009).
51 Changchien CS, Chen CL, Yen YH et al. Analysis of 6381 hepatocellular carcinoma patients in southern Taiwan: prognostic features, treatment outcome, and survival. J. Gastroenterol. 43(2), 159–170 (2008).
52 A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology 28(3), 751–755 (1998).
53 Prospective validation of the CLIP score: a new prognostic system for patients with cirrhosis and hepatocellular carcinoma. The Cancer of the Liver Italian Program (CLIP) investigators. Hepatology 31(4), 840–845 (2000).
54 Leung TW, Tang AM, Zee B et al. Construction of the Chinese University prognostic index for hepatocellular carcinoma and comparison with the TNM staging system, the Okuda staging system, and the Cancer of the Liver Italian Program staging system: a study based on 926 patients. Cancer 94(6), 1760–1769 (2002).
55 Kudo M, Chung H, Osaki Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J. Gastroenterol. 38(3), 207–215 (2003).
56 Kudo M, Chung H, Haji S et al. Validation of a new prognostic staging
Gish, Lencioni, Di Bisceglie, Raoul & Mazzaferro

www.expert-reviews.com 185
Review
system for hepatocellular carcinoma: the JIS score compared with the CLIP score. Hepatology 40(6), 1396–1405 (2004).
57 Nathan H, Bridges JF, Schulick RD et al. Understanding surgical decision making in early hepatocellular carcinoma. J. Clin. Oncol. 29(6), 619–625 (2011).
58 Mazzaferro V, Llovet JM, Miceli R et al. Metroticket Investigator Study Group. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet Oncol. 10(1), 35–43 (2009).
59 Borentain P, Gregoire E, Hardwigsen J et al. Liver transplantation in a patient treated by sorafenib for hepatocellular carcinoma. Clin. Res. Hepatol. Gastroenterol. 35(3), 234–236 (2011).
60 Palma LD. Diagnostic imaging and interventional therapy of hepatocellular carcinoma. Br. J. Radiol. 71(848), 808–818 (1998).
61 Cabrera R, Nelson DR. Review article: the management of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 31(4), 461–476 (2010).
62 Ayyappan AP, Jhaveri KS. CT and MRI of hepatocellular carcinoma: an update. Expert Rev. Anticancer Ther. 10(4), 507–519 (2010).
63 Livraghi T, Meloni F. Treatment of hepatocellular carcinoma by percutaneous interventional methods. Hepatogastroenterology 49(43), 62–71 (2002).
64 Bleicher RJ, Allegra DP, Nora DT, Wood TF, Foshag LJ, Bilchik AJ. Radiofrequency ablation in 447 complex unresectable liver tumors: lessons learned. Ann. Surg. Oncol. 10(1), 52–58 (2003).
65 Georgiades CS, Hong K, Geschwind JF. Radiofrequency ablation and chemoembolization for hepatocellular carcinoma. Cancer J. 14(2), 117–122 (2008).
66 Vilana R, Bruix J, Bru C, Ayuso C, Solé M, Rodés J. Tumor size determines the efficacy of percutaneous ethanol injection for the treatment of small hepatocellular carcinoma. Hepatology 16(2), 353–357 (1992).
67 Yin XY, Xie XY, Lu MD et al. Percutaneous thermal ablation of medium and large hepatocellular carcinoma: long-term outcome and prognostic factors. Cancer 115(9), 1914–1923 (2009).
68 Lencioni R. Loco-regional treatment of hepatocellular carcinoma. Hepatology 52(2), 762–773 (2010).
• RecentreviewoflocoregionaltreatmentmethodsforHCC,includingtranscatheterarterialchemoembolizationandradiofrequencyablation.
69 McWilliams JP, Yamamoto S, Raman SS et al. Percutaneous ablation of hepatocellular carcinoma: current status. J. Vasc. Interv. Radiol. 21(Suppl. 8), S204–S213 (2010).
70 Lencioni R, Crocetti L. A critical appraisal of the literature on local ablative therapies for hepatocellular carcinoma. Clin. Liver Dis. 9(2), 301–314 (2005).
71 Liapi E, Geschwind JF. Transcatheter and ablative therapeutic approaches for solid malignancies. J. Clin. Oncol. 25(8), 978–986 (2007).
72 Chou CH, Chen PJ, Lee PH, Cheng AL, Hsu HC, Cheng JC. Radiation-induced hepatitis B virus reactivation in liver mediated by the bystander effect from irradiated endothelial cells. Clin. Cancer Res. 13(3), 851–857 (2007).
73 Cheng LF, Ma KF, Fan WC, Yung AW, Li TM, Wong CS. Hepatocellular carcinoma with extrahepatic collateral arterial supply. J. Med. Imaging Radiat. Oncol. 54(1), 26–34 (2010).
74 Salem R, Hunter RD. Yttrium-90 microspheres for the treatment of hepatocellular carcinoma: a review. Int. J. Radiat. Oncol. Biol. Phys. 66(Suppl. 2), S83–S88 (2006).
75 Boucher E, Garin E, Guylligomarc’h A, Olivié D, Boudjema K, Raoul JL. Intra-arterial injection of iodine-131-labeled lipiodol for treatment of hepatocellular carcinoma. Radiother. Oncol. 82(1), 76–82 (2007).
76 Kojiro M. Pathology. In: Diagnosis and Treatment of Hepatocellular Carcinoma. Livraghi T, Makuuchi M, Buscarini L (Eds). Greenwich Medical Media, London, UK, 27–34 (1997).
77 Frau M, Biasi F, Feo F, Pascale RM. Prognostic markers and putative therapeutic targets for hepatocellular carcinoma. Mol. Aspects Med. 31(2), 179–193 (2010).
• RecentdetaileddescriptionofprognosticmarkersinHCCandpossibletreatmenttargets.
78 Seong J, Koom WS, Park HC. Radiotherapy for painful bone metastases from hepatocellular carcinoma. Liver Int. 25(2), 261–265 (2005).
79 Guan YS, Liu Y. Interventional treatments for hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int. 5(4), 495–500 (2006).
80 Jansen MC, van Hillegersberg R, Chamuleau RA, van Delden OM, Gouma DJ, van Gulik TM. Outcome of regional and local ablative therapies for hepatocellular carcinoma: a collective review. Eur. J. Surg. Oncol. 31(4), 331–347 (2005).
81 Mazzaferro V, Majno P. Principles for the best multidisciplinary meetings. Lancet Oncol. 12(4), 323–325 (2011).
Website
101 National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Hepatobiliary cancers, version 2 (2012). www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf (Accessed 6 February 2012)
Role of the multidisciplinary team in diagnosis & treatment of hepatocellular carcinoma