Embed Size (px)
Citation preview

J. Endocrinol. Invest. 17: 733-737,1994
CASE REPORT
Riedel's thyroiditis associated with high titers of anti microsomal and antithyroglobulin antibodies and hypothyroidism F. Zelmanovitz, T. Zelmanovitz, M. Beck, C.T. Cerski, H. Schmid, and M.A. Czepielewski Division of Endocrinology and Division of Pathology, Hospital de Clinicas de Porto Alegre, Universidade Federal do Rio Grande do Sui, Porto Alegre, Brazil
ABSTRACT. Riedel's thyroiditis is a rare, chronic inflammatory disease of the thyroid gland. The aggressive fibrosis with extension beyond the thyroid into adjacent tissues contrasts with the diffuse, but intracapsular fibrosis of Hashimoto's thyroiditis. Most current studies refute the possibility of progression from a highly fibrosing form of Hashimoto's thyroiditis to a Riedel's thyroiditis based on the distinct clinical and laboratory data, although an unknown immunological basis is suggested for both diseases. The authors describe a patient with Riedel's thy-
INTRODUCTION
Riedel's thyroiditis (invasive fibrous thyroiditis, ligneous Eisenharte struma or Riedel's struma) is a rare and chronic inflammatory disease of the thyroid gland described by Riedel in 1896 (1). Its agressive fibrosis tends to progress inexorably to complete destruction of the thyroid gland but also, characteristically, spreads beyond the thyroid capsule into adjacent tissues such as nerves, blood vessels, and muscles (2, 3). Thyroid fibrosis can occur also in cases of thyroiditis (subacute or chronic), radiation thyroiditis, nodular goiter, desmoplasia, scleroderma, trauma and amyloid disease, either focally or diffusely throughout the gland (4). The distinction between Riedel's thyroiditis and Hashimoto's thyroiditis (chronic Iymphocitic thyroiditis) is controversial since Dr. Hashimoto first described the disorder associated with his eponym (4, 5). It has been suggested that Riedel's thyroiditis may represent a late form of Hashimoto's thyroiditis, but since the microscopic cri-
Key-words: Riedel's thyroiditis, anti microsomal antibodies, antithyroglabulin antibodies, hypothyroidism.
Correspondence: Dr. Flavio Zelmanovitz, Rua Fernandes Vieira 181/202, Porto Alegre, RS, CEP 90035, Brazil.
Received August 30, 1993; accepted April 5, 1994.
733
roiditis, probably associated with Hashimoto's thyroiditis, sent to surgery because her cytological examination suggested thyroid malignancy. This patient had clinical and laboratory features of hypothyroidism and very high titers of antimicrosomal and antithyroglobulin antibodies, which decreased after surgery. Pathology studies disclosed Riedel's thyroiditis with intense lymphocytic infiltration suggestive of Hashimoto's thyroiditis. Quantitative immunohistochemical studies were not able to distinguish between both diseases.
teria for the diagnosis of Riedel's thyroiditis were established by Woolner and associates in 1957 (6), and the redefinition of the fibrosing variant of Hashimoto's thyroiditis in 1974 by Katz and Vickery (7), most authors now agree that they are distinct diseases (2-4, 8-10). We describe a patient with Riedel's thyroiditis, probably associated with Hashimoto's thyroiditis, subjected to surgery because thyroid malignancy was suspected at cytological examination.
CASE REPORT
A 43-year-old woman presented with a six-month progressive goiter. She complained of gaining 10 kg in this period, tired easily, had constipation, menstrual irregularity and increased sensitivity to cold. On physical examination her height was 1.54 m, the weight was 65.0 kg. There was facial oedema including the periorbital area, with no signs of conjunctival inflamation or eye muscle involvement. The thyroid was enlarged (about 80 g) and stony hard at palpation. There was a palpable 1 cm submandibular node. The laboratory evaluation showed T4-RIA 2,1ug/dL (N: 4-12); T3-RIA 40ug/dL (N: 70-190); TSH-IRMA 112m1U/L (N: 0,4-4,0); antithyroglobulin antibodies (detected by gelatin agglutination-Sera Tek-Ames) 1/102.400 (N: less than 1/100); antimi-

F. Zelmanovitz, T. Zelmanovitz, M Beck, et al.
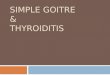
Fig. 1 - Fine needle aspiration: numerous follicular cells, some with enlarged and pleomorphic nuclei suggestive of follicular neoplasia. Giemsa stain, X 1000.
crossomal antibodies (detected by gelatin agglutination - Sera Tek - Ames) 1/1.638.400 (N: less than 1/100); calcium 9,5 mg/dL: phosphorus 4,0 mg/dL; and albumin 3,9 g/dL. The X-Ray examination of the cervical region defined a goiter with extensive calcifications which did not penetrate the mediastinum, but reduced the tracheal lumen. Fine needle aspiration of the thyroid was performed and revealed numerous follicular celis, some of which had atypies (enlarged and pleomorphic nuclei) suggestive of follicular neoplasia (Fig. 1). The patient was treated with thyroxine and underwent subtotal thyroidectomy. The procedure was not completed due to undefined tissue planes found just beneath the skin and between the goiter and the trachea. Tracheostomy was performed due to stenosis of the tracheal lumens and
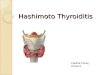
Fig. 2 - Residual follicle, extensive fibrosis and chronic inflamatory cells. HE, X 100.
734
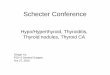
Fig . 3 - Riedel'S thyroiditis with extensive fibrosis and chronic inflamatory cells. HE, X 400.
the patient developed permanent postoperative hypoparathyroidism. Pathological studies disclosed Riedel's thyroiditis. There was diffuse fibrosis with intense lymphocytic infiltration and germinal centers in the thyroid (Fig. 2). The same histologic pattern was observed in the adjacent muscle and fat tissues (Fig. 3-4). No Hurthle cell was observed, although there was little residual thyroid tissue to be used for study. Quantitative immunohistochemical studies for Kappa and lambda chain detection with immunoperoxidase techniques was carried out on step sections taken in pairs at regular intervals throughout the block. One of each pair was used to locate Kappa chains and the other to locate Lambda chains individually. Each section was ran-
Fig. 4 - Riedel's thyroiditis with extensive fibrosis and chronic inflammatory cells infiltrating soft tissues in the immediate thyroid gland. HE, X 400.

Fig. 5 - Plasma cells containing Kappa chains. Immunoperoxidase technique, X 400.
domly examined at twenty affected fields, at a magnification of X 400, and numbers of Kappa and Lambda positive cells were expressed as a percentage of the total. The average percentage obtained was 45.6% for plasmocytes containing Kappa chains (Fig. 5) and 54.4% for plasmocytes containing Lambda chains (Fig. 6). Extracervical fibrosis was excluded by X-Rays and by computerized tomography of the abdomen and thorax. After 7 months, the patient was euthyroid and eucalcemic with thyroxine 150 I-1g q.d., calcium carbonate 2g b.i.d. and 1,25 dihydroxyvitamin 0 3 0.251-1g b.i.d.; and both the titers of antithyroglobulin antibodies and antimicrossomal antibodies decreased, respectively to 1/1600 and 1/25600, and further to 1/1600 and 1/640. Facial oedema desappeared.
Fig. 6 - Plasma cells containing Lambda chains. Immunoperoxidase technique, X 400.
Riedel's thyroiditis and hypothyroidism
DISCUSSION
Riedel's thyroiditis is a very rare disorder, with only 185 cases reported in the english language until 1988 (11), with a reported incidence between 0.03 and 0.98 of thyroidectomies in several surgical series (2). It was 0.06% in the Mayo Clinic series where only 37 cases were diagnosed between 1920 and 1984 (12). The etiology remains unknown and, although an immunological basis is suggested for it , as for Hashimoto's thyroiditis, only two cases of progression from the latter to Riedel's thyroiditis have been described (10,13). Harach and Williams suggested that immunochemical distinctions were possible by quantitative studies of the immunoglobulincontaining cells. These studies showed that, in fibrous Hashimoto's thyroiditis, cells containing kappa light chains outnumbered lambda-containing cells (64% vs 36%) and IgG-containing cells predominated over the IgA cells (85 vs 15%), but the opposite occurred in all Riedel's thyroiditis cases studied (29 vs 71 % and 53 vs 47%) (14). The same high proportion of IgA- and lambda-containing cells were found in the inflammatory cells infiltrating retroperitonial fibrosis, strengthening its common immunological basis with Riedel's thyroiditis (15). The patient described here had an inconclusive quantitative immunohistochemical study with results just between those found in Riedel's and Hashimoto's thyroiditis. Other clinical and pathologic features allow differentiation between Riedel's and Hashimoto's thyroiditis (Table 1), but some similar findings may exist and cause problems for the definitive diagnosis. Hay et al. found appreciable titers of thyroid autoantibodies in 45% of the patients with Riedel's thyroiditis tested in the Mayo Clinic series (12). Schwaegerle and associates, reviewing the 185 reported cases, found similar proportions of C04- and CD8-positive lymphocytes in Riedel's and Hashimoto's thyroiditis, and positive titers for thyroid antibodies in 67% of the 25 patients tested (11). Our patient showed very high titers of thyroid autoantibodies which declined after surgery. This is highly suggestive of the coexistence of Hashimoto's thyroiditis, but may also reflect an epiphenomenon, a reaction to antigens released from destroyed thyroid tissue as proposed by Schwaegerle (11). Livolsi describes the fibrosis of Hashimoto's thyroiditis as not destroying the gland lobulation that is noted at low power. Broad fibrous bands separate residual zones of degenerating thyroid. The latter shows changes reminiscent of classic chronic lymphocytic thyroiditis, including follicular atrophy, oxyphil metaplasia and lymphoid infiltration with ger-
735

F. Zelmanovitz, T Zelmanovitz, M Beck, et al.
Table 1 - Clinical and pathologic features of thyroiditis.
Riedel
30-70
2-4/1
Hashimoto
20-50 Age (years)
Sex (F/M)
Symptoms
Thyroid antibodies
Following
Pressure goiter
Negative/very low
Rare hypothyroidism
4-10/1
Goiter/hypothyroid
Positive/high
Common progression to hypothyroidism
No Lobulation
Consistency
Extrathyroid invasion
Hurtle cells
Lymphocitis
Stony hard
yes
no
Gland architecture
Vascular changes
sparse
Effaced
Vasculitis
minal centers. This findings may be used to distinguish Hashimoto's from Riedel's thyroiditis (4). The specimen obtained from our patient did not have enough thyroid tissue to show thyroid areas of integrallobulation and oxyphil metaplasia, but it had intense lymphoid infiltration and germinal centers. It is not unusual for a case of Riedel's thyroiditis to present as suspected neoplasia (16) . The differential diagnosis with an anaplastic carcinoma due to the iron-hard consistency and major involvement of cervical structures should be considered less likely in young patients. The anaplastic carcinoma hypothesis was considered more probable in our middle-aged patient because she had a positive citopathology study and because we have an unusually high incidence of anaplastic carcinoma (17% of cancers) , but just one case of Riedel 's thyroiditis in more than 480 thyroidectomies reviewed. Kini (17) describes the fine-needle byopsy specimen in Riedel's thyroiditis as acellular due to fibrosis , although the thyroid may be totally or partially involved (4) . The specimen obtained in our case revealed numerous follicular cells, some of which had atypies suggestive of follicular neoplasia. The same occured in a case described by Marin et al. (16) , and their patient also showed Hurthle cells and had antimicrosomal antibody titers of 1/25.000 and hypothyroidism. The possibility of Hashimoto's thyroiditis involving the areas not destroyed by Riedel's thyroiditis should be suspected in both cases, as Hashimoto's thyroiditis is a classic pitfall in cytopathology, simulating cancer of the thyroid (18) and since hypothyroidism is not very common in Riedel's thyroiditis.
736
yes
Firm
no
yes
Markedly diffuse
Preserved
Absent
The association of Riedel's thyroiditis with other extracervical fiblosclerosis was first reported by Bowlby in 1885 (19). It was increasingly recognized since 1962, in 34% of the published cases (11), and may occur as an orbital pseudotumor (20), lacrimal gland fibrosis (21), retroperitoneal fibrosis (22) , mediastinal fibrosis (23), sclerosing cholangitis (24) or fibrous parotitis (25) . The patient described here showed no evidence of mediastinal or retroperitonial fibrosis at X-Ray, and no symptoms related to fibrosis at other sites, but it is acknowledged that it may occur at some point after diagnosis, requiring strict follow-up (2) . Surgery is indicated in Riedel's thyroiditis for two main reasons: to exclude carcinoma, when it should be kept in mind to limit the extent of surgery if no malignancy is found; and to relieve tracheal compression, when the operation is limited to excising a wedge of thyroid isthmus if the process is diffuse (2) . A trial for more extensive surgical intervention, as performed in our case, may encounter major difficulties , for instance undefined tissue planes with an increased risk of injury to adjacent structures such as the carotid arteries, the trachea, the recurrent laringeal nerves or the parathyroids. The association with hypoparathyroidism is unusual , but its occurrence is not rare after thyroidectomy. This can be explained by the previous destruction of some of the parathyroid glands secondary to the invasive nature of Riedel's disease (16). In conclusion, Riedel's thyroiditis, although not necessarilya late stage of Hashimoto's thyroiditis , may be associated with it, further complicating the clinical and pathological diagnosis. It should always

be considered in the diferential diagnosis of large or stony-hard cervical lesions, especially in young patients, in order to prevent extensive and risky surgery.
REFERENCES 1. Riedel B.M.
Die chronische zur Bildung eisenharter Tumoren fuhrende Entzundung der Schilddruse. Vern. dt. Ges. Chir. 25: 101, 1896.
2. Volpe R. Invasive Fibrous (Riedel's) Thyroiditis In: Burrow G.N., Oppenheimer J.H., Volpe R. (Eds.), Thyroid function and disease. WB. Saunders Company, Philadelphia, 1989, p. 208.
3. Hay 1.0. Thyroiditis: a clinical update. Mayo Clin. Proc. 60: 836, 1985.
4. Li Volsi VA Fibrosis in the thyroid. In: Li Volsi VA (Ed.), Surgical Pathology of the Thyroid. W.B. Saunders Company, Philadelphia, 1990, p. 98.
5. Hashimoto H. Zur Kenntnis der Lymphomatosen Veranderung der Schildruse (Struma Lymphomatosa). Arch. Klin. Chir. 97: 219, 1912.
6. Woolner L.B., McConahey W.M., Beahrs O.H. Invasive fibrous thyroiditis (Riedel's struma). J. Clin. Endocrinol. Metab. 17: 201,1957.
7. Katz S.M., Vickery A.L. The fibrous variant of Hashimoto's thyroiditis. Hum. Pathol. 5: 161, 1974.
8. Oertel J.E., Li Volsi VA Pathology of thyroid disease. In: Ingbar S.H., Bravermann L.E. (Eds.), Werner's The thyroid. A fundamental and clinical text. J.B. Lippincott Company, Philadelphia, 1986, p. 658.
9. McGregor A.M., Hall R. Thyroiditis. In: De Groot L.J. (Ed.), Endocrinology. WB. Saunders Company, Philadelphia, 1989, p. 683.
10. Merrington W.R. Chronic thyroiditis: a case showing features of both Riedel's and Hashimoto's thyroiditis. Br. J. Surg. 35:423, 1948.
11. Schwaegerle S.M., Bauer TW., Esselstyn C.B. Riedel's thyroiditis. Am. J. Clin. Pathol. 90:715,1988.
12. Hay 1.0., McConahey WM., Carney JA, Woolner L.B. Invasive fibrous thyroiditis (Riedel's struma) and as-
737
Riedel's thyroiditis and hypothyroidism
sociated extracervical fibrosclerosis: Bowlby's disease revisited. Ann. Endocrinol. (Abstract) 43: 29A, 1982.
13. Beierwaltes W. Thyroiditis. Ann. N.Y. Acad. Sci. 124: 586, 1965.
14. Harach H.R., Williams ED. Fibrous thyroiditis-an immunological study. Histopathology 7: 739, 1983.
15. Munro J.M., Van Der Walt JD., Cox EL A comparison of cytoplasmatic immunoglobulins in retroperitoneal fibrosis and abdominal aortic aneurysms. Histopathology 10: 1163, 1986.
16. Marin F., Araujo R., Paramo C., Lucas T., Saito L. Riedel's thyroiditis associated with hypothyroidism and hypoparathyroidism. Postgrad. Med. J. 65: 381, 1989.
17. Kini S.R. Thyroiditis. In: Kini S.R. (Ed), Guides to clinical aspiration biopsy thyroid. Igaku-Shoin, New York, 1987, p. 235.
18. Worstman J., Dietrich J., Apesus J., Folse R. Hashimoto's thyroiditis simulating cancer of the thyroid. Arch. Surg. 116:386,1981.
19. Bowlby AA Diseases of the ductless glands. Infiltrating fibroma (?sarcoma) of the thyroid gland. Trans. Pathol. Soc. (London) 36.' 420, 1885.
20. Hadley J., Coady AT, Milford CA Pseudotumor of the maxillary antrum. J. Laryngol. Otol. 104: 244, 1990.
21. Sclare G., Luxton W Fibrosis of the thyroid and lacrimal glands. Br. J. Ophtalm 51.'173,1967.
22. Miro I., Bakir R., Chanu B., Brocheriou C., Brenot F., Rouffy J. Thyroidite de Riedel et fibrose retroperitoneale. Ann. Med. Interne 135: 212,1984.
23. Westhoff M. Riedel-Struma und fibrose Mediastinitis. Dtsch. Med. Wschr. 113:337,1988.
24. Bartholomew L.G., Cain J.C., Woolner L.B., Utz D.C., Ferris D.O. Sclerosing cholangitis: its possible association with Riedel's struma and fibrous retroperitonitis: report of two cases. N. Engl. J. Med. 269: 8,1963.
25. Hines R.C., Scheuermann H.A., Royster H.P., Rose E. Invasive fibrous (Riedel's thyroiditis) with bilateral fibrous parotitis. JAMA 213: 869,1970.




![Hashimoto’s Thyroiditis and Encephalopathy · Hashimoto’s Thyroiditis and Encephalopathy David S. Younger Department of Neurology, ... [36]. In humans, disease susceptibility](https://img.pdfslide.us/doc/110x75/5c814ac809d3f263728c0c55/hashimotos-thyroiditis-and-hashimotos-thyroiditis-and-encephalopathy-david.jpg)


![Riedel’s thyroiditis presenting as large retropharyngeal ... · in literature are multinodular goiters[2,8,9] with one large study failing to mention the pathology of the goiter.[3]](https://img.pdfslide.us/doc/110x75/5b6a1e7a7f8b9af6098bb781/riedels-thyroiditis-presenting-as-large-retropharyngeal-in-literature.jpg)